


Abstract
Background An abnormal postoperative lordosis distribution index (LDI), which quantifies the ratio between the lordosis at L4 to S1 and the lordosis at L1 to S1, contributes to the development of adjacent segment disease and increased revision rates in patients undergoing short-segment lumbar intervertebral fusions. Incorporating preoperative spinopelvic parameters and LDI into the surgical plan for short-segment fusion is important for guiding alignment restoration and preserving normal preoperative alignment in unfused segments. This study examined changes in LDI, segmental lordosis, and lordosis of the unfused levels in patients treated with personalized interbody cage (PIC) implants.
Methods This retrospective study evaluated radiographic measurements from 111 consecutively treated patients diagnosed with degenerative spinal conditions and treated with a short-segment fusion of L4 to L5, L5 to S1, or L4 to S1 using PIC implant(s) within 6 months of the fusion procedure. Comparisons of intervertebral lordosis for treated and untreated levels as well as LDI pre- and postoperatively were performed.
Results In patients with a preoperative hypolordotic distribution (LDI < 50%), statistically significant increases were found in LDI postoperatively, approaching the normal LDI range (LDI 50%–80%). Likewise, patients with hyperlordotic distribution preoperatively (LDI > 80%) experienced a decrease in LDI postoperatively, trending toward the normal range, although the changes were not statistically significant. Intervertebral lordosis for the L5 to S1 level increased significantly following the placement of a PIC in the normal and hypolordotic LDI groups. Changes in intervertebral lordosis for L5 to S1 were not significant for patients with preoperative hyperlordotic LDI. Reciprocal changes in intervertebral lordosis at L1 to L4 were not observed in any groups.
Conclusions PIC implants may provide a benefit for patients, particularly those with hypolordotic distributions preoperatively. They have the potential to further improve patient outcomes by helping surgeons to achieve patient-specific lordosis goals, which may help to reduce the risk of adjacent segment disease and revisions in patients undergoing short-segment lumbar intervertebral fusions.
Clinical Relevance Personalized implants can help surgeons achieve patient-specific alignment goals, potentially prevent adjacent segment disease, and reduce long-term reinterventions.
Level of Evidence 4.
- lumbar fusion
- lordosis
- personalized interbody cage
- LDI
- reciprocal changes
- adjacent segment disease
- short segment fusion
- preoperative planning
Introduction
Short-segment fusion of L4 to L5, L5 to S1, or L4 to S1 is 1 of the most commonly performed surgical procedures to address lumbar degenerative spinal diseases unresponsive to nonoperative treatment or decompression surgeries.1–3 The number of patients with persistent spinal malalignment after lumbar interbody fusion for degenerative spinal conditions is high.4,5 This persistent malalignment has been shown to increase the biomechanical load in the adjacent vertebral levels,6–8 leading to adjacent segment disease (ASD),9–11 which can increase the rate of revision surgery.12–14 Several factors have been described as predictive for postoperative ASD, including preoperative degenerative conditions at the adjacent levels, changes in spinal pelvic parameters, and the impact of certain segmental and lordosis distribution changes.9,11,14–17
Proper postoperative alignment of the segments involved in the fusion is associated with positive long-term outcomes and can minimize complications since it can directly impact segmental lordosis and the lordosis distribution index (LDI), which quantifies the ratio between the L4 to S1 lordosis and L1 to S1 lordosis.5,18–20 A poor postoperative LDI, 1 that is either hyperlordotic (>80%) or hypolordotic (<50%), in combination with a high difference between pelvic incidence and lumbar lordosis (PI−LL) mismatch, has been associated with higher revision rates following short-segment fusion.12–14 While stock fusion cages are available in a wide range of lordotic angles, there is a poor correlation between the wedge angles of the implants used and the resulting lordosis of the fused intervertebral segment.21–25 This poor correlation may be attributable to the fit between the irregular bony contours of the vertebral endplate and the uniform surface of a stock interbody device, which can interfere with achieving an optimal fit and potentially alter alignment.26
Designed to match the patient’s endplate anatomy, personalized interbody cages (PICs) aim to provide a more predictable alignment dictated by a surgical plan for foraminal height, coronal correction, and intervertebral lordosis (IVL). Matching the device surfaces to the unique morphology of each patient’s vertebral endplates aids in achieving the desired alignment.27
While the design of a PIC focuses on the proper alignment of the level being fused, subsequent changes in IVL of the untreated levels and in LDI can occur. This study examined changes in LDI, segmental lordosis, and lordosis of the unfused levels in patients treated with a PIC.
Methods
Study Design and Patient Population
This study is a retrospective comparison of pre- and postoperative radiographs from consecutively treated adult patients with degenerative spinal conditions who underwent short-segment lumbar interbody fusion including placement of a 3D-printed PIC in at least 1 of the levels treated. Personalized implants were manufactured for each patient by first creating a 3D model of planned correction based on computed tomographic imaging of the affected spine. Surgical planning for the 3D model incorporated the IVL angle, intervertebral coronal angle, posterior disc height, and global and lower lumbar lordosis (LLL) as determined by the surgeon for each patient. Single- or 2-level procedures were performed using an anterior lumbar interbody fusion, lateral lumbar interbody fusion, or transforaminal lumbar interbody fusion approach at L4 to L5, L5 to S1, or L4 to S1. None of the cases in this study were performed specifically to address nondegenerative conditions such as complex spinal deformity, tumor, or trauma.
Inclusion criteria were as follows: patients treated with de novo or revision fusion of L4 to L5, L5 to S1, or L4 to S1; implantation of PIC devices in 1 or both levels using an anterior lumbar interbody fusion, lateral lumbar interbody fusion, or transforaminal lumbar interbody fusion surgical approach; and standing radiographs of either the full spine or at least T12 to the femoral head taken within 6 months of the surgery date. Patients undergoing revision surgery were included only in cases where the final upper instrumented level was at L4 or L5, and the final lower instrumented level was S1; those with any instrumented level above L4 were excluded. All patients had supplemental posterior instrumentation.
Data Collection and Assessment
Full-length or lumbar spine standing anteroposterior and lateral radiographs were obtained for all patients pre- and postoperatively within 6 months of the surgery date. Radiographs were measured by an independent radiologist and an independent spine surgeon using validated DICOM viewer software (Microdicom, Microdicom Ltd, Sofia, Bulgaria). An adjudication process was performed in case of discrepancy in the measurements beyond 5°, leading to the final measurement agreement of that specific parameter. In case a radiological landmark for a certain parameter was determined to be insufficiently visible by 1 of the observers—due to poor image quality, severe obliquity, or interference caused by implant artifacts—that parameter was marked as not measurable.
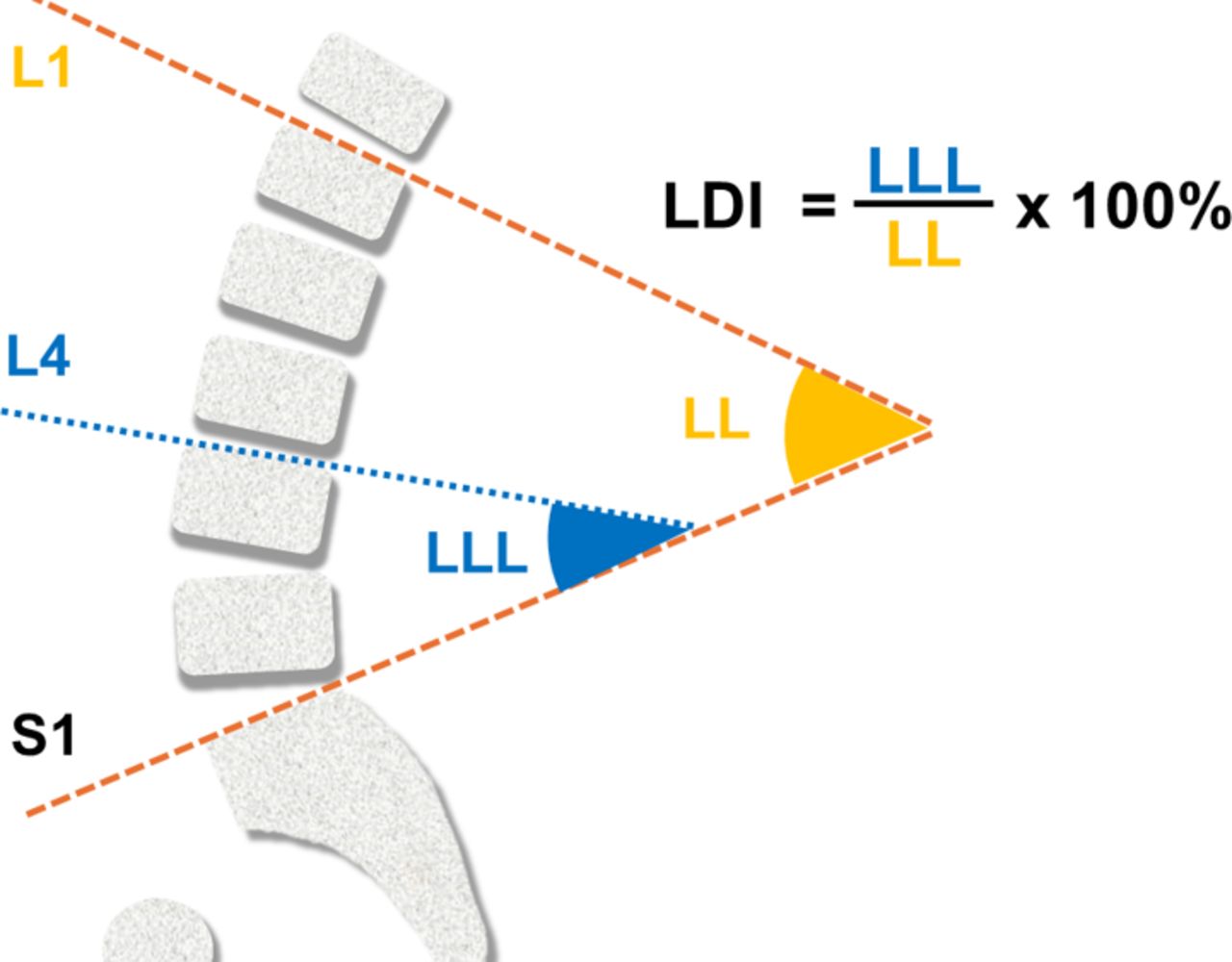
Radiographs were measured for spinopelvic parameters, including global lumbar lordosis (LL); pelvic incidence (PI); PI−LL; LLL; and LDI. Related to the lumbar spine segments, measurements were obtained at each level for IVL, defined as the angle formed between the lower endplate of the superior vertebra and the upper endplate of the inferior vertebra for each level (Figure 1). LL was measured from the upper endplate of L1 to the upper endplate of S1. PI was measured as the angle between the line perpendicular to the sacral plate at its midpoint and the line connecting this point to the femoral head axis. LLL was defined as the magnitude of lower-arc lordosis (upper endplate of L4–S1). LDI was calculated as the ratio between the lower arc (LLL) and global LL as shown in Figure 2.

Intervertebral lordosis (IVL) measurements.

Definition of lordosis distribution index (LDI). Abbreviations: LL, lumbar lordosis; LLL, lower lumbar lordosis
Patients were subcategorized according to their preoperative LDI as: normal (LDI 50%–80%), hypolordotic distribution (LDI < 50%), or hyperlordotic distribution (LDI > 80%).17 Figure 3 provides a graphical representation of the various lordosis categories.

Lordosis categories. Abbreviations: LDI, lordosis distribution index.
Statistical Methods
Statistical analysis was performed using SPSS version 29.0.2.0. Descriptive statistics were reported as mean ± SD for continuous variables and frequencies with percentages for categorical variables for the group as a whole as well as grouped by their preoperative LDI category and their postoperative measurements. Pre- and postoperative continuous variable data were compared using Student paired t test. All tests were 2-tailed, with a significance level (α) of 0.05.
Results
A total of 111 patients met the inclusion criteria with surgeries performed for degenerative spinal conditions. Single-level fusion with a single PIC implant was performed in 72 cases: 27 patients at L4 to L5 and 45 patients at L5 to S1. For the 39 cases of 2-level fusion from L4 to S1, 24 patients received 2 PIC implants, and 15 patients had only 1 PIC implant at either L4 to L5 or L5to S1. Patients with only 1 PIC implanted received posterior instrumentation and posterior lumbar fusion at the non-PIC level. Detailed patient demographics and operative parameters are provided in Table 1.
Baseline demographics and operative parameters.
Sagittal Radiographic Parameters
In the overall analysis, preoperative PI was 57° ± 13°, and LL was 51° ± 12°, leading to a PI−LL of 6° ± 11°. Postoperative LL was 55° ± 13°, an increase of 3° (P < 0.001) with a decrease of the PI−LL to 4° ± 11° (P = 0.003) (Tables 2 and 3).
Radiographic spinopelvic measurements.
Calculated lumbar parameters.
LDI and Sagittal Parameters
Preoperatively, 73% (81 out of 111) of patients fell into the normal lordotic distribution group (LDI 50%–80%); 13% (14 out of 116) were in the hypolordotic distribution group (LDI < 50%); and 14% (16 out of 111) were classified in the hyperlordotic distribution group (LDI > 80%; Table 4).
Patient LDI pre- and postoperatively (N = 111).
The normal LDI group had a preoperative LLL of 34° ± 8°, LL of 53° ± 12°, PI of 57° ± 12°, and PI−LL of 4° ± 10°. Postoperative LLL increased to 37° ± 10° (Δ = +3.5°, P < 0.001), LL increased to 56° ± 13° (Δ = +2.7°, P < 0.001), PI increased to 58° ± 12° (Δ = +1.3°, P = 0.002), and PI−LL decreased to 2° ± 10° (Δ = −1.5°, P < 0.001). The hypolordotic distribution group presented a preoperative LLL angle of 19° ± 7°, LL of 50° ± 8°, a PI of 64° ± 12°, and PI−LL of 13° ± 12°. Postoperative LLL angle increased to 27° ± 7° (Δ = +7.6°, P = 0.009), LL increased to 59° ± 5° (Δ = +8.2°, P = 0.011), and PI−LL decreased to 6° ± 13° (Δ = −7.6°, P = 0.031); there was no statistically significant change in PI for this group. The hyperlordotic distribution group presented a preoperative LLL angle of 38° ± 7°, LL of 42° ± 10°, a PI of 54° ± 13°, and PI−LL of 12° ± 10°. Mean values for postoperative LLL angle decreased to 36° ± 9° (Δ = −1.6°, P = 0.404), LL increased to 44° ± 9° (Δ = +1.8°, P = 0.230), and PI−LL decreased to 10° ± 13° (Δ = −2.2°, P = 0.241), although none of these changes were statistically significant (Tables 2 and 3).
Postoperative Changes in LDI
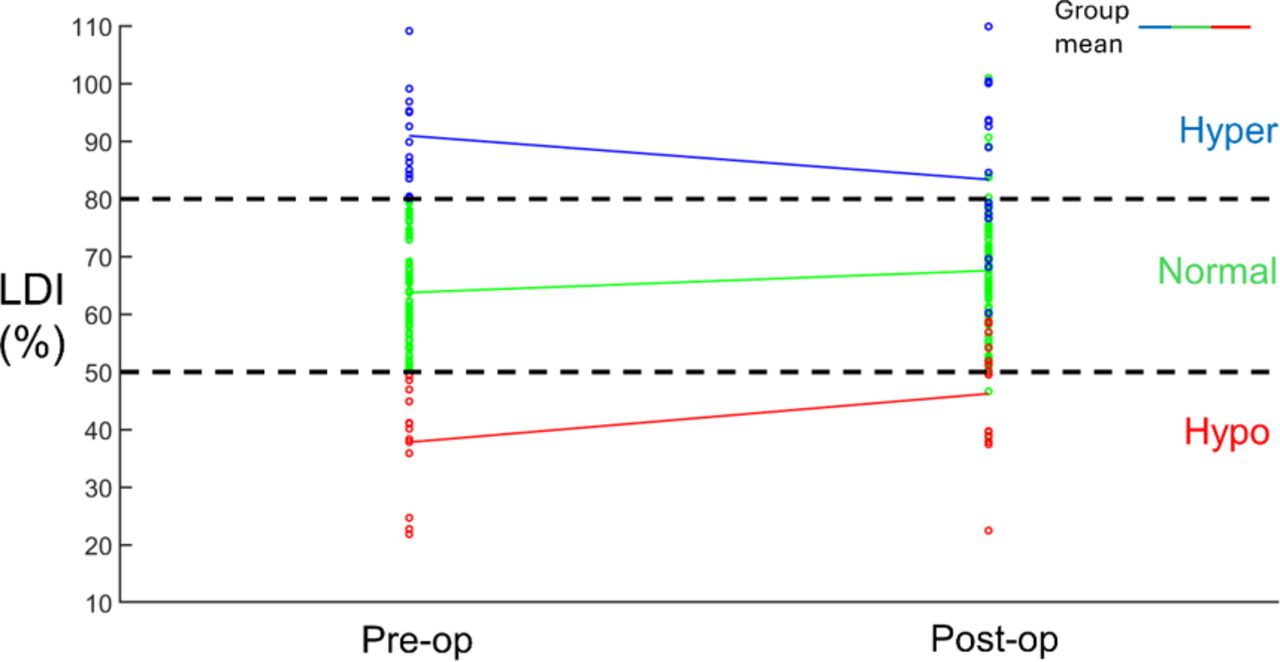
As represented in Figure 4, the mean LDI for the patients in the normal distribution group remained in the normal range postoperatively (preoperative LDI = 64% ± 8%, postoperative LDI = 68% ± 13%, P = 0.010). In contrast, the mean LDI for patients in the abnormal groups, hypolordotic and hyperlordotic, approached the normal range postoperatively. In patients with a hypolordotic distribution (LDI < 50%), statistically significant increases were found in LDI postoperatively, approaching the normal LDI range (LDI 50%–80%). Patients with hyperlordotic distribution preoperatively (LDI > 80%) experienced a decrease in LDI postoperatively, trending toward the normal range, although the changes were not statistically significant (hypolordotic: preoperative LDI = 38% ± 9%, postoperative LDI = 46% ± 10%, P = 0.030; hyperlordotic: preoperative LDI = 91% ± 8%, postoperative LDI = 83% ± 15%, P = 0.092).

Lordosis distribution index (LDI) pre- and postoperative comparisons for each patient color coded into different preoperative distribution groups.
Following fusion surgery, the LDI for some patients increased or decreased enough to fall into a different lordosis distribution category. The number of patients in each group having an LDI that fell in the range for a different LDI category postoperatively is provided in Table 4. For the normal group, 68 of the 81 patients maintained a normal LDI, while the remaining 13 had a postoperative LDI that fell into an abnormal range. Half of the 16 patients in the hyperlordotic group and 6 of the 14 patients in the hypolordotic group improved to an LDI in the normal range following the placement of a PIC implant.
Segmental Parameters
IVL measurements obtained pre and postoperatively are presented in Table 5. The IVL increased significantly at L5 to S1 for all patients combined and for the normal and hypolordotic groups following the placement of a PIC implant, while the other nonoperated lumbar levels did not exhibit significant changes in IVL compared with the preoperative lordosis angle in the same LDI group. There were no significant changes in IVL at any lumbar level for the hyperlordotic group pre- to postoperatively.
Radiographic intervertebral measurements.
A bar plot showing preoperative (left) and postoperative (right) average IVL values for L1 through L5 is provided in Figure 5a. The bar plot in Figure 5b correlates the IVL related to the overall LL, and it reflects the IVL/LL ratio. Patients are grouped into normal, hyperlordotic, and hypolordotic preoperative LDI.

(A) Intervertebral lordosis (IVL) distribution in the lumbar region. (B) The ratio of IVL to lumbar lordosis (LL) distribution in the lumbar region.
Discussion
Importance of Planning for Short-Segment Fusion
Understanding the natural lordosis distribution in the lumbar spine is important in preoperative planning for optimal restoration of spinal alignment during interbody fusion surgery. The significance of planning sagittal alignment in short-segment fusion for degenerative spinal diseases is increasingly recognized.27,28 Improved preoperative identification of ASD risk factors in individual patients and enhanced alignment planning17 will enable surgical strategies to minimize those risks. This, in turn, may reduce ASD occurrences and revision surgeries, fostering improved long-term outcomes. To improve planning, multiple previous studies have noted the importance of combining spinopelvic parameters with LDI and other parameters.14,16,28 Yilgor et al suggested that the use of LDI together with relative LL (measured minus ideal LL), instead of PI−LL for surgical planning, may result in better long-term health-related quality of life results with lower mechanical complication rates.17 The present study focused on the use of PIC in the lower lumber spine and aimed to analyze the changes in intervertebral and segmental lordosis from LLL, the resulting LDI changes, and reciprocal changes at the untreated lumbar levels, possibly helping to better inform surgical planning in short segment fusions.
Similar to a previous study by Bari et al that analyzed postoperative changes associated with LDI in short-segment fusions using stock implants for the treatment of lumbar degenerative diseases, the preoperative LL, on average, was in the normal range 52° ± 12°.14 However, in contrast to the findings of Bari et al, which documented a decrease of 4° in postoperative lordosis and an increase of 3° in PI−LL to 7.4° ± 13°, our findings showed a small but statistically significant increase in the postoperative lordosis to 55° ± 13° (P < 0.001) and a reduction of 2° in PI−LL to 3.7° ± 11° (P = 0.003; Tables 2 and 3). In addition, while Bari et al found a decrease of 6° in postoperative lordosis and an increase of 4° in PI−LL to 16.1° ± 17° for the hypolordotic LDI group, our findings showed a statistically significant increase in the postoperative lordosis of 8° to 59° ± 5° (P = 0.011) and a reduction of 7.5° in PI−LL to 6.2° ± 13° (P = 0.031; Tables 2 and 3).
Changes in Lordosis Distribution
Studies have shown that abnormal postoperative LDI is common in patients exhibiting ASD and is associated with increased revision rates.14,16,20,29 Examining changes in LDI within the normal lordotic distribution groups among patients having short-segment fusions have shown a substantial number of patients having an abnormal LDI postoperatively.14,16 Zheng et al determined that patients with a low postoperative LDI were statistically more likely to develop ASD than those who had normal postoperative LDI (25% vs 4.1%, P = 0.006), as were patients with a high postoperative LDI (18.4% vs 4.1%, P = 0.007).16 In previous studies,14,16 the abnormal LDI groups tend to continue in the same groups, while in this analysis, 50% of the patients in the hyperlordotic group and 43% of patients in the hypolordotic group improved to an LDI within the normal range (Figure 6).

Lordosis distribution index (LDI) comparisons for different distribution groups. The pre- to postoperative changes in LDI for each group as reported by Bari et al14 are also shown.
Patients with a postoperative hypolordotic distribution present a greater risk of developing ASD and are the most frequently likely to require revision surgery.14,16,20 In the present study, the hypolordotic group initially exhibited a preoperative LLL angle mean of 19° and an LL falling within the normal range at 50°, creating an average LDI of 38%. However, this was not adequately aligned with the PI of 64°, resulting in a PI−LL discrepancy of 13°. The utilization of personalized implants produced an increase in the LLL angle to 27°, creating a statistically significant increase in LDI to 46% and a statistically significant decrease in PI−LL to 6°. In hyperlordotic cases, the LLL angle was within an acceptable range at 38°, accompanied by an LL of 42° creating an average LDI of 91%. The average PI of 54° resulted in a PI−LL discrepancy of 12° (Tables 2 and 3). While the LLL angle was maintained postoperatively, an increase in LL reduced the PI−LL discrepancy to 10° and the average LDI to 83%. These changes were not statistically significant. The compensatory changes in the IVL in the proximal levels to L4 in each LDI group were also not statistically significant (Table 5).
Although there were improvements in the abnormal LDI groups, likely based on the preoperative plan related to PI−LL, future opportunities to optimize LDI through preoperative planning focusing on this index are warranted. A larger increment in the LLL angle could be pursued, possibly achieving normal LDI more reliably. A recent study has demonstrated that achieving ideal LLL and LDI can remarkably reduce complication rates after lumbar fusion surgery.30 As reported in previous studies, LLL was nearly constant (approximately 35°) and independent of the PI.30,31 These findings emphasize the advantages of using PIC that reliably achieves planned alignment at the treated levels.32
This study has some limitations. The number of patients included did not permit meaningful assessment of patient outcomes based on surgical approach. The follow-up time was insufficient to allow for assessment of the long-term changes due to the PIC. Other studies indicate continued changes in LL, LDI, and segmental lordosis after a follow-up of 1 to 7 years potentially leading to ASD or revision surgery.14,16,21 Another limitation is the lack of a control group implanted with a standard cage, which would allow for a side-by-side comparison of the data. In addition, the number of patients may have limited the ability to detect some changes at a statistically significant level.
Conclusion
PIC implants may provide a benefit for patients, particularly those with hypolordotic distribution preoperatively, which showed significant improvements in LDI and IVL angle at L5 to S1 with no measured reciprocal changes. Personalized implants have the potential to further improve patient outcomes by allowing surgeons to achieve individual lordosis correction goals identified during the planning process and achieve a more predictable lordosis at the distal segments (L4−S1). Focusing on LDI in addition to global lordosis is an important factor that should be addressed during the planning process. Further studies will be needed to fully explore the predictability of IVL changes at adjacent unfused levels when using PIC implants.
Footnotes
Funding This work was supported by funding from Carlsmed.
Declaration of Conflicting Interests Jeffrey P. Mullin discloses that he is a clinical research investigator and receives consulting fees from Carlsmed. Jahangir Asghar discloses that he is a clinical research investigator and receives consulting fees from Carlsmed. Ashvin I. Patel discloses that he receives consulting fees from Carlsmed. Joseph A. Osorio discloses that he is a clinical research investigator and receives consulting fees from Carlsmed. Justin S. Smith discloses that he is a shareholder and receives consulting fees from Carlsmed. Christopher P. Ames discloses that he is a clinical research investigator and receives consulting fees from Carlsmed. John Small discloses that he is a clinical research investigator for Carlsmed. Atman Desai discloses that he receives consulting fees from Carlsmed. Adrien Ponticorvo discloses that he is an employee of Carlsmed. Rodrigo J. Nicolau discloses that he is an employee of Carlsmed.
Disclosures In addition to the relationships listed in the Declaration of Conflicting Interests, Jeffrey Mullin reports consulting fees from Medtronic, Globus, and SI Bone, and serves on the CNS and AANS/CNS Joint Spine Section Executive Committees. Christopher Ames reports grants/contracts from SRS; royalties/licenses from DePuy Synthes, K2M, Next Orthosurgical, Stryker, Biomet Zimmer Spine, Medicrea, and NuVasive; consulting fees from DePuy Synthes, Medicrea, Agada Medical, Medtronic, and K2M; is the chair of the SRS Safety and Value Committee and serves on the executive committee of ISSG; serves on the editorial board for Operative Neurosurgery and Neurospine; is the director of Global Spinal Analytics, and has research interests with Titan Spine, ISSG, and DePuy Synthes. Justin Smith reports grants/contracts from SeaSpine/Orthofix, NREF, AO Spine, and DePuy Synthes/ISSGF; royalties/licenses from Highridge and Globus/NuVasive; consulting fees from Highridge, SeaSpine/Orthofix, Medtronic, Cerapedics, and Globus/NuVasive; support for attending meetings/travel from AO Spine; serving on the SRS Board of Directors and ISSGF Executive Committee; and stock/stock options from Alphatec and Globus/NuVasive. Altman Desai reports consulting fees from Stryker. Joseph Osorio reports grants/contracts from Medtronic; royalties/licenses from Alphatec; and consulting fees from Alphatec, Medtronic, and DePuy. John Small reports royalties/licenses from Astura Spine.
Ethics Approval This study utilized secondary research consisting of deidentified data for which consent is not required and was therefore exempt from institutional review board review under 45 CFR §46.104 (d)(4)(ii). No direct patient involvement occurred.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.