


Abstract
Background Three-dimensional (3D)-navigation in minimally invasive transforaminal lumbar interbody fusion (MI-TLIF) is an evolving procedure. It is used not only for its accuracy of pedicle screw fixation but also for other major steps in transforaminal lumbar interbody fusion. Multimodal outcomes of this procedure are very limited in the literature. The purpose of this study was to examine the application of 3D-navigation in minimally invasive transforaminal lumbar interbody fusion (MI-TLIF).
Methods Patients who underwent single-level MI-TLIF using 3D-navigation between January 2017 and July 2019 were evaluated for navigation setting time, radiation exposure, volume of nucleus pulposus excised, cage placement, accuracy of pedicle screw placement, and cranial facet-joint violation.
Results One hundred and two patients with a mean age of 60.2 years met the inclusion criteria. The mean presetting time of navigation was 46.65 ± 9.45 minutes. Radiation exposure, fluoroscopy use, and fluoroscopy time were 15.54 ± 0.65 mGy, 4.43 ± 0.87 Gy.cm², and 97.6 ± 11.67 seconds, respectively. The mean amount of nucleus pulposus excised from all quadrants was quantified. The cage was centrally placed in 87 patients, with 95.4% showing a Grade 0 pedicle breach and 94.6% showing Grade 0 cranial facet-joint violation.
Conclusion Registration and setting up 3D-navigation takes additional time. The amount of exposure to the patient is much less compared to routine computed tomography, and, importantly, the operating team is protected from radiation. Navigated MI-TLIF has high rates of accuracy with regard to placement of percutaneous pedicle screws and cages with the added advantage of protection of the cranial facet-joint.
Level of Evidence 5.
- lumbar spine
- minimally invasive spine surgery
- transforaminal lumbar interbody fusion
- 3D-navigation
- spinal navigation
INTRODUCTION
Minimally invasive transforaminal lumbar interbody fusion (MI-TLIF) is a well-established procedure and has several advantages.1–3 To a large extent, the entire operation is image guided. The most common image-guidance tool utilized is fluoroscopy, which is 2-dimensional (2D) in nature. This may result in increased radiation exposure4 and misplacement of implants5,6 with consequent complications. It is also associated with a high likelihood of contamination that may result in wound infections.7 Furthermore, delivery of poor-quality images is a major limitation of 2D-fluoroscopy in obese patients because of weak penetration. Coincidently, a majority of patients in need of this procedure are obese due to limited walking and lack of exercise as a result of neurogenic claudication. Situations such as rotated spine in degenerative scoliosis, poor anatomy on fluoroscopy, and asymmetric and abnormally shaped pedicles can deceive the operating surgeon, resulting in incorrect placement of pedicle screws and cages.8 Evidence shows high rates of unacceptable cranial facet-joint violation with fluoroscopy and 2D-navigation.5,6 Intraoperative 3-dimensional (3D)-navigation provides images in all planes like computed tomography (CT) and plays a dominant role in circumventing the challenges described previously. Studies that have examined the role of 3D-navigation in MI-TLIF show promising results, but they are hindered by small patient data sets.9 Although precise and safe insertion of pedicle screws is the foremost application of 3D-navigation, there are several other applications and features that need analysis. The authors ventured to assess the impact of 3D-navigation in MI-TLIF by evaluating (1) navigation setting time, (2) radiation exposure, (3) volume of nucleus pulposus excised, (4) cage placement, (5) accuracy of pedicle screw placement, and (6) cranial facet-joint violation.
MATERIALS AND METHODS
A prospective study of 117 consecutive series of patients who underwent single-level lumbar MI-TLIF with 3D-navigation operated by a single spine surgeon between January 2017 and July 2019 were evaluated. Among 117 patients, 6 patients were lost to follow-up and navigation registration failed in 9 patients. Therefore, 102 patients were included in the study. Institutional ethical committee approval was obtained. Patients were selected for MI-TLIF based on preoperative clinical findings, radiographs, and magnetic resonance imaging studies (Table 1). The study group had 44 men (n = 44) and 58 women (n = 58) with an average age of 60.2 years (46–74 years) with single-level pathology. The patients with degenerative scoliosis (4%) as an indication had a focal-level involvement and underwent a selective single-level fusion. Patients with a previous history of spine surgery at the respective level and traumatic and infective etiology were excluded from the study.
Indications for surgery.
3D C-arm (Siemens Arcadis Orbic3D) was used to retrieve the images. These images were uploaded onto the Stealthstation using synergy (S-7) software (Medtronic, Minneapolis, USA). Transforaminal lumbar interbody fusion (TLIF) was performed using a rigid 22-mm diameter tubular retractor (METRx tubular retractor system, Medtronic Sofamor Danek, Memphis, TN, USA). The percutaneous pedicle screw-rod systems utilized belonged to various sources such as Sextant (Medtronic Sofamor Danek, Memphis, TN, USA), Zimmer Biomet (PathFinder NXT pedicle screw system, USA), Globus Medical (Revolve, England), and Jayon (MIS Monolock, India).
Surgical Technique Under 3D-Navigation
The patients were positioned prone on a radiolucent table under endotracheal general anesthesia. The navigation reference frame was docked on the adjacent spinous process (usually one level above). The 3D C-arm was triggered to spin around the patient and the procured images were formatted into images in all planes (sagittal, coronal, and axial). These images were then transferred to the Stealth monitor. The Stealth camera can detect and track anatomy using infrared rays to whichever part or instrument the tracker is attached and registered to. As a first step, following verification, a navigated Jamshidi needle was registered and tracked to the optical system. Then pedicle cannulation was performed using real-time visualization in all 3 planes. Percutaneous guide wires were then passed into the pedicles through the Jamshidi needle. Using the Wiltse approach and with the help of the initial navigated and successive serial dilators of increasing diameters, the tubular retractor (22-mm diameter of adequate length) was accurately docked on the lamina-facet complex. The surgical microscope was moved into the field and decompression and interbody fusion was performed through the tubular retractor with variations in the operative steps as per the demands of the indication. Discectomy and disc space preparation was performed with the help of disc forceps, Kerrison rongeurs, bayonetted curettes, and rotating endplate shavers.
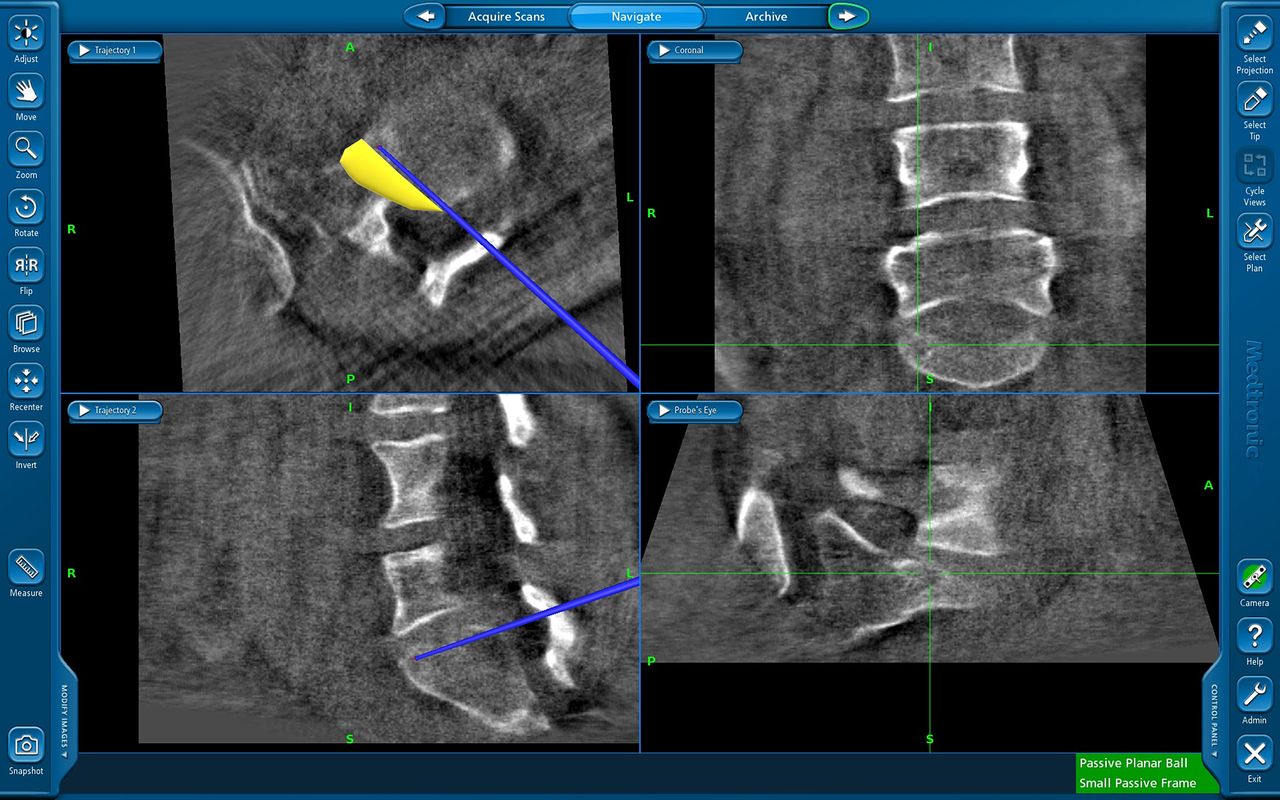
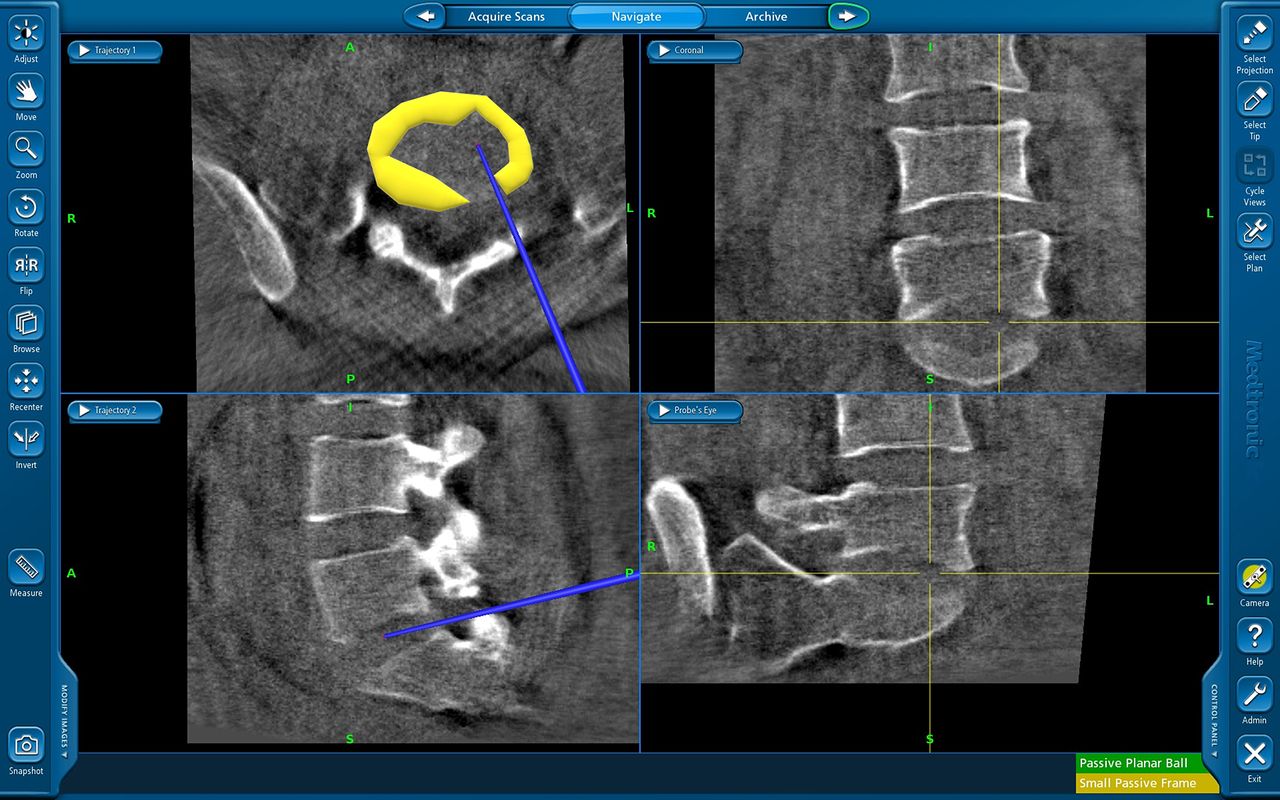
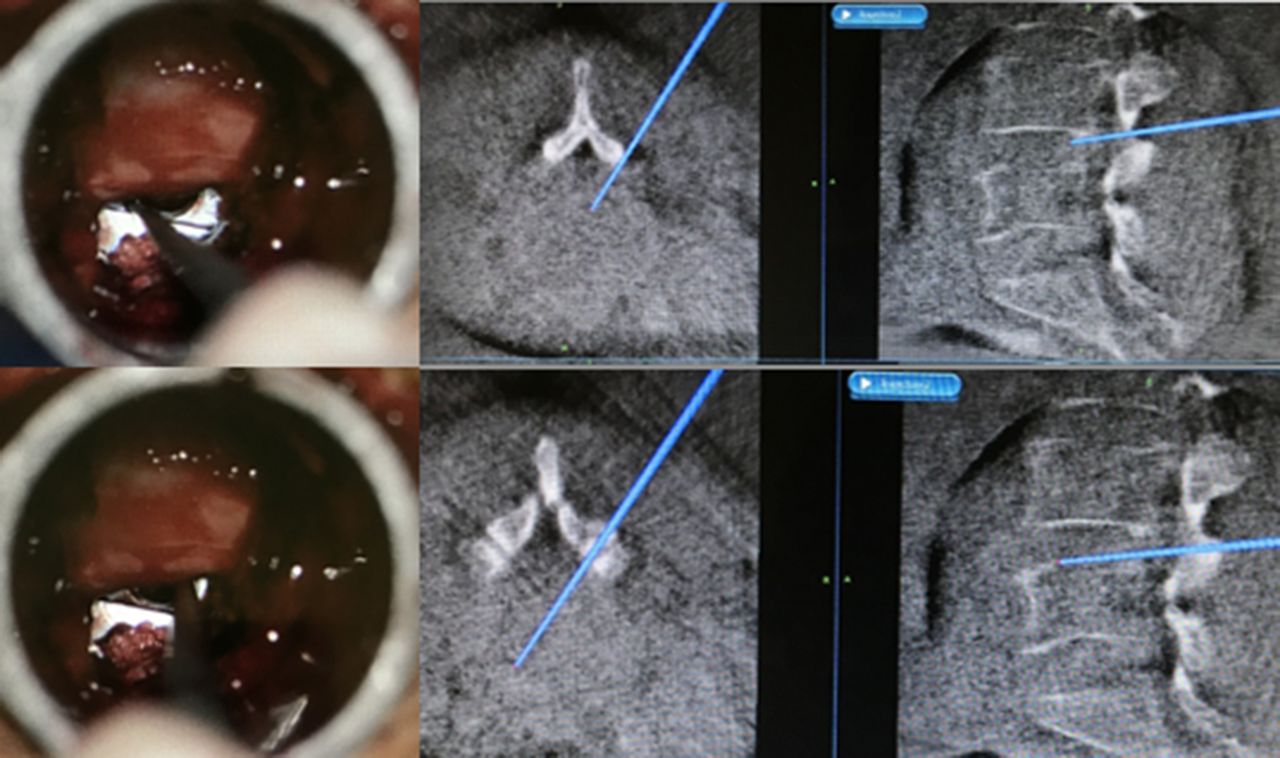
The completeness of excision of the intervertebral nucleus pulposus and cartilaginous endplate was evaluated by introducing the navigation array probe in all directions: contralateral posterior (Figure 1), contralateral anterior (Figure 2), ipsilateral anterior, and ipsilateral posterior10(Figure 3). The superior and inferior endplates were grated in all possible trajectories. The size and position of the cage to be placed was calculated using calibration applications on the Stealth monitor. Interbody fusions were performed using a titanium or polyetheretherketone cage and an autograft, the cage being precisely positioned with navigation assistance. The autograft consisted of local bone obtained from total facetectomy and laminotomy. Percutaneous pedicle screws were inserted using navigation assistance (ie, a tracker was attached to the handles of the tap and the pedicle screwdriver) over the preinserted guide wires (Figure 4). Once all the pedicle screws were inserted, rods were introduced to connect the screws on each side and segmental compression was achieved under fluoroscopy guidance. The wound was then closed in layers. The navigation array probe was utilized to verify the adequacy of decompression and to confirm the anatomical landmarks when necessary. A repeat 3D C-arm spin prior to extubation of the patient was performed to verify the position of the implants in doubtful situations.

Contralateral posterior quadrant where yellow margin indicates intact annulus fibrosis with remnant nucleus pulposus and blue navigation probe restricts beyond the annulus fibrosis.

Contralateral anterior area where nucleus pulposus is removed and rechecked with the navigation array probe.

Overall removal of the nucleus pulposus area with intact marginal annulus fibrosis.

Final position of all the pedicle screws in the navigation screen.
The methods to determine total navigation setting time, radiation exposure, volume of nucleus pulposus excised, cage placement, pedicle screw breach, and cranial facet-joint violation are as follows:
Total navigation setting time: The timings were noted from initializing the 3D C-arm, the navigation console, the integration of both, and the placement of the reference frame on the spinous process to registration after draping and painting.
Radiation exposure: Radiation exposure details from the C-arm (Siemens Arcadis Orbic3D, Bloomfield, USA) were noted. The parameters measured were cumulative radiation exposure (mGy), dose area product (Gy.cm2), and radiation time.
Volume of nucleus pulposus excised: Following disc space preparation that included discectomy and curettage of the cartilaginous endplates, a navigation array probe was used to assess the depth, width, and height of the nucleus pulposus emptied on the ipsilateral and contralateral sides of the corresponding level. The probe was used to feel the superior and inferior endplates in all trajectories which were verified on the monitor to confirm adequate and thorough cartilagenous endplate denudement. Later, the total volume of the emptied nucleus pulposus was calculated with digital imaging software (ImageJ, U.S. National Institutes of Health, Bethesda, MD).
Cage placement: Cage placement was determined using postoperative axial CT sections.
Pedicle screw breach: Screw placement was evaluated on the axial and sagittal sections of the CT scan and checked for any cortical breach. Pedicle screw breaches were assessed using the Gertzbein and Robbins scale.11
Cranial facet-joint violations: Cranial facet-joint violations of the pedicle screws were noted and classified according to Babu et al12 on the postoperative CT axial views.
In all cases, the postoperative CT scans were analyzed by a spine fellow and a certified radiologist. Placement of cage, pedicle screw breach, and cranial facet-joint violation were categorized as per the respective classifications. Statistical analysis was performed to examine interobserver reliability.
RESULTS
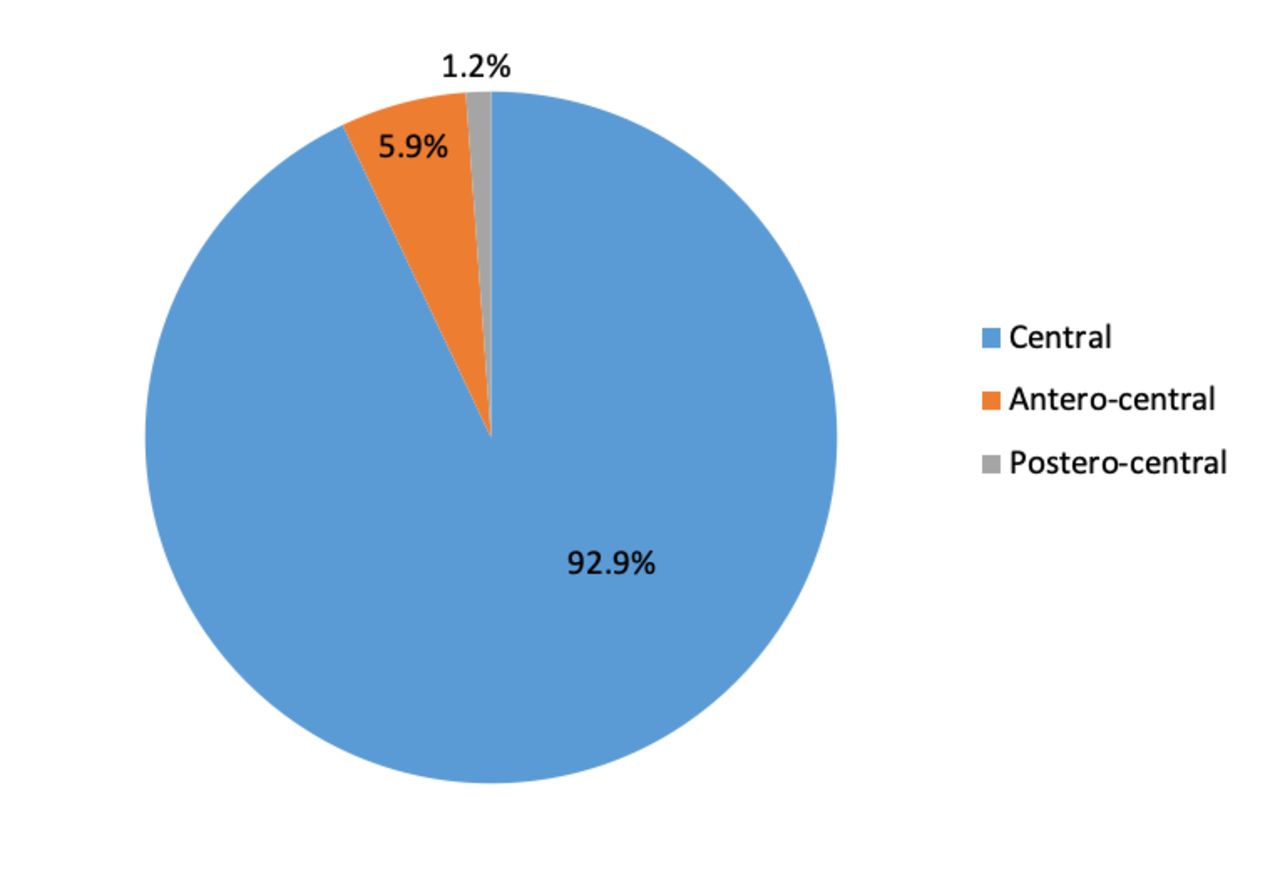
The current study included a total of 408 pedicle screws implanted in 102 patients. The number of patients undergoing MI-TLIF with 3D-navigation on corresponding levels were L2-L3 = 3, L3-L4 = 15, L4-L5 = 57, L5-S1 = 27. The mean navigation setting time from initializing the 3D C-arm to docking of the navigation reference array on the spinous process followed by registration was 46.65 ± 9.45 minutes. The mean time for the first 45 patients and the next 57 patients were 54.54 ± 6.23 minutes and 38.76 ± 9.54 minutes, respectively. The mean amount of radiation exposure was 15.54 ± 0.65 mGy. The mean time for fluoroscopy usage was 97.6 ± 11.67 seconds and the mean amount of radiation from fluoroscopy was 4.43 ± 0.87 Gy.cm². The amount of nucleus pulposus removed was 75% in the ipsilateral anterior quadrant, 81% in the ipsilateral posterior quadrant, 63% in the contralateral anterior quadrant, and 43% in the contralateral posterior quadrant (Figure 5). The cage position was central in 87 patients, contralateral anterocentral in 6 patients, and ipsilateral posterocentral in 8 patients, respectively (Figure 6). The Cohen’s kappa statistic test for interobserver correlation was 0.92 for the 2 examiners in regard to cage placement. Progressive posterior cage migration was noticed in a patient with initial posterolateral placement of the cage and this was corrected. The mean intraoperative blood loss was 89.65 ± 23.67 mL. Pedicle screw breach was graded as Grade 0 and Grade 1 in 95.4% and 4.4% of patients, respectively (Table 2). Again, 94.6% and 5.4% of pedicle screws demonstrated Grade 0 and Grade 1 cranial facet-joint violation, respectively (Table 3). In one case, a Grade 3 pedicle screw breach occurred. This was suspected intraoperatively while examining the C-arm images and confirmed by spinning the 3D C-arm again and extracting images before extubating the patient. This was probably due to a technical error and was immediately corrected. This was the same patient whose cage had migrated posteriorly, which had to be corrected. Postoperatively, the patient had paresthesia in the foot over L5 dermatomal distribution and weakness in ankle dorsiflexion. While the foot weakness resolved completely after 3 months, the paresthesia resolved only partially, and at their last follow-up, the patient complained of allodynia. The Cohen’s kappa statistic test results in regard to pedicle screw breach and cranial facet-joint violation were 0.889 and 0.878, respectively, which demonstrated high reproducible accuracy.

Percentage of disc space removed for cage placement by quadrant.

Position of cage placement.
Incidence of pedicle screw breach among the patients.
Incidence of cranial facet-joint violation among the patients.
DISCUSSION
In this prospective study, the authors analyzed the applications of 3D-navigation in MI-TLIF at various critical intraoperative steps (ie, placement of pedicle screw, disc space preparation, checking the adequacy of decompression, and cage placement). The study also included an evaluation of important features, such as the amount of radiation exposure and time taken for setting up navigation to the patient’s anatomy.
3D-Navigation Setting Time
Total time taken for setting up of navigation, including presurgical time (ie, initializing the 3D C-arm and the navigation workstation, mounting the reference array on the patient, acquiring scans, and transferring the scans onto the navigation workstation) was about 46.65 ± 9.45 minutes. As displayed in the results, the navigation setting time reduced as surgeon’s experience increased. Our setting time values were in consensus with a study conducted by Balling et al,13 who recorded an O-arm-guided 3D-navigation setting time of 46.2 ± 10.1 minutes in a prospective study of 306 posterior instrumentations. Again, while registration and navigation setting time takes additional time, the total operating time may reduce in patients with complex anatomy, as compared to fluoroscopy-assisted MI-TLIF. In our study, we experienced navigation error in 1 case probably due to translation of the reference array while operating. This caused a medial breach in 1 patient which was rectified immediately. Issues related to errors have been variably discussed in the literature. Rampersaud et al suggested that error margins were positive in translations less than 1 mm and 5° rotations of the patient reference array in all regions of spine.14 Furthermore, a study by Rahmathulla et al, with his experience of 1500 cases in navigation, commented that turning on the warmers during registration can cause image artifacts that can lead to error.15 To minimize anatomical errors that could be secondary to respiratory movements, the authors temporarily suspended ventilation (generally for a minute) at the time of image capture by the C-arm.16
Also, failure of navigation registration is not uncommon in the initial cases until one is well-versed in the technical skills required to use the equipment. This may lead to abandoning the use of navigation and reverting to the basic mode of acquiring real-time images with the C-arm. Interface failure (ie, failure of image acquisition due to error in network connection between the navigation and imaging device) was the culprit in 5 cases. In the other 4 cases, improper positioning of the navigation optical camera that led to failure in tracing the “start” and “end” positions of the 3D C-arm (with the imaging tracker) was the most probable reason for the failure of registration.
Radiation Exposure
Pennington et al17 noted in their meta-analysis that intraoperative CT-guided navigation increases the radiation exposure to the patient rather than the surgical team. This is possible since the surgical team has the ability to leave the operating room while the C-arm spins around the patient to capture the imagery. Although the patients are exposed to higher amounts of radiation, radiation emitted by the isocentric C-arm is less significant compared to the radiation routinely used in clinical practice, such as staging CT (1:380 risk) or a whole-body trauma CT (1:340 risk).18 While the surgical team is routinely exposed to radiation, it may be a once-in-a-lifetime CT-radiation exposure for the patient. Villard et al19 mentioned that the radiation exposure to the surgical team is 9.96 times (1884.8 cGy.cm2) higher in non-navigated cases (free-hand) compared to navigated cases (887 cGy.cm2). Fomekong et al20 observed a reduced level of radiation exposure not only to the patients but also to the surgeons and staff in the navigation group compared to the fluoroscopy group. Other studies show that navigation shows promise as a method to decrease radiation exposure during minimally invasive spine surgery with an acceptable clinical safety profile for patients undergoing complex spine sugery.21–23
Volume of Nucleus Pulposus Excised
An adequate amount of nucleus pulposus excision is extremely vital for optimum fusion. Following discectomy, Hurley et al10 compared the area of empty disc space between 2 techniques: cone beam navigation and open technique using a navigation probe. Discs removed using cone beam navigation were ipsilateral anterior (75%), ipsilateral posterior (81%), contralateral anterior (63%), and contralateral posterior (43%). Rihn et al24 did a comparative study of the open technique and MI-TLIF and demonstrated that the total disc removed by volume was 80% vs 77%, respectively, and total nucleus pulposus removed by area was 73% vs 71%, respectively. Their study indicated that the least amount of disc was removed in the posterior contralateral quadrant (roughly 60%).
Cage Placement
TLIF entails packing the anterior one-third of the disc space with a bone graft. Navigation allows for assessing the thickness of this mantle of bone graft using the navigation probe (Figure 7). While the guidelines for exact placement of the cage have not been published, numerous papers show encouraging results with anterior and central placements within the intervertebral disc space.25–27 Navigation also allows the surgeon to place and impact the cage in the desired spot and, most importantly, to avoid mishaps such as accidental penetration of the anterior longitudinal ligament and retroperitoneal positioning of the cage.28

Assessment of cage placement with navigated array probe.
Pedicle Screw Placement
The high accuracy rate of percutaneous pedicle screw placement noted in the current study is the most important benefit of navigation. The insertion of percutaneous pedicle screws exposes the patient to a high amount of iatrogenic radiation if fluoroscopy is utilized.29 3D-navigation ensures that the pedicle screw is implanted with the most precise trajectory in all 3 planes with the added benefit of protection against radiation.30,31 There is substantial supporting literature to demonstrate the supremacy of 3D-navigation over fluoroscopy and 2D-navigation in terms of safety as well as precision.31–34 Hohenhaus et al showed the superior accuracy of 3D-navigation in pedicle screw positioning compared to fluoroscopy-guided positioning.35 An advancement over navigated Jamshidi needles and guide wires would be the use of image-guided drills with no guide wires for screw placement or awl-tipped taps to reduce the number of steps in screw placement.
Cranial Facet-Joint Violation
The cranial facet-joint is a critical anatomic structure and protection of this joint is vital in avoiding adjacent segment disease.36,37 Surgeons are unable to visualize and palpate bony landmarks and therefore depend on fluoroscopic assistance for minimally invasive spine surgery. Facet anatomy is also difficult to evaluate with 2D-fluoroscopy. 3D-imaging during surgery can result in better anatomic recognition and higher safety outcomes.38,39 In the current study, only 25 out of 408 pedicle screws (6.1%) violated the cranial facet-joint, reinforcing the advantages of navigation-assisted insertion of pedicle screws. Again, the degree of violation in the 6.1% of screws appears relatively inconsequential (Grade 1), based on the classification of Babu et al.12 Ohba et al40 reviewed 194 pedicle screws in 28 consecutive patients and found that 87.5% of screws inserted using conventional fluoroscopy and 94% of screws inserted using 3D-navigation did not violate the facet-joint. Park et al36 reported a high rate of cranial facet-joint violation in fluoroscopic minimally invasive spine surgery when compared to open surgeries (31.5% vs 15.2% of all screws, P < 0.001).
CONCLUSION
While registration and setting up of 3D-navigation takes additional time, the total operating time may be reduced in patients with complex anatomy as compared to fluoroscopy-assisted MI-TLIF. Although radiation exposure to the patient is unavoidable, the amount of exposure to the patient is much less compared to a routine CT and the operating team is protected from radiation. Studies of navigated MI-TLIF show high rates of accuracy in regard to placement of percutaneous pedicle screws and cages with the added advantage of protection of the cranial facet-joint. 3D-navigation also has the benefit of guiding and confirming the anatomical landmarks during the operation, especially in checking the amount of nucleus pulposus excised from each quadrant as well as confirming the adequacy of decompression.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosure The authors report no financial disclosures related to this article.
Ethics Approval The study was approved by the institutional review board.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.