


Abstract
Background Historically, iliac crest bone graft has been used as the graft of choice for lumbar spine fusion procedures. Because fusion techniques have become less invasive, the demand for minimally disruptive grafting options has increased. This prospective study was performed to assess clinical and radiographic outcomes of patients treated with an iliac crest bone graft alternative and lateral lumbar interbody fusion.
Methods Fifty degenerative lumbar patients were treated with the extreme lateral approach to interbody fusion and a β-tricalcium phosphate–hydroxyapatite graft with bone marrow aspirate (BMA) at 1 or 2 adjacent levels. BMA was collected from the iliac crest with a bone aspiration needle and applied to the FormaGraft (NuVasive, Inc., San Diego, California) in a 1:1 ratio. Radiolucent cages were filled with FormaGraft strips, granules, or blocks and implanted in a standard fashion. Clinical data were collected at baseline, 6 weeks, and 3, 6, and 12 months and included visual analog scale, Oswestry Disability Index, and Short Form 36 patient-reported assessments. Fusion assessments were made from neutral anteroposterior/lateral radiographs, lateral flexion/extension radiographs, and computed tomography images taken at least 12 months after surgery.
Results Forty-four patients treated at 49 levels completed follow-up. The mean patient age was 54.7 ± 10.8 years, and mean body mass index was 30.8 ± 7.7 kg/m2. Radiographic fusion was observed in 41 of 44 assessed levels (93.2%). Blood loss was less than 100 mL in 95.5% of patients. Of the patients, 93.2% spent 1 night or less in the hospital. By the 6-week follow-up, all clinical outcomes were significantly improved (P < .05). Improvements were maintained or increased throughout the course of follow-up.
Conclusions This report shows that the technique of extreme lateral approach to interbody fusion in combination with FormaGraft and BMA in the interbody space is a safe and effective treatment option for interbody fusion of the lumbar spine when compared with other approaches and biologic options.
The clinical and radiographic outcomes after a lumbar interbody fusion procedure are influenced by a number of factors, including surgical approach, interbody implant, internal fixation, and application of biologics.
The extreme lateral approach to interbody fusion (XLIF) (NuVasive, Inc., San Diego, California) is a minimally disruptive technique for fusion of the anterior spine. The technique was first described in 20061 and has gained wide-spread acceptance within the spine community.
With decreased morbidity at the surgical site, there has been an increased demand for minimally disruptive grafting options as well. Traditionally, interbody fusion procedures have included the use of iliac crest bone graft (ICBG) to increase fusion success and healing. However, concerns about graft-site morbidity and resultant changes in clinical and financial outcomes have fed a demand for alternatives. Bone marrow aspirate (BMA) has the same osteogenic qualities as ICBG and can be collected from either the vertebral bodies or the iliac crest with a thin aspirate needle. The combination of BMA with osteoconductive materials such as hydroxyapatite (HAp) and β-tricalcium phosphate (β-TCP) can theoretically provide a minimally disruptive alternative to ICBG. HAp and β-TCP graft alternatives have been studied in a number of applications and have been shown to perform as well as or better than iliac crest autograft in comparative studies,2–4 observational studies,5–8 and a number of animal studies.9, 10
Methods
Study design
The use of a β-TCP–HAp composite (FormaGraft; NuVasive, Inc.) with BMA as a substitute for iliac crest bone autograft was prospectively studied in 54 nonrandomized patients undergoing the XLIF procedure at 1 or 2 levels between February and November 2008. The study was approved and overseen by an institutional review board. Before enrollment, all patients gave their written consent for participation.
Study participation was limited to patients aged between 18 and 70 years with a primary diagnosis of internal disc disruption at 1 or 2 contiguous lumbar levels between L1 and L5 and persistent back or leg pain for at least 6 weeks. Patients were excluded if they had more than 1 previous failed fusion or active or latent infection of the disc or spine.
Surgical protocol
The procedure was performed by standard surgical technique as previously described,1 with optional internal fixation. BMA was collected from the iliac crest with a bone aspiration needle during the primary procedure. A maximum of 2 mL of BMA was collected per aspiration site, for a total of 15 to 20 mL on average. The FormaGraft was prepared by applying BMA to the graft in a 1:1 ratio by volume. Radiolucent cages were filled with synthetic graft strips, granules, or blocks and implanted in a standard fashion.
Outcome measures
Baseline demographics were collected at the preoperative visit. Surgical outcomes, including estimated blood loss, surgical time, method of graft application, and intraoperative complications, were captured during surgery.
Clinical outcome measures were collected at each visit and included complication assessments, work status, and visual analog scale (VAS), Oswestry Disability Index (ODI), and Short Form 36 patient-reported assessments. Outcome measures were completed by patients preoperatively and postoperatively at 6 weeks and 3, 6, and 12 months.
Anteroposterior and neutral lateral radiographs were collected at every visit. Flexion and extension lateral radiographs were collected preoperatively and postoperatively at 3, 6, and 12 months. Computed tomography (CT) scans were performed after the 12-month visit to assess fusion. Radiographic assessment of interbody fusion was conducted by an independent board-certified orthopedic surgeon using a modification of the Lenke grading system,11 where grade I and grade II levels were classified as fused and grade III and grade IV levels were classified as unfused. In addition to the Lenke scale, a secondary scale was used to describe the volume of bone present in the disc space. The Lenke scale and volume scales are defined in Table 1.
Radiographic evaluation scales
Results
Patient demographics
A total of 55 levels were treated in 50 patients at a single center. Two patients died of causes unrelated to their spine condition or procedure, and 4 patients were lost to follow-up. At the end of the study, 44 patients (31 women and 13 men) had completed a clinical evaluation and/or radiographic evaluation at least 12 months after surgery: 36 had both clinical and radiographic records, 5 had CT scans without 12-month clinical outcomes, and 3 had 12-month clinical outcomes without radiographs. Baseline and procedure data are reported for all 44 patients, clinical data are limited to those patients who completed a 12-month clinical assessment, and the fusion assessment is limited to those patients with CT evaluations at least 12 months after surgery.
At baseline, the mean patient age was 54.7 ± 10.8 years (range, 24–70 years) and mean body mass index was 30.8 ± 7.7 kg/m2. Significant comorbidities included smoking (n = 21, 42.0%), obesity (n = 24, 48.0%), and diabetes mellitus (n = 4, 8.0%). Before surgery, 13 patients (26.0%) were working, 17 (34.0%) were retired voluntarily, 6 (12.0%) were retired because of illness, 7 (14.0%) were medically disabled, and 2 (4.0%) were homemakers.
Indications for surgery included 1 or more of the following: spondylolisthesis (n = 26, 52.0%), degenerative disc disease (n = 22, 44.0%), stenosis (n = 22, 44.0%), lateral listhesis (n = 8, 16.0%), adjacent segment disease (n = 7, 14.0%), instability (n = 7, 14.0%), scoliosis (n = 7, 14.0%), herniated nucleus pulposus (n 4, 8.0%), and post-laminectomy instability (n = 2, 4.0%). On average, patients were treated at 1.1 levels. L4-5 was included in 28 procedures (63.6%) and accounted for over half of levels treated. L1-2 was included in 2 procedures (4.5%), L2-3 in 5 (11.4%), and L3-4 in 14 (31.8%). Six patients were also treated at L5-S1 with a trans-sacral approach (TranS1 Inc., Wilmington, North Carolina); these levels are not included in the fusion results of this study.
Operative data
Intraoperatively, 22 patients (50.0%) lost less than 50 mL of blood, 20 (45.5%) lost between 50 and 100 mL, and 2 (4.5%) lost greater than 100 mL. The operative time for patients ranged from 40 to 138 minutes (mean, 66.0 ± 27.4 minutes). All levels were treated with polyetheretherketone cages in the interdisc space. Supplemental posterior internal fixation included unilateral posterior pedicle screw fixation (n = 26, 59.1%) or bilateral posterior pedicle screw fixation (n = 7, 15.9%). In 11 patients (25%) posterior pedicle screws were not used; rather, they were treated with supplemental lateral fixation.
A combination of β-TCP–HAp strips, granules, and blocks was used with BMA; patients were treated with strips alone (n = 22, 50.0%), both strips and granules (n = 20, 45.5%), or blocks alone (n = 2, 4.5%). Length of hospitalization ranged from 0 to 4 days, with 90.7% of patients spending 1 night or less in the hospital. There were no complications noted during surgery or hospital stay.
Patient-reported clinical outcomes
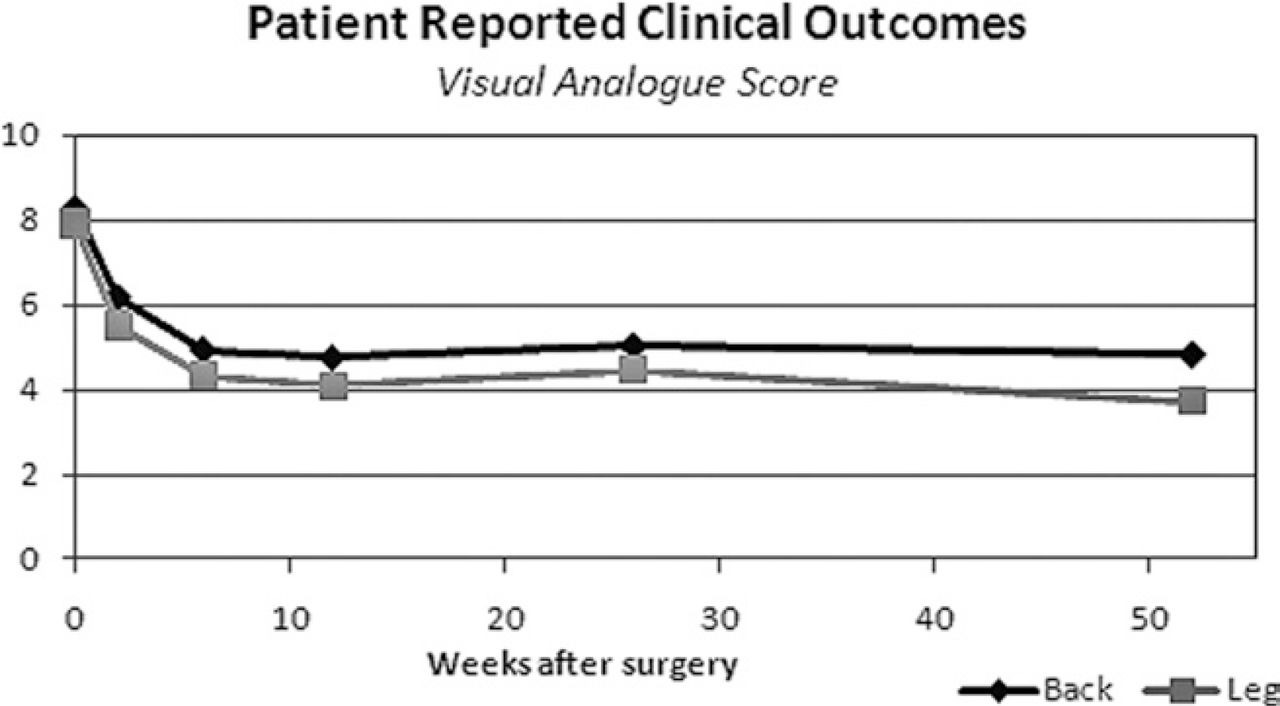
Mean baseline scores were as follows: Visual Analogue Scale (VAS) for back pain, 8.2 ± 1.8 cm; VAS for leg pain, 7.9 ± 2.0 cm; and ODI, 50.9% ± 15.2%. By the 6-week follow-up, all clinical outcomes were significantly improved (P < .05). Improvements were maintained or increased throughout the course of follow-up. At 12 months, the mean VAS score for back pain was 4.8 ± 3.1 cm and the mean VAS score for leg pain was 3.7 ± 3.1 cm. The mean ODI was 33.1% ± 19.6%, and the mean Short Form 36 score was 53.3 ± 19.5 (Figs. 1 and 2).

Short Form 36 (SF-36) and ODI scores over time.

VAS scores over time.
Early complications—defined as those that occurred up to 6 weeks after surgery—included 1 readmission to the hospital for pain and swelling within 24 hours of discharge, as well as 1 revision for residual stenosis. Late complications—defined as those that occurred more than 6 weeks after surgery—included 1 incident of residual stenosis at the operative level that required surgical intervention, as well as 1 patient who underwent excision of a subcutaneous lesion believed to be residual graft material 12 months after the index procedure, performed by another surgeon. There were no complications reported related to BMA collection or implant subsidence.
Radiographic results
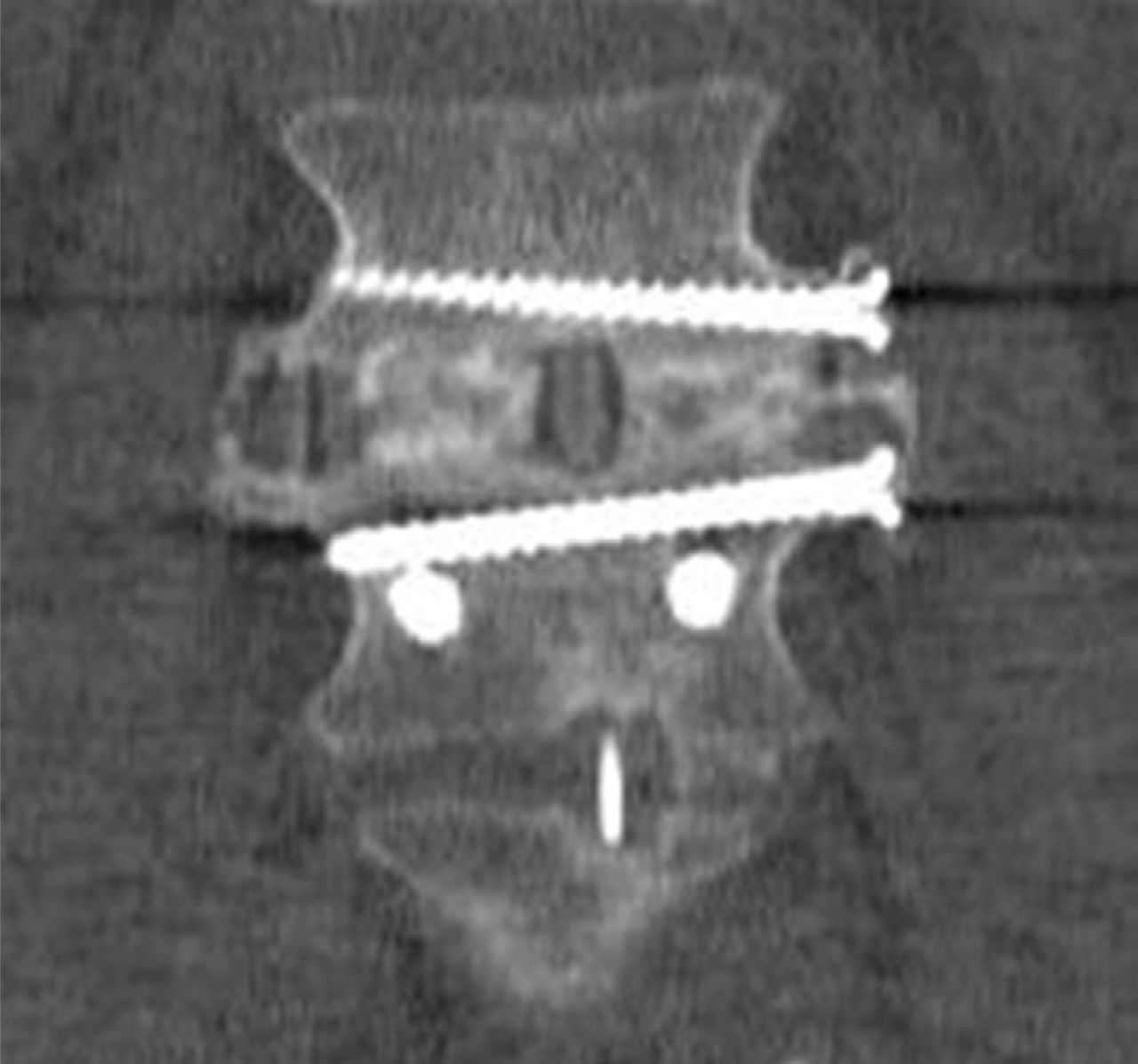
CT scans used to assess fusion were collected a mean of 17.3 months (range, 12–31 months) after surgery. At the time of radiographic review, 41 of the 44 levels assessed (93.2%) were fused (Fig. 3). A modification of the Lenke interbody fusion scores22 yielded the following: grade I, 68.1% (n = 30); grade II, 25.0% (n = 11); grade III, 6.8% (n = 3); and grade IV, 0% (n = 0). Volume assessments were as follows: grade I, 0% (n = 0); grade II, 6.8% (n = 3); and grade III, 93.2% (n = 41).

Example of fusion on CT scan.
Discussion
All patients in this series were treated with BMA from the iliac crest. Although this application requires multiple aspiration sites in the iliac crest, harvesting BMA is quicker and far less invasive than removing ICBG. None of the patients in this series had any complications at the site of BMA collection, and none required revisions related to graft subsidence or nonunion.
In 2008 Dai and Jiang reported on 62 spinal stenosis patients who were randomized to receive β-TCP and local autograft or ICBG and local autograft to supplement their posterolateral fusions.5 Three years after surgery, fusion results and clinical outcomes were comparable, but all ICBG patients reported at least some pain at the ICBG donor site, showing not only the effectiveness of β-TCP as an ICBG alternative but also the potentially lasting morbidity after ICBG harvesting.3
Bone morphogenetic protein (BMP) is an ICBG alternative that has been associated with high fusion rates but also with a number of complications, including radiographic graft resorption, ectopic and heterotopic bone formation, radiculopathies, epidural cyst formation, and seromas.12, 13 In 2009 Rihn et al. reported on a cohort of 130 Transforaminal Lumbar Interbody Fusion (TLIF) patients treated with either recombinant BMP or ICBG.13 Despite reasonable fusion success (96.4% in cohort with no significant difference between groups), both patient groups had considerable complications, many of which were directly attributable to the graft used. In the recombinant human BMP group, 5.8% of patients had symptomatic vertebral osteolysis and 2.3% had ectopic bone formation; 30.3% of ICBG patients had documented donor-site morbidity. The only graft-related complication in this cohort is presumed presence of residual subcutaneous graft material—at the time of excision, no ectopic ossification was reported by the operating surgeon.
In our study successful fusion was achieved in 93.2% of levels, with abundant new bone growth. There were no revisions for segmental nonunions in this cohort. Recently reported lumbar fusion rates have ranged from 91% to 100% for XLIF14–17 and 90% to 100% for posterior lumbar interbody fusion (PLIF)/TLIF,18–21 with no apparent difference between minimally invasive and traditional open techniques.
In 2010 Schuster et al. reported on infection and concluded that case-specific factors including blood loss and case length influence the incidence of postoperative infection.22 In 2009 Rihn et al. reported the combined autograft harvest site/lumbar wound infection rate of single-level TLIF with ICBG at 9.2%.13 In this series, there was 1 report of wound swelling that did not require surgical treatment and there was no incidence of postoperative infection. Through the use of a minimal incision and the elimination of an additional surgical site for ICBG harvesting, the lateral approach with β-TCP–HAp may have effectively reduced the risk of infection by reducing surgical times and blood loss.
Conclusion
This report shows that the XLIF technique in combination with FormaGraft and BMA in the interbody space is a safe and effective treatment option for interbody fusion of the lumbar spine when compared with reports of other approaches and biologic options.
Footnotes
NuVasive, Inc. has provided research funding to support this study.
- © 2012 ISASS - International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.