


Abstract
Background Although it is well established that surgically treated patients with cervical degenerative myelopathy (CDM) improve irrespective of the anterior decompression technique used, no consensus exists on what technique is superior in terms of neurological recovery. A general concern exists that anterior cervical discectomy with arthroplasty (ACDA) leads to less favorable outcomes in CDM due to microtrauma caused by preserved mobility. It is remarkable that current literature mainly uses pain scores to assess clinical outcomes after anterior decompression surgery, especially considering that pain may not be the most relevant outcome for CDM. This systematic review evaluated the literature concerning neurological outcomes in patients with CDM treated with anterior decompression surgery and assessed by validated myelopathy scores.
Methods Systematic searches were carried out in PubMed, EMBASE, Web of Science, CINAHL, and the Cochrane Library. Prospective studies were included when patients with isolated CDM were treated with anterior decompression surgery, and a validated myelopathy outcome score was used.
Results A total of 11 studies were included from the 16,032 identified studies. All studies used the modified Japanese Orthopedic Association (JOA) outcome score and showed improvement for all anterior techniques. The mean improvement in anterior cervical discectomy and fusion (ACDF) was 4.80 and 3.64 for the modified JOA and JOA outcome scores, respectively. The JOA for ACDA showed a mean improvement of 5.51. The overall quality of the included articles was low to moderate according to the Cochrane tool.
Conclusion Neurological recovery of CDM is similar after all anterior decompression techniques, including ACDA when compared with ACDF.
Clinical Relevance The current literature gives no reason to dissuade the use of ACDA in cervical myelopathy.
Level of Evidence 3.
- cervical spine
- myelopathy
- cervical degenerative disc disease
- cervical arthroplasty
- anterior cervical discectomy and fusion
- systematic review
- cervical disc replacement
INTRODUCTION
Surgical decompression of the spinal cord is recommended for patients with symptomatic cervical degenerative myelopathy (CDM).1 However, the optimal surgical strategy and timing for management of CDM remain controversial. Many studies report clinical outcomes of anterior cervical decompressive surgeries for cervical degenerative disc disease (CDDD) in terms of pain or disability induced by pain. Whereas cervical degenerative radiculopathy (CDR) predominantly presents with neck and/or arm pain, CDM clinically manifests with neurological deficits such as paresthesia, sensory dysfunction, paresis, disturbed proprioception, gait disturbances, decreased hand dexterity, and hyper-reflexia.2 Pain may thus not be the most relevant outcome measure for the majority of patients with CDM.
Surgical decisions are based on pathology, clinical presentation, location of compression, sagittal alignment, and patient-specific factors.3 However, surgical decision-making seems to be strongly dependent on country, center, and surgeon, mainly based on experience. One of the most common treatment options for patients with single- or multilevel CDDD is anterior cervical discectomy with fusion (ACDF) or, in Europe, without anterior cervical discectomy.4 Good short-term clinical results are achieved with both techniques in 90% to 100% of the patients with radiculopathy.5 This has also been described for myelopathy, where postoperative improvement was both statistically and clinically significant.6 A drop in patient satisfaction at long-term follow-up is described in multiple studies.7–9 This is thought to be due to the development of clinical adjacent segment pathology (CASP), which is defined as the development of new radiculopathy and/or myelopathy at a segment adjacent to the site of the previous surgery. Adjacent segment pathology has been postulated to be accelerated by loss of motion in the fused segment, thereby overstraining the adjacent segments. Both techniques result in a high rate of fusion, 70% to 80% for anterior cervical discectomy and 95% to 100% for ACDF, possibly increasing the risk on adjacent segment pathology.5
Anterior cervical discectomy with arthroplasty (ACDA) is thought to reduce the chance on developing CASP by preserving motion in the operated segment.10 Several studies have investigated the clinical outcomes of ACD(F) compared with ACDA in CDDD and found no significant differences in terms of pain, disability, and quality of life.11,12 One can reason that no differences in clinical effectivity are expected as all techniques equally aim for adequate decompression of the neurological tissue, resulting in similar neurological recovery. Still, long-term follow-up results show significantly lower rates of subsequent surgery due to CASP in ACDA compared with ACD(F), suggesting a potential higher long-term effectivity.13–17 In contrast, there is a concern that motion preservation may provoke microtrauma to the spinal cord in patients with CDM and negatively affects the clinical recovery after ACDA.11,18,19 However, this has not been confirmed by studies evaluating the outcomes for patients with CDR in comparison with CDM for both ACDA and ACD(F). Additionally, none of these studies describe a single patient with deterioration of neurological function when treated with ACDA for CDM.11,20
The majority of studies focus on mixed populations of CDR and CDM patients using the same outcome measures for clinical effectivity, like the visual analog pain scale (VAS) and Neck Disability Index (NDI), for both groups.21–25 It is remarkable that current literature mainly uses these pain scores to assess clinical outcomes, especially as pain may not be the most relevant outcome for CDM.
Therefore, this systematic review aims to evaluate neurological outcomes of anterior decompression surgery for patients with isolated CDM as assessed by validated myelopathy scores. The quality of the included studies will be determined.
MATERIALS AND METHODS
Review Protocol
This systematic review was executed in accordance with the preferred reporting items for systematic reviews and meta-analyses statement.26,27 The study protocol was published in the PROSPERO database (registration number CRD42020153495) before the study commenced.
Search Strategy and Eligibility Criteria
Searches for clinical studies were systematically carried out in PubMed, EMBASE (OVID), Web of Science (Clarivate Analytics), CINAHL (EBSCO), and the Cochrane Library (CENTRAL). The search was conducted without using search limiters. The initial search was conducted on 10 October 2019 and finally updated on 24 November 2020 (Appendix A). Studies were included if they met all of the following eligibility criteria: (1) prospective randomized controlled trial or cohort, (2) patient population with isolated CDM or separate reporting of CDM or CDR patients, and (3) presence of a validated myelopathy outcome score. Studies were excluded if (1) patients with myeloradiculopathy were considered as a single population, (2) the follow-up time was shorter than 1 year, (iii) anterior and posterior techniques were compared, (3) less than 10 CDM patients were included, or (4) patients with a diagnosis of rheumatologic disease, ossification of the posterior longitudinal ligament, diffuse idiopathic skeletal hyperostosis, ankylosing spondylitis, or Klippel-Feil or neurological compression due to infectious, traumatic, or oncologic pathology.
Study Selection and Data Collection
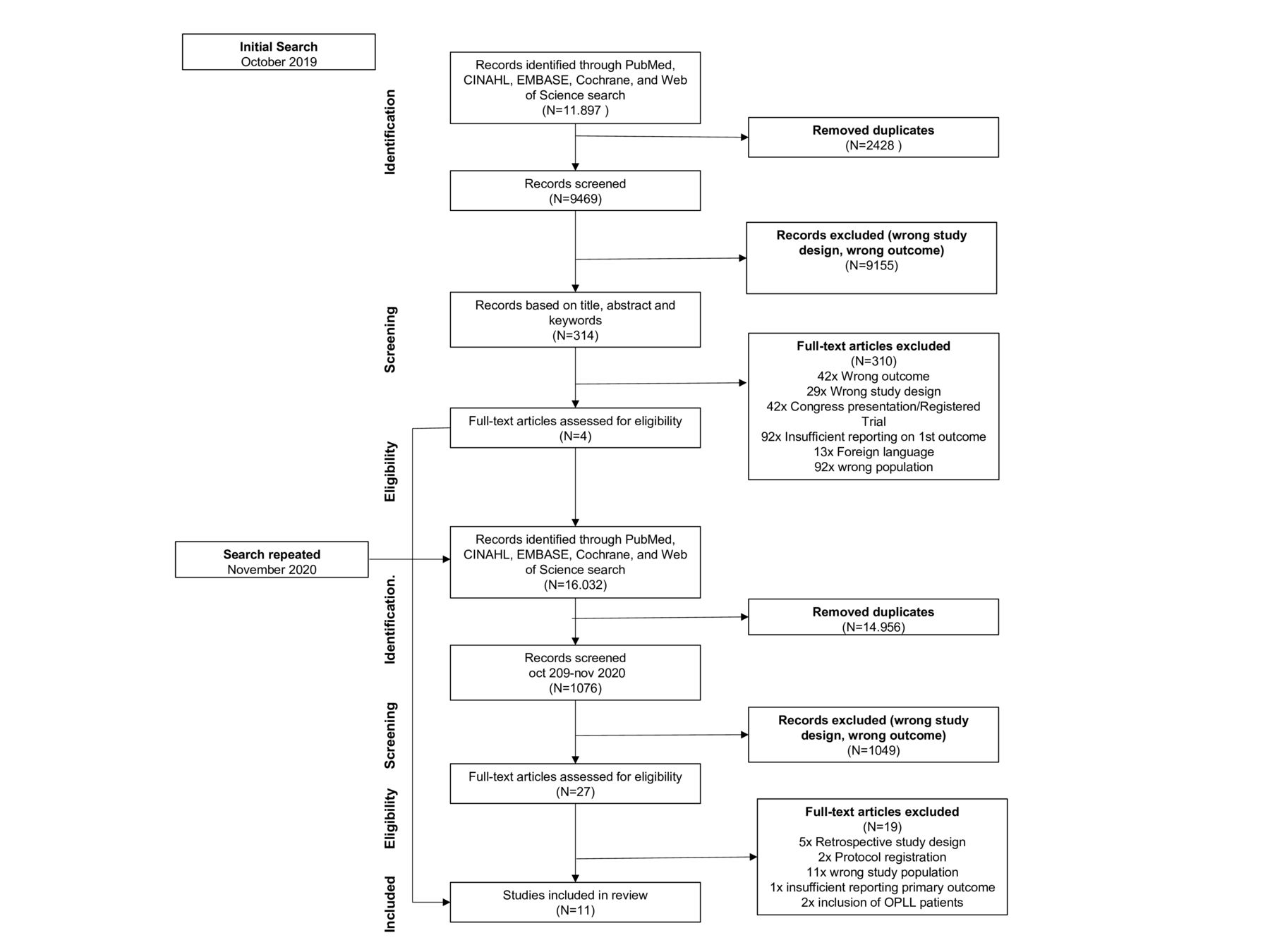
The study selection process is reflected in the Figure. Duplicates were removed, and articles were screened based on title and abstract. The abstracts were assessed by 2 independent researchers (V.S., A.S.) blinded for each other’s decision. If necessary, consensus was reached with assistance through discussion or with assistance of a third independent researcher (H.V.S.). The assessment was performed using Rayyan—a web and mobile app for systematic reviews.28 The following data were extracted from the included articles: study design, year of publication, country, time span, number of patients, baseline characteristics of patients, type of interventions, and primary and secondary outcome measures as described above. The complete data collection sheet is outlined in Appendix File B.

Preferred reporting items for systematic reviews and meta-analyses flowchart of inclusion process.
Quality Assessment
Risk of bias was assessed by 2 independent researchers (V.E.S., L.G.C.V.D.K.), blinded for each other’s decision. Consensus was reached through assessment by a third independent researcher (S.M.M.H.). Randomized controlled trials were assessed through the Cochrane Risk of Bias tool in Review Manager 5.3.29 Nonrandomized controlled trials were assessed with the Risk of Bias in Nonrandomized Studies of Interventions tool.30 The full risk of bias assessment sheet is outlined in Appendix File C.
Statistics
Heterogeneity was assessed with the χ 2 test in Cochrane Collaborations Review Manager version 5.3.31 Descriptive statistics were used and reported in a narrative summary according to the Cochrane handbook.29 The measures of treatment effect are determined through the mean difference or standardized mean difference and ranges for continuous data.
RESULTS
Study Selection
The initial systematic search (October 2019) in the databases yielded 11,897 articles, 9469 of which remained after removal of duplicates. A total of 4 articles met inclusion criteria. The systematic search was repeated in all databases (November 2020) and yielded a total of 16,032 articles, of which 1076 remained after duplicate removal and removal of duplicate articles from the initial search. Of these, 27 articles were screened on full text. This led to the inclusion of an additional 7 articles, which resulted in a total of 11 studies.32–43 A flowchart of the selection process is presented in the Figure.
Study Characteristics
Table 1 displays the characteristics and results of the included studies. Two randomized studies directly compared ACDA and ACDF.32,33 One study compared ACDF with corpectomy,37 and 1 study compared ACDF with a novel distraction technique.36 The remaining 7 studies reported on cohorts; 3 included ACDF patients,41–43 2 included ACDA patients,34,35 and 1 included corpectomy patients.38 Publication years ranged from 200737 to 2020.36,38,42,44 Follow-up time ranged from 136,40,41 to 5 years.44 Six studies were performed in China,32,33,35,36,39,40,43 1 in India,41 and the remaining 4 in Europe (Italy, Turkey, Germany, and Greece).34,37,38,42 Six of the studies determined neurological outcomes according to the Japanese Orthopedic Association (JOA)32–36,40 and 5 according to the modified JOA (mJOA),37,38,41–43 1 study additionally reported Nurick grades.41 JOA and mJOA scores will be reported separately as it is not advised to use them interchangeably.45
Results of included studies.
Study Results
The I 2 test revealed a heterogeneity of >75% for both JOA and mJOA, a meta-analysis was thus not performed.
All studies showed general postoperative neurological improvement, according to the (m)JOA, for all groups, with all of the evaluated techniques (Table 1). One study reported a statistically significant higher improvement for the ACDA group in comparison with the ACDF group; however, this difference was not clinically relevant.33 The baseline JOA and mJOA scores for ACDF were 8.5 (range 7.5–9.0) and 12.0 (range 10.8–12.4), respectively. The JOA for ACDF improved with 4.8 points to an average postoperative score of 14.6. The mJOA for ACDF improved with 3.6 points to an average postoperative score of 15.6. In the ACDA group, the JOA was 10.4 (range 7.4–14.0) at baseline. The JOA for ACDA increased with an average increase of 5.5 points to a postoperative score of 15.9 (range 15.2–16.6). The improvement in JOA scores was, therefore, higher in ACDA than ACDF. The reported ranges reflect a high degree of heterogeneity in the baseline neurological functioning of the included groups.
Secondary outcome measures are presented in Table 2. Four of the included studies assessed pain using the VAS.32,34,43,46 An overall decrease in VAS for neck and arm pain combined was reported in all studies with an average decrease of 1.6 for ACDF and 4.0 for ACDA. Additionally, 4 studies32–34,43 reported outcomes in terms of NDI. For ACDA, a decrease from 42.0 at baseline (range 36.7–50.6) to 6.4 postoperative (range 1.7–7.1) was reported. For ACDF, a decrease from 32.4 (range 9.7–50.1) at baseline to 7.96 (range 2.8–7.0) at postoperative follow-up was reported. Again, the ranges show a large heterogeneity in the reported baseline NDI scores.
Secondary outcomes.
The intent was to evaluate reoperation and complication rates. However, only 2 studies reported on complication rates,33,35 and no studies reported on reoperation rates. This was similar to quality of life, which was only assessed in 1 study.47 The complete data collection sheet is presented in Appendix File B.
Quality of Identified Studies
The studies included were critically assessed using the Cochrane risk of bias tool. According to the criteria for randomized trials, the overall risk of bias was moderate, and according to the criteria for nonrandomized trials (Risk of Bias in Nonrandomized Studies of Interventions), the overall risk of bias was considered low (Appendix File C).
DISCUSSION
The main aim of this review is to evaluate the functional and neurological outcome in patients with isolated symptoms of myelopathy after anterior decompression surgery for CDDD.
Few prospective studies focus on anterior decompression surgery for isolated CDM, even fewer use a validated myelopathy outcome score. A significant number of studies on the subject have been published by the end of 2019 and in 2020, as was discovered when the search was repeated in November 2020. This shows a growing interest in research about the neurological outcome of these surgical techniques for CDM.
The majority of studies were excluded because of the use of VAS and/or NDI as the primary outcome measure. Another prominent reason for exclusion was the inability to retrieve outcome results for CDM patients separately, as studies included a mixed population of CDR and CDM patients.
The available studies that primarily investigate CDM in anterior decompression surgery with validated myelopathy scores are often retrospective, have a short follow-up time, or have small sample sizes.19,48–51
Of the 11 included studies, only 2 were comparative studies, and the overall quality of the studies was low to moderate. Moreover, for most of the included studies, a validated myelopathy score was used but not as the primary outcome measure. This makes the study design suboptimal for the evaluation of neurological recovery. This shows that there is inadequate literature on neurological recovery in CDM patients, which limits the extrapolation of solid conclusions.
Overall differences in (m)JOA scores between the anterior decompression techniques were minimal and not clinically relevant. A remarkable heterogeneity was observed between the included studies at baseline. Reported (m)JOA, but also secondary outcomes such as VAS and NDI varied strongly. This reflects a variation in baseline population studied, especially in the severity of myelopathy. The average age between study populations was rather homogenous, but wide ranges and standard deviations are reported. Most studies included single- and multilevel surgeries, and 2 studies assessed single-level surgery only (Table 1). Besides the heterogeneity in baseline characteristics, the extent of improvement from pre- to postoperative also varied strongly between studies. This may be the consequence of the discrepancy in patient populations, despite the strict inclusion criteria of this review.
The lack of a clinically significant difference between outcomes is not surprising since all techniques aim to reach adequate decompression of the spinal cord.12 As neurological recovery after anterior decompression surgery for CDM was similar for all groups, the concern that ACDA is inferior to ACDF for the treatment of CDM is contradicted.52,53 Although clinical effectivity between techniques is similar, it may be possible that there is a difference in cost-effectiveness.
This systematic review was executed in accordance with the preferred reporting items for systematic reviews and meta-analyses statement. A large number of studies were reviewed, which makes bias due to missing data less likely. The study protocol was published online before the start of the study to ensure transparency. The main limitation of this systematic review is the inclusion of only full text and published studies but not conference proceedings, PhD dissertations, or gray literature. However, we do not expect that large trials and important studies on the subject remain unpublished and thus estimate a limited influence on our results.
CONCLUSION
Neurological recovery after anterior decompression surgeries in patients with CDM is equal for all decompression techniques in this systematic review. The lack of high-quality research about neurological recovery for patients with isolated myelopathy, assessed by validated myelopathy scores, is remarkable. To further establish the long-term neurological recovery in CDM patients for anterior decompression techniques, future studies should have an adequate follow-up duration and use a validated myelopathy score as the primary outcome measure.
Supplementary material
Appendix A
Appendix B
Appendix C
Acknowledgments
We would like to thank Mrs. Marion Heymans, medical information specialist, for her assistance in optimizing the search strategy.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article. All authors gave final approval to the version to be published.
Declaration of Conflicting Interests The authors report no conflicts of interest or financial disclosures with respect to the research, authorship, and/or publication of this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.