


Abstract
Background Surgeons have scrutinized spinal alignment and its impact on improving clinical outcomes following anterior cervical discectomy and fusion (ACDF). The primary analysis of this study examines the relationship between change in perioperative cervical lordosis (CL) and health-related quality-of-life (HRQOL) outcomes after ACDF. Secondary analysis evaluates the effects of fusion construct length on outcomes in patients grouped by preoperative cervical alignment.
Methods A retrospective cohort study was performed on an institutional database including patients who underwent 1- to 3-level ACDF. C2-C7 CL was measured preoperatively and at final follow-up. For primary analysis, patients were classified based on their perioperative cervical lordotic correction: (1) kyphotic, (2) maintained, and (3) restored. For secondary analysis, patients were categorized based on their preoperative C2-C7 CL: (1) kyphotic, (2) neutral, and (3) lordotic. Demographics and perioperative change in patient-reported outcome measures were compared between groups.
Results A total of 308 patients were included. A significant difference was noted among maintained, restored, and kyphotic groups in terms of delta physical compositeshort form-12 score (ΔPCS-12) (9.0 vs 10.3 vs 1.5; P = 0.04) and delta visual analog scale score (ΔVAS) for arm pain (−0.9 vs −3.8 vs −0.6; P = 0.03). Regression analysis revealed significantly greater improvement of PCS-12 (β: 8.6; P = 0.03) and VAS arm (β: −2.0; P = 0.03) scores in restored patients compared with kyphotic patients. The length of fusion construct in patients grouped by preoperative cervical alignment had no significant impact on the clinical outcomes on regression analysis.
Conclusions Significantly greater PCS-12 and VAS arm improvement were seen in patients whose cervical sagittal alignment was restored to neutral/lordotic compared with those who remained kyphotic. Multivariate analysis demonstrated no association between construct length and perioperative outcomes.
Clinical Relevance The results of this study highlight the importance of sagittal alignment and restoration of CL after short-segment ACDF. Irrespective of preoperative sagittal alignment, the length of ACDF fusion construct does not have a significant impact on clinical outcomes.
Level of Evidence 3.
- cervical lordosis
- kyphosis
- patient-reported clinical outcomes (PROMs)
- anterior cervical discectomy and fusion (ACDF)
- alignment, HRQOL
- construct length
INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) is one of the most commonly performed spine procedures, with a nonlinear increase of 5.7% (120,617–127,500) in ACDF cases from 2006 to 2013.1 Prior studies have overwhelmingly shown the efficacy of ACDF in improving clinical outcomes and radiographic fusion rates for various pathologies, including symptomatic cervical spondylosis, moderate-to-severe disc herniations, and cervical deformity.2–5
Debousset’s “cone of economy” theory describes a stable region of spine alignment over which the patient expends minimal muscle energy in order to maintain an upright balance.6 While the majority of current literature describes the importance of sagittal lumbosacral alignment on clinical outcomes, the effect of Debousset’s theory on the cervical spine has ignited recent academic interest. A previous investigation of patients with adult spinal deformity demonstrated that mild positive cervical sagittal imbalance resulted in patients reporting significantly worse health-related quality-of-life (HRQOL) outcomes.7 Furthermore, a retrospective study in 235 asymptomatic volunteers found a 37% prevalence rate of cervical kyphosis, which was associated with significantly lower HRQOL outcome scores compared with volunteers with cervical lordosis (CL).8
Pre- and postoperative cervical alignment is important in the modern health care era with increasing emphasis on value-based care dependent on improved patient outcomes. The primary aim of this study was to explore the effects of perioperative correction of CL on HRQOL outcomes. The secondary aim was to examine the relationship between fusion construct length and HRQOL outcomes in patients grouped by preoperative cervical alignment.
METHODS
Upon obtaining Institutional Review Board (No. 19D.508) approval, a retrospective cohort study was conducted in patients who underwent a 1- to 3-level ACDF between January 2013 and December 2017 at a single academic medical center. A waiver was granted for patient-informed consent as a minimal risk research study. All procedures were performed by 1 of 7 fellowship-trained spine surgeons. Patients were identified via a standardized query language search using the following Common Procedural Terminology codes: 22551, 22552, 22853, 22859, and 22845. Study inclusion criteria were as follows: (1) patients aged ≥18 years and (2) patients who underwent a primary ACDF procedure. Patients were excluded if they (1) were younger than 18 years; (2) had surgical indications including infection, malignancy, or trauma; (3) underwent a related revision surgery; or (4) had combined anterior/posterior cervical fusion procedures.
Patient Demographics, Surgical Characteristics, and HRQOL Outcomes
Patient demographic data and surgical case characteristics were obtained via standardized query language search and manual chart review. Demographic data of interest included age, sex, body mass index (BMI), smoking status, and Charlson Comorbidity Index (CCI). Surgical case characteristics of interest included preoperative diagnosis, number of levels fused, and length of follow-up.
HRQOL outcomes were collected in person during clinic appointments using an electronic tablet. HRQOL data were retrieved from the OBERD software system (Columbia, MO, USA) in the form of Short Form-12 Physical Composite Score (PCS-12) and Mental Composite Score (MCS-12), Neck Disability Index (NDI), and visual analog scale (VAS) arm and back scores.
Preoperative CL, Length of Fusion Construct, and HRQOL Outcomes
Radiographic parameters were measured on a Sectra Workstation IDS7 Version 21.1 (Sectra AB; Linköping, Sweden) by a single observer. C2-C7 CL measurement was performed using standing lateral cervical radiographs before the operation and at last postoperative follow-up. C2-C7 cervical sagittal alignment was measured as the angle between the inferior endplate of C2 and inferior endplate of C7. Given prior studies demonstrating C2-C7 CL >10° for asymptomatic individuals, patients were classified into 1 of 3 groups based on the preoperative C2-C7 cervical sagittal alignment: kyphotic, neutral, and lordotic.9–11 Patients were classified into each group based on the following measurements:
Kyphotic: C2-C7 CL <0°
Neutral: 0°≤ C2-C7 CL <10°
Lordotic: C2-C7 CL ≥10°
HRQOL outcomes within each of the 3 aforementioned groups were compared based on the number of levels fused.
Perioperative Change of CL and HRQOL Outcomes
Patients were classified into 1 of 3 groups based on the change in C2-C7 cervical sagittal alignment from the preoperative to postoperative time state: “kyphotic,” “maintained,” or “restored” groups. Patients were classified into each group based on the following criteria:
Kyphotic: Patients with a preoperative kyphotic C2-C7 CL to postoperative kyphotic C2-C7 CL.
Maintained: Patients with a preoperative neutral/lordotic C2-C7 CL to postoperative neutral/lordotic C2-C7 CL.
Restored: Patients with a preoperative kyphotic C2-C7 CL to postoperative neutral/lordotic C2-7 CL.
No patients within the cohort were found to have a C2-C7 CL change from preoperative straight/lordotic to postoperative kyphotic. HRQOL outcomes were compared between groups.
Statistical Analysis
Standard descriptive statistics, including proportions, means/medians, and 95%CIs/interquartile ranges, were reported for patient demographic data, follow-up, functional outcomes, and radiographic outcomes (subsidence and alignment data). Normally distributed data were compared using parametric tests and reported as means and 95% CIs, while non-normally distributed (skewed) data were compared using nonparametric tests and reported as medians with interquartile ranges. Sample means between the 3 groups were compared using a parametric analysis of variance test or a nonparametric Kruskal-Wallis test. Categorical data were compared using Pearson’s χ 2 test. Multivariate linear regression analysis was performed to determine the effect of the correction of C2-C7 CL, as well as fusion construct length in groups based on preoperative CL, on HRQOL outcome after controlling for age, BMI, CCI, and perioperative diagnosis. For all analyses, P values less than 0.05 were considered statistically significant. All statistical analyses were performed using SPSS Statistics version 26 (IBM Corporation, Armonk, NY).
RESULTS
Baseline Characteristics
A total of 308 patients were included in the final analysis. The median age for the cohort was 57.0 (49.0, 64.0) years with the majority of patients being men (52.9%). Of the total patient population, 204 (66.2%) patients reported never having smoked, while 72 (23.4%) patients reported being former smokers, and 32 (10.4%) reported being current smokers. Univariate analysis comparing maintained, restored, and kyphotic group patients showed a significant difference in sex (P = 0.02), with a higher proportion of kyphotic patients being women (66.7% vs 33.3%) and a higher proportion of restored patients being men (61.4% vs 38.6%) (Table 1). Furthermore, there was a significant difference in the 3 groups in terms of preoperative (8.9 vs −5.6 vs −7.2; P < 0.001) and postoperative (12.3 vs 8.2 vs −6.2; P < 0.001) degrees of C2-C7 CL (maintained, restored, and kyphotic groups, respectively). Example pre- and postoperative x-ray images for each group are presented in the Figure. No significant differences were present in age, BMI, smoking status, CCI, preoperative diagnosis, levels fused, or follow-up duration between groups.
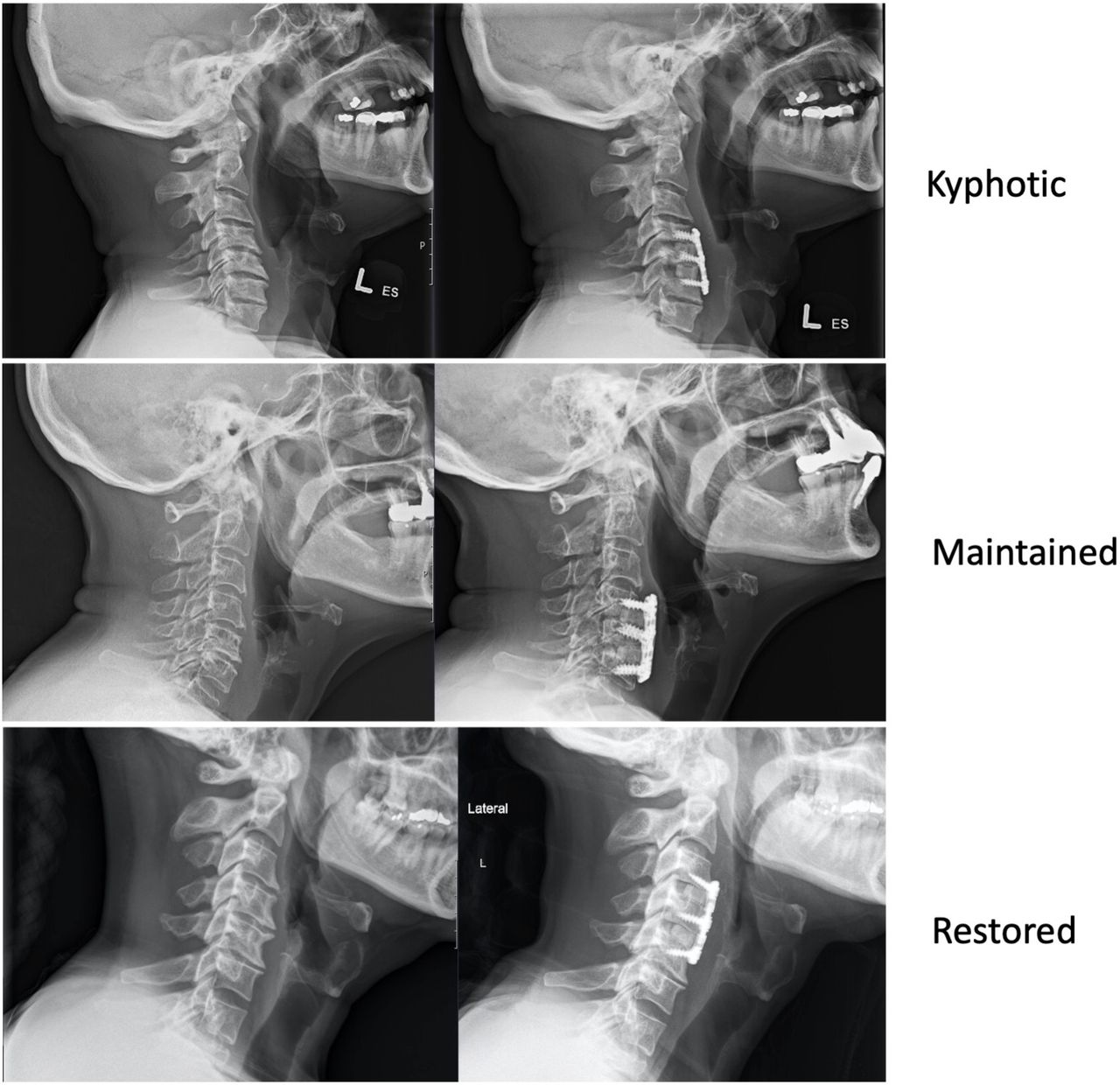
Example pre- and postoperative lateral x-ray images for each group.
Baseline characteristics.
Perioperative Change of CL and HRQOL Outcomes
A significant difference was appreciated among maintained, restored, and kyphotic patients in PCS-12 postoperative (41.6 vs 45.8 vs 36.6, respectively, P = 0.02) and delta (9.0 vs 10.3 vs 1.5, respectively, P = 0.04) scores, with the restored cohort reporting the highest postoperative scores and delta improvement (Table 2). Similarly, there was a significant difference in VAS arm preoperative (3.3 vs 5.3 vs 2.8, respectively, P = 0.02) and delta (−0.9 vs −3.8 vs −0.6, respectively, P = 0.03) scores, with patients in the restored cohort reporting the highest preoperative arm pain scores but the greatest perioperative improvement. Regression analysis showed significantly greater improvement in restored patients compared with kyphotic patients in PCS-12 (β: 8.6; P = 0.03) and VAS arm (β: −2.0; P = 0.03) scores (Table 3). No further significant differences were observed between groups in any of the other HRQOL outcomes. Patients within each group showed a significant improvement from the preoperative to postoperative period, with the exception of Short Form-12 Mental Composite Scores of the restored (P = 0.22) and kyphotic (P = 0.07) groups.
Health-related quality-of-life outcomes stratified by postoperative correction of cervical lordosis.
Regression analysis comparing correction of cervical lordosis and health-related quality-of-life outcomes.
Preoperative CL, Length of Fusion Construct, and HRQOL Outcomes
There were 130 patients with preoperative cervical kyphosis (kyphotic), 114 patients with preoperative neutral cervical alignment (neutral), and 64 patients with preoperative CL (lordotic).
Patients in the preoperative kyphotic group demonstrated a significant difference in VAS neck postoperative scores among patients who underwent a 1-, 2-, and 3-level ACDF, with 3-level ACDF patients reporting the worst scores (3.0 vs 1.5 vs 1.6, respectively, P = 0.01) (Table 4). However, univariate and regression analysis failed to show a significant difference in perioperative improvement in VAS neck postoperative scores among the 3 groups. No other significant differences between fusion construct lengths were observed in any of the other 4 HRQOL outcomes.
Health-related quality-of-life outcomes in patients with preoperative cervical lordosis less than 0° (kyphotic).
Patients in the preoperative neutral group demonstrated a significant difference in VAS arm preoperative (4.7 vs 6.1 vs 2.5, P < 0.001) and delta (−2.5 vs −4.2 vs −0.9, P = 0.003) scores among patients who underwent a 1-, 2-, and 3-level ACDF, respectively. Similar differences were seen in VAS neck postoperative (0.9 vs 1.7 vs 2.9) and delta (−3.9 vs −5.2 vs −2.5) scores, as well as PCS-12 postoperative (44.8 vs 39.1 vs 38.8, P = 0.02) (Table 5). However, regression analysis failed to demonstrate a significant relationship between length of fusion construct and HRQOL outcomes.
Health-related quality-of-life outcomes in patients with preoperative cervical lordosis between 0° and 10° (neutral).
Patients in the preoperative lordotic group demonstrated a significant difference in VAS arm preoperative (6.4 vs 6.7 vs 2.9, P = 0.01) and delta (−4.2 vs −5.5 vs −1.3, P = 0.01) scores among patients who underwent a 1-, 2-, and 3-level ACDF, respectively (Table 6). Similarly, a significant difference was demonstrated in VAS neck postoperative (0.6 vs 1.0 vs 2.2, P = 0.04) scores. However, regression analysis failed to demonstrate a significant relationship between the length of fusion construct and HRQOL outcomes.
Health-related quality-of-life outcomes in patients with preoperative cervical lordosis greater than 10° (lordotic).
DISCUSSION
ACDF is an increasingly common procedure performed in the United States.12,13 Cervical sagittal alignment and the importance of restoration of proper cervical alignment have gained significant interest recently.14–16 Lordosis of the cervical spine provides patients with proper motor function and balance; however, degenerative changes over time can result in loss of CL.17,18 As a result, patients can experience myelopathy or radiculopathy leading to disability and inability to perform activities of daily living. The present study investigated the effects of perioperative change of CL on HRQOL outcomes, demonstrating significantly greater improvement in outcomes for patients whose cervical sagittal alignment was restored to neutral/lordotic vs compared with those who remained kyphotic.
Our study showed significantly greater PCS-12 and VAS arm improvement in patients whose cervical sagittal alignment was restored to neutral/lordotic vs those who remained kyphotic postoperatively. In contrast, a previous study examining the effects of change in perioperative CL after ACDF demonstrated no significant difference in VAS arm or neck pain scores among similar maintained, restored, and kyphotic study groups.19 The authors did report significantly greater improvement between the restored/maintained groups and restored/kyphotic groups, although the improvement was noted in a different HRQOL outcome parameter (NDI) than that of the present study. Our results include a minimum 1-year follow-up, allowing for longer assessment of cervical sagittal alignment postoperatively compared with the prior study. This is important, considering the observed change in CL that occurs with longer follow-up times.20–22 In addition, the larger patient sample of our cohort compared with the aforementioned study (308 vs 104) provides superior power for statistical analysis.19 Our data suggest that correction of cervical sagittal alignment does contribute to improved clinical outcomes. This finding is corroborated by prior studies, including a prospective, randomized study of 122 patients demonstrating that patients with maintained or improved C2-C7 CL had significantly greater clinical improvement compared with patients with decreased CL postoperatively.23–25
When evaluating the effect of fusion construct length on HRQOL outcomes in patients grouped by their preoperative cervical alignment, multivariate regression demonstrated no significant associations. Other reports have confirmed these findings.26,27 In a retrospective cohort study comparing 1-, 2-, and mutlilevel ACDF fusions, no significant difference in improvement of VAS arm, VAS neck, or NDI scores was found.27 Similarly, another retrospective study comparing patients who underwent 1-, 2-, and 3-level ACDF procedures in terms of HRQOL outcomes reported no significant difference among the fusion groups.26
While our study shows improvements in certain clinical outcomes when considering perioperative change in CL, it is important that providers consider the interplay that exists between CL and other cervical spine alignment parameters. An adequate balance between cervical alignment parameters, such as CL, T1 slope (measured as the angle between the superior T1 endplate and horizontal), and cervical sagittal vertical axis (measured as the horizontal distance from the C2 plumb line to posterior-superior aspect of C7), is essential to maintaining a stable cervical spine and preserving horizontal gaze.28,29 Previous studies have established the relationship between these parameters, with cervical sagittal vertical axis inversely correlated with CL and directly correlated with T1 slope.21,30 Recently, Goldschmidt et al established a model to use preoperative CL to predict postoperative cervical sagittal vertical axis:31

where cSVA is the cervical sagittal vertical axis, CH is the cervical height (measured as the vertical distance from the anterior aspect of T1 to upper endplate of C2), T1S is the T1 slope, and CL is the cervical lordosis. This equation ultimately allows surgeons to understand the compensation of C2-C7 CL in relation to T1 slope, as well as predict postoperative ccervical sagittal vertical axis to help tailor cervical interbody grafts using patient-specific alignment parameters. Similarly, another retrospective study evaluated 70 preoperative kyphotic patients in an attempt to predict the ideal postoperative CL associated with improved clinical outcomes.32 They reported a ratio of postoperative CL to C7 slope (measured as the angle between the superior C7 endplate and horizontal) greater than 0.7 correlated with better postoperative outcomes. These relationships exemplify the ability to use preoperative cervical alignment parameters to aid in surgical planning and help set patient expectations.
While the current study provides evidence regarding the importance of cervical sagittal correction, it is not without limitations. First, due to the retrospective nature of the study, available HRQOL outcome data and radiographic imaging limited the sample size, thus resulting in a relatively smaller cohort of kyphotic group patients and underpowered subanalysis of the impact of preoperative CL on HRQOL outcomes. Second, variations in operative techniques and postoperative management exist among surgeons, and confounding is a possible source of bias. Multivariate regression analysis, controlling for patient demographic and surgical case characteristics, was employed to help mitigate this bias. Finally, while the present study focused on the impact of preoperative and perioperative change in cervical sagittal alignment, further information regarding lumbosacral sagittal alignment and its impact on cervical deformity, HRQOL outcomes, and clinical outcomes should be considered in future, high-quality studies.
CONCLUSION
Overall, our study shows restoring CL after ACDF results in significant improvements in PCS-12 and VAS arm scores. The length of fusion construct in patients grouped by preoperative cervical alignment had no significant impact on outcomes. Preoperative planning is an essential part of patient care when considering operative management, and this study provides evidence for the effectiveness of ACDF procedures in patients with varying degrees of cervical alignment.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosure The authors report no financial disclosures related to this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.