


Abstract
Background Posterior long-segment (LS) fixation, short-segment (SS) fixation, and short segment fixation with intermediate screws (SI) have shown good outcomes for the treatment of thoracolumbar burst fractures. However, limited data compared the biomechanical properties between LS fixation and SI. The purpose of this study was to compare the von Mises stresses on the pedicular screw system and bone between posterior LS fixation, SS fixation, and SI for the treatment of thoracolumbar burst fracture.
Materials and Methods The finite element model of thoracolumbar spines from T11 to L3 was created based on the computed tomography image of a patient with a burst fracture of the L1 vertebral body. The models of pedicular screws, rods, and locking nuts were constructed based on information from the manufacturer. Three models with different fixation configurations—that is, LS, SS, and SI—were established. The axial load was applied to the superior surface of the model. The inferior surface was fixed. The stress on each screw, rod, and vertebral body was analyzed.
Results The motion of the spine in SS (0.5 mm) and SI (0.9 mm) was higher than in LS (0.2 mm). In all models, the lowest pedicle screws are the most stressed. The stress along the connecting rods was comparable between SI and LS (50 MPa). At the fracture level, stress was found at the pedicles and vertebral bodies in SI. There was relatively little stress around the fractured vertebral body in LS and SS.
Conclusions Posterior SI preserves more spinal motion than the LS. In addition, it provides favorable biomechanical properties than the SS. The stress that occurred around the pedicle screws in SI was the least among the 3 constructs, which might reduce complications such as implant failure. SI produces more stress in the fractured vertebral body than LS and SS, which could potentially aid in bone healing according to the Wolff law.
Clinical Relevance SI has proved to be a biomechanically favorable construct and helps preserve the spinal motion segment. It could be an alternative surgical option for treating patients who present with thoracolumbar burst fractures.
Level of Evidence 5.
Introduction
Thoracolumbar junction is the most common site of spine injury. The incidence of these injuries is still rising according to an increasing number of high-energy traumas.1 Although common, definitive treatment of thoracolumbar burst fracture is still controversial. In patients with stable thoracolumbar burst fracture without neurological deficits, conservative treatment has shown an improvement in pain, functional outcome, fewer complications, length of hospital stay, and treatment cost.2,3 While operative treatment for unstable fracture has shown earlier improved pain, improved functional outcome, better kyphosis correction, and better neurologic recovery, the ideal surgical procedure is still disputed.2,3
Many operative techniques have been described for adequate treatment of thoracolumbar burst fracture, including anterior stabilization, posterior stabilization, and combined anterior-posterior stabilization with or without fusion. As for posterior stabilization, long-segment (LS) fixation has shown better surgical and radiographic outcomes than short-segment (SS) fixation.4–7 However, decreased spinal range of motion from the LS fixation may lead to unfavorable results.8
Recently, posterior short-segment fixation with intermediate screws (SI) has been introduced, showing good biomechanical stability, kyphosis correction, and motion preservation.9–12 Nevertheless, there are limited data comparing the biomechanical properties between LS and SI. Our study compared biomechanical parameters between posterior LS fixation, SS fixation, and SI for the treatment of thoracolumbar burst fracture by using the finite element model analysis.13–16
Methods
This research was financially supported by a grant from Ratchadapiseksompotch Fund, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand (Grant number RA57/030). Written informed consent was waived.
Finite Element Models Generation
A model of thoracolumbar spines from T11 to L3 was created based on computed tomography images of a patient with a burst fracture of the L1 vertebral body with a McCormack score <7, according to McCormack’s load sharing classification of spine fractures, using a 3-dimensional image processing software, Mimics (Materialise, 2018). The finite element model was then developed from the 3-dimensional model obtained from the computed tomography image with the meshing software, HyperMesh (Altair Engineering, USA). The finite element volume meshes, which consisted of 4-node tetrahedral elements, were generated with mesh positions to allow for force transmission and simulation of contacts between vertebral bodies and intervertebral discs inside the model. The material and anatomical properties of the vertebral bodies, intervertebral disc, and ligaments were based on the previous literature.14,16 The models of pedicular screws, rods, and locking nuts were constructed based on the information from the manufacturer (Medtronic, MN, USA). A finite element solver, Marc Mentat (MSC Software, USA), was used to perform all the finite element analyses in this study.
Finite Element Models Validation
The finite element models of thoracolumbar spines were tested for biomechanical properties and compared with the solid model of the thoracolumbar spine. The models of pedicular screws, rods, and locking nuts were tested for biomechanical properties and compared with the actual pedicular screws, rods, and locking nuts from the manufacturer (Medtronic, MN, USA).
Instrumentations
Three types of construct models, including LS, SS, and SI, were created and attached to the burst fracture model. The diameter of the screw was 6.5 mm, and the total length of the screw was 45 mm. The LS consisted of pedicular screws at T11 to L3, except at the L1 level. The SS consisted of pedicular screws at T12 to L2, except at the L1 level, and SI consisted of pedicular screws from T12 to L2.
Biomechanical Testing
The inferior surface of the L3 vertebral body was constrained to the surface to prevent movement in all degrees of freedom. The other vertebral bodies had no restrictions in all directions. A compressive load of 1000 N was applied to the superior surface of the T11 vertebral body, representing the physiologic load supported by the spine of a 70-kg man in a standing position.17 The highest stress and stress distribution on each pedicular screw, connecting rod, vertebral body, and pedicle were analyzed. The sagittal range of motion of the whole model was recorded.
Results
Motion
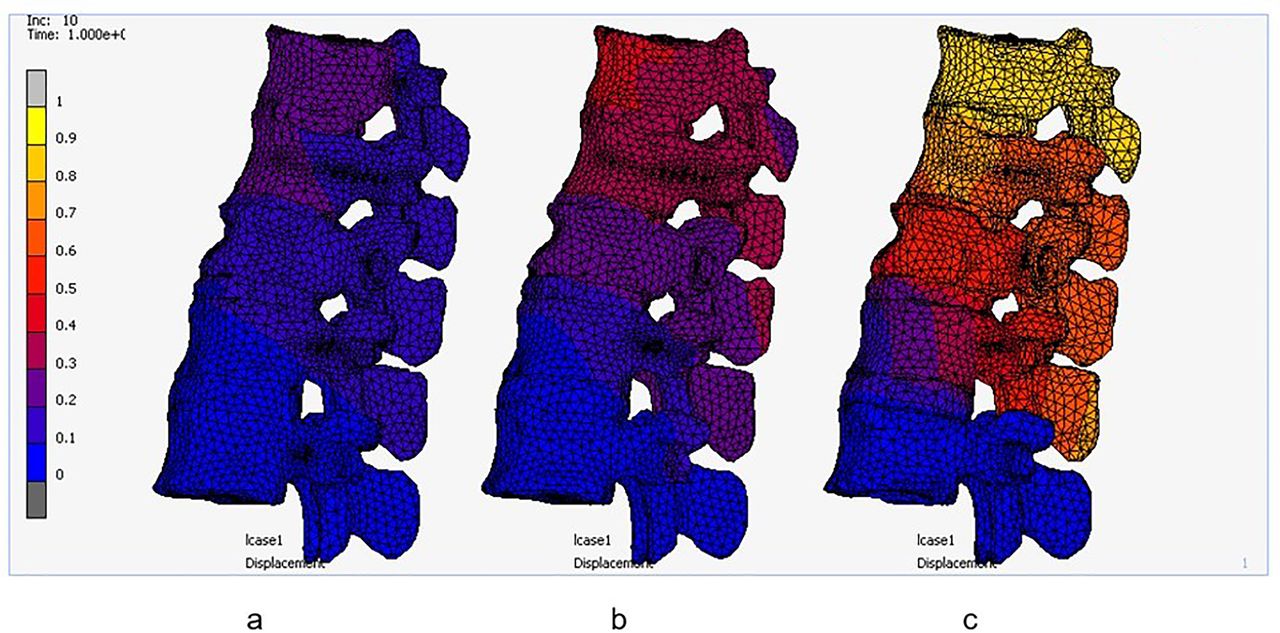
Both SS and SI showed a higher sagittal range of motion than LS. Total displacement in the sagittal plane of the spine model was 0.2 mm for LS, 0.5 mm for SS fixation, and 0.9 mm for SI (Figure 1).
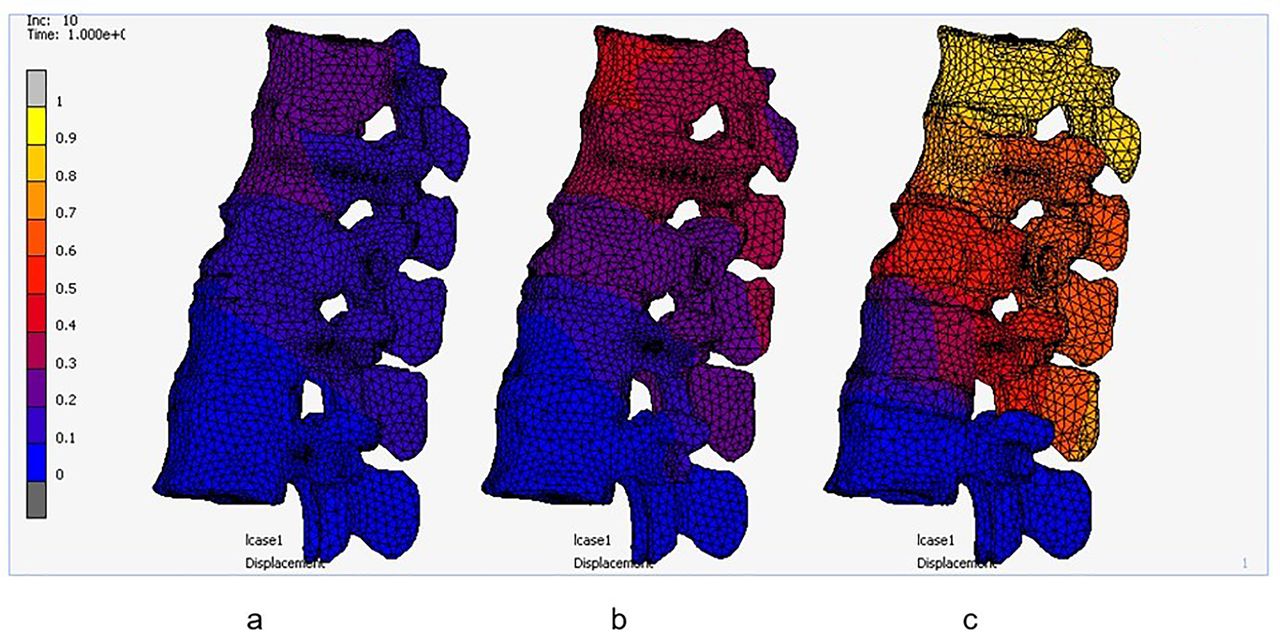
Total displacement after applying load (mm). (a) Long-segment fixation, (b) short-segment fixation, and (c) short-segment fixation with intermediate screws.
Stress on Pedicle Screws and Rods
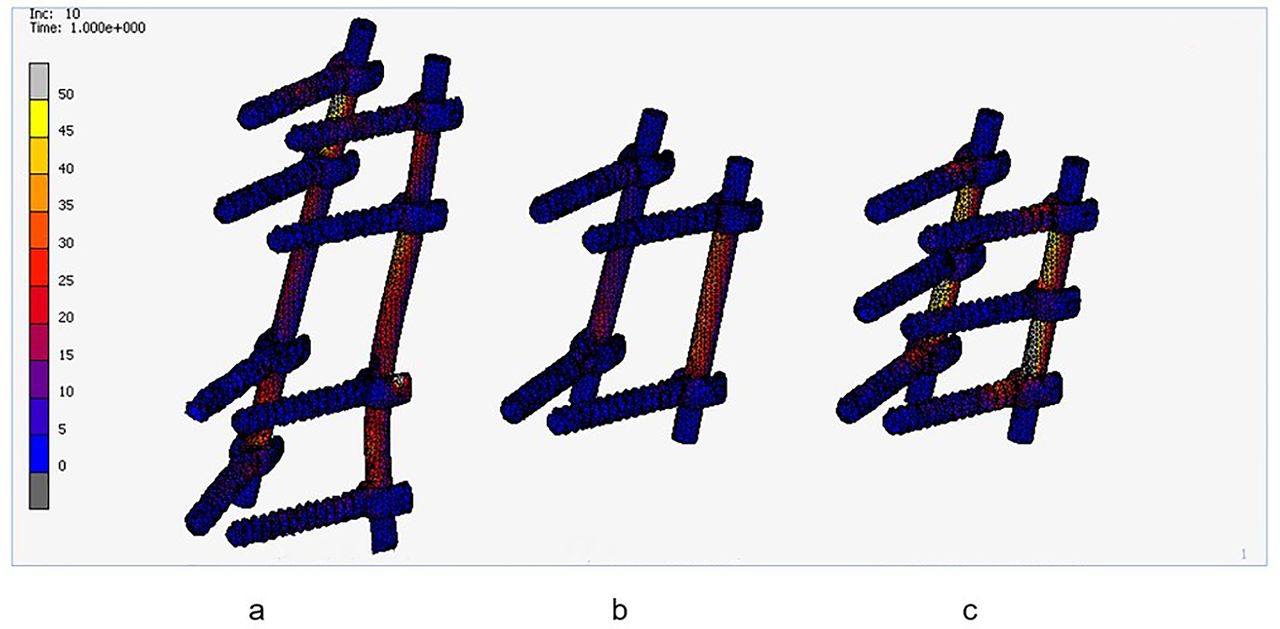
The stresses that occurred along the connecting rods (Figure 2) were found to be the highest in LS and SI (50 MPa) when compared with SS (30 MPa). While the highest stress on pedicle screws was found at the lowest pedicle screw level in every model (Figures 3–7), a small difference in stress concentration on pedicle screws was found.
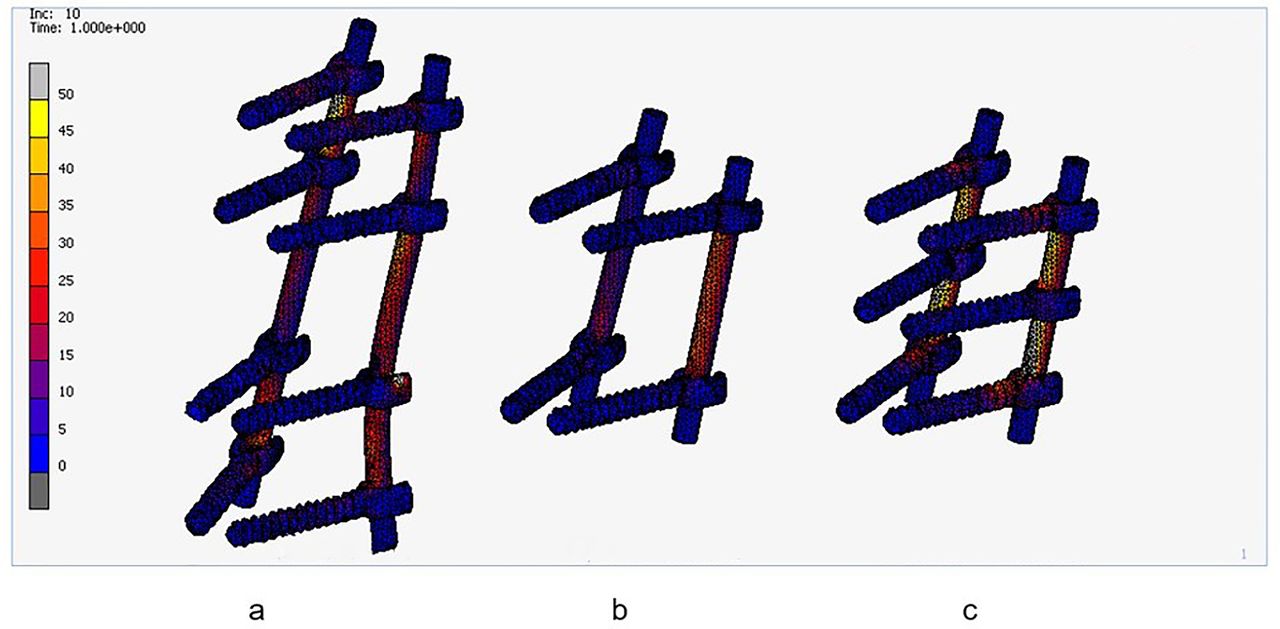
Stress in the rods after applying load (MPa). (a) Long-segment fixation, (b) short-segment fixation, and (c) short-segment fixation with intermediate screws.
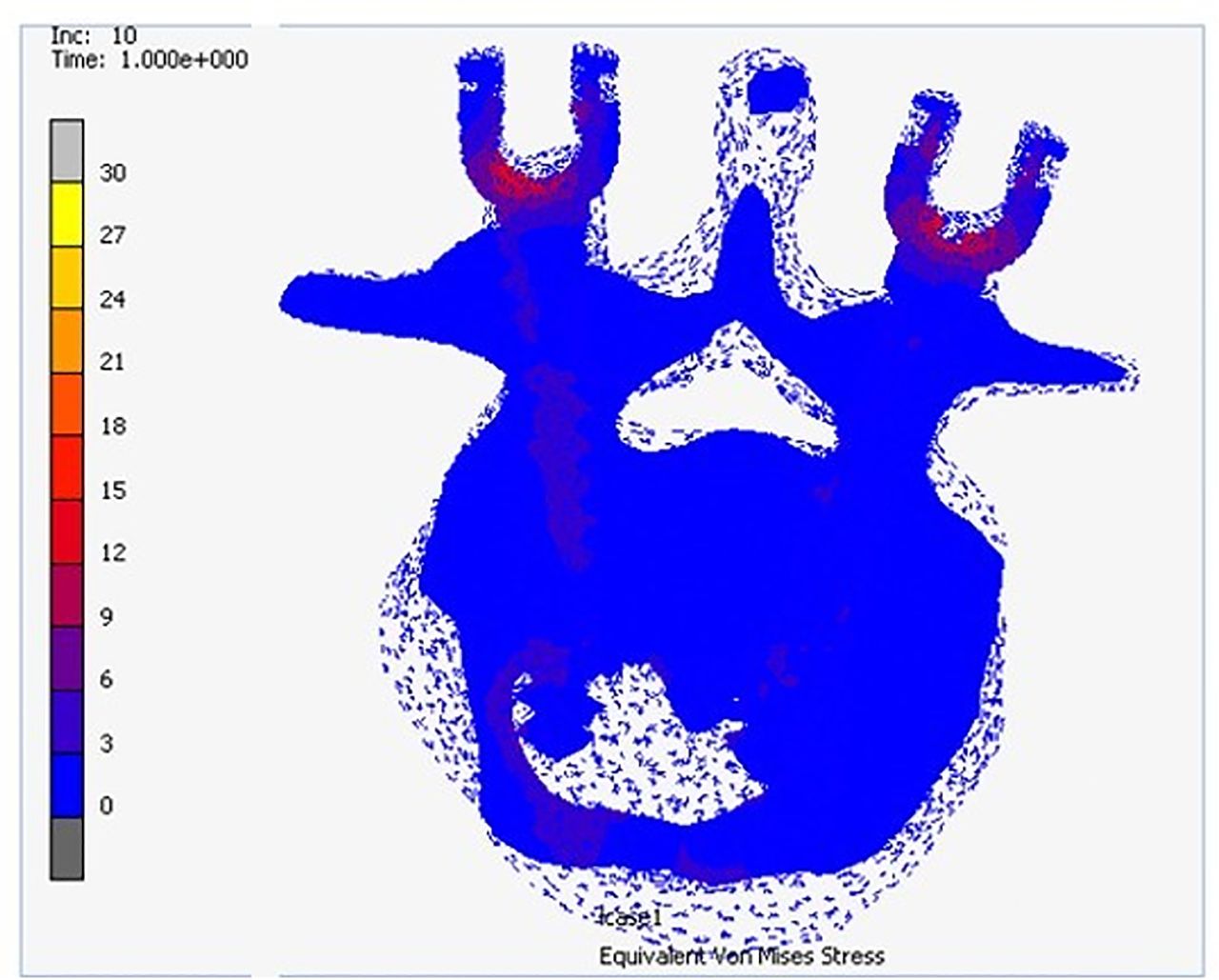
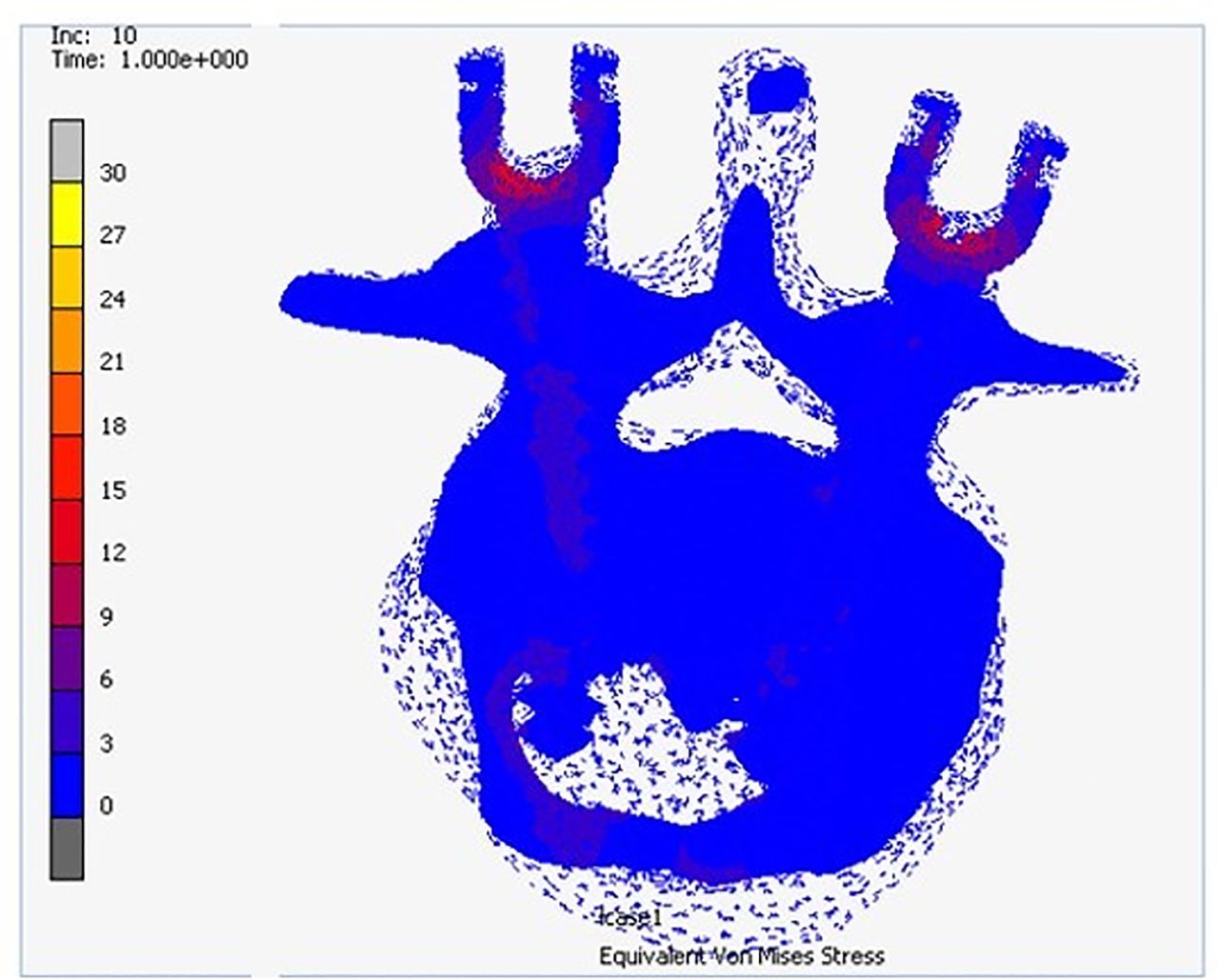
Stress in the T11 vertebral body after applying load (MPa) in long-segment fixation.
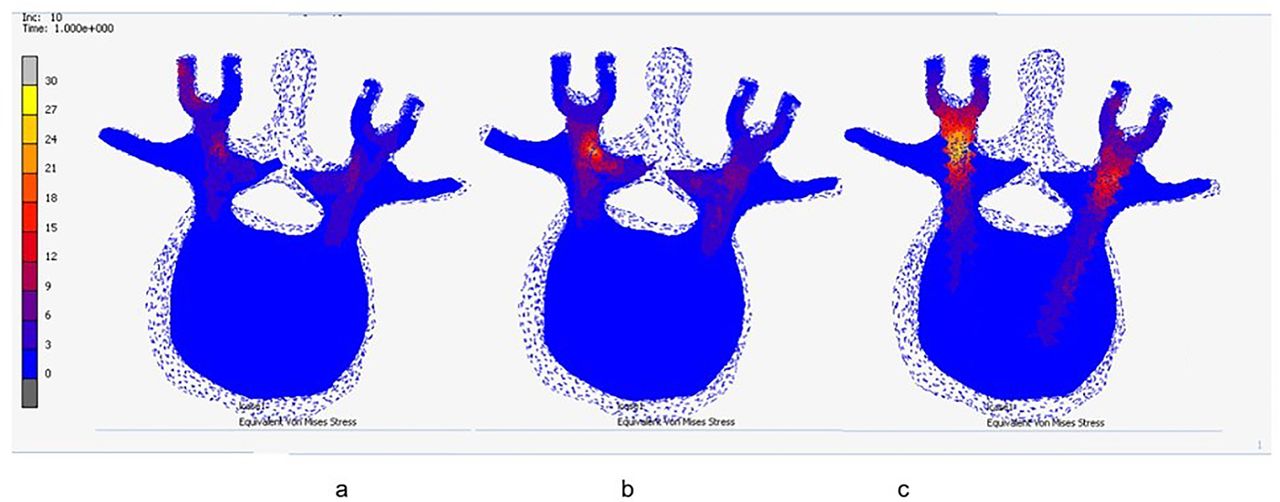
Stress in the T12 vertebral body after applying load (MPa). (a) Long-segment fixation, (b) short-segment fixation, and (c) short-segment fixation with intermediate screws.
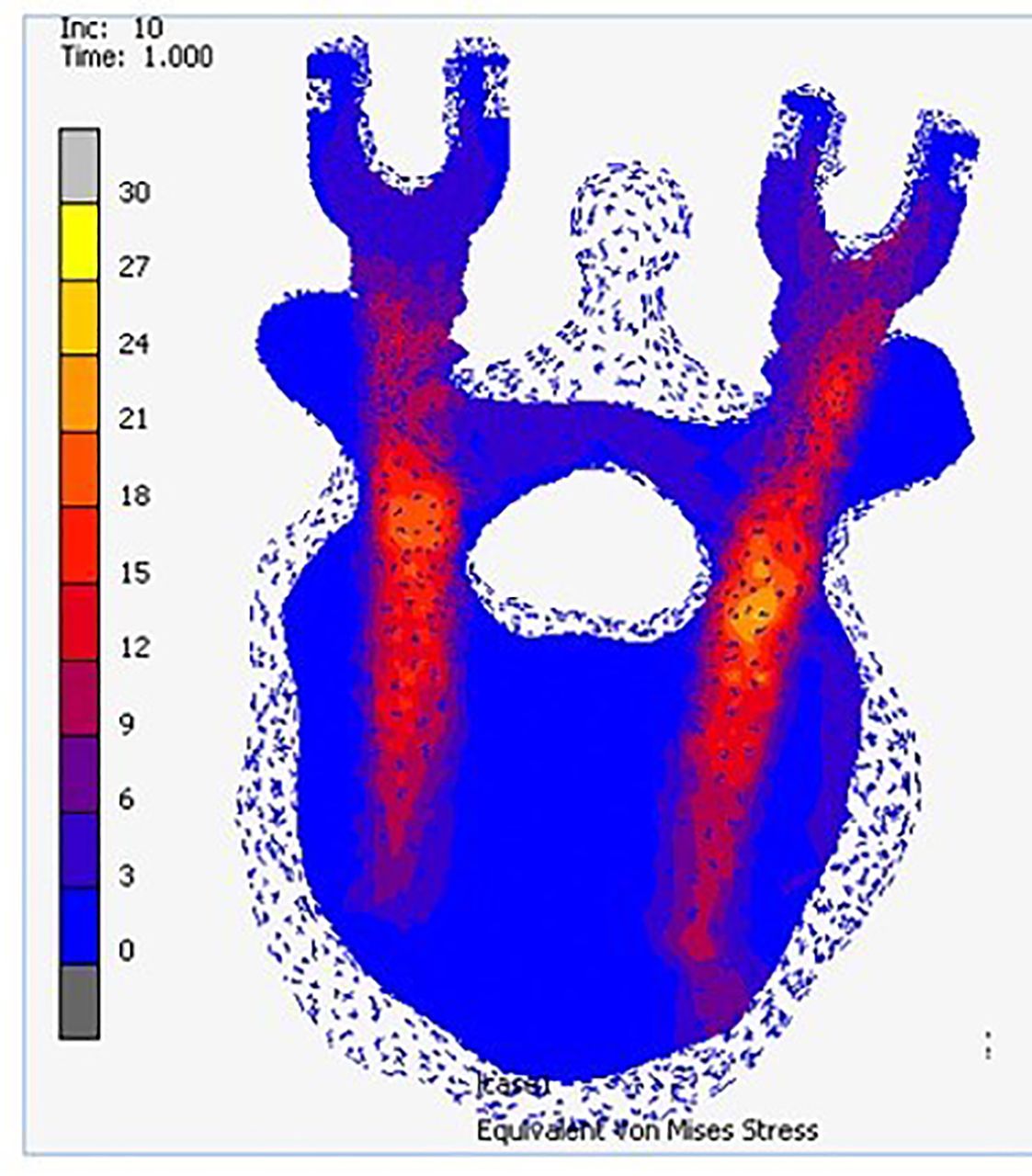
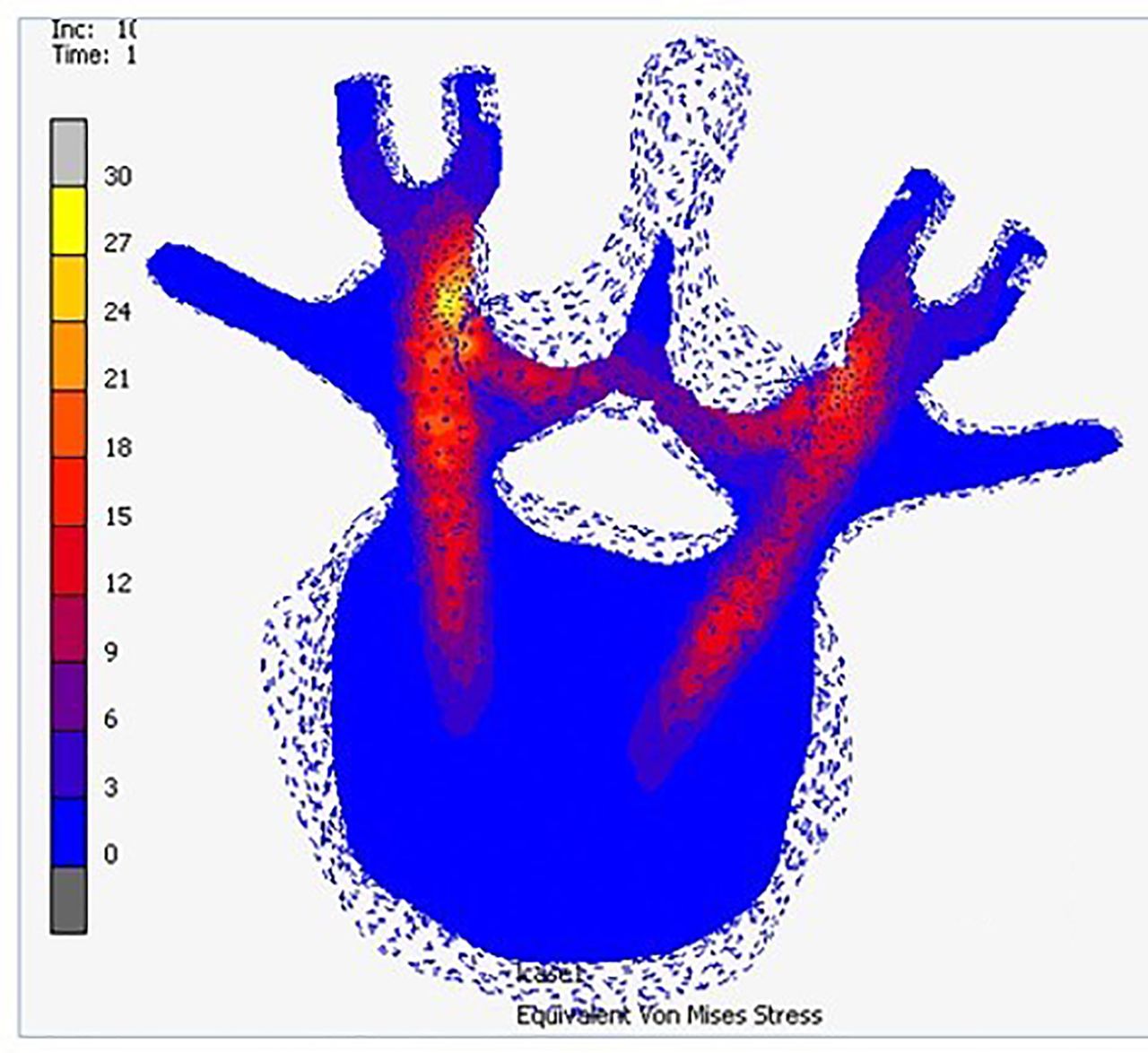
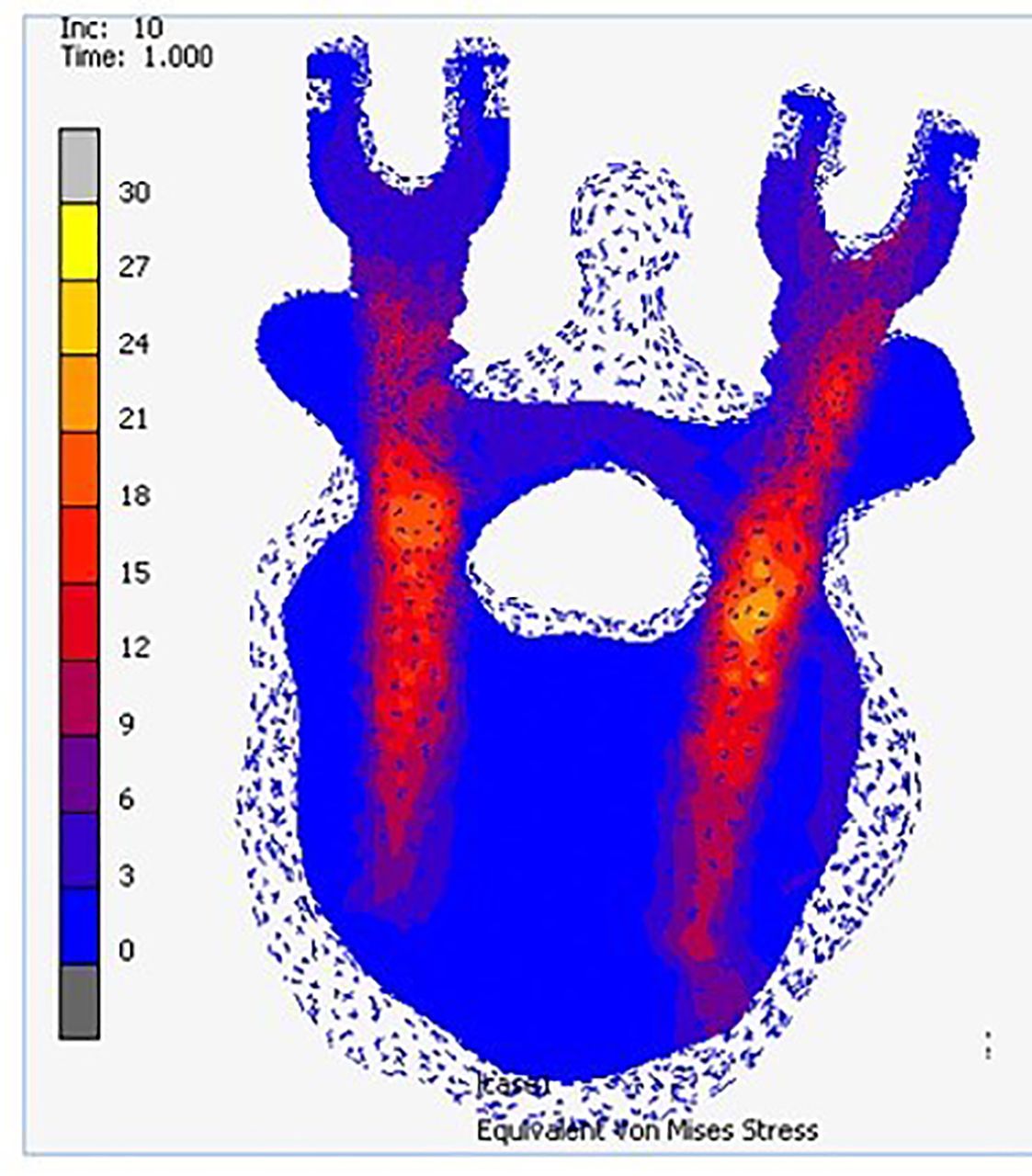
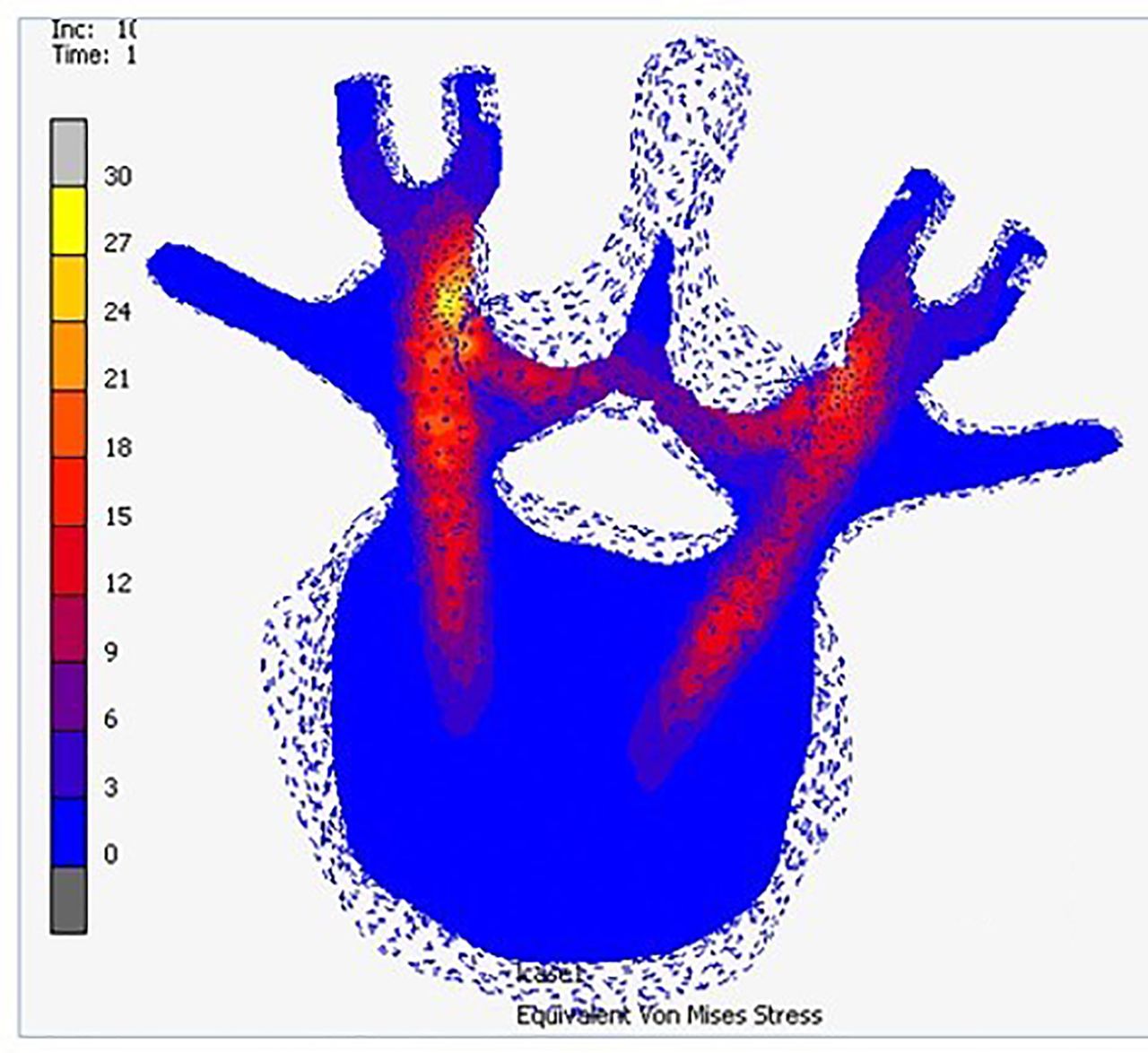
Stress in the L1 vertebral body after applying load (MPa) in short-segment fixation with intermediate screws.
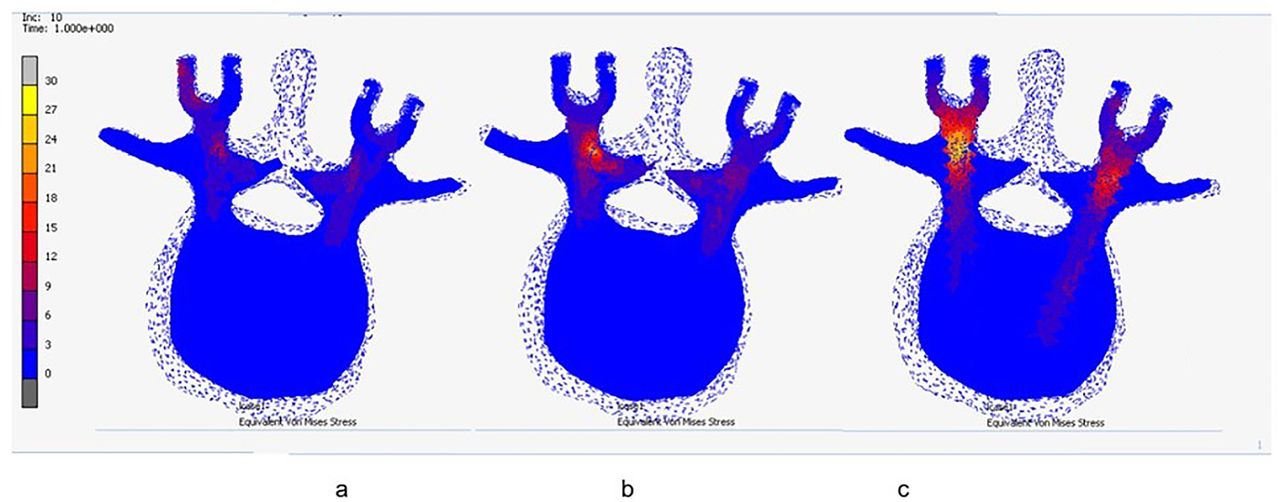
Stress in the L2 vertebral body after applying load (MPa). (a) Long-segment fixation, (b) short-segment fixation, and (c) short-segment fixation with intermediate screws.
Stress in the L3 vertebral body after applying load (MPa) in long-segment fixation.
Stress on Bone
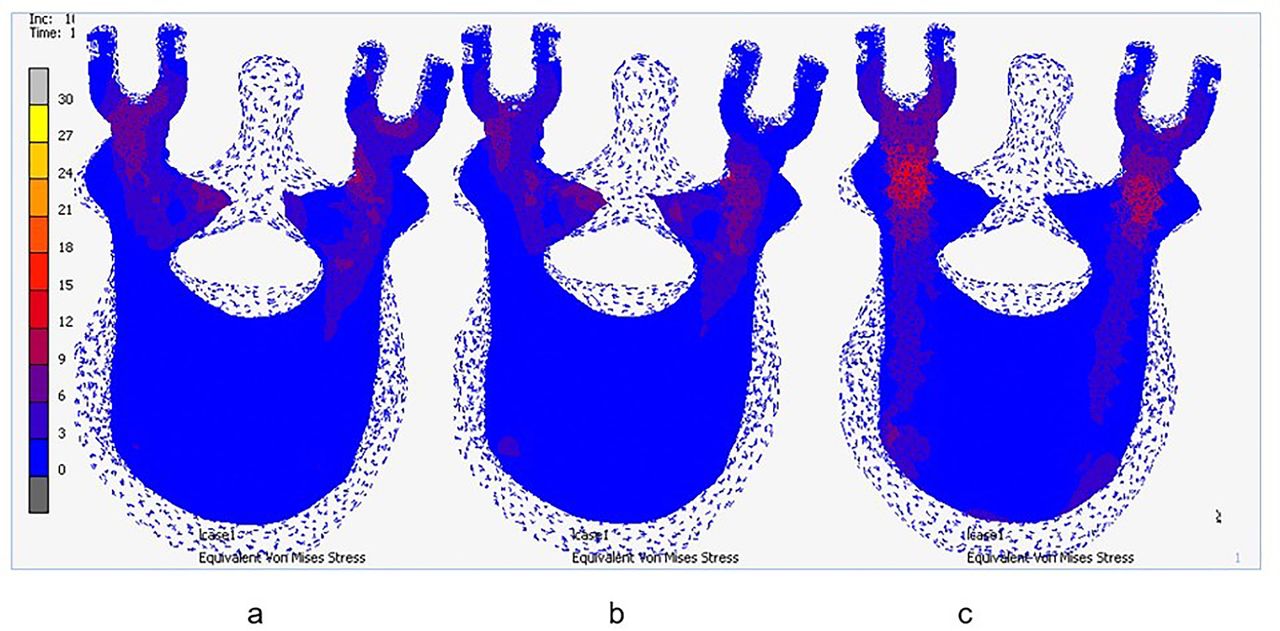
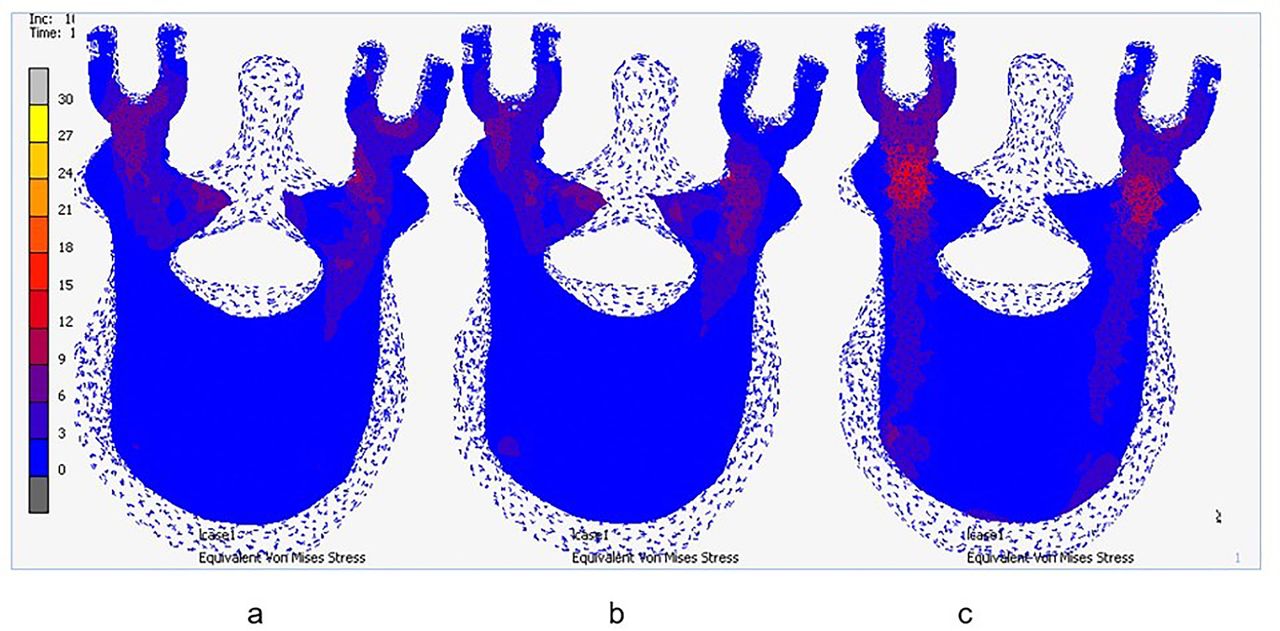
The highest stress on the vertebral body was observed at the lowest level in both LS and SS. The magnitude of the resulting von Mises stress on the pedicle of LS fixation (31.56 MPa) and SS fixation (42.16 MPa) was approximately 3 to 4 times that of the resulting stress on the pedicle of SI (10.67 MPa).
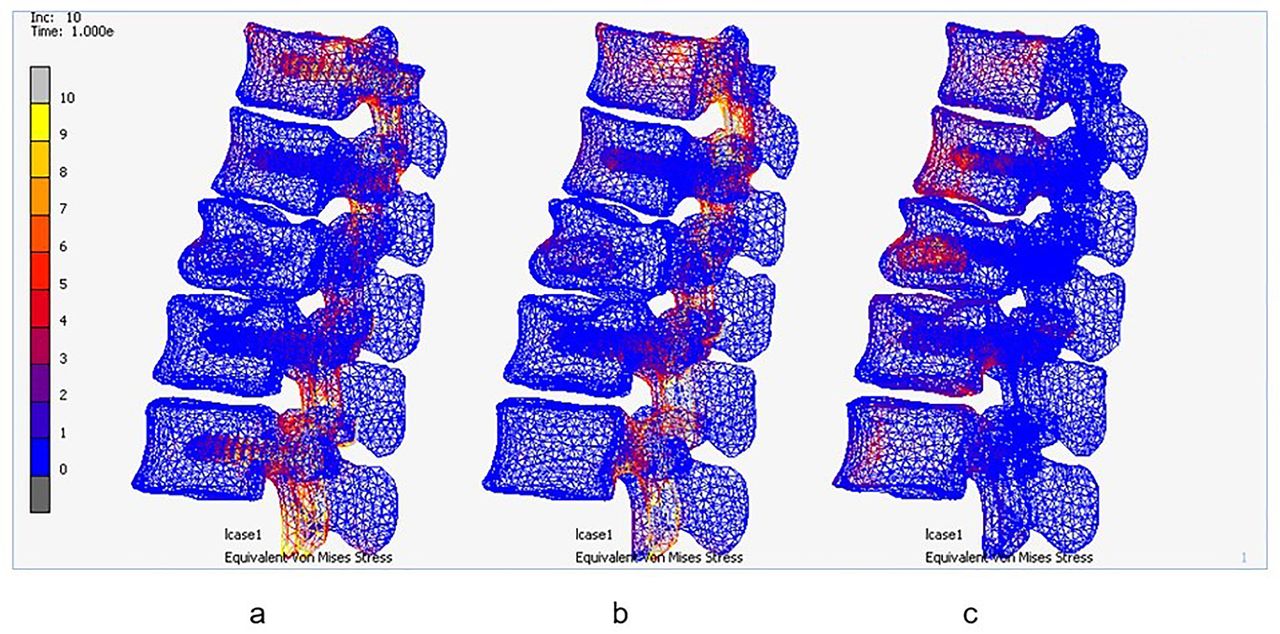
There were some differences in the amount of stress that occurred at the fracture level (Figure 8). There was relatively little stress that occurred around the fractured vertebral body in LS and SS, whereas a noticeable amount of stress was predicted at the pedicle and the fractured vertebral body in SI.
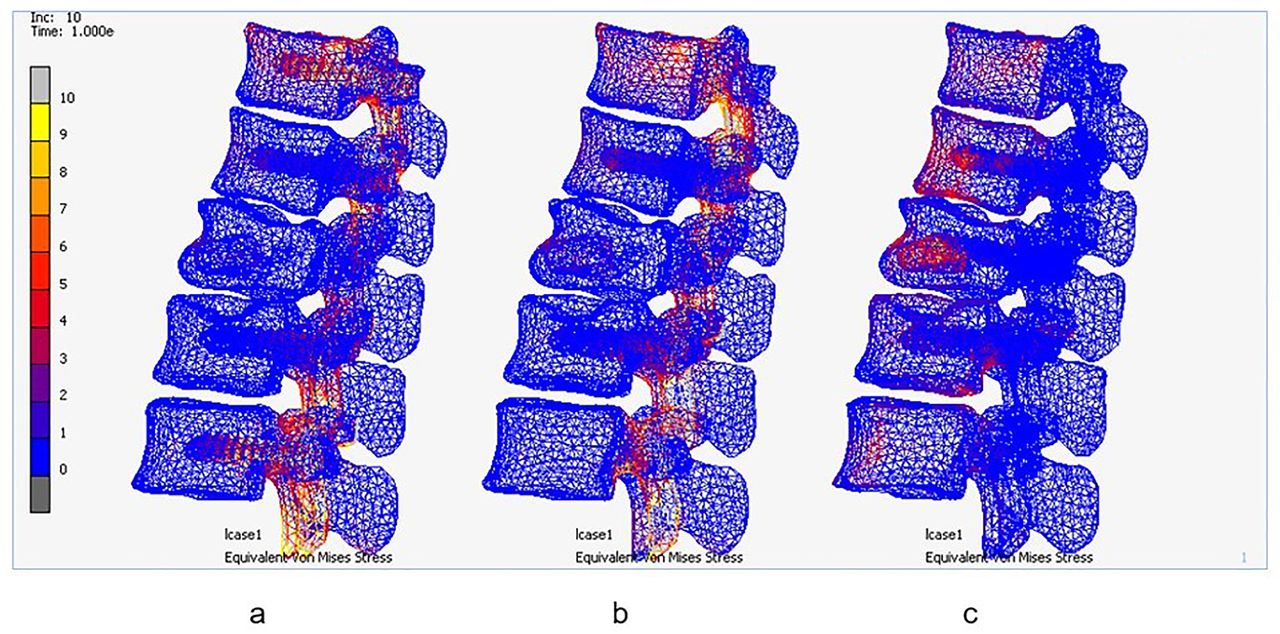
Stress in the bones after applying load (MPa). (a) Long-segment fixation, (b) short-segment fixation, and (c) short-segment fixation with intermediate screws.
Discussion
Spinal fusion was associated with decreased spinal range of motion.8 The number of fusion levels was also associated with an increased risk of adjacent segment disease.18 Lazaro et al reported a significantly restricted range of motion during extension and lateral bending after LS than the most rigid SS construct in their study.4 Altay et al suggested SS in patients who needed more spinal mobility.5 Kim et al discovered that SI is comparable with or better than LS and has the added benefit of preserving an extra mobile segment.12 However, the study comparing the biomechanical properties between LS, SS, and SI is still limited. In our study, the models of SS and SI showed a greater range of motion than LS under the same axial load, which could confirm that SS and SI could preserve more spinal motion than LS.
Instrumentation failure could be found after operative treatment for thoracolumbar burst fracture, especially when using posterior SS in unstable fractures. While screw bending, breakage, loosening, and backing out were the common failures of pedicle screws,19–21 fatigue failure was a common mode of failure for connecting rods.22 Mahar et al reported improved biomechanical stability of the construct after fixation with screws at the fracture level.9 Eno et al also reported a decrease in implant failure rates and reoperation rates after performing the SI compared with the SS.11 In our study, SI showed better biomechanical properties than the other fixations. The stress that occurred around the connecting rods showed no difference between LS and SI. Additionally, there was little difference in the amount of stress that occurred around the pedicular screws of the 3 models. The highest amount of stress would occur at the lowest pedicular screws. Pedicles at T12 to L5 levels could accommodate screws of 7 mm diameter.23 Increasing the diameter of screws, withstanding higher stress, and increasing pull-out strength could also decrease the rate of instrument failure.22
One of the complications of a thoracolumbar burst fracture that could cause pain, sagittal collapse, and neurological deficits was kyphotic deformity.24 The best treatment is prevention of this complication. Altay et al reported better correction values of the Sagittal Index and canal compromise after LS when compared with SS.5 Tezeren et al also reported correction loss of >10° with a 55% implant failure rate in the SS group, whereas none of the patients had a correction loss >10° and there was no failure in the LS group.6 Sapkas et al used radiographic measurements to compare LS and SS and found better kyphotic correction in LS.7 Farrokhi et al reported better kyphotic correction, fewer instrument failures, and no additional complications after adding the intermediate screws when compared with SS.10 The stress on the pedicles of LS and SS was approximately 3 to 4 times higher when compared with SI. Thus, using SI may reduce the correction loss and failure rates after operative treatment in patients with thoracolumbar burst fracture. Additionally, several studies have investigated the relationship between bone fracture healing and bone mechanoregulation.25–27 Stresses at the fracture level, which occurred around the pedicles and vertebral body in SI, were higher than those of LS and SS. This phenomenon would potentially aid in bone healing process according to the Wolff law.
According to this study, an operative treatment with SI in a patient with thoracolumbar burst fracture whose McCormack score is <7 would result in a stable fixation with a good spinal range of motion and low correction loss and failure rates. Nonetheless, there were some limitations to this study. First, the study design was a descriptive study. Second, the differences between the models could not be compared significantly. Third, the load applied to the models was a 1-time load that represented a normal physiologic load. The spine would be subjected to a larger and more repetitive load in everyday life than in this study. Furthermore, the sagittal motion of the models was measured after the axial load was applied, and the maximal range of motion of the models was not estimated. Last, this study compared only pedicle screw fixation systems. Other instrument systems and constructs should also be considered and studied. Further research is needed to compare and determine the best treatment for thoracolumbar burst fracture.
Conclusions
Posterior SI preserves more spinal motion than LS. In addition, it provides more favorable biomechanical properties than SS. The stress that occurred around the pedicle screws in SI was the least among the 3 constructs, which might reduce complications such as implant failure. SI produces more stress in the fractured vertebral body than LS and SS, which could potentially aid in bone healing according to the Wolff law.
Acknowledgments
The authors thank Thanachaporn Kittipibul, MD, and the Clinical Research Center at Chulalongkorn University for their support of this study.
Footnotes
Funding This research was financially supported by a grant from the Ratchadapiseksompotch Fund, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand (Grant number RA57/030).
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval The Human Investigation Committee of Faculty of Medicine, Chulalongkorn University Institutional Review Board (IRB) approved this study (IRB number 062/58). Written informed consent was waived.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.