


Abstract
Background Lumbar decompression can result in postsurgical instability and spondylolisthesis in patients with lumbar spinal stenosis (LSS). While pedicle screw (PS) constructs improve stability and support fusion, their use can lead to adjacent level degeneration due to rigidity and resultant overload of anatomical structures. The FFX device is a facet spacer designed to be a less invasive alternative for obtaining fusion compared with PS.
Objective The present study aimed to compare biomechanical performance of the FFX device to different lumbar spine procedures using the finite element (FE) method.
Study Design Comparative biomechanical study by FE method.
Methods An FE model for the lumbar spine was developed and validated to assess vertebral displacement and stress variations in the facet joints and discs following surgery. Modeled scenarios included a healthy spine as a reference model, laminectomy (LAM), and prior to/following L4-L5 fusion for LAM + FFX and LAM + PS.
Results LAM increased displacement compared with the healthy spine and both instrumented spine procedures. Facet joint stress at adjacent levels for LAM + PS was significantly higher than with LAM + FFX prior to fusion (+13.5% for L3-L4; +15.7% for L5-S1). Adjacent level disc stress at L5-S1 was 7.7% higher for LAM + PS vs LAM + FFX. Adjacent level facet joint and disc stresses for LAM + FFX were equivalent to LAM + PS once fusion occurred.
Conclusions Instrumented spine fixation prevents the risk of lumbar instability associated with LAM alone. Compared with PS, the FFX device is a less invasive alternative for the treatment of LSS, which potentially lowers the risk of adjacent segment degeneration prior to fusion that provides equivalent stability once fusion is achieved.
Level of Evidence 5.
Introduction
Lumbar laminectomy (LAM) with or without fusion is commonly performed in the treatment of lumbar spinal stenosis (LSS).1,2 Lumbar decompression alone without fusion has been shown to be associated with an increase in postsurgical instability and risk for developing postoperative spondylolisthesis.3 A recent meta-analysis of the literature reported that 12.0% of patients experienced new or an increased incidence of radiographically documented postoperative spondylolisthesis and a reoperation rate for instability of 4.1% after a minimum of 12 months following open laminectomy.4 This reported reoperation rate was twice as likely in patients with pre-existing spondylolisthesis.
Pedicle screw (PS) fixation is currently considered as a standard technique for lumbar fusion to increase spinal stability following lumbar decompression.1 Unfortunately, the use of PS constructs can result in adjacent level degeneration due to the rigidity produced by this approach and the resultant overload of anatomical structures.5 While it is unclear if this rigidity itself creates the progression of the pathology or if its natural progression of the patient’s condition, stress changes and deformation of anatomical structures may lead to early onset degeneration.6 The addition of PS constructs to lumbar decompression is also associated with increased operative time and surgical blood loss compared with decompression alone.3,7
The potential for development of lumbar instability and risk of spondylolisthesis associated with decompression procedures along with the invasiveness and potential risk of adjacent segment disease with PS constructs have led to the development of newer surgical techniques designed to mitigate these problems.1 This includes a novel facet spacer (FFX, SC Medica, Strasbourg, France), which is designed to increase foraminal space and promote fusion while reducing load projections on adjacent lumbar levels. The procedure for placing the device is also less invasive than with PS constructs. The FFX spacer is a titanium constructed, D-shaped device with a serrated surface, which facilitates device stabilization (Figure 1). The device is surgically positioned between the facet joints, with its apex oriented anteriorly (Figure 2). Bone graft material is placed inside and posterior to the device to facilitate fusion over time.8

Image of the FFX device (Courtesy of SC MEDICA).

X-ray image showing bilateral placement of the FFX device in the L4-L5 facet joint, lateral view.
The biomechanics of different spinal constructs has previously been studied with cadaveric testing, and more recently, with finite element (FE) methods. FE is a numeric modeling method that provides both qualitative and quantitative data related to stress and strain distribution, contact forces, and displacement field, which may help the understanding of mechanisms and the comparing of different cases.9 FE analysis may be preferable to cadaver studies because the latter has limitations related to the reproducibility of the results.10,11 FE analysis avoids the variability of cadaver specimen testing and enables repeatable, truly comparative study of differing procedural approaches. It also permits the ability to analyze stresses wherever they appear without the need to predetermine the anatomical location or where to place gauges, the latter which may not always be possible. FE analysis also enables the reproduction of various experiments at the exact same anatomical location of the spine and avoids the need for statistical analyses to compare results collected on spines with variations in morphology, bone, and ligament quality. This approach can also be used when cadaveric studies are not possible, including when stress patterns need to be analyzed.12
FE analysis has its own limitations, as reproducibility issues occur resulting from inter- and intrauser variations in modeling protocols. Two different steps were used to overcome this limitation for the present study. First, we had only 1 individual perform the modeling and used a single spine model to generate all scenarios. Second, other researchers have developed and published several lumbosacral models, which study the sensitivity of various factors on FE model load and displacement (or stiffness) accuracy.13,14 This information was used to effectively simplify the present model, maintain the accuracy of the aforementioned parameters, and justify the choices made.
The goal of the present study was to compare the biomechanical effects of the FFX device with laminectomy alone and with the use of PS constructs to produce lumbar fusion using a validated FE model.
Materials and Methods
FE Model
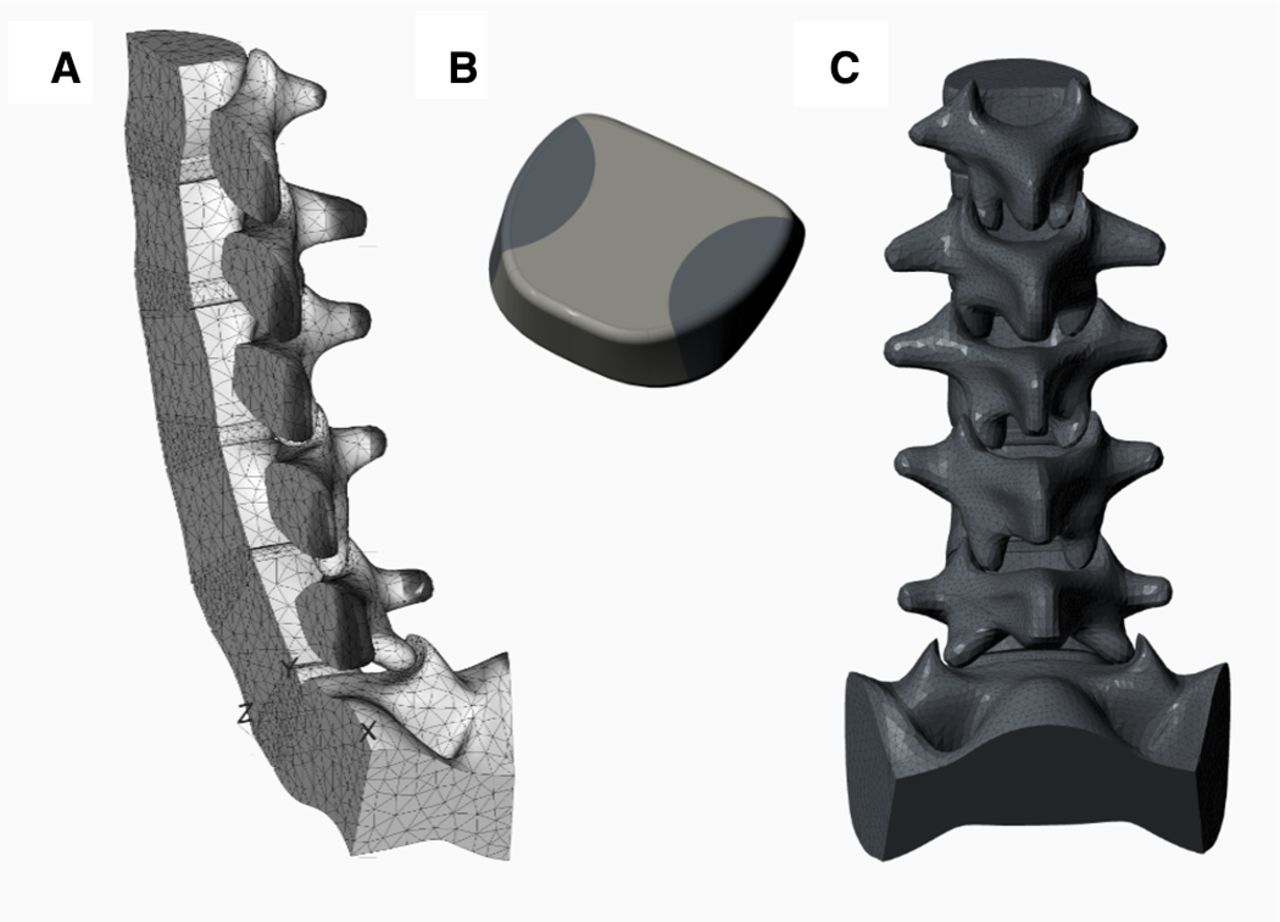
A 3-dimensional L1-S1 intact lumbar spine FE model (Figure 3A) was built using Creo Parametric 3.0 (PTC Inc., Boston, Massachusetts, USA) based on previously described models.14–16 The model was developed to obtain objective quantitative and qualitative information about the biomechanical impact of differing lumbar spine procedures, enable comparison of both the levels and patterns of stress produced, and assess the projection of these stresses to adjacent spinal levels. The shape and dimensions for each vertebra used in the present model were adjusted to the mean size (50th percentile) of a healthy spine as reported in the literature.15–17 The disc was built of 3 separate elements (Figure 3B) in order to produce a lateral rigidity 3 times lower than the anteroposterior (AP) rigidity,14 with the 2 lateral elements having a lower rigidity than the medial element. Since torsion was only planned to be evaluated on the healthy model for the present study, there was no need to cut capsular ligaments for the comparative study that was performed. Capsular ligament stiffness was simulated by a torsional spring added between the 2 vertebrae, simplifying the model because torsional rigidity is very high and difficult to reproduce in a model.14

Finite element model of the lumbar spine (L1-S1) used for the present study. (A) Lateral view. (B) Disc alone. (C) Posterior view.
A mesh was generated on the above geometry (Figure 3A and C) using Creo Simulate 3.0 (PTC Inc., Boston, Massachusetts). This software uses the p-version of the FE method (p-FEM), which utilizes higher degree polynomials as opposed to increasing the number of elements (h-FEM).18 This method enables the ability to check whether the solution converges with only a single mesh step as opposed to iteratively refine the mesh using the h-method.
While the mechanical response of intervertebral discs and ligaments is nonlinear, a decision was made to use the most linear solver for the present model in order to reduce calculation time and computer processing capacity since the current study was limited to comparing 1 scenario to another. While the modeled bone and disc behavior were chosen to follow linear models, facet orientation and contact definition introduced a nonlinearity that made the model more consistent with actual human anatomy. This decision implies to limit the work to loading ranges where the values produced by the mostly linear model were comparable with what is reported in the literature, but still allows comparisons in this limited loading range. Because previous studies have demonstrated that the most important parameters influencing spine mobility are disc height and facet orientation,14,15 we did not model other ligaments except for the analysis of disc rigidity.
The final lumbosacral model included 32,000 tetrahedron elements with the sacrum being considered fixed, with a pure moment load applied to the superior L1 endplate19 to produce flexion, extension, lateral bending, and axial rotation. After assembling all parts of the model, adjustments were made to respect the anatomical lordosis of the spine and to ensure load-displacement curves, which matched what is reported in the literature.20,21 Table 1 lists the final material properties of the model.
Material properties for the lumbosacral model utilized for the present study.
FE Validation
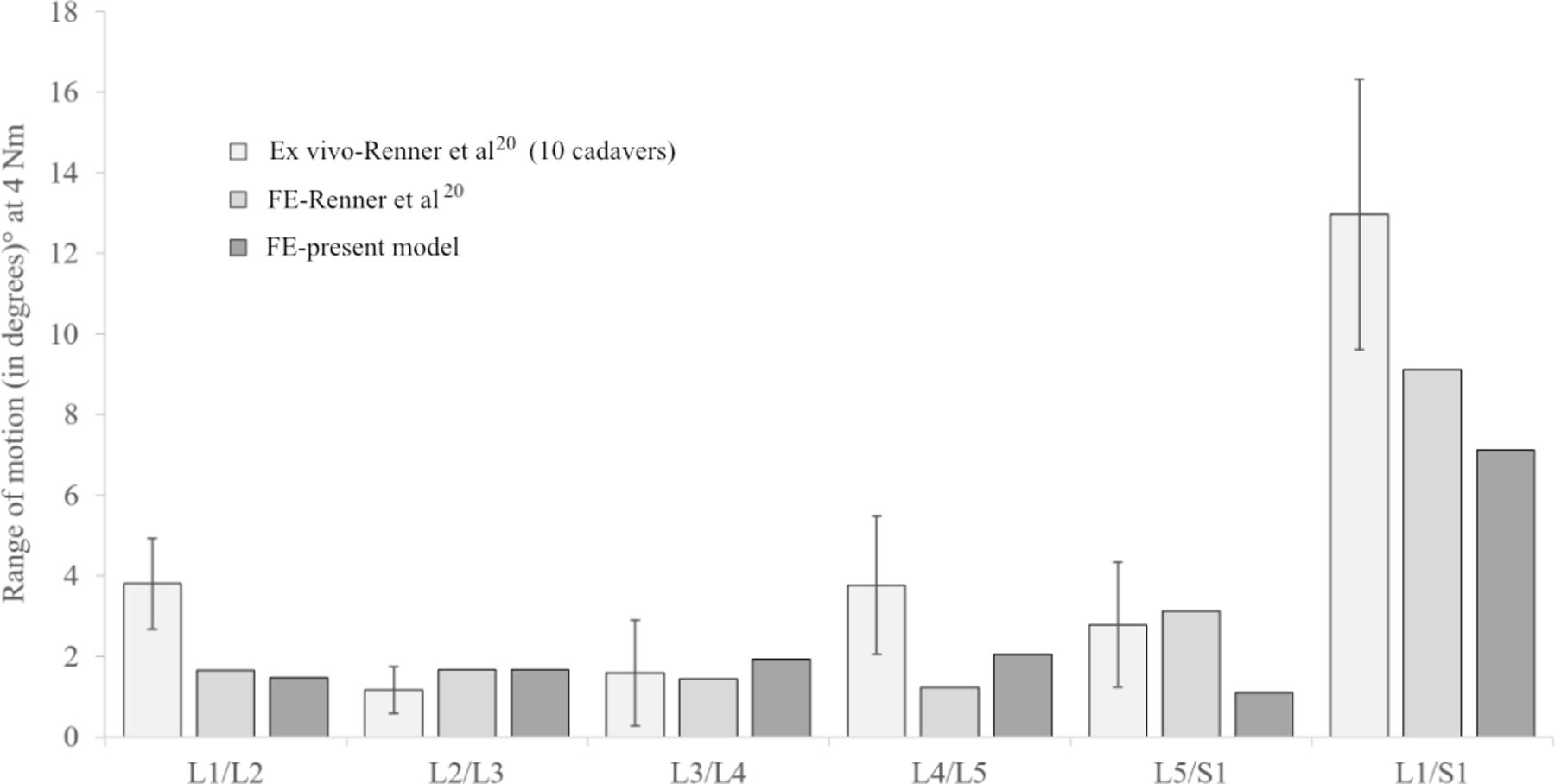
The model was validated by comparing it with experimental results from 3 different studies reporting the angular range of motion (ROM) for each level of the lumbar spine (Figures 4–6).22–24 This included a study by Guan et al,22 which measured flexion, extension, and lateral bending ROM for each spine level using 10 cadaveric spines; a study by Dreischarf et al23 using 8 different FE models to check variations in the overall ROM of the lumbar spine for flexion, extension, lateral bending, and axial rotation; and a study by Renner et al24 using an FE model and 10 cadaveric spines to measure axial-only ROM for each spine level. All of the above utilized moment loads up to 4 Nm, with up to 7 Nm added in extension in Dreischarf et al.23

Comparison of current model vs model reported by Guan et al.19
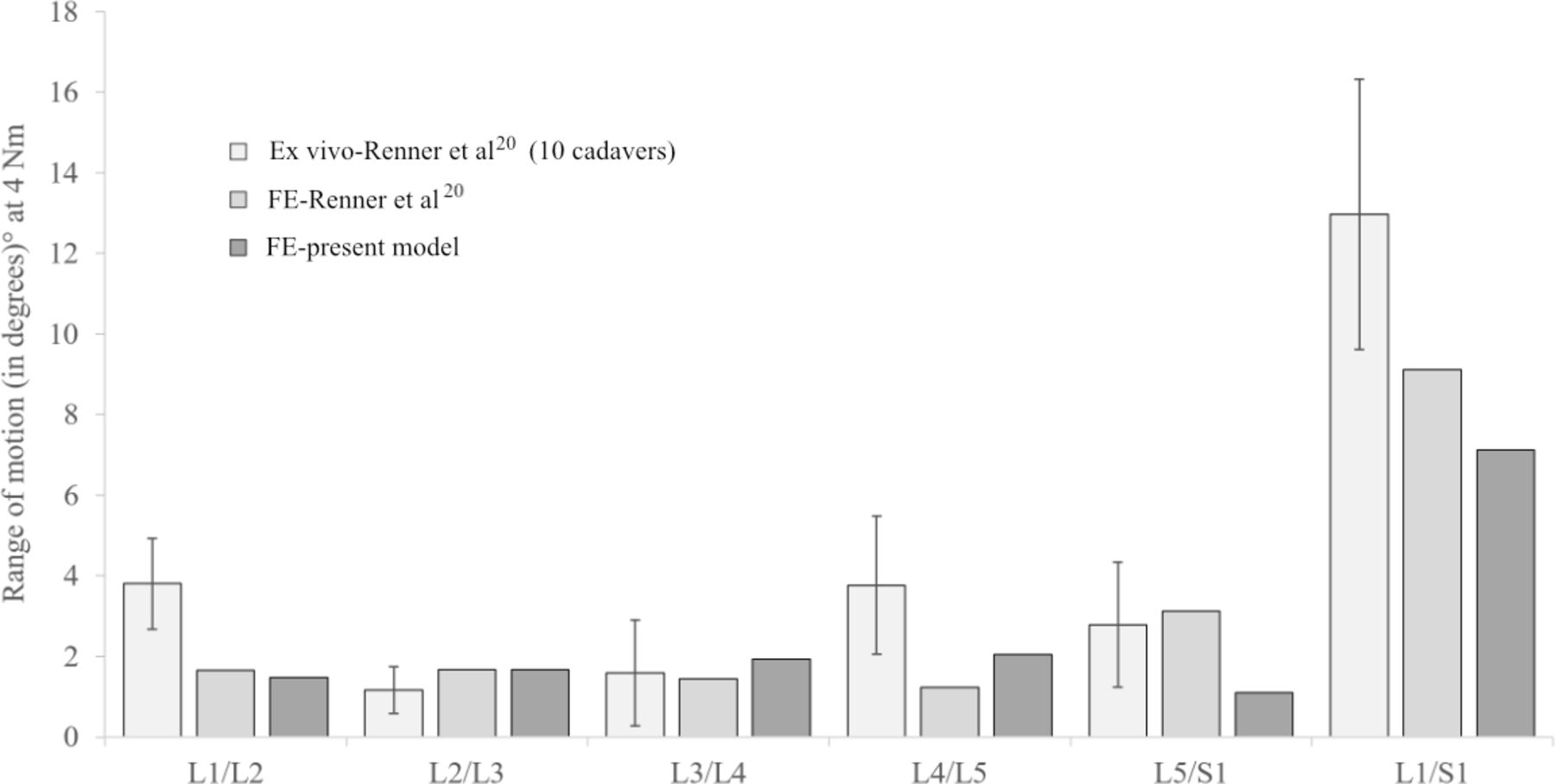
Comparison of current model vs ex vivo (cadaveric) and finite element (FE) models reported by Renner et al.21
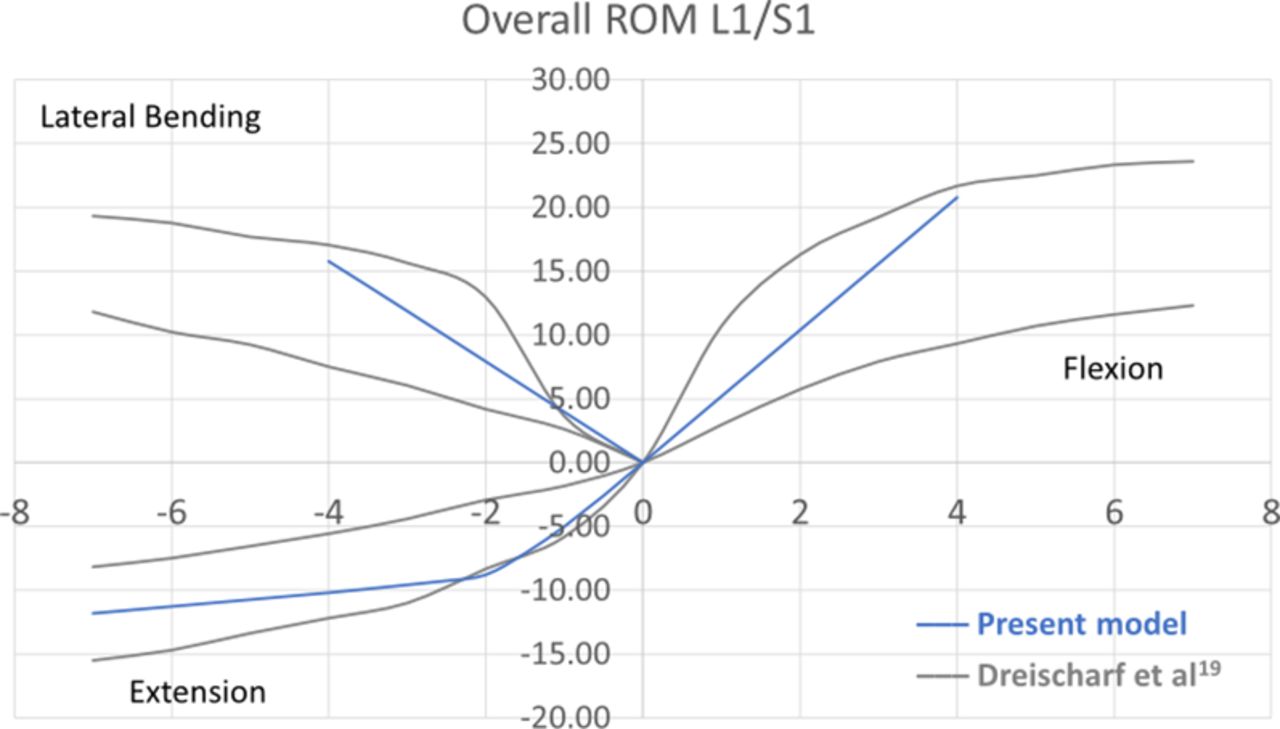
Comparison of current model vs model reported by Dreischarf et al.20
Comparative Studies
Following validation, the model was utilized to compare the impact of a series of differing lumbar spinal constructs on vertebral AP displacement, ROM at an individual level of the spine, and stress in the facet joints and disc (Figure 7). This included (a) the comparison of a laminectomized spine to a healthy spine to determine whether the development of spondylolisthesis after uninstrumented laminectomy could be explained by the model, (b) the comparison of a laminectomized spine with and without the bilateral placement of the FFX device to understand differences in spinal biomechanics associated with each procedure, and (c) the comparison of a FFX fixation construct to a PS construct to obtain quantitative comparative data on the biomechanical changes before and after fusion with these 2 types of implants.
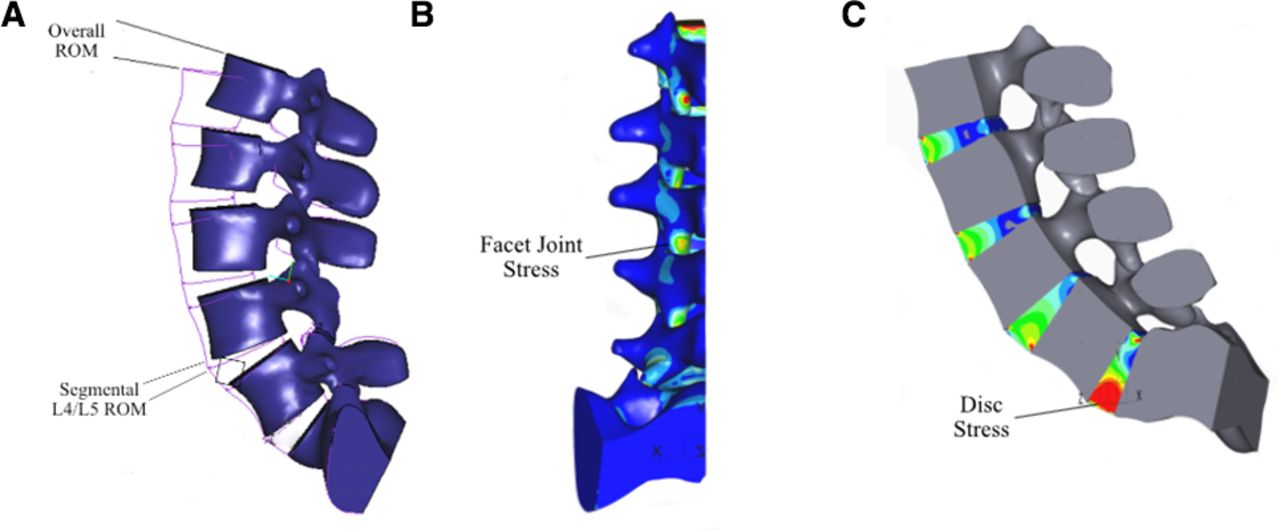
Location of assessments used for comparative studies using finite element model of lumbar spine. (A) Range of motion (ROM; overall and segmental). (B) Facet joint stress. (C) Disc stress.
The FE model presumed bilateral placement of the PS (with rods) and FFX devices at the L4-L5 level. Table 2 lists the various scenarios, which were modeled with an extension loading mode. The model was adapted for both the PS and FFX to include both nonfusion and fusion at the level the devices were implanted. For PS, the screws were numerically stuck at the bone-implant interface. The fused model included the addition of a cortical bone strut which connected the transverse processes of L4 and L5. For FFX, the unfused model was configured with 1 surface of the implant fixed to the bone, and the second surface in contact with the bone also penetrating the serrated surface of the implant. For the FFX-fused model, both faces of the implant were numerically fixed to the bone.
Lumbar spine scenarios which were modeled.
Vertebral displacement for the various scenarios was modeled using a 4-Nm extension moment load. A fixed point was applied to the model geometry to enable the measurement of the displacements, which occurred following the application of this load. For stress and segmental ROM studies, the load set for each model simulation was adjusted in order to produce the same overall ROM (iso-ROM) as the healthy spine model when loaded with 4 Nm (Table 2). This enabled a comparison of the constraints the modeled spine underwent for each scenario to produce the same motion from a patient’s perspective.21 An extension loading mode was selected since it enabled the ability to monitor both the disc and facet stresses at the same time (i.e., in the same single calculation as opposed to flexion where only the disc is loaded), and because extension represents spinal compression in a standing position.22 As this loading mode is symmetrically relative to the sagittal plane, the same phenomena happen on both sides of the plane, and the model can be divided into 2 symmetrical parts with only 1 being studied. This reduced the number of elements required as well as the calculation time, increased the stability of the model, while leading to the same final precision.
Results
Model Validation
The ROM results for the present FE model were compared with previous experimental results by Guan et al21 (Figure 4), Dreischarf et al23 (Figure 5), and Renner et al24 (Figure 6). The use of linear laws in the present FE model would be a significant deviation from the nonlinear hysteresis loop response of cadaveric models if the model would have been used beyond the loads for which it was validated. With the contact (nonlinear) and within the limited range of loads used for its validation, however, these comparisons demonstrated that the ROM for the model was within the envelope curves of published data when a moment load ranging from 0 to 4 Nm was applied for flexion, extension, and lateral bending, and a load up to 7 Nm was applied in extension compared with Dreischarf et al.23 The numerical error calculated at the peak load in all scenarios for the present study was controlled to always be less than 2.2%. The threshold of 4.4% utilized for determining significance when comparing 2 scenarios was therefore conservative.
Vertebral Displacement
The initial results from the model demonstrated that the stress pattern on the facets shifted from AP loading on a healthy spine before LAM to a mediolateral loading in the laminectomized arch after LAM (Figure 8). This resulted in the facets being forced inward, changing the stress pattern and inducing a significantly greater forward displacement variation between L4 and L5 for LAM compared with the healthy spine (+33% displacement variation) (Table 3).
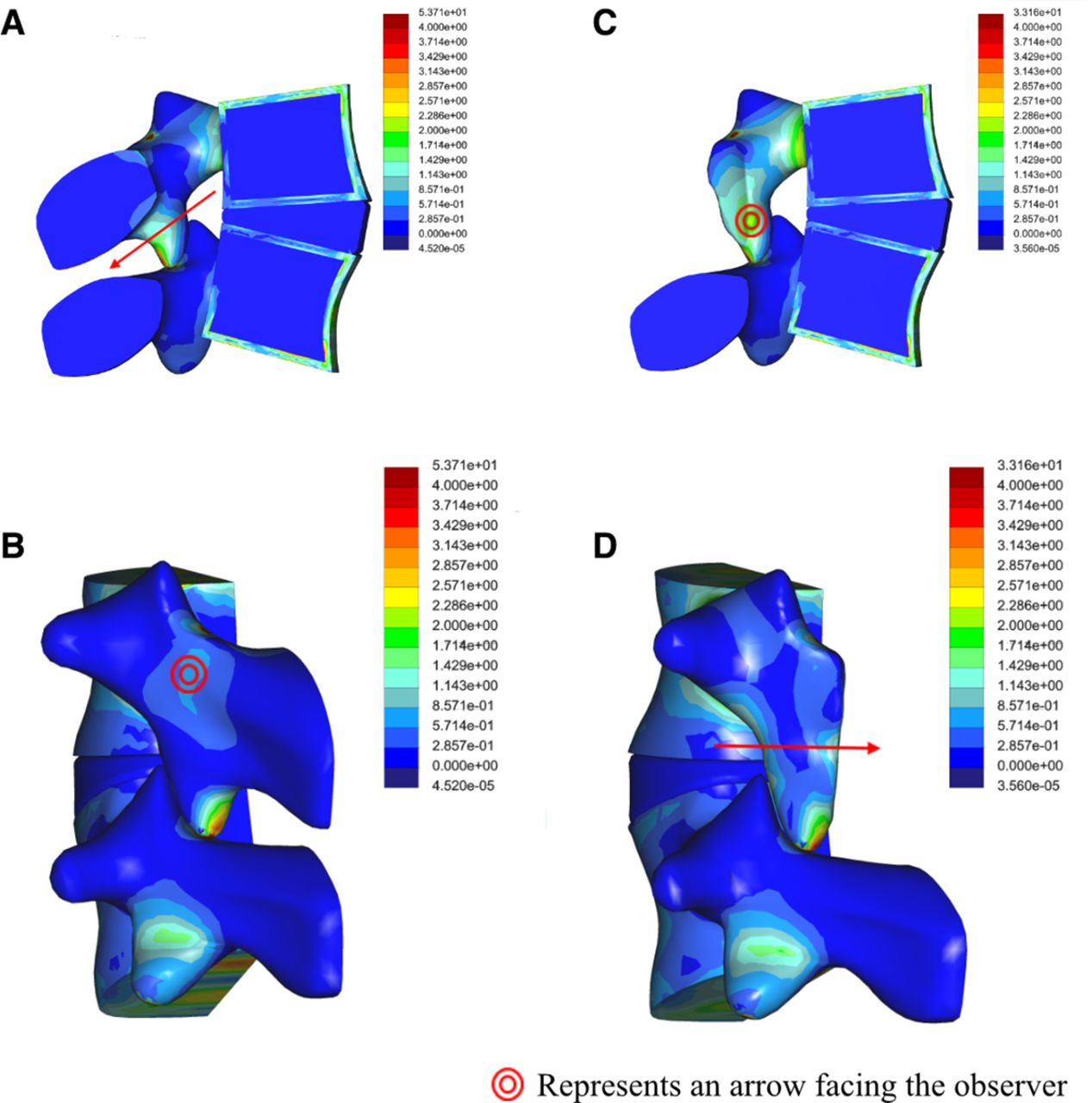
Stress pattern before laminectomy in (A) frontal and (B) sagittal views and after laminectomy in (C) frontal and (D) sagittal views. The force direction (arrows) is perpendicular to the stress gradient. The force applied on the facet joints changes following laminectomy from anteroposterior (A) in the healthy spine to mediolateral (D) in the laminectomized spine with a net result of an inward movement of the facets.
Forward displacement in L4-L5 at a 4 Nm load by procedure.a
The opposite effect was seen between the healthy spine for the FFX and PS fixation scenarios both before and after fusion. LAM + FFX and LAM + PS prior to fusion produced −67% and −73% displacement variations, respectively, compared with the healthy spine. As anticipated, there was no difference in displacement variation between LAM + FFX and LAM + PS when fused with both having a −100% displacement variation (i.e., no displacement) compared with the healthy spine. A significant displacement variation was also observed when comparing unfused LAM + FFX vs unfused LAM + PS (−6.7%).
Segmental ROM
Segmental ROM associated with LAM was similar to the healthy spine (1.38° vs 1.4°) and was decreased at the L4-L5 segment level for all the implants and increased correspondingly at other levels (Table 4). Segmental ROM was 34.8% lower for LAM + FFX (unfused) (0.9°) compared with LAM alone. LAM + PS (unfused) produced more stiffness compared with LAM + FFX as a result of the reduction in ROM at the level of surgery (0.4°) and transfer of the load to other levels. Segmental ROM at L4-L5 was 58% lower with LAM + PS compared with LAM + FFX (0.4° vs 0.9°).
Segmental ROM by procedure type.
Facet Joint and Disc Stresses
Modeling showed that the amount of facet joint and disc von Mises stresses associated with LAM was similar to that of the healthy spine (Tables 5 and 6). While the above stresses amounts need to be considered at the time of the surgery, the stress pattern changes after laminectomy resulting in the facets being forced inward which results in greater vertebral mobility. Guha et al4 reported that radiographic changes or instability (i.e., no kinematic change) are not observed before 12 months, indicating that patient conditions change over time. This correlates with the results from the present study since while the amount of stress does not change immediately, the stress pattern and direction of forces may induce geometrical changes over time (bone remodeling, arthrosis),25 which can lead to the changes observed clinically.
Facet joints von Mises stress (MPa) by procedure type.
Disc von Mises stress (MPa) by procedure type.
There was a significant increase in adjacent level facet joint stress associated with LAM + PS (unfused) compared with LAM + FFX (unfused) for L3-L4 (7.40 vs 6.52 MPa) and for L5-S1 (3.10 vs 2.68 MPa) representing a 13.5% and 15.7% increase, respectively (Table 5). Adjacent level disc stress was significantly greater with LAM + PS (unfused) vs LAM + FFX (unfused) at L5-S1 only (0.42 vs 0.39 MPa), representing a 7.7% difference (Table 6). LAM + FFX was noninferior to LAM + PS relative to adjacent level facet joint and disc stress after fusion.
Discussion
The present study simulated the biomechanics of 3 surgical alternatives for the treatment of LSS in order to compare their effects on spinal stability and load distribution. A 3-dimensional L1-S1 intact lumbar spine FE model was developed and validated by comparing the ROM vs load results with 3 similar models previously reported.22–24 The findings from these comparisons validated the current FE model within the use cases exposed and for comparative studies only and enabled its use for investigating the comparative behavior of differing lumbar spine implants (FFX and PS) while also comparing these to a healthy spine and a noninstrumented spinal procedure (LAM).
The design of the FFX device is intended to prevent facet motion and relieve pain in patient with LSS and to prevent postlaminectomy instability which can appear over time4 , while limiting the rigidity associated with conventional spinal constructs prior to fusion being achieved. The present study confirmed our hypothesis that the device design and placement location result in less projected load (stress) on adjacent levels compared with PS prior to fusion. This effect of the device shape is shown in Figure 9 where the stress is moved from the isthmus to the base of the spine pedicle. The results from the present study suggest that the FFX device could potentially provide a spinal fixation option that can reduce adjacent segment disease prior to fusion, limiting iatrogenic damage to the adjacent discs and facets during this period.

Stress mapping comparing (A) a healthy spine, (B) laminectomy (LAM), and (C) LAM plus bilateral placement of FFX devices prior to fusion.
The increased AP displacement observed with LAM alone compared with LAM + FFX (Table 3) may provide insight on early onset of bone remodeling as is seen with spondylolisthesis.26 It is also interesting that the stress pattern with FFX implants is moved to the base of the pedicle, thus relieving stress in the articular process. This is possibly due to the flat shape of the FFX device and resultant tendency to spread stress at the contact point. Theoretically, this would reduce the risk of facet remodeling during the fusion process and lead to fusion occurring over time, thus preventing the risk of spondylolisthesis.
The significant difference in facet joint and disc stress between LAM + FFX and LAM + PS prior to fusion is likely due to differences in the primary anchorage mode of both implants. PS is immediately and rigidly fixed into bone when implanted, while the FFX is associated with micromotion at the bone-implant interface. This difference disappears after fusion because both implants are rigidly fixed to the bone. The higher disc stress with LAM + FFX at the L4-L5 level compared LAM + PS (0.14 vs 0.08 MPa) correlates with the disc stress seen in the healthy spine (0.16 MPa). This suggests the biomechanics associated with LAM + FFX are more similar to that of a healthy spine compared with LAM + PS prior to fusion.
The use of the FFX device in conjunction with laminectomy offers a technique which can improve postsurgical spinal stability by promoting a high rate of fusion,8 and based on the results of the present study, may provide benefit of decreased rigidity compared with PS constructs prior to achieving fusion. This combined with the less invasive surgical approach for placing the FFX devices compared with PS and the associated potential for a reduction in operative time and blood loss, also support the clinical utility of the device for LSS.
There are several potential limitations to this study. The model used was not comprehensive, in that it did not include other factors such as body weight, and muscles which may impact load levels, movements, and patterns. Sensitivity studies for the model utilized for the present analysis demonstrated that some elements did not contribute to the results (i.e., inactive ligaments for certain movements), thus allowing the ability to simplify the FE model used and not including parameters which did not impact the results presented. Similar to other cadaver testing or FE studies, our model was designed to gain an understanding of the general effects of various spine procedures for LSS on spine biomechanics in order to compare differences between these differing techniques and/or devices. Our model was also limited to linear laws of behavior with the points of contact being the only nonlinear features. This resulted in limits on the loads it could be validated for. For all movements, the validation was limited to a load of 4 Nm except for extension where the validation load could be increased to 7 Nm.
Finally, we chose the indicators according to the way the model was built and according to the capabilities of the software utilized. Since the software used had limitations relative to calculating contact stress, we rather used bending stress in the posterior arch where the loads are transmitted to the facets but away from the facet contact points to avoid local unrepresentative peak values of stress. Also, as the disc is built in 3 parts and not as an annulus and nucleus, we measured stress in the middle plane of the disc as opposed to disc pressure.
Results from validation studies for the model used in the current study demonstrated it was equivalent to the literature references used to develop the model, both in overall and segmental ROM. Actual stress values depend on many parameters and modeling for particular combinations of cortical bone thickness, bone quality, and ligament stiffness would require a very accurate model to be truly meaningful. The objective of the present study was rather to compare the results of each study to one another and analyze the stress variation in level and pattern as opposed to focusing on the stress value itself.
Conclusions
The findings of the present study indicate that in case of LSS, the FFX device has less impact on the biomechanics of the spine compared with PS and an improved stability compared with LAM alone, thus potentially preventing the risk of postsurgical spondylolisthesis by promoting fusion.8 Our results suggest the use of the FFX device also has a reduced risk of impacting adjacent anatomical structures compared with PS as a result of a reduced amount of projected stress on the facets and adjacent level discs during the prefusion period, while having equivalent mechanical stability following fusion. Appropriately designed clinical studies are needed to confirm the above.
Footnotes
Funding Funding to support the development and analysis of the finite element models utilized for the present study was provided to LSCF by SC Medica (Strasbourg, France).
Declaration of Conflicting Interests L.S. and R.B. are employees of LSCF and are paid consultants of SC Medica. R.S. reports being listed as a designer in the patents of the FFX device and having a relative that is employed by SC Medica. X.H. has previously received consulting fees from SC Medica. The remaining author reports no conflicts of interest.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}