


Abstract
Background Adult spinal deformity (ASD) surgery often involves the placement of pedicle screws using various methods, including freehand technique, fluoroscopic guidance, and computer-assisted intraoperative navigation, each with distinct limitations. Particularly challenging is the instrumentation of pedicles with small or absent cancellous channels (Watanabe types C and D pedicles), commonly found at the apex of large curves where precise screw placement is crucial for effective deformity correction. 3D-printed pedicle screw drill guides (3DPSG) may assist in accurately placing pedicle screws while minimally disrupting the standard ASD surgery workflow. This study aims to evaluate the safety and efficacy of 3DPSG in ASD patients with Watanabe types C and D pedicles, where the safe corridor for screw placement is limited.
Methods 3DPSG were designed using fine cut (≤1.25 mm) computed tomography scans. Preoperative screw trajectory planning and guide manufacturing were conducted using computer-aided design software (Mighty Oak Medical, Englewood, CO). Four ASD surgeons with varying experience levels placed the guides. Data on patient demographics, pedicle morphology, number of levels instrumented, and implant-related complications were collected.
Results The study included 115 patients (median age 67, range 18–81 years) with 2210 screws placed from T1 to L5. The median number of levels instrumented per case was 11 (range 7–12). Diagnoses included adult degenerative scoliosis (n = 62), adult idiopathic scoliosis (n = 30), Scheuermann’s kyphosis (n = 2), and other complex conditions (n = 21). The overall accuracy rate for pedicle screw placement was 99.5%, with a 0% malposition rate in type C and D pedicles. No vascular or neurological complications or reoperations related to screw placement were reported.
Conclusion 3DPSG facilitates safe and accurate pedicle screw placement regardless of pedicle morphology in ASD surgeries. This includes the challenging Watanabe types C and D pedicles, typically found at curve apices, enabling surgeons to achieve high implant density and optimal spinal fixation in ASD patients.
Level of Evidence 4.
- 3D-printed patient specific guide (3DPSG)
- pedicle morphology
- pedicle screw insertion
- adult spine deformity
Introduction
Accurate positioning of pedicle screw instrumentation in the thoracic and lumbar spine is necessary for the modern surgical treatment of adult spinal deformity (ASD) to assist with deformity correction.1 Conventionally, pedicle screw placement has relied on techniques such as the freehand method, fluoroscopic guidance, or computer-assisted navigation, each with its advantages and limitations.2 In the context of ASD surgery, the presence of small or absent cancellous channels within pedicles, such as those in Watanabe types C and D pedicles, can make accurate and safe positioning of pedicle screws difficult and time consuming.3 These pedicle types are frequently encountered at the concave apex of large curves.3 The ability to accurately achieve high-implant density at the apex of a deformity can aid in optimal deformity correction.3
The emergence of 3D-printed pedicle screw guides (3DPSG) offers a promising solution for enhancing the accuracy and speed of pedicle screw placement while minimizing disruptions to a conventional open ASD surgical workflow.4,5 However, the efficacy and safety of using 3DPSG in patients with small or entirely cortical pedicles has not previously been evaluated.
In this study, we evaluated the effect of pedicle morphology on the safety and accuracy of pedicle screw placement utilizing 3DPSG in a large single-center series of ASD patients. Our goal was to determine if pedicle screws could accurately be placed in Watanabe types C and D pedicles (absent cancellous channel or cortical slit only) and to examine the characteristics of misplaced pedicle screws using this technique.
Material and Methods
Study Design
We performed a retrospective analysis of patients who underwent ASD surgery over a 5-year period (2019–2023) at our center. This study was conducted in accordance with the principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the institutional review board (IRB 15063) prior to the commencement of data collection and analysis. Patient confidentiality and privacy were strictly maintained throughout the study process.
Patient Selection
Patients included in the study were patients who underwent surgery for correction of ASD and had pedicle screws placed using 3DPSG. Patients were excluded from the study if complete operative notes (including correct instrumentation levels and intraoperative complications) and preoperative computed tomography (CT) or intraoperative O-arm images (for assessing pedicle type and breaches of pedicle margins) were not available.
Data Collection
Demographic data, including patient age, sex, and diagnosis, were collected from medical record. Fine-cut CT scans (1.25 mm or less) were utilized for detailed assessment of pedicle morphology based on the Watanabe classification.3 Briefly, Watanabe and colleagues described pedicles as type A (normal cancellous channel), type B (small cancellous channel), type C (absent cancellous channel), or type D (cortical slit only). The number of levels instrumented using 3DPSG per case was documented. Any misplaced or revised pedicle screws were noted from the operative record and/or from a review of the intraoperative CT scan (Medtronic O-arm, Minneapolis, MN, USA) images obtained after instrumentation placement using 3DPSG.
Pedicle Screw Placement Technique
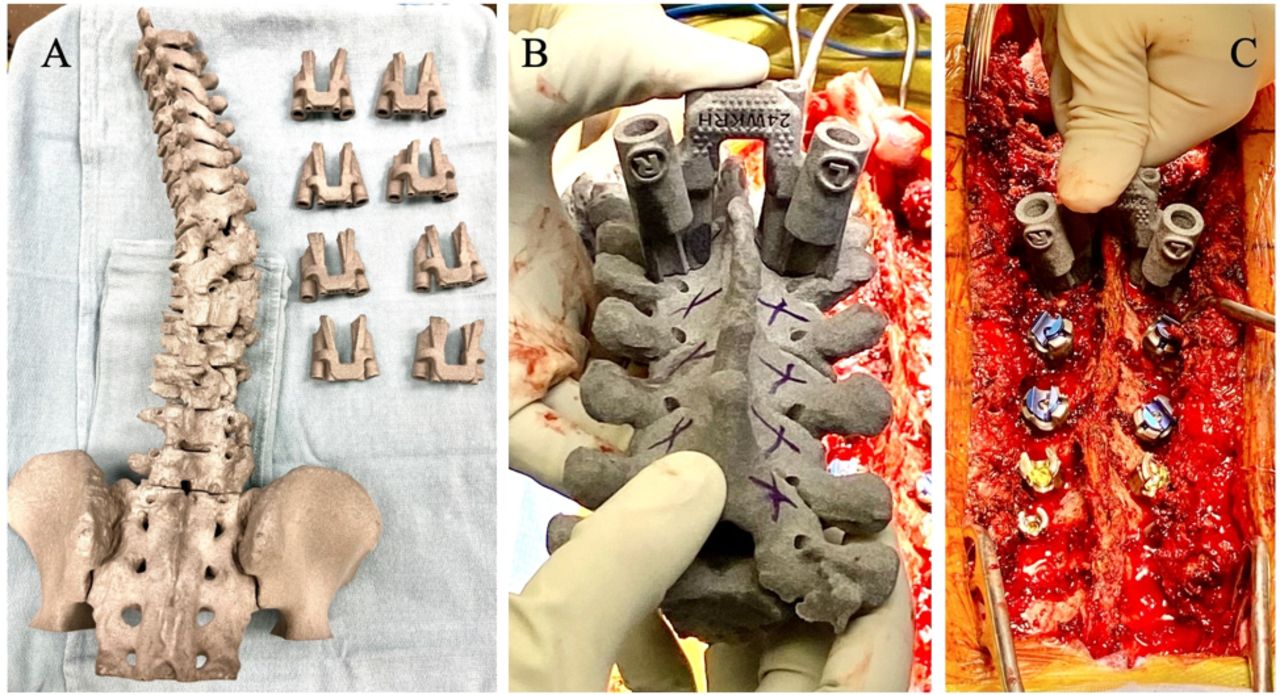
The 3DPSG was designed and manufactured based on preoperative CT scans with fine-cut slices (1.25 mm or less). Screw trajectories were planned using computer-aided design software prior to surgery (Mighty Oak Medical, Englewood, CO). Each guide relied on surface fit on the bony posterior elements on a level-by-level basis (Figure 1A and B). Occasionally in the setting of a confirmed fusion, a block guide was utilized that relied on points of contact on several vertebral levels at once.

Intraoperative images of custom 3D-printed pedicle screw guides. (A) Sterile, back table preparation of all 3D-printed guides for a specific patient. (B) One specific guide being placed at planned instrumented level. (C) A pedicle tract being drilled with orientation provided by the custom 3D-printed guide.
After meticulous dissection of the spine to expose the bony anatomy, the guide was placed onto the spine at the level of interest, and then a 2.4 mm drill bit was used to cannulate the pedicle, followed by tapping through the guide to enlarge the tract, followed by drilling, and tapping of the other pedicle at the same vertebral level (Figure 1C). The guide was then removed, the tracts palpated to ensure no bony breaches, and the screws placed down the previously prepared tracts. This uniform technique was utilized by all of the surgeons, for all of the cases in this series.
Outcome Measures
The primary outcomes assessed in this study were the safety and accuracy of pedicle screw placement using 3DPSG. The accurate placement was defined as the successful positioning of screws within the pedicle without any breach or malposition and the screw tip contained within the vertebral body, which was assessed by intraoperative O-arm spin after screw placement (Figure 2). The incidence of misplaced or revised screws, implant-related complications, including vascular or neurological injury, and the need for reoperation related to screw placement were also evaluated. The image assessment for malpositioned screws was performed by a neurosurgical spine fellow.

Computed tomography axial image showing safe placement of thoracic pedicle screw instrumentation into a type B pedicle on the left and type D pedicle on the right (A and B).
Data Analysis
Descriptive statistics, including median, interquartile range, and percentages, were utilized to summarize patient demographics, pedicle morphology, number of instrumented levels, and implant-related complications. The rate of accurate pedicle screw placement, as well as any associated complications, was calculated. Subgroup analyses were performed to assess the impact of pedicle morphology on the safety and accuracy of screw placement.
Results
A total of 115 patients were included in the study, with a median age of 67 years (age range: 18–81 years) and woman-to-man ratio of 7.2:1. The cohort consisted of patients with various types of spinal deformities, including adult degenerative scoliosis (n = 62), adult idiopathic scoliosis (n = 30), Scheuermann kyphosis (n = 2), and other complex conditions (pathological scoliosis, congenital scoliosis, and kyphoscoliosis; n = 23; Table 1).
Demographic details and primary diagnosis of patient cohort (N = 115).
Across the cohort, a total of 2210 pedicle screws were placed using 3DPSG (Table 2). The guided levels ranged from T1 to L5, with a median number of 11 levels instrumented per case (interquartile range: 7–12). Seventy-five percent of Watanabe type C pedicles and 86% of Watanabe type D pedicles were located on the concavity of the thoracic or thoracolumbar scoliosis (Table 3).
Details of pedicle screw instrumentation (N = 115).
Details of type C and D pedicles.
Out of the 2210 screws placed, 2200 were correctly positioned within the pedicle leading to an accuracy rate of 99.5%. The 10 misplaced screws were all placed in Watanabe types A or B pedicles (Table 4). Of the misplaced screws, there were 4 medial and 6 lateral breaches. All of the misplaced screws were in pedicles located on the concave side of the scoliosis (Table 5). These screws were either removed and abandoned or replaced via a freehand or fluoroscopy-assisted technique. Notably, there were no instances of screw malposition in Watanabe types C or D pedicles using 3DPSG (Table 4). Additionally, there were no vascular or neurological complications, and no reoperations associated with pedicle screw placement using 3DPSG.
Summary of pedicle screws placed using 3DPSG.
Details for misplaced/revised pedicle screws.
Discussion
The results of this study show that the use of 3DPSG for instrumentation placement in ASD surgery is safe and effective, including in challenging Watanabe types C and D pedicle morphology where we had a 100% accuracy rate. 3DPSG are thus safe and effective as a technique for screw placement in ASD patients with challenging pedicle anatomy.
There are various other techniques currently utilized worldwide for pedicle screw placement in patients with ASD including freehand technique with or without fluoroscopy-assisted, computer-assisted navigation, and robotic-assisted navigation.
Freehand Technique
Pedicle screw placement accuracy using freehand technique with or without intraoperative fluoroscopy ranges from 84.6% in the thoracic spine to 90.9% in the lumbar spine.6 Castro et al reported a 71% accuracy rate in lumbar pedicle screw placement.7 Similarly, Weinstein et al reported a 79% accuracy rate for fluoroscopy-guided pedicle screws, with 92% of the breached screws having a breach of the medial pedicle wall.8 Suk et al retrospective study on 462 deformity patients with screws placed via freehand technique showed an accuracy of 89.6%, with 0.8% experiencing new neurological deficits.9 Certainly, in experienced hands, these accuracy rates can be higher, but there appears to be a non-negligible rate of pedicle screw misplacement when using a freehand technique but with a low rate of new neurological or vascular injuries.
Computer-Assisted and Robotic Navigation
The accuracy rates reported using navigation or robotics are generally higher than those reported for the freehand technique. Rajasekaran et al reported in a randomized controlled trial a 98% accuracy in thoracic pedicle screw placement for spinal deformity correction using navigation.10 Rivkin et al retrospective review of 266 patients undergoing thoracolumbar pedicle screw fixation using Stealth navigation (Medtronic, Memphis, TN) showed a 94.7% overall accuracy rate.11 Likewise, Van et al multinational, multicenter, prospective clinical study reported a 97.5% pedicle screw placement accuracy rate using Stealth navigation, with 1.8% classified as “unacceptable” and revised during the same procedure.12 Fan and colleagues compared screws placed using robotic-assisted navigation with screws placed using a freehand technique and found that in the robotic-guided group, 95.3% of screws were perfectly positioned, and 98.7% were deemed acceptable, compared with the freehand technique which resulted in 86.1% of screws being perfectly positioned and 93.5% deemed acceptable (P < 0.01).13 Yu et al compared robotic-assisted vs computer-assisted navigation for screw placement and found smaller screw angular deviations and a higher incidence of acceptable screws in the robot-assisted group suggesting enhanced accuracy using robotic technology.14
There are several downsides to the use of computer-assisted navigation and robotic-assisted navigation for the placement of spinal instrumentation for ASD surgery. First is the potential for shifting of the reference array during the often-long duration of surgery which can cause inaccuracies during navigation and risks misplacement of instrumentation. This can be somewhat mitigated with the use of multiple arrays, but this is cumbersome and alters the normal open ASD surgery workflow. Second is the effect of soft tissue pressure caused by retractors or instruments brought into the field, which can also cause shifting of the registration and inaccuracies in the navigation. Third, there is a tendency when using these technologies to look away from the open spine and at a monitor displaying the images. This removes the visual feedback of seeing the anatomy and can also result in grossly misplaced instrumentation if there is an error in the navigation, often worse than what might happen with an experienced freehand surgeon. Fourth, there can be a significant capital cost associated with acquiring navigation or robotic technology if it is not already present at a hospital. These limitations are significantly mitigated with the use of 3DPSG where there is level-by-level fit of the guides, no need for intraoperative registration, and minimal disruption to the typical workflow for ASD surgery. With regard to cost, 3DPSG are typically purchased on a case-by-case basis and do not require capital expenditure and thus may be easier to get into a hospital system in this era of cost-containment.
Here, we showed that with the use of 3DPSG, we had a 99.5% accuracy rate with pedicle screw placement in ASD surgery. This was in line with the results of an RCT comparing 3DPSG vs freehand placement, which showed an accuracy rate of 3DPSG of 90%.15 To our knowledge, there has not previously been a report examining the accuracy of pedicle screw placement using 3DPSG in adult spine deformity surgery with respect to pedicle morphology. In our study, the screw malposition rate was 0% in Watanabe types C and D pedicles, which are the most challenging pedicles in which to achieve solid and safe fixation.3 Given that these pedicle types are often present in the apex of scoliosis, achieving solid fixation in these pedicles can allow for more aggressive corrective forces to be applied to the spine and likely can improve overall curve correction.
Interestingly, the majority of misplaced pedicle screws were observed to have lateral breaches, all of which occurred on the concave side of the spinal deformity curve. It is important to note that the screw itself is ultimately placed freehand, and the guides only assist with initial cannulation and for expansion of the pedicle using a tap. Given that the lateral pedicle wall has less dense bone than the medial pedicle wall, we hypothesize that it is easier for the screw to inadvertently breach laterally through the soft lateral cortex, whereas misdirection of the screw medially through the hard cortical bone of the medial pedicle wall is more rare.
The implications of these findings carry significant clinical relevance, presenting potential advantages for both surgeons and patients undergoing ASD reconstruction. By facilitating more precise and accurate pedicle screw placement, 3DPSG holds the promise of improving surgical efficiency, reducing operative duration, and diminishing the necessity for intraoperative revisions. This aligns with the conclusions drawn by Lopez et al in their meta-analysis, which indicated that the utilization of 3D-printed pedicle screw templates may lead to enhanced accuracy and precision in screw placement, decreased operative time, and reduced perioperative complications and radiation exposure when compared to non–3D-printed (fluoroscopy or CT) guided procedures.2 Furthermore, the capability to achieve high implant density, even in scenarios involving challenging pedicle morphologies, may contribute to enhanced deformity correction and favorable long-term clinical outcomes for patients with ASD.
Despite the promising results observed in this study, a few limitations warrant consideration. First, as a retrospective cohort study, inherent biases and confounding factors may influence the interpretation of results. Also, the resolution of an O arm image is not equivalent to a formal CT scan; thus, mild breaches might have been difficult to detect especially with the placement of large screws into small pedicles. Given the resolution limitations with O arm imaging, the standardized Gertzbein and Robbins classification system for accurate pedicle screw positioning was not used. Notably, small breaches (Gertzbein-Robbins B or C) are typically clinically insignificant, and notably in our series, there were no vascular injuries and no new neurological deficits associated with screw placement. Additionally, the study’s single-center design and lack of a comparison group limits the generalizability of findings to broader surgical practice settings. Furthermore, our center has a very large experience utilizing 3DPSG, and less experienced surgeons may have more misplaced screws given the learning curve inherent in using the technique. The 4 surgeons in this study have used 3DPSG for a minimum of 5 years. It should also be noted that in this series, 5 of the misplaced screws occurred in 2019 to 2020, and 5 occurred in 2021 to 2023 suggesting no large difference in malposition rate over time. Moreover, while the absence of immediate complications related to screw placement is encouraging, multicenter prospective data are needed to assess the durability and sustainability of surgical outcomes achieved with 3DPSG.
Looking ahead, future research endeavors could focus on prospective, multicenter studies to validate the findings of this study in diverse patient populations and surgical settings and provide direct comparison with navigation or robotically placed screws. Additionally, prospective comparative studies evaluating the cost-effectiveness of 3DPSG vs conventional techniques could provide valuable insights into the economic implications of adopting this technology in ASD surgery.
Conclusion
Our study demonstrates the accuracy and intraoperative safety of using 3DPSG for the placement of pedicle screws in ASD patients. Through meticulous analysis, we have demonstrated that this technique provides a dependable solution for navigating challenging pedicle morphologies, resulting in high implant density and improved surgical outcomes for patients with ASD. This technique provides a safe and effective alternative to freehand technique, computer-, or robotic-assisted navigation for placement of pedicle screws with minimal changes to a typical open ASD surgery workflow.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Jean-Christophe Leveque reports consulting fees from Axis Spine; speaking/teaching arrangements with SI-Bone; and serving on a scientific advisory board for SI-Bone. Philip Louie reports consulting fees from Alphatec, DePuy Synthes, Viscon, and Augmedics; serving on a scientific advisory board for AO Spine; and receiving fellowship support form AO Spine. Venu Nemani reports consulting fees from Medtronic, ATEC, and DePuy Synthes; speaking/teaching arrangements from Medtronic, ATEC, and Augmedics; and fellowship support from AO Spine.
Ethics Approval Ethical approval was obtained from the institutional review board (IRB 15063) prior to the commencement of data collection and analysis.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.