


Abstract
Background Bone morphogenetic protein (BMP) is a costly agent commonly used in spine surgery. Its effectiveness and complication profile have never been studied in a large, propensity-matched population following its approval by the Food and Drug Administration for use in single-level anterior lumbar interbody fusion (ALIF) surgeries.
Objective To investigate the rate of symptomatic pseudarthrosis or need for revision surgery after single-level stand-alone ALIFs with and without the use of BMP.
Methods Medicare Standard Analytic files derived from Medicare parts A and B were used to identify adult patients who underwent single-level ALIF procedures with and without use of BMP between 2004 and 2014. Patients were propensity matched based on their age, gender, and history of diabetes mellitus, hypertension, chronic kidney disease, body mass index greater than 30 kg/m2, smoking, rheumatoid arthritis, and osteoporosis. Sensitivity analysis using adjusted multivariate logistic regression models was also performed. The primary outcomes were the rates of symptomatic pseudarthrosis or need for revision surgery.
Results The propensity-matched population analyzed in this study contained 22,380 patients undergoing single-level ALIF (8971 [40.6%] with BMP and 13,139 [59.4%] without BMP). Both patient groups were balanced at baseline. The rate of symptomatic pseudarthrosis in the propensity-matched analysis was higher in the BMP group (1.9% vs 1.4%, P < 0.05). BMP use during single-level ALIFs was associated with 44% increased odds of developing pseudarthrosis (OR 1.44, 95% CI 1.16–1.76). However, there was no statistically significant difference in the rate of revision surgery between groups (3.7% vs 3.5%, P = 0.49).
Conclusions BMP use in single-level ALIFs may be associated with increased risk of symptomatic pseudarthrosis. Large prospective pragmatic trials are needed to corroborate our findings.
Level of Evidence 3.
INTRODUCTION
Arthrodesis is one of the most common approaches in the treatment of degenerative, infectious, traumatic, developmental, and neoplastic disorders of the spine. The failure of these interventions occurs, in part, due to nonunion or pseudarthrosis, which in turn results in symptomatic pain, deformity, spinal cord compression, or hardware failure.1,2 Efforts to reduce the rate of pseudarthrosis have been multifaceted, including implantable electrical stimulation devices, magnetic fields, and pulsed ultrasounds.3–5 Additionally, the use of substrates between vertebrae to create more permissive environments for fusion has been a common approach.6–11 Traditionally, autologous grafts, most commonly from the iliac crest, have been used; however, these types of grafts prolong surgery times, increase morbidity, and are specifically associated with hematoma, infection, fracture, and postoperative graft site pain.12–17 To reduce these mostly harvest-related complications, bone graft substitutes such as bone marrow aspirate, ceramics, mesenchymal stem cells, demineralized bone matrixes, and human recombinant bone morphogenetic protein (BMP) have been investigated as alternatives to iliac crest bone grafts (ICBGs).18–23 In 2002, the approval of recombinant BMP-2, a human cellular growth factor involved in the regulation of bone induction, maintenance, and repair, by the Food and Drug Administration (FDA) for use in single-level anterior lumbar interbody fusion (ALIF) was spurred by early studies demonstrating equivalent or improved fusion rates with no associated major complications. Despite its cost of $3500 to $5500, this approval demonstrated efficacy, and its favorable side effect profile led to use in up to 48% of all ALIFs performed nationally, including off-label use in many spine surgeries.6,8–11,24–29 Despite early research demonstrating BMP as a promising alternative to ICBG, several subsequent studies reported conflicting results, suggesting a range of efficacy spanning from inferior to equivalent rates of fusion when compared with ICBG. Other studies have demonstrated significant complications associated with BMP use, including bone resorption or remodeling, retrograde ejaculation, ectopic bone formation, hematoma, and seroma.30–41 To this end, we have undertaken a review of all of the cases in which BMP was used for the initially FDA-approved indication—single-level ALIFs—and compared outcomes to patients in which BMP was not used to determine the potential risks and benefits that might be associated with BMP use in Medicare beneficiaries.
METHODS
Data Collection
Medicare Standard Analytic files containing all inpatient and outpatient facility records billed to Medicare derived from Medicare parts A and B, which cover 51 million patients, from January 2004 to December 2014 were retrospectively analyzed. Patients undergoing single-level ALIF were identified based on International Statistical Classification of Diseases, 9th editiong (ICD-9), diagnosis codes, ICD-9 procedure codes, and current procedural terminology (CPT) codes.
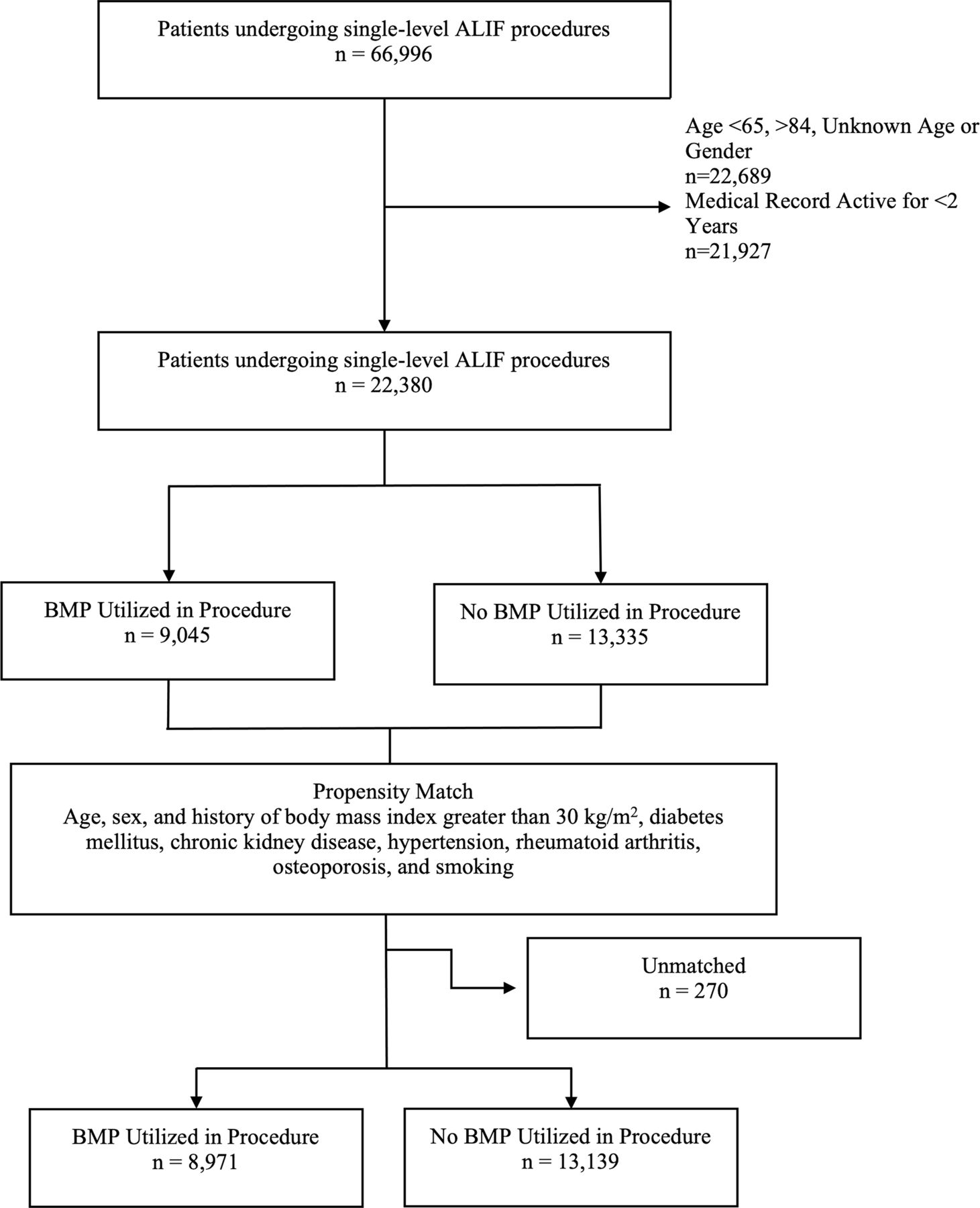
Patients undergoing ALIF were identified by querying the database for coincidence of the following CPT codes or ICD-9 Procedure Coding System codes: (1) CPT-22558 (anterior interbody fusion, lumbar) or ICD-9–81.06 (lumbar and lumbosacral fusion of the anterior column, anterior technique) and (2) CPT-22851 (application of intrabody device). Only patients undergoing single-level fusions were included in the study. Likewise, patients who received BMP were identified by the concurrent coding indicating its use, CPT-8452 (Figure 1).

Patient selection flow chart. ALIF, anterior lumbar interbody fusion; BMP, bone morphogenetic protein.
Comorbidities
Demographic data for aggregate records included sex and age. ICD-9-CM diagnosis codes were used to identify comorbidities as previously described and listed in Supplemental Table 1. Comorbidities were noted as follows: body mass index (BMI) greater than 30 kg/m2, diabetes mellitus, chronic kidney disease, hypertension, rheumatoid arthritis, osteoporosis, and smoking status.
Complications
Postoperative outcomes of pseudarthrosis and revision surgery were assessed at ≤2 years following surgery. ICD-9-CM codes used to identify these outcomes are listed in Supplemental Table 2.
Statistical Analysis
Descriptive statistics were calculated for age, sex, comorbidities, and postoperative outcomes. Sensitivity analysis using adjusted multivariate logistic regression models was performed to access factors that may be independently associated with pseudarthrosis and revision following ALIF. Patients undergoing single-level ALIFs with and without BMP were matched with the use of propensity score matching based on age, gender, and history of diabetes mellitus, hypertension, chronic kidney disease, BMI greater than 30 kg/m2, smoking, rheumatoid arthritis, and osteoporosis, as previously described.42 ,43
χ 2 tests were calculated to compare demographic data and comorbidities in each cohort. Odds ratios were calculated to compare pseudarthrosis and revision surgery based on BMP use. The data were analyzed using R statistical software (version 3.6.0, 2019, R Foundation, Vienna, Austria).
RESULTS
Descriptive Characteristics
Between January 2004 and December 2014, 22,380 Medicare beneficiaries between the ages of 65 and 84 years with benefit enrollment for at least 2 years underwent single-level ALIFs (Figure 1). The descriptive characteristics and outcomes of the total population are summarized in Supplemental Tables 3 and 4. The propensity-matched population analyzed in this study contained 22,110 patients split into 8971 (40.6%) patients undergoing single-level ALIF with BMP and 13,139 (59.4%) patients undergoing single-level ALIF without the use of BMP. The demographic distribution and postoperative complication rates are summarized in Table 1. The majority of patients undergoing ALIFs with and without BMP were women (n = 5733, 63.9% and n = 8370, 63.7%, respectively). The ages of patients in the BMP and no BMP groups were as follows: 3920 (43.7%) and 5388 (41.0%) between 65 and 69 years, 2766 (30.8%) and 4133 (31.5%) between 70 and 74 years, 1658 (18.5%) and 2536 (19.3%) between 75 and 79 years, and 627 (7.0%) and 1082 (8.2%) between 80 and 84 years, respectively.
Propensity-matched characteristics of patients undergoing single-level anterior lumbar interbody fusion surgeries.
The rates of BMI >30 (5.2% vs 5.4%, P = 0.52), chronic kidney disease (3.8% vs 4.0%, P = 0.46), rheumatoid arthritis (3.1% vs 2.8%, P = 0.24), osteoporosis (9.1% vs 8.6%, P = 0.26), and smoking status (9.5% vs 9.9%, P = 0.30) did not differ significantly between patients who underwent single-level ALIFs with and without BMP. Although the rates of diabetes mellitus (19.2% vs 21.4%, P < 0.05) and hypertension (51.3% vs 53.1%, P < 0.05) were found to be statically different, these differences were not likely of significant clinical importance (Table 1).
Postoperative Outcomes
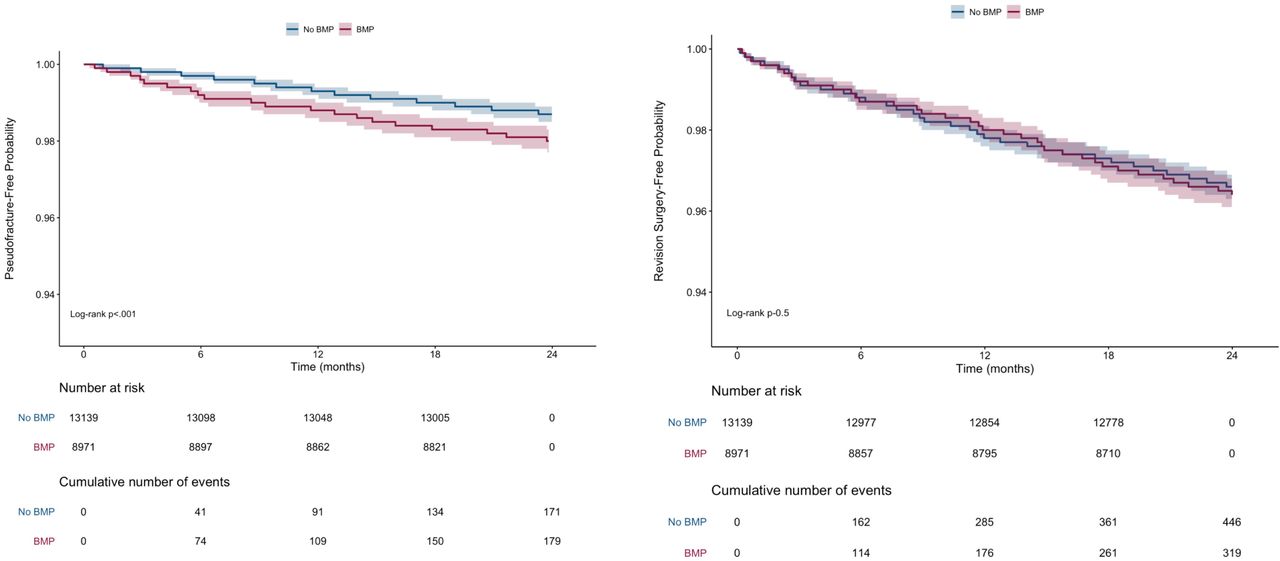
Although patients undergoing single-level ALIFs with BMP had statistically higher rates of pseudarthrosis (1.9% vs 1.4%, P < 0.05) and this difference trended toward statistical significance (log rank P < 0.001), the rates of revision surgery (3.7% vs 3.5%, P = 0.49) were not significantly different and did not trend toward statistical significance (log rank P = 0.5) (Table 1 and Figure 2).

Kaplan-Meier plot for pseudarthrosis and revision surgery occurring within 2 y postoperatively. BMP, bone morphogenetic protein.
The odds of developing pseudarthrosis (OR 1.44, 95% CI 1.16–1.76) were significantly higher among the BMP cohort. The odds of requiring revision surgery did not significantly differ between cohorts (OR 1.06, 95% CI 0.91–1.22) (Table 2). These effects were confirmed using multivariable regression testing (Supplemental Table S5).
Propensity-matched odds of complications among bone morphogenetic protein treatment cohort who underwent single-level anterior lumbar interbody fusion surgeries compared with the control cohort.
DISCUSSION
A retrospective analysis of a propensity-matched group of 22,110 patients undergoing ALIFs with and without BMP was performed. Patients who received BMP during their procedures had an overall significantly greater tendency for pseudarthrosis; however, they were found to not have a significant difference in their rate of revision surgery at up to 2 years following surgery.
Early studies of BMP use in ALIF and other approaches for lumbar fusion demonstrated greater fusion rates coupled with more favorable side effect profiles; however, some more recent studies have demonstrated no differences in fusion rates.1,6,7,9–11,28,32–37,44–55 In a systematic review of 4 prospective randomized control trials of patients undergoing single-level ALIF procedures with and without BMP, Galimberti et al’s analysis of 589 patients found a significant improvement in the rates of fusion in procedures using BMP compared with those without BMP at 2 years (OR 7.08, 95% CI 1.54–32.67, P = 0.01).7,8,10,39,46 Similarly, a meta-analysis of 19 prospective randomized control trials by Zhang et al of 1852 patients who received single-level ALIF with BMP or with ICBG found significantly increased fusion rates (relative risk [RR] 1.13, 95% CI 1.05–1.23, P = 0.001); however, they also found no difference in success of the clinical outcomes (RR 1.04, 95% CI 0.95–1.13, P = 0.38).56 Conversely, Manzur et al conducted a systematic review of 55 randomized and nonrandomized prospective, retrospective, and randomized control trials that reported fusion rates of single and multilevel ALIF with or without BMP and autograft vs allograft; this study found no significant difference in the pooled rates of fusion between the 3991 patients who underwent surgeries with and without BMP (94.4% vs 84.8%, P = 0.106).55 Likewise, a meta-analysis of 5 Medtronic-sponsored randomized control trials by Fu et al whose analysis included 416 patients undergoing single-level ALIF with BMP vs ICBG found no difference in the odds of fusion (OR 1.05, 95% CI 0.88–1.124, P > 0.05).36
Studies and case reports have found specific complications associated with BMP in ALIF such as radiculitis, heterotopic ossification, osteolysis, subsidence, soft tissue swelling, local inflammation, sterile cyst formation, and retrograde ejaculation. These adverse events were entirely unreported in the original 5 industry-funded studies promoting the safety and efficacy of BMP in ALIF; however, more recent literature has consistently demonstrated these complications are specific to or exacerbated with BMP use.49,57–67 The present study, which to the knowledge of the authors is the largest study on the topic, demonstrates a 1.44-fold increase in the odds of pseudarthrosis with the use of BMP. In addition, the rate of revision surgery was similar with and without the use of BMP, with no trend toward statistical significance (3.7% vs 3.5%, P = 0.49). The significant findings of our study may be attributable to the increased capture of adverse events by longitudinal administrative databases compared with clinical trials. These results add to the existing literature demonstrating a lower than previously described efficacy and significant side effect profile.
Global Impact of BMP’s Approval for Use in Spine Surgery
Initial data demonstrating the safety and efficacy of the use of BMP in ALIF procedures have spurred its increased use in many off-label indications. Some of these indications, though initially, have demonstrated some promise.6–9,11,26,28,44,54,60,68,69 Adverse events, like those that lead to the FDA to release a warning against BMP’s use in anterior cervical discectomy and fusion procedures, have warned against its use in some contexts.70 Furthermore, its off-label use in the lumbar spine in posterior, lateral, and oblique approaches and for multiple-level procedures has been controversial in the literature due to varying reports of its safety and efficacy in these contexts.6–11,27,34,35,44,50,55,56,71–74 Finally, taking the recently mounting evidence of lower than previously demonstrated efficacy, significant side effect profile, and significant costs associated with the use of BMP, its use should be more thoroughly evaluated not only in off-label uses in spine surgery but also in its approved use in ALIF surgeries.35,75,76
Limitations
There exist a number of limitations that should be considered in interpreting the results of our investigation. The administrative data found in this study were generated for financial and administrative use rather than clinical research purposes and therefore may vary in detail and accuracy. The application of ICD-9 codes may be subjective as they rely on an interpretation of physician records by the medical reviewer entering the codes and subject to changing coding practices. Notably, there is also no way to assess how pseudarthrosis was specifically diagnosed in our cohort. In order to assess the true rate of pseudarthrosis, a radiologic review would be necessary but is unable to be conducted on the database used. Moreover, we are unable to discern the exact indication, dose, and location of placement in regard to BMP. Of note, the appropriate indication and dose have been poorly specified historically, and dosing regimens may have varied throughout the study period as more literature has been published on adverse effects.30,36,37,40 Furthermore, we are unable to discern whether recombinant human bone morphogenetic protein-2 (hBMP-2) or osteogenic protein-1 (OP-1, also termed BMP-7) was used. These administrative data also do not provide qualifiable details on the severity of disease states (eg, spinal alignment), provide patient-reported outcome scores, or allow for standardization of treatment protocols or surgeon technique or expertise (eg, implant type and material), which may mask certain confounding factors. Finally, the use of propensity score matching is by no means a substitute for a prospective trial. While we sought to control demographic factors and comorbidities to the best of our abilities, the groups did vary significantly in regard to malnutrition (8.4% vs 7.9%, P = 0.03) and Elixhauser Comorbidity Index (6.86 vs 6.79, P = 0.046). These differences were not determined to be clinically significant. While these aforementioned limitations should be carefully considered, we believe the results of our investigation add to the current body of literature pertaining to the use of BMP and pose interesting further areas of research that may be investigated through prospective trials.
CONCLUSIONS
BMP use in single-level ALIFs may be associated with increased risk of symptomatic pseudarthrosis, and no improvement in the rate of need for revision surgery. In addition, its great cost may further depreciate its utility. Large prospective pragmatic trials are needed to corroborate our findings.
Supplementary material
TABLE S1.
TABLE S2.
TABLE S3.
TABLE S4.
TABLE S5.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosure The authors report no financial disclosures related to this article.
IRB Approval The present study was deepend to be exempt from institutional review board review by our institution
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.