


Abstract
Background We sought to determine which aspect of the upper instrumented vertebrae (UIV)—tilt angle or screw angle—was more strongly associated with: (1) proximal junctional kyphosis/failure (PJK/F), (2) other mechanical complications and reoperations, and (3) patient-reported outcome measures (PROMs).
Methods A single-institution, retrospective cohort study was undertaken for patients undergoing adult spinal deformity (ASD) surgery from 2011 to 2017. Only patients with UIV at T7 or below were included. The primary exposure variables were UIV tilt angle (the angle of the UIV inferior endplate and the horizontal) and UIV screw angle (the angle of the UIV screws and superior endplate). Multivariable logistic regression included age, body mass index, osteopenia/osteoporosis, postoperative sagittal vertical axis, postoperative pelvic-incidence lumbar lordosis mismatch, UIV tilt angle, and UIV screw angle.
Results One hundred and seventeen patients underwent adult spinal deformity surgery with a minimum of 2-year follow-up. A total of 41 patients (35.0%) had PJK and 26 (22.2%) had PJF. (1) UIV tilt angle: 96 (82.1%) had lordotic UIV tilt angles, 6 (5.1%) were neutral, and 15 (12.8%) were kyphotic. (2) UIV screw angle: 38 (32.5%) had cranially directed screws, 4 (3.4%) were neutral, and 75 (64.1%) were caudally directed. Both lordotic-angled UIV endplate (OR = 1.06, 95% CI = 1.01–1.12, and P = 0.020) and cranially directed screws (OR = 1.19, 95% CI = 1.07–1.33, and P < 0.001) were associated with higher odds of PJK, with a more pronounced effect of UIV screw angle compared with UIV tilt angle (Wald test, 9.40 vs 4.42). Similar results were found for PJF. Neither parameter was associated with other mechanical complications, reoperations, or patient-reported outcome measures.
Conclusions UIV screw angle was more strongly associated with development of PJK/F compared with tilt angle. Overall, these modifiable parameters are directly under the surgeon’s control and can mitigate the development of PJK/F.
Clinical Relevance Surgeons may consider selecting a UIV with a neutral or kyphotically directed UIV tilt angle when performing ASD surgery with a UIV in the lower thoracic or lumbar region, as well as use UIV screw angles that are caudally directed, for the purprose of decreasing the risk of developing PJK/F.
Level of Evidence 3.
- Adult spinal deformity
- vertebral tilt angle
- upper instrumented vertebra
- screw angle
- proximal junctional kyphosis
- mechanical complications
- patient-reported outcomes
Introduction
Symptomatic adult spinal deformity (ASD) is a notable cause of morbidity in our aging population.1 The most common mechanical complication following ASD correction is proximal junctional kyphosis (PJK), defined as focal kyphosis of 10° and an increase in kyphosis by 10° 2 levels above the upper instrumented vertebrae (UIV).2 Proximal junctional failure (PJF) is defined as a direct fracture of the UIV or adjacent vertebrae, often requiring reoperation.2 Both PJK and PJF (or PJK/F) can be associated with a neurological deficit. Efforts to limit PJK/F remain at the forefront of research efforts.
Several factors about the UIV may predispose patients to PJK, 2 of which include UIV tilt angle and UIV screw angle. Select studies have demonstrated an association between UIV screw angle and the development of postoperative mechanical complications.3–5 In addition, UIV tilt angle—the angle of the superior endplate of the UIV compared with the horizontal—may also be a risk factor for PJK. In 1 study examining long-construct lumbar fusions, Lewis et al6 demonstrated that a higher UIV tilt angle (a more cranially directed superior endplate) was associated with significantly higher rates of UIV fracture. In another study, Buell et al7 found that a greater UIV tilt angle was associated with PJK in the upper lumbar spine of patients who underwent ASD surgery with subsequent posterior tethering.
To our knowledge, the interplay between UIV tilt angle, UIV screw angle, and PJK/F has not been collectively explored in an ASD cohort. Specifically, prior literature lacks concrete evidence and validation of the association between UIV tilt angle or UIV screw angle with PJK/F. In a cohort of patients undergoing ASD surgery with a UIV in the lower thoracic or lumbar spine, we sought to determine which aspect of the UIV—the UIV tilt angle or UIV screw angle—was more strongly associated with (1) PJK/F, (2) other types of mechanical complications and reoperation, and (3) patient-reported outcome measures (PROMs).
Methods
Study Design
A single-institution, retrospective cohort study was undertaken between 2011 and 2017. Three full-time employees completed clinical data collection, whose roles included contacting patients to collect pre- and postoperative PROMs. A total of 5 fellowship-trained neurosurgery and orthopedic spine surgeons contributed to all ASD cases. The Vanderbilt University Medical Center Institutional Review Board (IRB) approval was obtained (IRB#211290). A signed consent for participation was collected from all study participants.
Patient Population
Inclusion criteria were as follows: age ≥18 years, elective surgery, ≥5-level fusions, Cobb angle ≥30°, sagittal vertical axis (SVA) ≥5 cm, coronal vertical axis (CVA) ≥3 cm, pelvic tilt of ≥25°, and thoracic kyphosis ≥60°. Only patients with UIV at T7 or below, in the lower thoracic or lumbar region, were included. Given that the vertebral tilt in the upper and lower thoracic vertebrae may vary substantially, we sought to homogenize our sample by only including patients with a UIV in the upper lumbar or lower thoracic spine. Rates of PJK/F are considerably lower in patients with a UIV in the upper thoracic spine,8 and an a-priori agreement was reached by all senior authors that fusions to the upper thoracic spine would be excluded. In keeping with prior literature, UIV screw angle was mainly investigated in the thoracolumbar spine.1 Therefore, an agreement of keeping the analysis to the thoracolumbar UIV to keep a homogeneous population was reached among the senior authors. Moreover, all patients had a minimum of 2-year follow-up available as defined by the last office visit.
Exposure Variables
The 2 principal exposure variables were (1) UIV tilt angle and (2) UIV screw angle relative to the superior endplate. All measurements were taken from the first postoperative lateral radiographs. The UIV tilt angle was measured as described by Lewis et al6 and was defined as the angle created by the inferior endplate of the UIV with the horizontal line of the film (Figure 1). UIV tilt angles were classified as positive, negative, or neutral. Positive angles constituted lordotic angles, pointed cranially, while negative angles constituted kyphotic angles, pointed caudally. An angle of 0° ± 2° was considered neutral and parallel to the horizontal according to prior literature.1

Illustration of positive (A), neural (B), and negative (C) upper instrumented vertebrae (UIV) tilt angle.
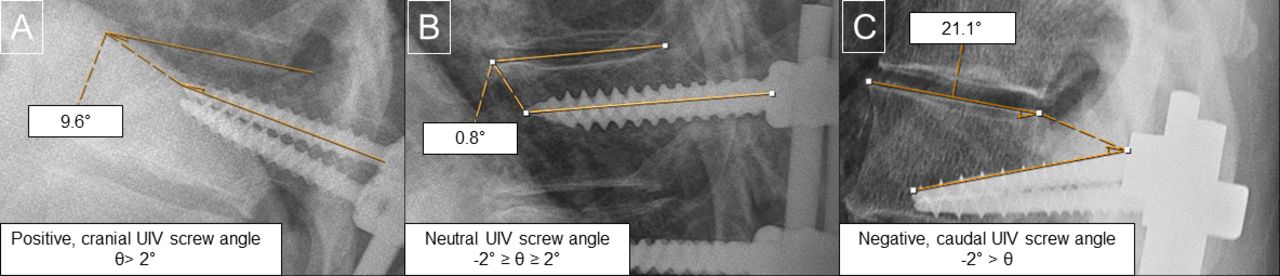
UIV screw angle was measured in a similar fashion as reported by Harris et al5 and was defined by the angle formed by the screw shaft and the superior vertebral endplate (Figure 2). A cranially directed screw angle (θ > 2°) toward the UIV superior endplate was considered positive (“+”), while a caudally directed screw (−2° > θ) away from the UIV superior endplate was considered negative (“–”). A neutral angle of –2° ≥ θ ≥ 2° was defined as parallel to the superior endplate within 2° according to prior literature.1 For patients with divergent screws, 1 positive and 1 negative UIV screw angle (n = 23), as stated above, the mean screw angle was used.

Illustration of positive (A), neural (B), and negative (C) upper instrumented vertebrae (UIV) screw angle.
Outcome Variables
The primary outcome was the development of PJK/F. PJK was defined as an angle between the UIV inferior endplate and UIV + 2 superior endplate ≥10° and a concomitant ≥10° change compared with preoperative imaging, in keeping with prior literature.1 All outcomes were evaluated with a minimum of 2-year follow-up.
Secondary outcomes included other types of mechanical complications, reoperation, and 2-year PROMs. Mechanical complications included rod fracture, pseudarthrosis, distal junctional kyphosis (DJK), and implant failure. PROMs included Oswestry Disability Index (ODI), Numeric Rating Scale (NRS) Back/Leg, and EQ-5D. DJK was defined as ≥10° increase in kyphosis between the lowest instrumented vertebra (LIV) and LIV-1 on postoperative radiographs. Rod fracture was defined as the presence of single or double rod breakage on the postoperative radiograph. Implant failure included screw pullout, fracture, loosening, or dislodgment.
Statistical Analysis
Descriptive statistics were reported for patient demographics, pre- and postoperative characteristics, and radiographic measurements. Mean and SD for continuous variables and frequency for categorical variables were calculated. UIV tilt angle and UIV screw angle were treated as continuous variables. Due to the overlapping nature of patients with pseudarthrosis and rod fracture, this group was analyzed as 1 group. Minimal clinically important difference (MCID) was calculated for PROMs and was set at 30% improvement at 2 years postoperatively.1 UIV tilt angle and UIV screw angle were compared using both Student’s t test and χ 2 between patients with and without PJK. Univariable and multivariable logistic regression was then performed with the primary outcome of PJK/F. Multivariable regression included only 1 consistent model to assess the impact of UIV tilt angle and UIV screw angle with outcomes. The only logistic regression model that was performed in our analysis consisted of the following variables: age, body mass index, the presence of osteopenia/osteoporosis, postoperative SVA, postoperative pelvic incidence lumbar lordosis mismatch, UIV tilt angle, and UIV screw angle. The difference between Wald statistics and the degree of freedom was calculated to compare the association between UIV tilt angle and UIV screw angle with outcome variables to determine which exposure variable was more strongly associated with the outcome. The Wald statistic is a versatile way to test whether explanatory variables in a model are significant and to compare the significance among the independent variables.9 Since P values alone do not represent the effect size, we chose the Wald statistic and degree of freedom as a way to compare significance among the exposure variables. Furthermore, the P value does take into consideration the measure of uncertainty in statistical inference. The Wald statistics is a commonly used method for hypothesis testing in regression analysis and other statistical models. In other words, the Wald statistics assess the significance of the estimated parameter by comparing it to its estimated SE, which is a measure of uncertainty associated with the coefficient estimate.9 The Wald statistics were deemed particularly useful for assessing the relative importance of the independent variables when the odds ratios and confidence intervals were similar, as they can help distinguish between variables that might otherwise appear closely associated. A larger Wald statistic indicates a stronger relationship between the independent variable and the dependent variable.10 Statistical significance was considered at an alpha level of <0.05. All analyses were performed using R version 4.1.3 (The R Foundation, Vienna, Austria).
Results
Patient Demographics
During the study period, 117 patients underwent ASD surgery with a UIV at T7 or below. An additional 153 patients underwent ASD surgery but did not have a complete follow-up to the 2-year mark and were subsequently excluded from the analysis. Among the 117 included patients, the mean age was 65.6 ± 9.2 and the mean number of instrumented levels was 8.9 ± 1.7. A total of 111 (94.9%) patients had constructs that extended to the sacrum. Full demographics of the ASD cohort are present in Table 1.
Demographics, operative variables, radiographic measurements, and PROMs of the total cohort.
UIV Tilt Angle and UIV Screw Angle
Regarding UIV tilt angle, 96 (82.1%) had lordotic endplate angles, 6 (5.1%) had neutral endplate angles, and 15 (12.8%) had kyphotic endplate angles. Regarding the UIV screw angle, 38 (32.5%) had positive (cranially directed) screws, 4 (3.4%) had neutral screws, and 75 (64.1%) had negative (caudally directed) screws. The mean UIV tilt angle was 12.9° ± 13.6°, while the mean UIV screw angle was –3.2° ± 8.0°. The distribution of mean UIV tilt angle and mean UIV screw angle is shown in Figure 3.

Distribution of upper instrumented vertebrae (UIV) tilt angle (A) and UIV screw angle (B). Abbreviation: IQR, interquartile range.
PPJK/F
Overall, 70 (59.8%) patients had a mechanical complication, and 54 (46.2%) patients required reoperation. A total of 41 (35.0%) patients had PJK and 26 (22.2%) had PJF. The summary of outcome variables is presented in Table 2.
Summary of outcome variables.
In bivariate comparison testing, the UIV tilt angle was not significantly different between patients with and without PJK (13.6° ± 14.1° vs 12.5° ± 13.4°, P = 0.689). When treated as a categorical variable, PJK was not significantly different in patients with kyphotic vs lordotic UIV tilt angle (36.9% vs 28.0%, P = 0.405). UIV screw angles for patients with PJK and without PJK were significantly different (–0.4° ± 7.9° vs –4.7° ± 7.7°, P = 0.005). Of patients with positive, cranially directed screws, 53.1% had PJK, whereas in patients with neutral/negative (caudally directed) screws, 28.2% had PJK (P = 0.012; Table 3).
Comparison of the UIV tilt angle and UIV screw angle in patients with and without proximal junctional kyphosis.
Multivariable logistic regression analysis controlling for age, body mass index, osteopenia/osteoporosis, postoperative SVA, postoperative pelvic incidence lumbar lordosis, UIV tilt angle, and UIV screw angle found that lordotic UIV angles were associated with higher odds of PJK (OR = 1.06, 95% CI = 1.01–1.12, P = 0.020), and positive, cranially directed screws were also associated with higher odds of PJK (OR = 1.19, 95% CI = 1.07–1.33, P < 0.001). An evaluation of the predictor importance (Wald-df) indicated that the UIV screw angle was a stronger predictor of PJK than the UIV tilt angle (Wald test, 9.40 vs 4.42) when controlling for the aforementioned covariates, with a lower P value in the UIV screw angle compared with UIV tilt angle when predicting PJK (P < 0.001 vs P = 0.020). Figure 4 represents the distribution of UIV tilt angles and UIV screw angles associated with PJK compared with patients without PJK. Similarly, UIV angles were associated with significant increased odds of PJF (OR = 1.06, 95% CI = 1.01–1.12, P = 0.049), and positive, cranially directed screws were associated with higher PJF (OR = 1.14, 95% CI = 1.02–1.27, P = 0.013). An evaluation of the predictor importance (Wald-df) indicated that the UIV screw angle was a stronger predictor of PJF as compared with the UIV tilt angle (Wald -df, 5.13 vs 2.86) when controlling for the aforementioned covariates.

Distribution of upper instrumented vertebrae (UIV) tilt angle (A) and UIV screw angle (B) with proximal junctional kyphosis (PJK) occurrence.
Remaining Mechanical Complications, Reoperation, and PROMs
The overall prevalence of remaining types of mechanical complications (ie, not including PJK/F) was not significantly different between cohorts. Neither univariable nor multivariable analyses found significant associations between positive UIV tilt or UIV screw angles and overall mechanical complications, rod failure, pseudarthrosis, implant failure, or reoperations (Table 4). DJK was not included in the univariable and multivariable regression as it only occurred in 1 patient.
Univariate and multivariable logistic regression predicting PJK. Multivariable regression model included age, body mass index, osteopenia/osteoporosis, postoperative sagittal vertical axis, postoperative pelvic incidence lumbar lordosis, UIV tilt angle, and UIV screw angle.
Postoperative PROMs of ODI, NRS-Back, and NRS-Leg are presented in Table 2. A multivariable logistic regression controlling for the aforementioned variables showed no significant associations between UIV tilt angle and UIV screw angle with MCID ODI, MCID NRS-Back, and MCID NRS-Leg (Table 4).
Discussion
The current study analyzed the impact of UIV tilt angle and UIV screw angle on PJK/F in ASD patients with a UIV in the lower thoracic or lumbar region. When controlling for several confounding variables associated with PJK/F, lordotically angled UIVs were significantly associated with increased odds of PJK/F. Furthermore, cranially directed UIV screws were associated with increased odds of PJK/F. Comparing the 2, it appeared that the UIV screw angle was the stronger predictor of PJK/F than the UIV tilt angle. Conversely, neither variable demonstrated a significant relationship with the remaining types of mechanical complications or with PROMs.
UIV tilt angle and the development of mechanical complications have been less rigorously studied than pedicle screw placement/angle. A recent study of 190 patients undergoing ASD surgery found that PJK occurred more frequently in patients with a higher postoperative UIV slope, but this association was not significant on regression analysis.11 However, the authors did not control for the UIV screw angle, which showed a significant association with PJK in previous literature. Lafage et al12 found that posterior construct inclination, or more lordotically angled UIV endplates, were present more often in patients who developed PJK. However, neither of these studies accounted for screw angle when assessing UIV tilt. Our data suggest that more lordotically angled UIVs in the thoracolumbar spine are associated with increased odds of PJK/F, which was present when controlling for other factors, including the UIV screw angle. However, UIV tilt angle proved to be the less important variable in predicting PJK/F than UIV screw angle.
UIV screw angle was more strongly associated with the development of PJK/F than the UIV tilt angle in the current analysis. Specifically, cranially directed UIV screw angles were associated with increased odds of the development of PJK/F. Several potential reasons exist as to why UIV screw angle was the more important factor to UIV tilt angle. A screw that compromises the integrity of the unfused facet joint or violates the superior endplate may accelerate the degeneration process and lead to the development of PJK/F. In contrast, a perfectly placed screw, parallel to the superior endplate or slightly caudally directed, in an otherwise lordotic UIV, may have a lower chance of failure. Our findings are in line with at least 2 previous studies. Harris et al5 found that UIV pedicle screws angled ≥3° cranially had significantly greater odds of developing PJK and PJF, compared with those with screws angled <3° cranially. Similarly, Jung et al13 found that straightforward screws at the thoracolumbar junction were protective against PJK (straightforward screws are functionally caudally angled due to the natural lordotic curvature of the thoracolumbar junction). Although we produced similar findings, our study offered a larger cohort (117 vs 96 and 83 patients) and provided insight into the importance of the relationship between UIV screw and tilt angles. Importantly, our study focused on ASD fusions to the lower thoracic or upper lumbar spine, which represents a different population that fusions to the upper thoracic spine. Furthermore, our study found that UIV screw angle was neither associated with any additional varieties of mechanical complications nor was it predictive of differences in PROMs, an assessment that has not been conducted in the existing literature.
While the current study cannot explain causation, several potential theories may explain our findings. In terms of the UIV angle, a lordotic UIV tilt angle may predispose one to PJK/F due to excessive spinal realignment during ASD surgery, causing undue force on the construct. Conversely, a UIV angle in line with the horizontal may allow for more flexibility at the top end of the construct and may reduce exogenous forces that predispose one to adjacent segment degeneration. According to the Roussouly classification,14 if the lower arc of spinal kyphosis is too pronounced, the unfused spine may have to compensate with more kyphosis, thus precipitating PJK/F. Regarding UIV screw angle, more cranially directed UIV screw angles may be associated with increased odds of PJK/F secondary to multiple factors. First, as constructs settle and patients become more active after surgery, cranially directed screws may disrupt the suprajacent disc space/endplate. Even if the screws do not violate the disc space, as cranially directed screws approach the endplate, they may begin to erode the bone abutting the endplate, thus decreasing cortical purchase and predisposing to mechanical complications. It is also possible that caudally directed screws are placed in a different vector than the vector in which screws are most biomechanically predisposed to pullout. By being placed in a more downward direction, not in line with the easiest method of loosening and failure, caudally directed screws may protect against a more horizontal pullout force. Finally, the more cranially directed screws may provide a greater pullout strength, as has been suggested in prior biomechanical studies,3,4 and may in turn make the construct more stiff than is optimal and may hasten adjacent segment degeneration.
The development of, and therefore the prevention of, PJK/F itself is likely multifactorial. Other factors have been studied that may contribute to the development of PJK/F such as bone density, the use of adjuncts such as cement, hooks, or tethers, and selection of the UIV.3,4,7,15,16 These factors should also be carefully considered alongside UIV parameters. As UIV tilt angle and UIV screw angle are modifiable factors under the surgeon’s control, taken together they may be a useful tool to help mitigate the development of this complication. The surgeon should select a UIV level that is neutral when possible and ensure screws placed at the UIV are neutrally or caudally directed in order to minimize the risk of developing PJK/F. Nevertheless, the potential clinical implications should be exercised with caution, given that the current study was not designed to establish causality between these parameters and PJK/F. Future prospective studies should further investigate the causal relationships by including a control group to rigorously assess the impact of UIV tilt angle and UIV screw angle on the occurrence of PJK/F while controlling for potential confounding factors, thereby providing more robust evidence for clinical decision-making.
This study recognizes its limitations. First, a retrospective analysis of prospective data within a single institution has inherent limitations as some information might be lost. Prospective multicenter studies are encouraged to control for bias and increase generalizability. In addition, while we used Wald statistics and degree of freedom to compare the impact of tilt angle and screw angle on patient outcomes, the significant association does not imply causation due to the inherent limitations of a retrospective study with a small sample size. Retrospective studies pose significant limitations of the statistical analysis, making it challenging to confidently determine the association between UIV tilt angle and UIV screw angle with outcomes. Second, UIV tilt angle can be modified by patient position, and minor variation may occur during positioning for imaging, which may in turn affect study results. Third, factors such as screw length, screw-entry location, or endplate violation may affect the development of PJK/F and were not considered in this study. Fourth, a limited sample size may reduce the generalizability of the conclusions drawn, and further studies including larger cohorts should validate these findings. More than half of the total cohort were lost to follow-up and subsequently excluded from the analysis, which may further limit the generalizability of our analysis. However, given that these patients were from the same institution, it is likely that their exclusion would not substantially impact the overall findings and conclusions of our study. Fifth, the choice of the UIV between T7-L2 may have increased the heterogeneity of our patients sample due to the inherent difference in thoracic kyphosis, inflection point, and lumbar lordosis. Sixth, while we adopted the radiographic diagnosis of PJK,17 a consensus regarding the diagnosis of PJK remains poorly established. A normal reciprocal change in kyphosis angle due to the correction of hypolordosis of the lumbar spine may sometimes be mistaken with PJK, which may have overestimated our findings. A growing body of literature indicates that the classic definition of PJK may be inappropriately low.18 Seventh, since prior literature has shown that pelvic instrumentation may not directly impact the risk of PJK/F,19 we opted to include patients with and without pelvic extension of the arthrodesis. On the other hand, one of the major drawbacks of spinal deformity studies is that mechanical complications are multifactorial processes, and not all cofactors can be consistently accounted for. Even though we have accounted for multiple covariates, confounding bias may still exist due to the inherent limitation of retrospective studies and the multifactorial nature of mechanical complications. Finally, the mechanical complication rates were higher than previously reported in the literature, which may be due to the registry including operations from more than a decade ago, when techniques and knowledge of ASD surgery were evolving. It is likely that these complication rates do not reflect the current practice at our institution among the 4 fellowship-trained spine surgeons doing ASD surgery. However, we still found meaning in reporting our institution’s data to investigate the impact of UIV tilt angle and UIV screw angle on patient outcomes. Subsequently, it is important to mention that our current practice consists of optimizing bone mineral density preoperatively through anabolic prescriptions prior to proceeding with the surgery to mitigate the risk imposed by osteoporosis on postoperative outcomes, which we have controlled for in our regression analysis. Furthermore, ways to prevent PJK/F are currently being used, including surgical cements and adjunct devices, such as hooks and tethers. We also routinely incorporate spinal alignment principles as described by Roussouly, which has reinforced the importance of low lordosis and different spinal shapes dictated by pelvic incidence and sacral slope.
Conclusion
In ASD fusions with a UIV in the lower thoracic or lumbar region, both lordotically angled UIV endplates and cranially directed UIV screws were associated with higher odds of PJK/F. Although we had a high dropout rate, the UIV screw angle appeared to be more strongly associated with the development of PJK/F, with a lesser contribution from the UIV tilt angle. The potential clinical implications should be approached cautiously given the multifactorial nature of PJK/F. When performing ASD surgery with a UIV in the lower thoracic or lumbar region, surgeons may consider selecting a UIV with a neutral or kyphotically directed UIV tilt angle, as well as use UIV screw angles that are caudally directed to help minimize the risk of developing PJK/F. Further research, including prospective studies with control groups, is needed to provide more robust evidence for these surgical decisions.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Dr. Zuckerman reports being an unaffiliated neurotrauma consultant for the National Football League and consultant for Medtronic. Dr. Stephens is a consultant for Nuvasive and Carbofix and receives institutional research support from Nuvasive and Stryker Spine. Dr. Abtahi received an institutional research support from Stryker Spine. No other perceived conflict of interest by any of the listed authors.
Ethics Approval Statement This study was approved by the IRB committee at Vanderbilt University Medical Center (IRB#211290). We certify that the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.