


Abstract
Background Different procedures have been used for the treatment of lumbar juxtafacet cysts (JFCs). Recently, full-endoscopic cyst excision has been suggested as a reasonable alternative. We performed a meta-analysis to assess the overall rates of favorable outcomes and adverse events for each available treatment and determine the outcome and complication rates concerning spine stability.
Methods Multiple databases were searched for English-language studies involving adult patients with lumbar JFCs who had been followed for more than 6 months. Outcomes included the proportion of patients with a satisfactory outcome. Adverse events included recurrence and revision rates as well as intraoperative complications. We further stratified the analysis based on the spine’s condition (degenerative listhesis vs without degenerative listhesis).
Results A total of 43 studies, including 2226 patients, were identified. Over 80% of patients experienced satisfactory improvement after surgical excision but only 66.2% after percutaneous cyst rupture and aspiration. Overall, recurrence and revision rates were almost double in patients with preoperative degenerative listhesis at the cyst level, especially in the minimally invasive group (2.1% vs 31.3% and 6.8% vs 13.1%, respectively). The rate of full-endoscopic satisfactory outcomes was approximately 90%, with low rates of adverse events (<2%).
Conclusion We analyzed the outcome and adverse event rates for each kind of available treatment for JFC. Full endoscopy has outcomes and rates of adverse events that overlap with open and minimally invasive approaches.
Level of Evidence 2A.
INTRODUCTION
Lumbar juxtafacet cysts (JFCs) are common in patients with degenerative spine disease and are responsible for radicular pain and neurological symptoms. The development of JFCs is linked to degenerative spondylosis, segmental instability, and trauma.1–3 The reported incidence of JFCs among patients undergoing lumbar surgery ranges from 0.1% to 0.8%, and degenerative listhesis is estimated to be present in 38% to 75% of these patients.4,5
JFC treatment’s mainstay is laminectomy/hemilaminectomy and cyst excision, sometimes coupled with total facetectomy and fusion.6 Conservative management or percutaneous cyst rupture and aspiration,7 typically used in the elderly or those unwilling or unsuited for surgical treatment,8 is mostly temporarily effective and has high recurrence rates.9–12
Recently, minimally invasive techniques have been used to treat such patients, expanding spinal surgeons' therapeutic choices.13 The full-endoscopic approach has also gained importance in the surgeon’s armamentarium and, more recently, has been used for degenerative disease treatment.14
Several studies have tried to review and compare the outcomes and adverse events of different surgical techniques for JFCs.15–17 However, because some of these studies did not report results per the surgical procedure, they lacked detailed information about their possible outcomes. This is especially true regarding patient selection based on suspected spine instability at the cyst level. Therefore, we restricted our literature analysis to studies with detailed information about surgical management and spine stability to compare actual surgical options. For the first time in literature, this resulted in an extensive stratified analysis of outcomes and adverse events for each type of procedure: open, minimally invasive, percutaneous, and full-endoscopic management of lumbar JFCs.
Methods
A comprehensive search of several databases (ie, PubMed, Epub Ahead of Print, Ovid MEDLINE In-Process & Other Non-Indexed Citations, Ovid MEDLINE, Ovid EMBASE, Ovid Cochrane Central Register of Controlled Trials, Ovid Cochrane Database of Systematic Reviews, and Scopus) was conducted with the help of an expert medical reference librarian. The search terms were “juxtafacet cyst,” “synovial,” “ganglion,” “lumbar,” “lumbar cysts,” “cyst,” and “spinal cyst,” which were used alone and in combination. Controlled vocabulary supplemented with the keywords was used to search for JFC formation in patients diagnosed with degenerative spinal diseases.
Inclusion criteria were as follows:
description of JFCs in both longitudinal and retrospective series that discussed the following:
synovial cysts in continuity with the capsule of the facet joints
ganglion cyst
≥5 patients
mean or median follow-up <6 months
published in English between January 2000 and April 2020
consecutive series of patients treated with the following:
percutaneous techniques (cyst rupture and aspiration)
open surgery (interlaminar approach or laminectomy/hemilaminectomy and cyst excision)
minimally invasive approaches (ipsilateral or contralateral microsurgical tubular approaches)
full-endoscopic surgery (interlaminar and/or transforaminal full-endoscopic access)
intraoperative or histological confirmation of JFCs
preoperative imaging adequate to assess spinal stability (either spine CT or MRI and dynamic x-ray)
patients who did not undergo instrumented fusion at the cyst level
patients with or without preoperative degenerative listhesis at cyst level
Studies dealing with patients with higher than grade I preoperative degenerative listhesis based on the Meyerding classification,18 with vertebral body slippage confirmed through dynamic x-rays or in case of isthmic spondylolisthesis, were excluded. Among these patients, the spine was considered severely unstable and suitable only for fusion procedures, thus perceiving cyst formation as an epiphenomenon of severe spinal instability. Studies with patients who underwent prior instrumented fusion at the cyst level were excluded.
Data Abstraction
We categorized the studies into 4 groups based on surgical technique, including patients who underwent either surgical or microsurgical cyst excision in the open surgery group. We included studies on patients who underwent microsurgical cyst excision with tubular retraction system in the minimally invasive group. The full-endoscopic group included those studies with patients who underwent endoscopic interlaminar or transforaminal approaches. In the percutaneous group, we included studies only on patients who had undergone computed tomography (CT or fluoroscopically guided JFC rupture and aspiration).
For each study, we extracted the following data: patient’s age (years), sex, JFC level, operative time (minutes), hospitalization time (days), follow-up (months), overall outcome, description of the procedure, intraoperative adverse events, whether the adverse events (both medical and surgical) manifested after more than 30 days, same-level JFC recurrence, the proportion of patients with preoperative spinal instability, method of assessing spinal instability (ie, spine CT, dynamic x-rays, or spine magnetic resonance imaging [MRI]), time from lumbar cyst treatment to the development of spinal instability at the affected level (months), and the proportion of patients requiring revision surgery for recurrence or developing instability at the treated level. We noted the surgical approach utilized for each surgical procedure (open vs minimally invasive vs full endoscopic vs percutaneous). We excluded patients with prior fusion surgery at the level of the JFC, but we collected the percentage of patients undergoing fusion surgery either at the surgery time or at developing instability.
The outcomes were defined as "satisfactory" based on MacNab or modified MacNab criteria,19 and the values were collected at the last follow-up visit or at least 6 months after the intervention. Only excellent and good scores were considered satisfactory. In some studies, we extracted the degree of postoperative satisfaction (“excellent” and “good”) from scores or scales similar to or attributable to MacNab’s criteria.
We included preoperative degenerative listhesis when the listhesis at the cyst level described in the pooled studies was within: (1) Meyerding grade 1 and (2) without vertebral body slippage on dynamic lumbar x-ray.
Every other intervention at the previously treated level or additional arthrodesis to overcome a developing spinal instability was considered as “revision surgery.” In the percutaneous group, revisions were divided into 2 subgroups: those needing an additional percutaneous cyst puncture and those requiring surgical cyst excision for symptom control. The following intraoperative adverse events were considered: nerve root damage, dural tear, seroma, and epidural hematoma.
When possible, we separately extracted the subpopulations of patients with confirmed preoperative degenerative listhesis from the investigated segment, calculating outcomes and adverse events for each population (no signs of preoperative degenerative listhesis or instability vs preoperative degenerative listhesis). We also abstracted the mean interval between the first surgery and the development of a more severe degree of spinal instability (ie, Meyerding grade <I or significant mobility in dynamic x-rays).
Study Evaluation
For each study, we evaluated the design, population, and imaging used in the follow-up. We also evaluated the risk of bias with a modified New Castle-Ottawa Quality Assessment Scale.20 The risk of bias was assessed based on the following questions: Did the study include all patients or consecutive patients with adequate radiological follow-up (spine MRI, CT, and dynamic x-rays)? Was the follow-up enough to ascertain the development of spinal instability or cysts recurrence (<24 months)? Was histological confirmation reported? (the histological confirmation is a measure of the original study’s methodological quality; also, JFCs may have different presentation stages [from fluid to sclerotic content], and histology may help to confirm JFCs excision). The studies were divided into “high” (≥6 points), “moderate” (4 or 5 points), and “low”(≤3 points) risk of bias categories, and 2 tiers were separately compared and analyzed to see whether there was any statistically significant difference between each (Table 1). Low risk of bias studies was defined as those with a predefined study protocol (randomized or prospective) and adequate imaging follow-up (spine MRI, CT, and dynamic x-rays; follow-up <24 months).
Statistical Analysis
Descriptive statistics were reported as a mean/range for continuous variables and proportion/percentage for categorical variables. For each technique, the proportion of patients considered improved and with adverse events was estimated. Estimates from each cohort were pooled in a random-effects meta-analysis model, as described by DerSimonian and Laird. Anticipating heterogeneity between studies, we chose this model a priori because it incorporates within- and between-study variance. In addition, because in some studies, the rate of outcomes was close to 0 or 1, the Freeman-Tukey double-arcsine transformation was utilized. We then made pairwise comparisons between groups for the respective outcomes. All statistical analyses were performed using Stata version 13.0 (StataCorp LLC, College Station, TX).
RESULTS
Literature Search and Study Characteristics
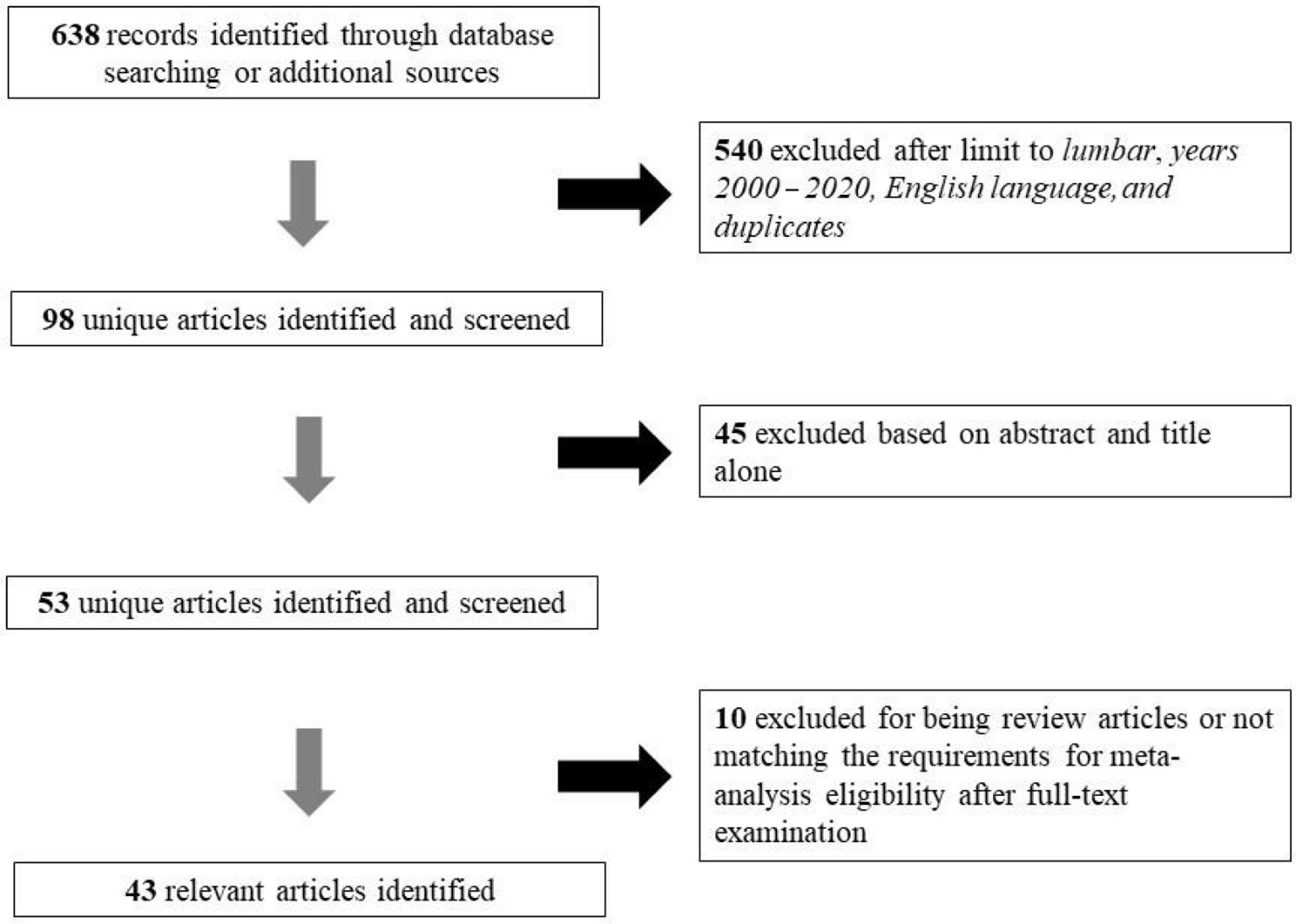
The initial literature search yielded 638 articles. Upon review of abstracts and titles, 540 were excluded. In full-text review, 53 more articles were excluded because they did not match the eligibility criteria for this meta-analysis, mainly including the length of follow-up, an adequate definition of lumbar JFCs, or surgical outcomes definition (Figure 1).
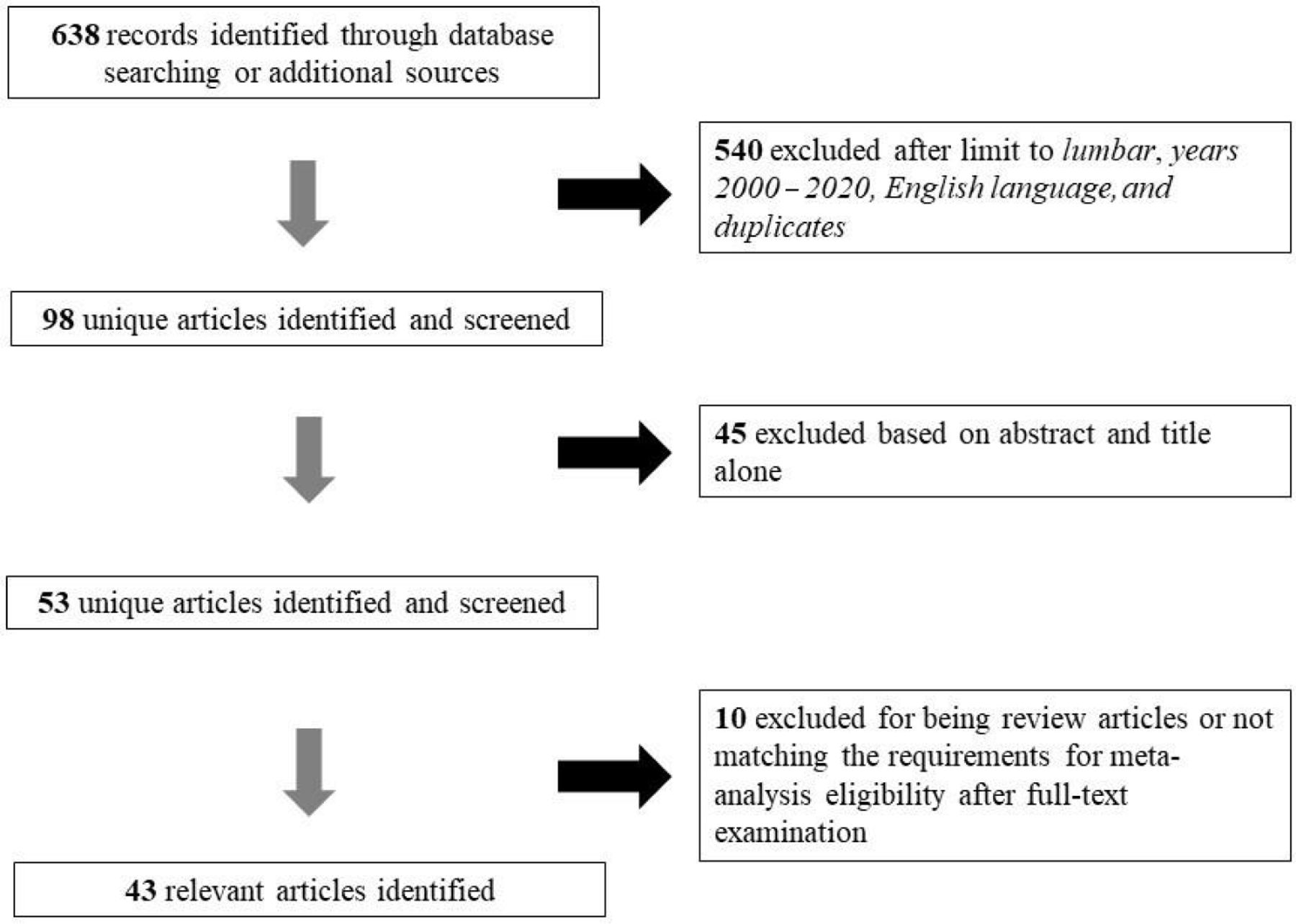
Flow diagram summarizing the process of study selection.
Forty-three studies, with 2226 patients, describing outcomes and adverse events of JFC treatment were included. Eighteen of these studies report outcomes after open surgery (1112 patients), 7 exclusively concern minimally invasive treatment (276 patients), 8 used full-endoscopic treatment (233 patients), and 7 used percutaneous rupture and aspiration procedures (477 patients). Three studies compare different kinds of surgical treatment: 1 study compares outcomes between full-endoscopic and open surgery (60 patients) and 1 study compares outcomes between percutaneous techniques and open surgery (45 patients). In another study reporting individual patient data, we were able to extract and separately analyze the outcomes of open vs minimally invasive approaches (23 patients).
Thirty-four studies were retrospective and 9 prospective. Of the 43 studies included in our meta-analysis, 5 had a high risk of bias, 25 had a moderate risk, and 13 had a low risk of bias.
A study-selection flow diagram compiled following the PRISMA guidelines21 is provided in Figure 1. A summary of the included studies is provided in Table 1. Methodological quality indicators are summarized in Table 2. Overall, these noncomparative series appeared to have adequate quality.
Summary of the characteristics of the included studies.
Methodological quality evaluation.
Open Surgery
A total of 21 studies, including 1112 patients (51.9% female), were identified. The mean age was 63 years (range 54.4–73 years). L4-L5 was the most affected level (67.3%), followed by L3-L4 (16%), L5-S1 (13.5%), L2-L3 (2.2%), and L1-L2 (1.0%). The average follow-up was 39.5 months (range 8.3–116.4 months). On average, hospital stays ranged from 3 to 7 days. Nineteen studies report the proportion of patients with preoperative degenerative listhesis at the JFC level to be 33.6%.
The most frequently used approach was laminectomy/hemilaminectomy (87.6%), followed by the interlaminar approach and flavectomy (7.5%), and laminectomy and instrumented fusion (4.9%). A medial facetectomy was usually chosen for cyst excision over a total facetectomy (5.4% vs 4.6%, P < 0.001).
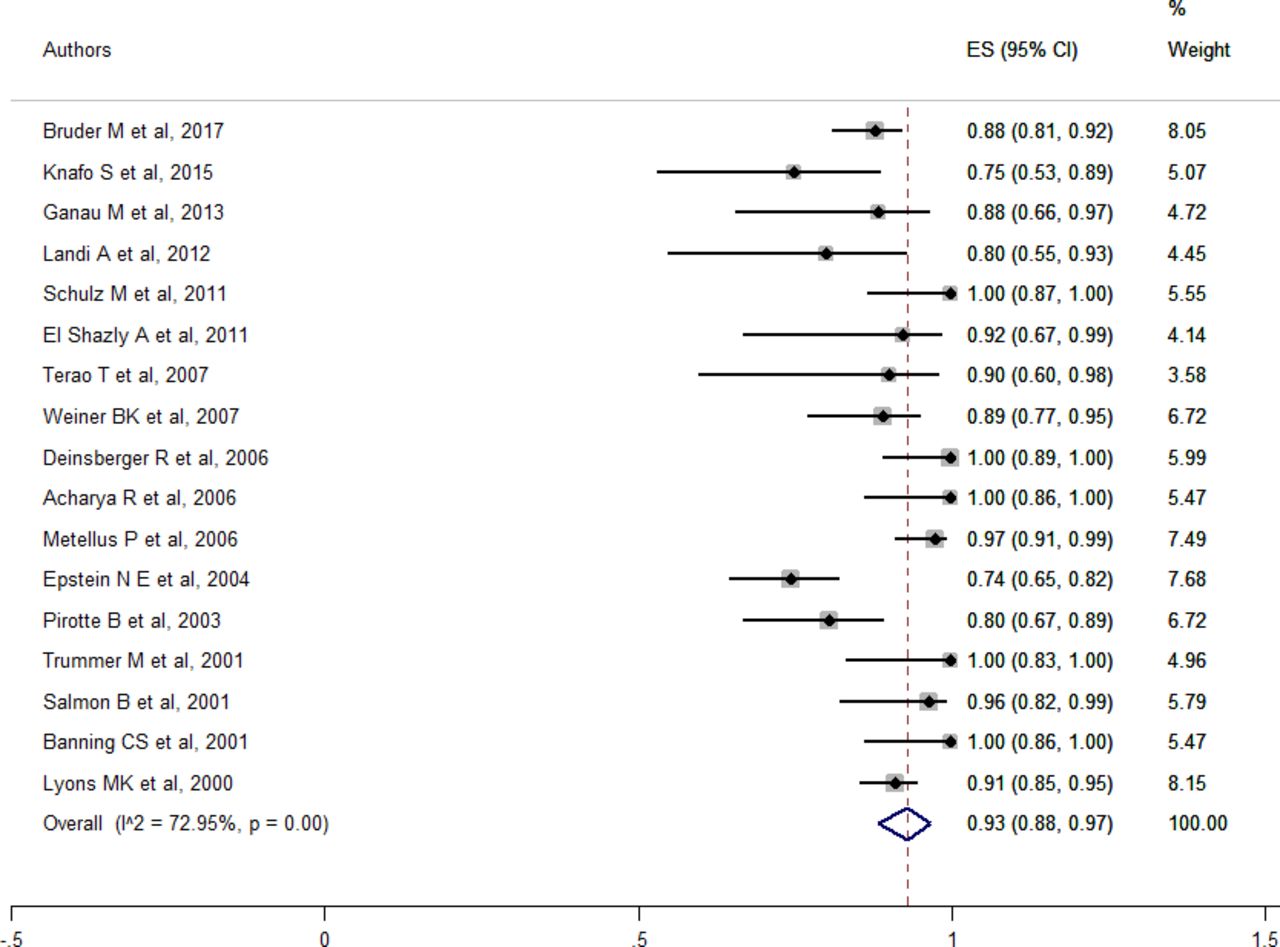
Overall, the satisfactory outcome rate after open surgical cysts excision was 93.0% (95% CI 88.3%–96.7%) (Figure 2), while the surgical adverse event rate was 1.1% (95% CI 0.1%–3.0%). Almost all the intraoperative adverse events were dural tears; only 3 epidural hematoma cases and 1 seroma occurred. Recurrence rate was low, 1.4% (95% CI 0.3%–3.2%), and surgical revision rate was 3.0% (95% CI 1.3%–5.3%). The rate of postoperative medical adverse events was negligible 0.1% (95% CI 0.0%–0.8%).
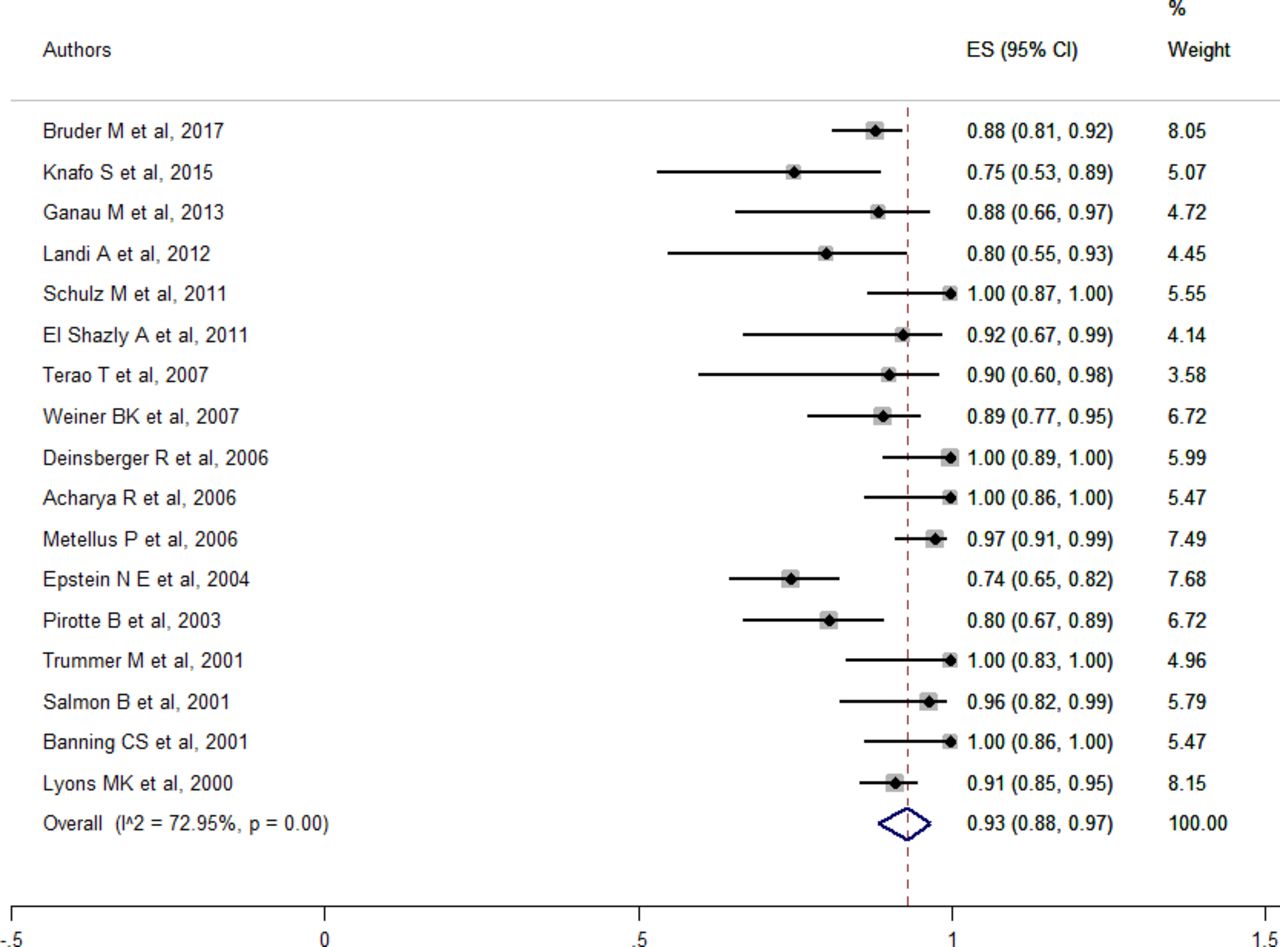
Forest plot for open surgery overall outcomes. ES, effect size.

Forest plot for minimally invasive overall outcomes. ES, effect size.
Overall, 5.9% (95% CI 0.0%–18.2%) of patients underwent unplanned intraoperative concomitant fusion in surgery, and 3.5% (95% CI 0.6%–8.0%) developed overt postoperative instability at the treated level. In the laminectomy group, 8.5% of patients had recurrence or revision surgery for developing instability at the decompressed level. In contrast, none of the patients who underwent concomitant instrumented fusion experienced recurrences or required additional surgery for developing instability in the follow-up period (P < 0.001).
Comparing satisfactory outcomes between patients with and without preoperative degenerative listhesis (92.7% [95% CI 85.7%–97.7%] vs 93.1% [95% CI 89.1%–95.6%]), we did not find significant differences (P = 0.854). Also, no significant differences in recurrence rates between patients with and without degenerative listhesis were found (2.5% vs 3.0%, respectively, P = 0.726). However, a significantly higher proportion of patients with preoperative degenerative listhesis required revision surgery than patients without listhesis (6.8% vs 3.1%, respectively, P = 0.020). The mean time to first intervention and revision surgery ranged from 7.5 to 24 months.
Minimally Invasive Approach
A total of 8 studies including 279 patients (women = 55.6%; mean age = 65.3 years, range 62.0–72.4 years) were identified. The most affected level was L4-L5 (62.2%), followed by L3-L4 (20.8%), L5-S1 (12.4%), and L2-L3 (4.6%). The average follow-up was 24.0 months (range 11.5–79 months). Hospital stay was consistently reported within 24 hours, while mean operative time was 130 minutes (range 58–184 minutes). Three studies describe a contralateral approach for tubular system insertion and cysts excision, while an ipsilateral method was used in 5. Six studies reported the proportion of patients with preoperative instability at the cyst level: 21.1%.
Overall, favorable outcomes were reported in 82.7% of patients (95% CI 61.2%–97.5%) (Figure 3), while surgical adverse events rate was 8.4% (95% CI 2.7%–16.3%). Most intraoperative adverse events were dural tears, and only 1 case of epidural hematoma occurred. The overall rate of patients who developed some postoperative instability was 3.2% (95% CI 0.2%–8.4%). The overall revision rate was 3.6% (95% CI 1.0%–2.3%), while overall recurrence rate was 2.3% (95% CI 0.3%–5.5%). There was no postoperative medical adversity reported. The mean time to first intervention and revision surgery ranged from 7 to 25.2 months. None of the patients underwent concomitant fusion at the time of intervention.
When comparing outcomes between patients with and without preoperative degenerative listhesis (77.8% [95% CI 46.7%–98.4%] vs 89.7% [95% CI 78.8%–97.6%], respectively), we found a slight decrease in the unstable patients’ outcomes (P = 0.011). Also, higher rates of revision surgery (13.1 % [95% CI 4.8%–24.0%] vs 3.6% [95% CI 0.2%–9.4%], P = 0.004) and intraoperative adverse events (31.3% [95% CI 18.9%–45.2%] vs 4.8% [95% CI 1.2%–9.9%], P < 0.001) were found in the degenerative listhesis group. No differences were found between these 2 groups in terms of recurrence and adverse medical events. No differences in outcomes and adverse events were found when stratifying patients by ipsilateral and contralateral minimally invasive approach.
Full-Endoscopic Approach
A total of 9 studies, including 263 patients (52.9% women, mean age = 49.2 years, range = 23.1–68.6 years), were identified. The most affected level was L4-L5 (70.1%), followed by L5-S1 (19.6%) and L3-L4 (10.3%). The average follow-up was 27.5 months (range 18–55.5 months). Hospital stay was consistently reported to be <24 hours, while mean operative time was 60.3 minutes (range 32–78 minutes). Three studies report the proportion of patients with degenerative listhesis at the cyst level to be 8.3%. None of the patients required additional fusion surgery in the follow-up time examined.
Overall, favorable outcome after full-endoscopic cysts excision was 90.9% (95% CI 83.8%–96.4%) (Figure 4), while surgical adverse events rate was 1.8% (95% CI 0.0%–5.3%). Except for an epidural hematoma, all the intraoperative adverse events were dural tears, and none required additional intervention for cerebrospinal fluid (CSF) fistula development. The overall JFC recurrence rate was 3.0% (95% CI 0.0%–9.9%), while the revision rate was 2.2% (95% CI 0.0%–8.3%). There were no postoperative infections or medical complications reported.

Forest plot for full endoscopy overall outcomes. ES, effect size.
Percutaneous Treatment
A total of 8 studies, including 497 patients (women = 57.8%, mean age = 63.2 years, range = 58.7–68.2 years), were identified. In all the studies examined, the JFC aspiration and rupture were attempted, and corticosteroids were locally injected. Five studies reported the caliber of the needle utilized for rupture and aspiration of cyst’s content. Four studies used a 22-gauge needle , while one used a 20-gauge needle. The most affected level was L4-L5 (69.5%), followed by L5-S1 (16.5%), L3-L4 (11.6%), and L2-L3 (2.4%). The average follow-up was 24.2 months (range 11–44.5 months). On average, hospital stay was less than 1 day. One study reported the proportion of patients with preoperative instability at the cyst level to be 3.9%.
Favorable outcome rate after percutaneous rupture and aspiration was 66.2% (95% CI 52.9%–78.4%) (Figure 5), while procedural adverse events rate was 0.1% (95% CI 0.0%–1.2%). There were 2 cases of cyst rupture and bleeding in the epidural space. The overall recurrence rate was 34.3% (95% CI 20.3%–49.6%), and among those, 60.7% required additional treatment (revision). Of the revision procedures, 47.3% underwent repeated percutaneous cyst aspiration and rupture, while 52.7 % underwent surgical excision by one of the above mentioned methods. The other recurrences were treated conservatively.

Forest plot for percutaneous fluoroscopic- or CT-guided overall outcomes. ES, effect size.
Outcomes and Adverse Events Comparison
Overall median time from JFC excision to recurrence, excluding patients undergoing concomitant fusion surgery, was 23 months (range 1–60 months; mean 23.6 ± 20.6 months). There were no statistically significant differences in overall satisfactory outcomes between patients undergoing open, minimally invasive, and full-endoscopic approaches (Table 3). Statistically, significantly lower satisfaction rates were found between open, minimally invasive, and full-endoscopic approaches and percutaneous cysts rupture and aspiration (P < 0.001). Higher recurrence rates were found among percutaneous cyst aspiration and rupture patients than open, minimally invasive, and full endoscopy ones (P < 0.001). No differences in overall recurrences rates were found between open and minimally invasive (P = 0.281), open and full-endoscopic (P = 0.072), and minimally invasive and full endoscopy (P = 0.612) procedures.
Summary of outcomes and adverse events for each treatment modality.
No differences in overall revision rates were found between open and minimally invasive (P = 0.606), open and full-endoscopic (P = 0.483), and minimally invasive and full endoscopy procedures (P = 0.334). Percutaneous cysts rupture and aspiration recurrences and revision rates were significantly higher than all other procedures (P < 0.001). No differences in postoperative instability rates were found between open and minimally invasive approaches (P = 0.806).
No differences in overall surgical adverse event rates were found between open and full-endoscopic procedures (P = 0.355) but higher rates between minimally invasive and open (P < 0.001) and full-endoscopic procedures (P = 0.001). As expected, procedural adverse events were significantly lower for percutaneous cysts rupture and aspiration than open, minimally invasive, and full-endoscopic procedures (P = 0.001).
In our subgroup analysis (patients with preoperative degenerative listhesis vs without preoperative degenerative listhesis), open and minimally invasive surgery was used more than full-endoscopic and percutaneous procedures among patients with preoperative degenerative listhesis (P = 0.001, respectively). We additionally found lower rates of satisfactory outcomes in patients with preoperative degenerative listhesis undergoing minimally invasive approaches compared to open surgical approaches (77.8% vs 92.7%, P < 0.001) but higher rates of adverse surgical events (31.3% vs 2.1%, P < 0.001) and of patients requiring revision surgery (13.1% vs 6.8%, P value = 0.042).
DISCUSSION
To the best of our knowledge, this is the most up-to-date systematic review and meta-analysis on outcomes and complications of lumbar JFC treatment. We estimated overall outcomes and adverse event rates for each surgical procedure, including percutaneous-guided cysts rupture and aspiration. We also stratified results based on preoperative spinal stability conditions. This was done to provide a better insight into JFCs treatment, especially for open and minimally invasive procedures.
Overall, we did not find significant differences in outcomes between open, minimally invasive, and full-endoscopic cysts excision but lower satisfactory rates in patients undergoing percutaneous cysts rupture and aspiration as well as higher recurrences and revision rates. After stratifying results between patients with and without preoperative degenerative listhesis, we found slightly lower satisfactory rates but higher intraoperative adverse events and revision rates in patients with degenerative listhesis at the cyst level. Revision and adverse event rates, mainly attributable to dural tears, were higher in patients undergoing minimally invasive surgery and carrying preoperative degenerative listhesis.
Laminectomy/Hemilaminectomy has shown satisfactory outcomes in approximately 90% of patients over 6 months of follow-up,6,29,37,44,46–48,50,52 though some patients still require concomitant fusion because of preoperative instability while others required subsequent fusion due to the development of postoperative instability.25,27,38,50
Cystectomy alone may be enough for back/leg pain relief in 90% of patients, at least initially. However, decompression alone in the presence of underlying segmental instability may predispose cyst recurrence.28,29,40,42 Of note, same-site recurrence was never reported in any patients receiving concomitant spinal fusion.6,40,41,52
JFC recurrence was higher in the laminectomy/hemilaminectomy patients than in patients undergoing fusion. Patients with preoperative degenerative listhesis have almost twice the risk of recurrence or revision surgery due to developing instability at the treated level.8,49 However, indiscriminate fusion might aggravate adjacent level degeneration53 while raising perioperative morbidity, extending hospital stay, and resulting in a higher risk of incidental durotomy and greater blood loss.25,27,32,54
Minimally invasive surgery aims to preserve the dorsal muscular and ligamentous attachments that are paramount for spinal stability.30,31,36,43 It has been shown to have successful outcomes over the short- and long-term in 95% of patients.43 However, the tubular approach is challenging and burdened with a higher risk of durotomy, epidural hematoma, and CSF leak in nonexperienced hands. This may be explained by the limited field of view and steep learning curve. Also, cysts adherent to the dural sheath can make dissection demanding.45 These factors may explain the higher revision and adverse event rates among patients with preoperative degenerative listhesis.
Eventually, full-endoscopic techniques have reported satisfactory outcomes in treating symptomatic JFC cysts in the vast majority of cases over a mean follow-up period of <24 months.22,23,35 However, it is clear from our analysis by the significantly lower percentage of patients with preoperative degenerative listhesis than open or minimally invasive approaches that endoscopic patients were carefully selected in each series.33 Full endoscopy, especially the transforaminal approach, is associated with milder surgical trauma,24 shorter operating time, negligible blood loss and CSF leakage, mild postoperative back pain, and shorter hospitalization time.13
New instruments (eg, shavers and diamond burrs) provide adequate bone resection and make cyst removal technically feasible,26 but the learning curve is steep, and appropriate training is paramount for success.39
The minimally invasive technique offers similar results compared to open surgery at the cost of slightly higher adverse event rates in patients with preoperative degenerative listhesis. A trend toward higher adverse event rates, particularly postoperative nerve roots paresthesia, is similarly reported by studies comparing minimally invasive to open lumbar surgery51. By pooling such a large number of patients in subgroup analysis, we were able to confirm this trend. Our minimally invasive group results reflect a higher challenging procedure in more degenerate segments, speculatively consequent to a limited field of view and surgical freedom (instruments) inside a narrowed space leading to significant nerve root traction and manipulation compared to open surgery. Similar results may have been found in the full-endoscopic groups; however, the procedure’s novelty and the stricter patient selection precluded most of the patients with degenerative degenerate segments at the cyst level to undergo endoscopy. It would be interesting to evaluate such occurrences in future analyses.
By comparison, full-endoscopic JFC excision is even less traumatic and more respectful of the articular process integrity.34 Indeed, the transforaminal approach allows root and foraminal decompression without compromising spinal stability and without scar formation developing.55 Thus, it is feasible to control symptoms even in mild spinal instability. Eventually, laminectomy/hemilaminectomy and fusion should be reserved in overt spinal instability cases or when total facetectomy is required for cyst excision (ie, in recurrent cases), while percutaneous cyst rupture and aspiration to patients not suited or unwilling to undergoing invasive procedures.
Limitations
The main limitation is the lack of individual patient data, which makes prognostic analysis subject to confounding bias and limits our ability to stratify outcomes. Findings may also have been impacted by inter- and intraobserver variability in assessing the prevalence of clinical improvement, especially regarding “excellent” and “good” outcomes.
Additionally, not all the studies report every outcome evaluated in this review. Although this may have impacted the results, every attempt was made to account for heterogeneity using statistical methods. Moreover, only 5 studies were estimated to have an elevated risk of bias. Additionally, it may be argued that those cases chosen to be treated with minimally invasive or full endoscopic procedures may not be the same as treated with a conventional open procedure. Also, there is an inherent bias in the studies pooled in the meta-analysis. Many of the studies, especially minimally invasive and endoscopic, may be biased toward those procedures, thus introducing a selection bias. However, we carefully evaluated the existing literature and relative methodological flaws to account for missing information and unanswered questions relating to JFCs treatment. Considering JFCs treatments’ heterogeneity, such an extensive analysis is virtually impossible without a meta-analysis process, which allows for group comparison. Therefore, the studies included in this meta-analysis were selected following a strict a priori established protocol, the literature search included multiple databases, and study selection was rigorous and based on the criteria established by the most recent guidelines. Eventually, in the meta-analysis, only studies with homogenous outcomes were included (objective and validated outcomes as described in the Methods section), excluding those who were uncertain or derived from a subjective surgeon evaluation.
CONCLUSIONS
Besides confirming the safety and efficacy of open and minimally invasive approaches, we highlighted how full endoscopy has outcomes, rates of adverse events, and operative times that overlap those of the open and minimally invasive approaches. We believe that the spine surgeon’s wealth of knowledge must include all of these techniques. These results may help the surgeon in the reasoning process of each case.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Financial Disclosures and Conflicts of Interest All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.