


Abstract
Background The practice of cement augmentation in pedicle screw fixation is well established. However, there is a lack of consensus regarding the optimal screw design or cement type. This remains a clinically important question given the incidence of cement augmentation-associated complications. While fenestrated screws have become widely used in clinical practice, the relationship between fenestration placement along the screw axis and cement plume geometry and pullout strength have yet to be clarified. This study was designed to evaluate the mechanical and geometric properties of different fenestrated screw designs and cement viscosities in pedicle screw fixation.
Methods Three different screw fenestration configurations and 2 different cement viscosities were examined in this study. Axial pullout tests were conducted in both foam blocks and cadaveric vertebrae. All vertebral specimens underwent tests of bone mineral density. In the foam blocks, 6 tests were conducted for each augmentation combination and also for nonaugmented controls. In the cadaveric testing, 36 lumbar vertebrae were instrumented with a cemented and uncemented control screw to compare features of fixation. Computed tomography (CT) images were taken to assess the geometric profile of the cement plumes in both the foam blocks and the cadaveric vertebrae.
Results In both foam blocks and vertebral specimens, cementation was shown to confer a significant increase in pullout strength. Significant correlations existed between the anterior-posterior and lateral cement plume diameters and pullout strength in cadaveric vertebra and foam blocks, respectively. Within instrumented vertebra, variables such as the width of the vertebral body and screw insertion were found to significantly correlate with enhanced fixation. CT analysis of the instrumented vertebra demonstrated that a centrally distributed pattern of fenestrations was found to result in a cement plume with consistently predictable distribution within the vertebral body, without evidence of leak.
Conclusion Cementation of fenestrated pedicle screws increases overall pullout forces; however, there is an unclear relationship between the geometric properties of the cement plume and the overall strength of the screw-bone interface. This study demonstrates that the plume diameter, vertebral body width, and angle of screw insertion are correlated with enhanced pullout strength. Furthermore, varying the fenestration design of injectable screws resulted in a set of predictable plume patterns, which may be associated with fewer complications. Further investigation is required to clarify the optimal geometric and biomechanical properties of injectable pedicle screws and their role in establishing the cement-bone interface.
Clinical Relevance This study is relevant to currently practicing spinal surgeons and biomechanical engineers.
Level of Evidence 5.
Background
Complications of pedicle screw fixation such as screw loosening and migration are known to be influenced by the quality of the bone-screw interface, with higher incidences reported in osteoporotic populations.1–3 Cement augmentation has been established as a valid approach to enhancing the strength of the bone-screw interface4 and thus reducing the risk of fixation failure while improving overall clinical outcomes.5–8 As such, cement augmentation has become increasingly used over the past 5 years, with polymethylmethacrylate (PMMA) cements being the most widely used.8–10 Despite its widespread use, there remain significant concerns regarding the use of cementation during spinal instrumentation. Cement leakage is the most common complication associated with cement augmentation, particularly in osteoporotic spines, with studies reporting incidence rates from 13% to 17%11–15 to as high as 62.3% to 66.7%16–18 in more recent studies.
Cement leakage represents a spectrum of complications, relating to the anatomical distribution of the plume. When confined to the intraspinous space, they may result in localized radiculopathies and pain associated with their adjacent neural elements. However, vascular intrusion into the perivertebral venous plexus, epidural veins, or the great vessels may result in cement embolism.19,20 While these complications are typically seen in percutaneous vertebroplasties, there are numerous reports of symptomatic cement leakage and pulmonary embolisms that have occurred following cement augmentation of pedicle screws.16,18 Such complications are more likely to occur in patients with underlying osteoporosis.7,13
There is a lack of consensus regarding the optimal method for cement-augmented pedicle screw fixation, with respect to the screw design, cement viscosity, volume, and the method of cement delivery.9 Defining these variables will confer a cement augmentation system that leverages the strength-enhancing benefits of augmented pedicle screw fixation, while reducing the risk of complications associated with cement leakage and instrumentation failure.
A limited number of studies have investigated the design of the screw fenestrations and its relationship with the cement plume within the vertebral body. Hu et al13 have previously reported that fenestrations of the distal third of the screw result in the highest fixation strength, whereas Chen et al21 have noted that those with the most proximal fenestrations result in greater fixation strength. Both studies report that proximal fenestration designs are associated with a greater risk of cement leakage into the perineural spaces. A recent study by Liu et al8 has further contributed to this discussion, in evaluating a design with fenestrations confined to the anterior two-fifths of the screw. In view of these limited studies, there is a need to clarify the comparative strength profiles of these different screw designs.
While some studies have reported that prefilling of PMMA confers some mechanical advantage over injection through fenestrations,22,23 more recent studies support the use of fenestrated screws over alternative methods of cement augmentation.22–25
Fenestrated screw design is broadly guided by the need for greater predictability and control of the resulting cement plume. There are limited data exploring the effect of fenestration placement along the screw axis and its effect on plume geometry or axial pullout strength.8,13,24,26,27 Limited conclusions can be drawn from these studies given the material variability between the study designs.
This study investigates the mechanical and geometric relationships between screw fenestration pattern, plume geometry, and pullout forces. Using a human cadaveric lumbar vertebra, we explored the following hypotheses:
Cement augmentation will confer a significant increase in axial pullout forces, in vertebra of both osteoporotic and normal density.
A fenestration pattern resulting in a plume distribution toward the cortical bone of the pedicle will result in greatest pullout forces.
Other geometrical features of the plume geometry will correlate with pullout strength.
Plume geometry will be influenced by the viscosity of the cement and the distribution of screw fenestrations.
Methods
This study was designed to examine the effects of screw fenestration design and cement viscosity on overall pullout strength and to correlate geometric features of the cement plume with fixation integrity. Tests were conducted in both foam blocks (Open Cell 5.5 PCF Block, SAWBONES, Washington, USA) and cadaveric lumbar vertebra (ScienceCare, Arizona, USA). The test vertebrae were subjected to dual energy x-ray absorptiometry scans (Lunar Prodigy Advance Bone Densitometer, GE Healthcare) to establish bone mineral density (BMD). Ethics was provided by Macquarie University (Ref. 5201300835).
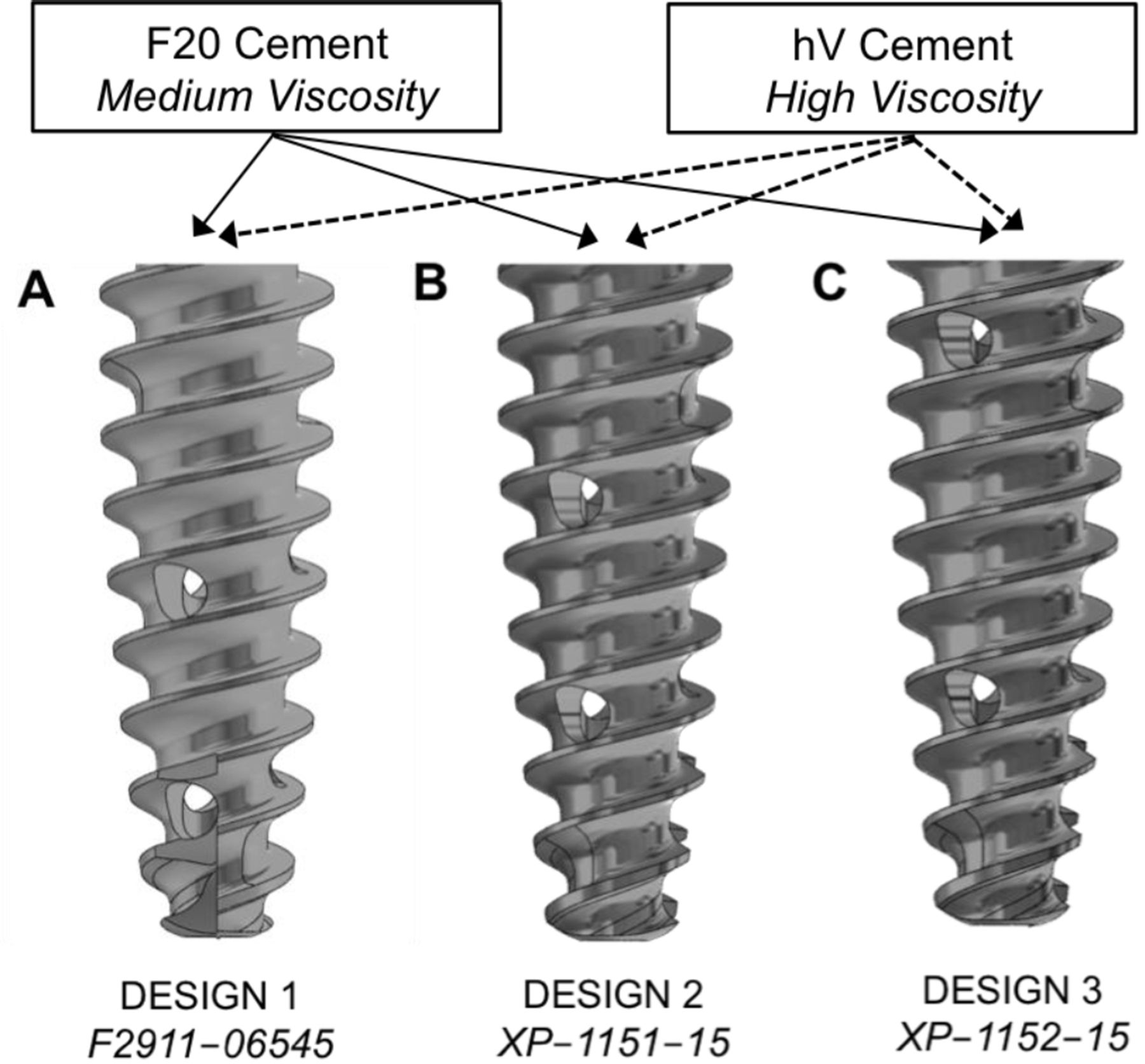
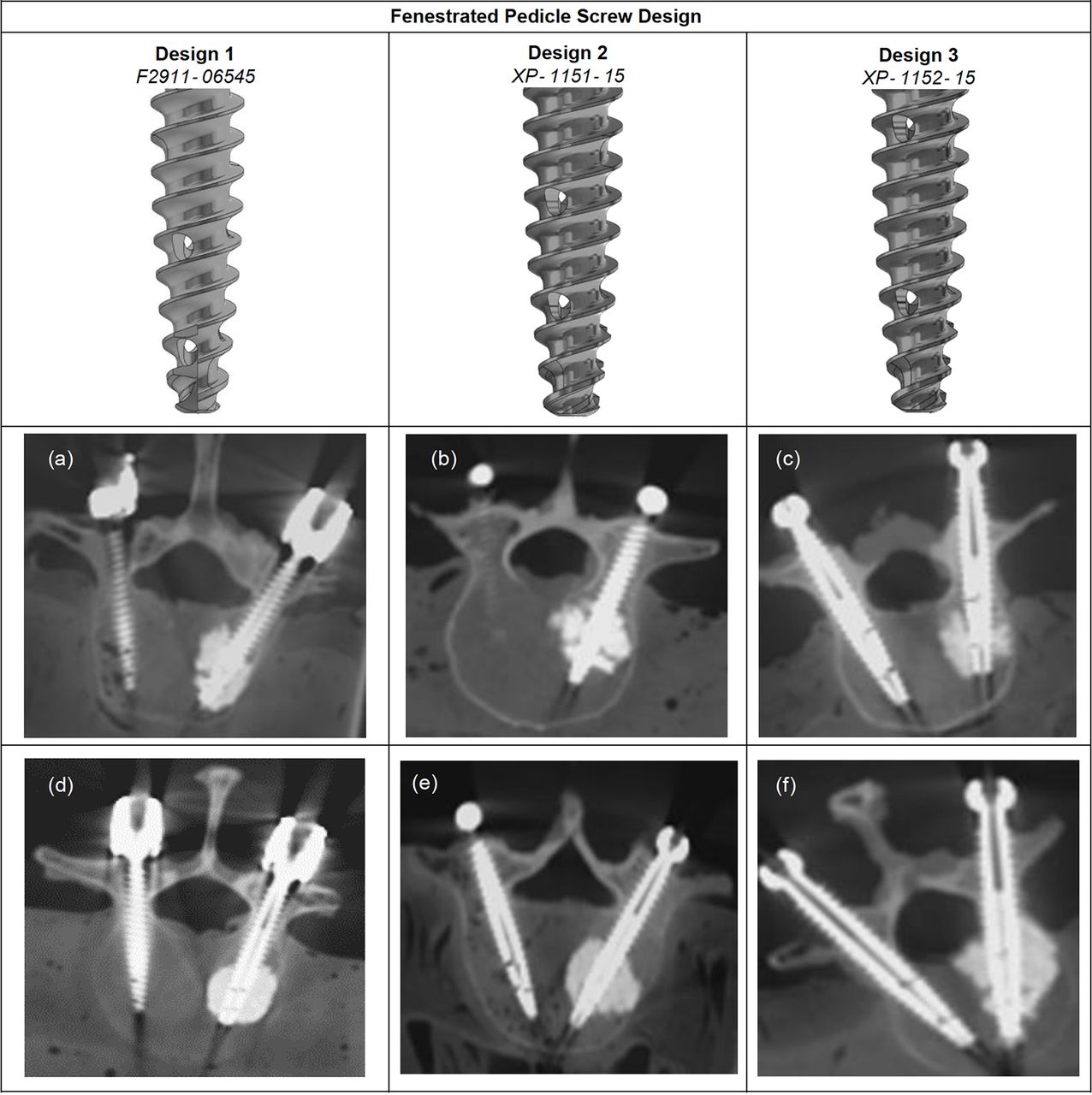
Three fenestrated Everest screw designs manufactured by K2M (Stryker, Michigan, USA) with varying fenestration distribution were selected (Figure 1). Design 1 (F2911-06545) represented the most distally located fenestrations (Figure 1A); design 2 (XP-1151–15) represented an intermediate distribution (Figure 1B); and design 3 (XP-1152–15) represented the most proximally distributed fenestration pattern (Figure 1C). Screw pitch (6.5 × 45 mm), inner diameter (1.8 mm), and fenestration size (1.6 mm) were common to all screw types.

Illustration of the fenestrated screw designs and cement types used in the different experimental groups for the study. All the titanium alloy Everest screws are designed such that their inner diameters measure 1.8 mm, with each fenestration measuring 1.6 mm. The 2 Teknimed polymethylmethacrylate cements vary in their viscosity. There are 6 possible combinations of fenestration design and cement viscosity.
Two PMMA cements from Teknimed (L’Union, France) were selected for this study: a medium-viscosity (F20) and a high-viscosity (High V+) cement. Both cements were injected via a 15 G needle into the cannulation of the fixated pedicle screws with a fixed volume of 2 cc and allowed to cure for a minimum of 24 hours.
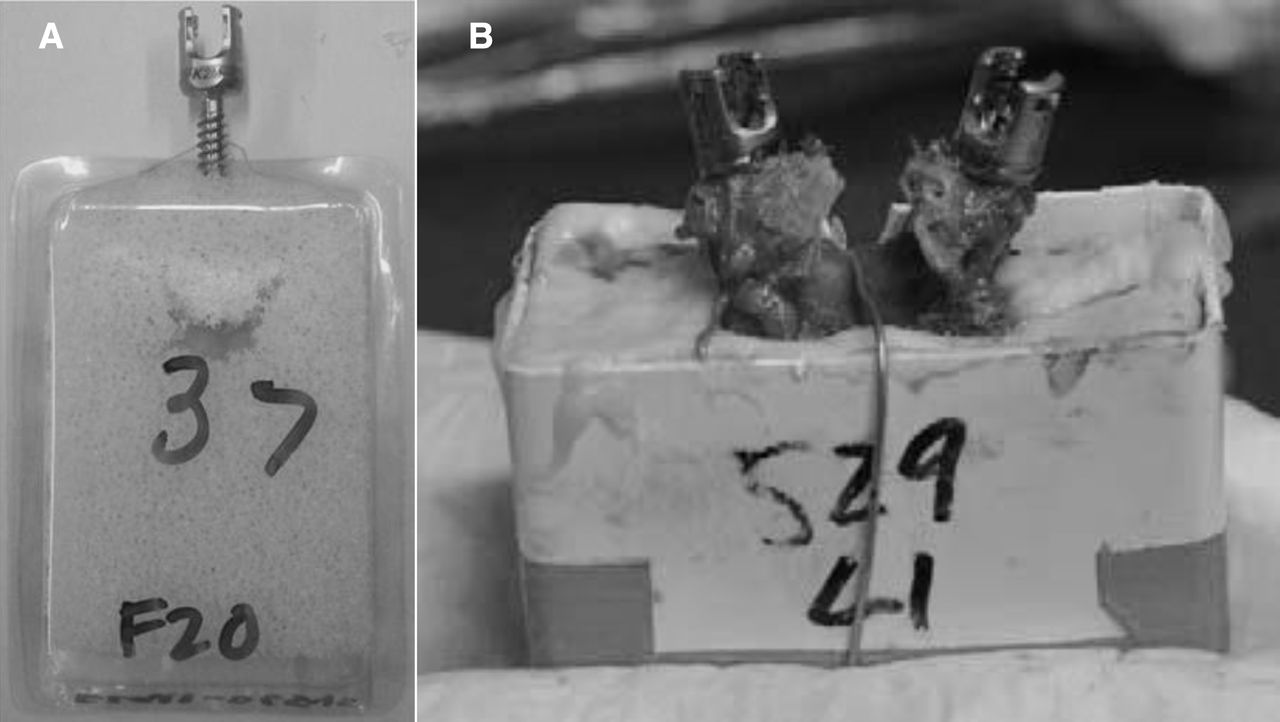
Foam block testing was designed such that each screw and cement group were tested in individual foam blocks and compared with a control group of uncemented screws, yielding a total of 7 groups with 6 specimens per group. The instrumented foam blocks (Figure 2A) were retained in a custom plastic case and fixed to the Instron base using a vice (Figure 3A).

Illustrative example of specimen preparation for experimental testing of relationship between fenestrated pedicle screw design and cement plume geometry on pullout forces, conducted in (A) foam blocks and (B) vertebral specimens. Foam blocks with the density of cancellous bone were encased in plastic, prior to being instrumented with 1 of 3 fenestrated pedicle screw designs from Everest. Cadaveric vertebra were bilaterally instrumented with the same screw type; one side was augmented with cement, while the other side was left uncemented and used as a control. Test screws within the foam and vertebral specimens were augmented with Teknimed polymethylmethacrylate cements of medium and high viscosity.
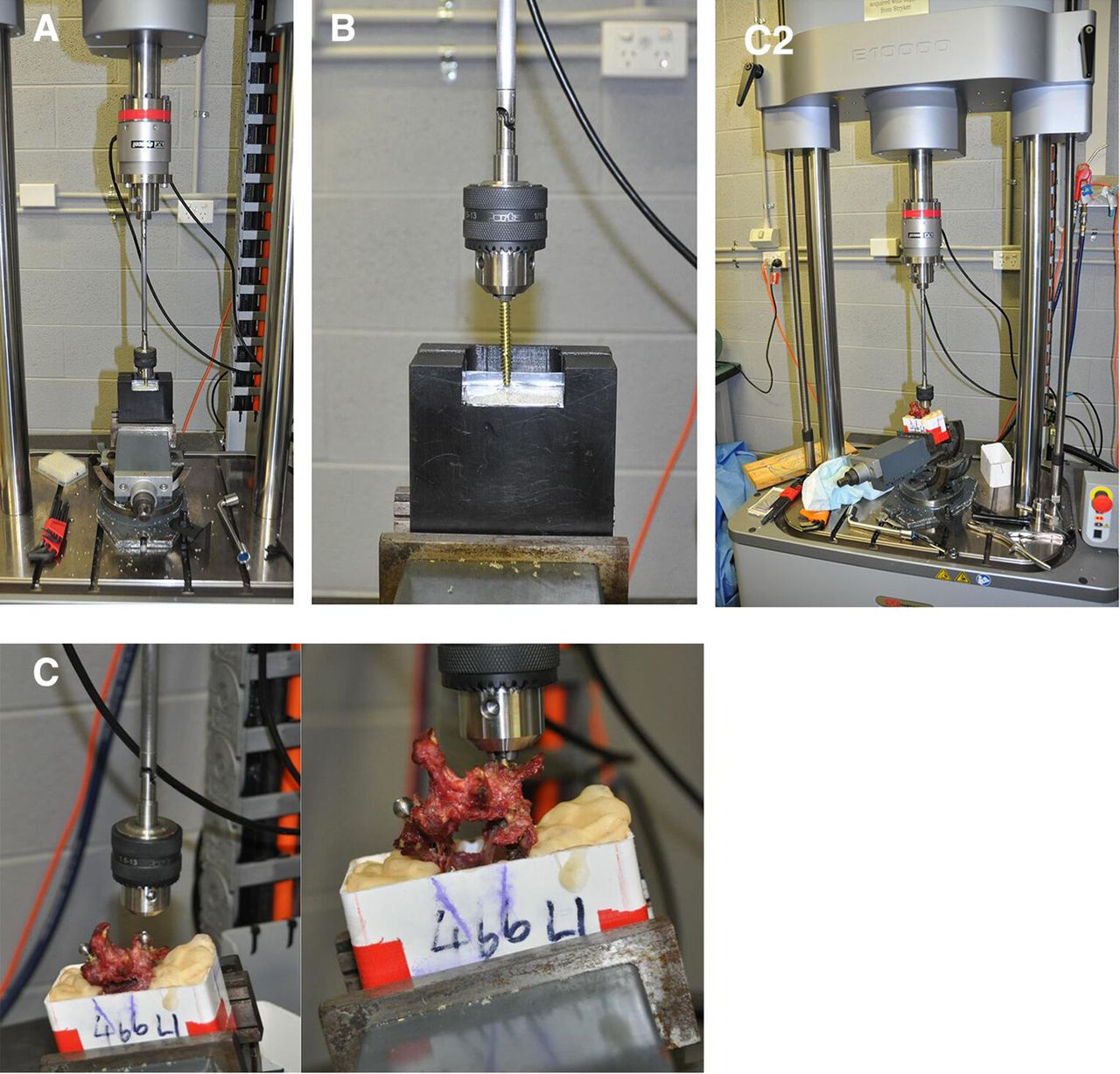
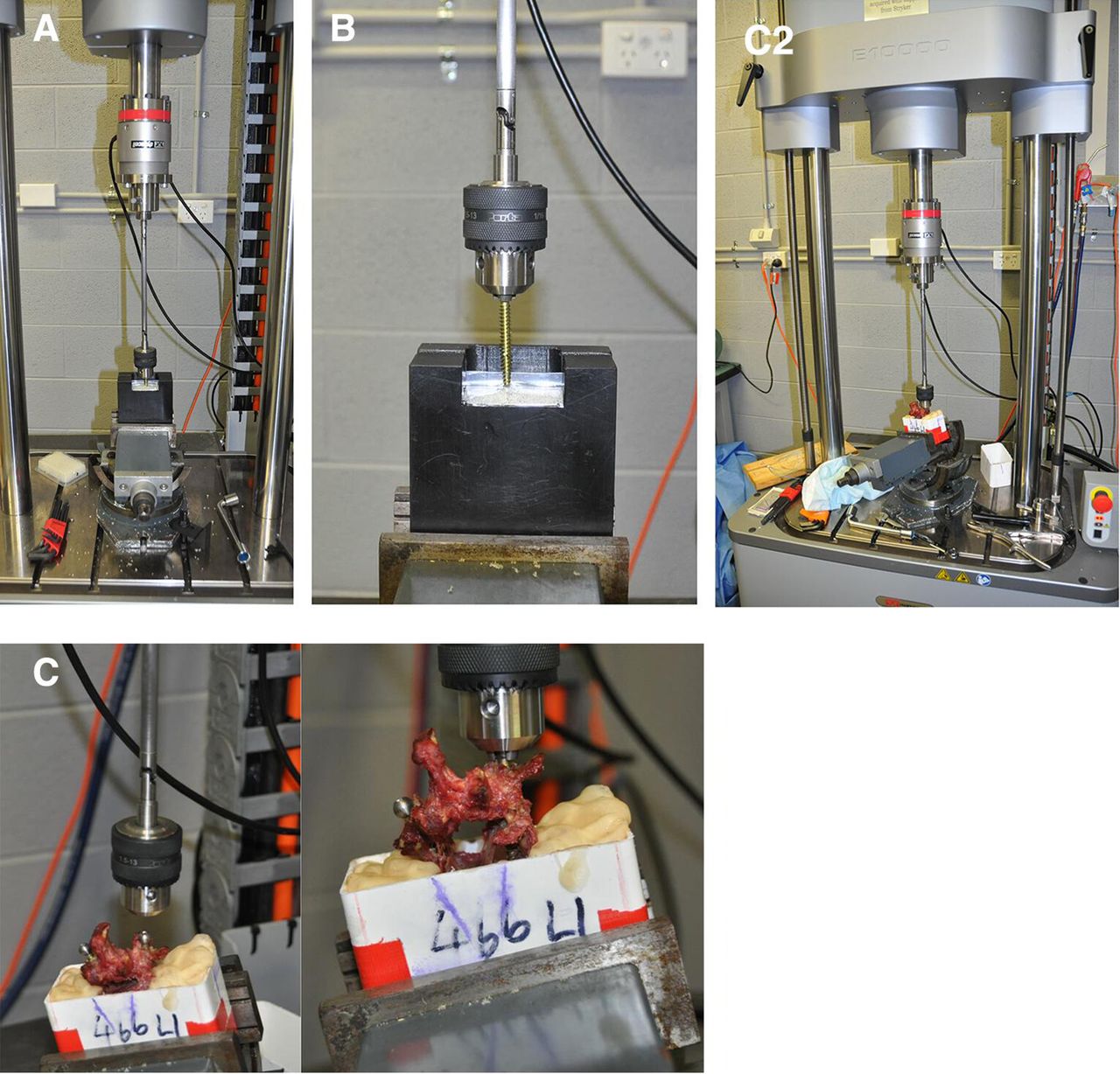
Experimental setup for pullout testing of different fenestrated pedicle screw designs from instrumented foam blocks and vertebral specimens. (A) The foam blocks and potted vertebra were fixed to the base of an Instron E10000 universal testing machine, with a vice yielding 3° of rotational freedom, which permitted coaxial alignment of the screw axis with the axis of the pullout force. (B) A Jacobs chuck was used to grip the screw head. The chuck was fixed to the Instron loadcell via 2 universal joints to limit motion artifact. The loadcell was connected to the Instron linear actuator. All screws were pulled out at a displacement rate of 5 mm/min. (C and C2) Illustrative example of an instrumented vertebral specimen undergoing pullout testing.
A total of 36 lumbar vertebra from 8 cadavers were used for testing (3 men, 5 women; mean age at death, 66 years; age range, 47–97 years). The same 6 combinations of fenestration design and cement viscosities were tested with 6 per group. Each vertebra was potted within a rectangular polyvinyl chloride pipe using PMMA cement (Figure 2B). All vertebrae were bilaterally instrumented with 2 identical fenestrated pedicle screws; 1 serving as the control with no cement and the other designated as the cement-augmented test screw. By having an internal control screw for each vertebra, the effect of varying bone density between specimens could be minimized. The spinous process was excised from the potted specimens to decouple the instrumented pedicles during testing. Furthermore, securing of the potted specimens was achieved with wire and wooden spreaders (Figure 2B).
To examine the distribution geometry of the cement plume, each instrumented vertebra and foam block were subject to both computed tomography imaging and dimensional analysis (Supplemental Table 1). Cement plume measures included the anterior-posterior (A/P) and lateral diameters of the plume, and the respective distances of the plume from the tip and head of the fenestrated screw, relational measures of the screw, and the insertion angle (Supplemental Figure 1).
Supplemental Tables.
Supplemental Figures.
Experimental Setup for Pullout Testing
The foam blocks and potted vertebra were fixed to the base of an Instron E10000 universal testing machine, using a vice with 3° of rotational freedom (Figure 3), which allowed coaxial alignment of the long axis of the pedicle screws with the Instron linear actuator. A Jacobs chuck was used to grip the screw head; this was fixed to the Instron loadcell via 2 universal joints to limit motion artifact. The loadcell was connected to the Instron linear actuator. All screws were pulled out at a constant displacement rate of 5 mm/min.
Statistical Analysis
All records were maintained in logbooks, and data stored in Microsoft Excel and Prism. Statistical analyses were conducted with Microsoft SPSS.
BMD Analysis
Dual energy x-ray absorptiometry scores were recorded for all donor specimens in order to establish mean density scores of each test specimen.
Foam Block Data Analysis
Data from the foam block pullout tests were subjected to 1-way analysis of variance (ANOVA) in order to interrogate the difference between pullout forces between a control group and a cement-augmented group.
Vertebral Body Data Analysis
To examine the effect of augmentation on pullout strength, the difference between test and control results was compared. By interrogating the difference between the augmented and control values within each individual vertebra, we were able to eliminate the influence of intrinsic variation between the vertebral specimens on the observed outcome. Two-way ANOVA was used to investigate the joint effects of the cement type and the screw type on the overall pullout strength.
Geometric Analysis of the Cement Plume
The geometric properties of the cement plume were compared with the pullout strength for all augmented specimens, for both the foam blocks and vertebral bodies. Tests of correlation were conducted using both Pearson and Spearman analysis, with scatterplot analysis to assess linear relationships.
Results
Foam Block Testing
Foam Block: Effect of Cement Augmentation
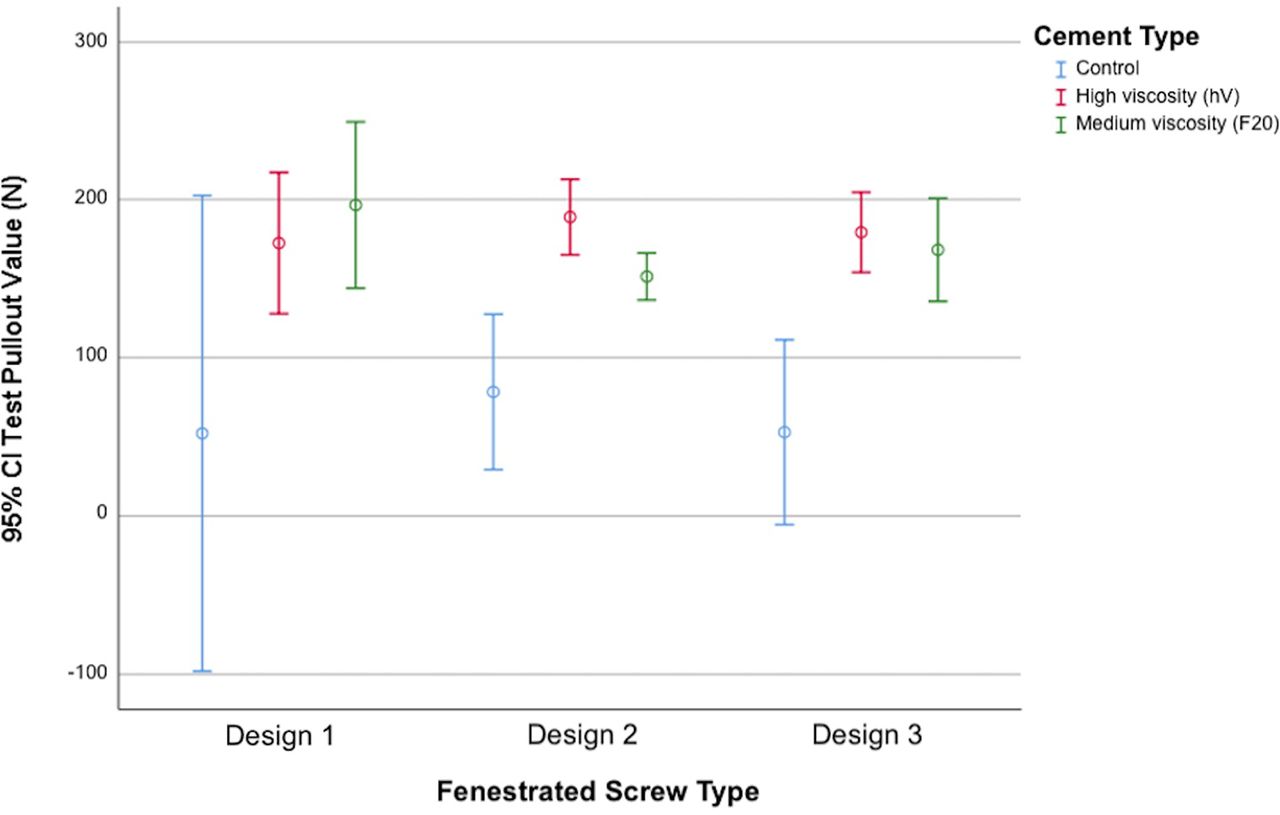
The results of cement augmentation of pedicle screw fixation in foam blocks are presented in Figure 4. The mean pullout strength of the control group was 61.15 ± 6.43 N compared with the augmented specimens, which was 176.06 ± 34.03 N. The mean pullout forces of the augmented design 1 screws were 172.42 ± 42.50 and 196.44 ± 50.05 N for hV and F20, respectively. The design 2 augmented group demonstrated a mean pullout for 188.85 ± 22.78 (hV) and 151.27 ± 154.15 N (F20). Augmentation of design 3 resulted in a mean of 179.19 ± 24.06 (hV) and 168.16 ± 31.01 N (F20). No significant difference was demonstrated between the different cement-augmented groups when tested by 2-way ANOVA. Tests of between-subject effects showed that there was no interaction between the screw design and cement type (P = 0.153) on the amount of pullout force that was generated.
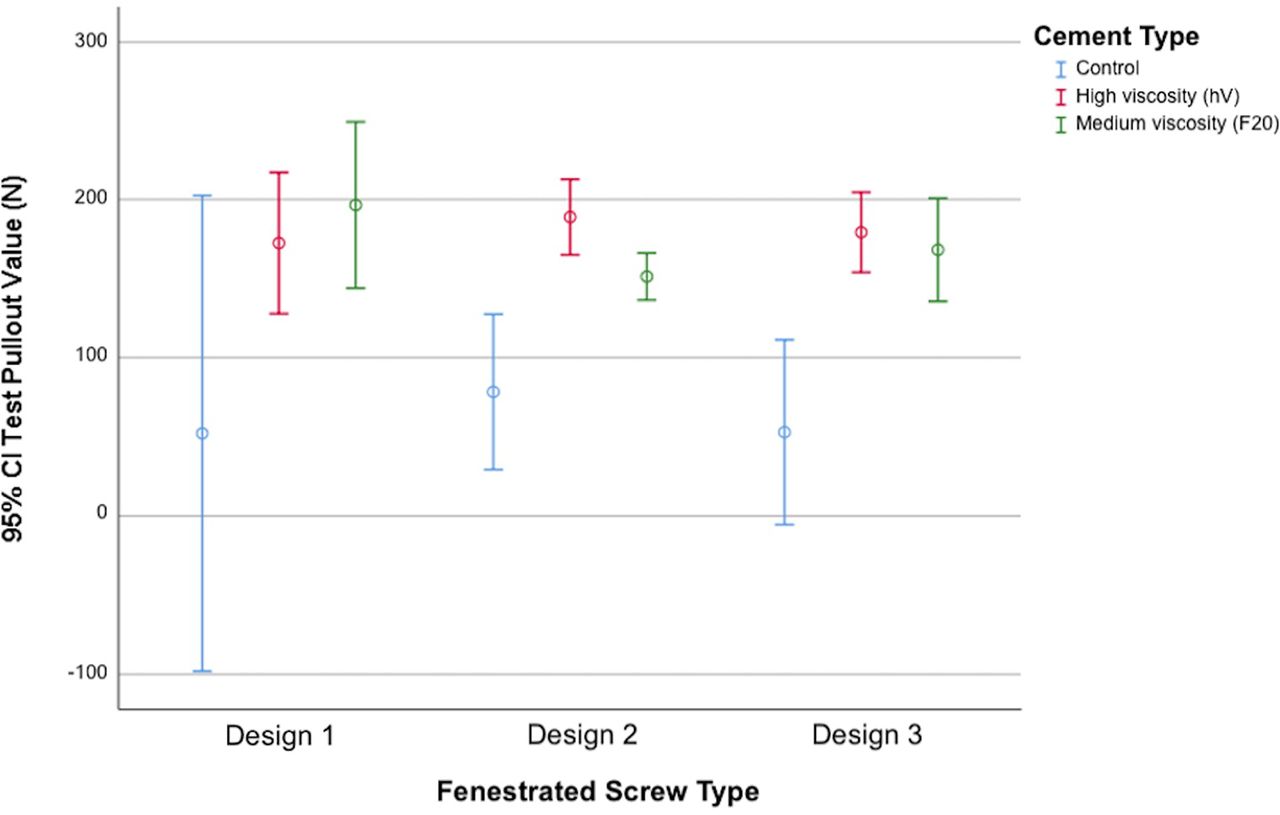
Effect of polymethylmethacrylate (PMMA) cement augmentation on pullout loads of fenestrated pedicle screws when tested in foam blocks. Tests were conducted with 3 different screw designs manufactured by Everest with varying fenestration distribution and Teknimed PMMA cements of medium and high viscosity.
Foam Block: Correlation Testing
Raw data of the plume geometry measurements taken from the augmented foam block groups are available in (Supplemental Table 2). Corresponding Pearson correlations between variables have been presented as scatter plots (Supplemental Figure 2). Of the examined variables, only the lateral plume diameter was shown to significantly correlate with pullout force (Figure 5; coefficient = 0.386, P = 0.020).

Scatterplot demonstrating a significant correlation between lateral plume diameter and pullout strength when tested within foam blocks (coefficient = 0.386, P = 0.02).
Vertebral Body Testing
Vertebra: Effect of Cement Augmentation
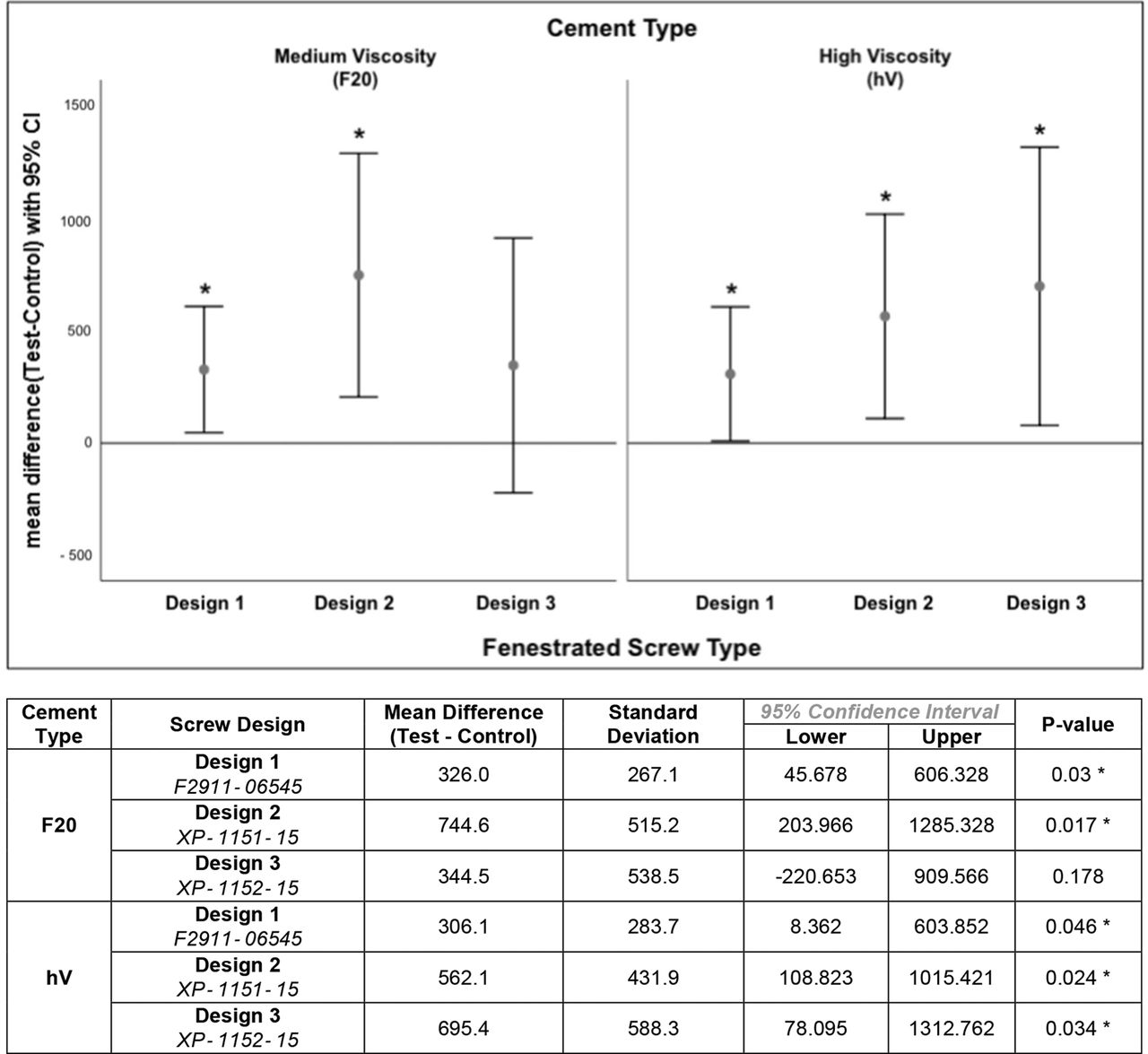
Results of the vertebral tests between cemented and noncemented screws are demonstrated in Figure 6. When analyzed according to screw design and cement type, the design 3 screw with the F20 cement augmentation failed to reach a significant increase in overall pullout strength when compared with its noncemented control (P = 0.178). No single screw-cement combination demonstrated a significant biomechanical advantage in pullout strength. Two-way ANOVA was used to investigate the joint effects of the cement type and screw type on between-subject effects. There was no evidence for any interaction (P = 0.351), nor was there an evidence of a difference due to the screw type (P = 0.205) or cement viscosity (P = 0.747).
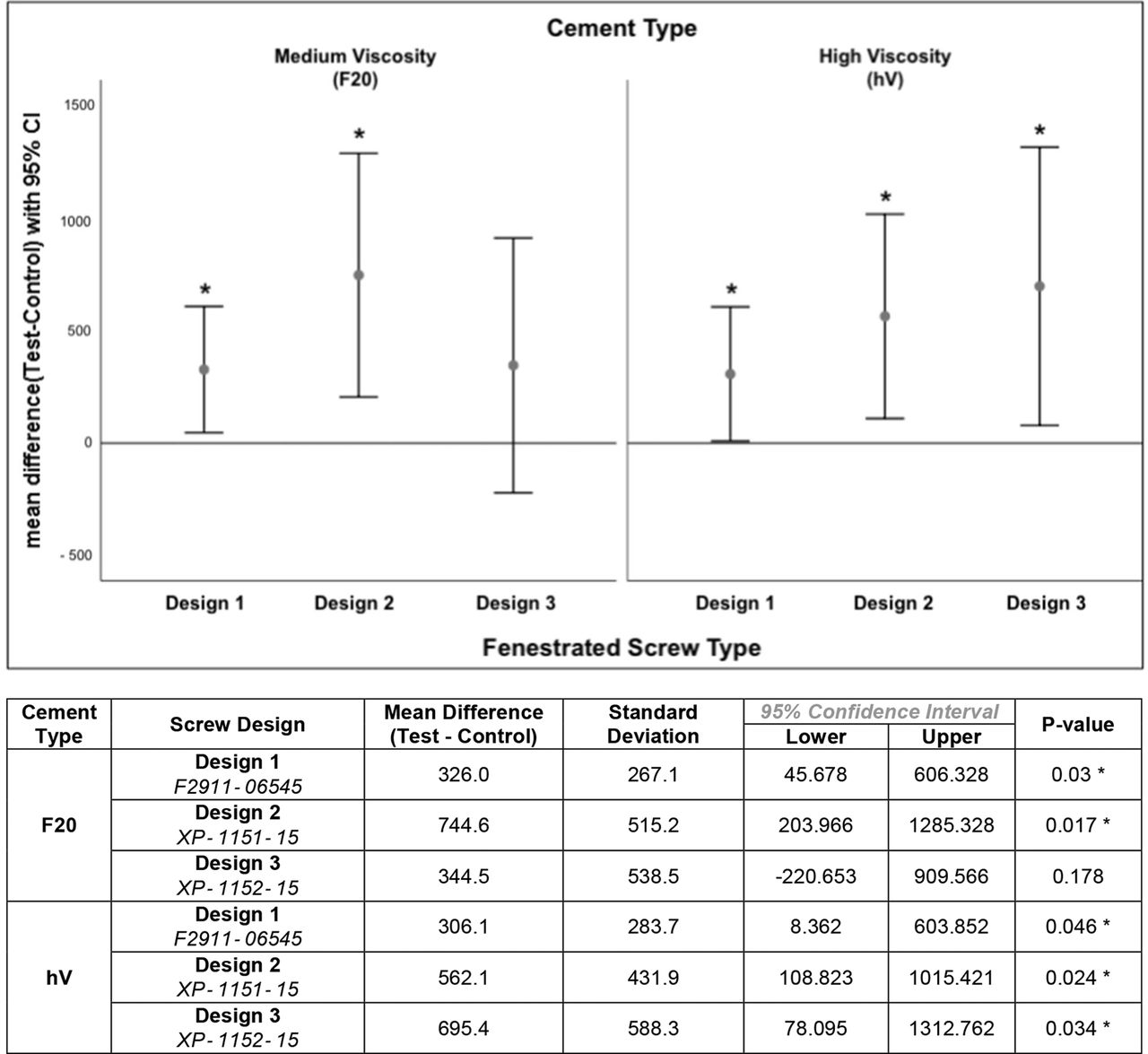
Vertebral body testing: Effect of cement augmentation with Teknimed F20 or hV on 3 different fenestrated screw designs when tested within lumbar vertebra. In all but the XP1152-15 (design 3) with F20 group, cementation resulted in a statistically significant increase in pullout forces when compared with a matched control. The mean difference between test and control is represented with 95% CI. (*P < 0.05).
Vertebra: Correlation Testing
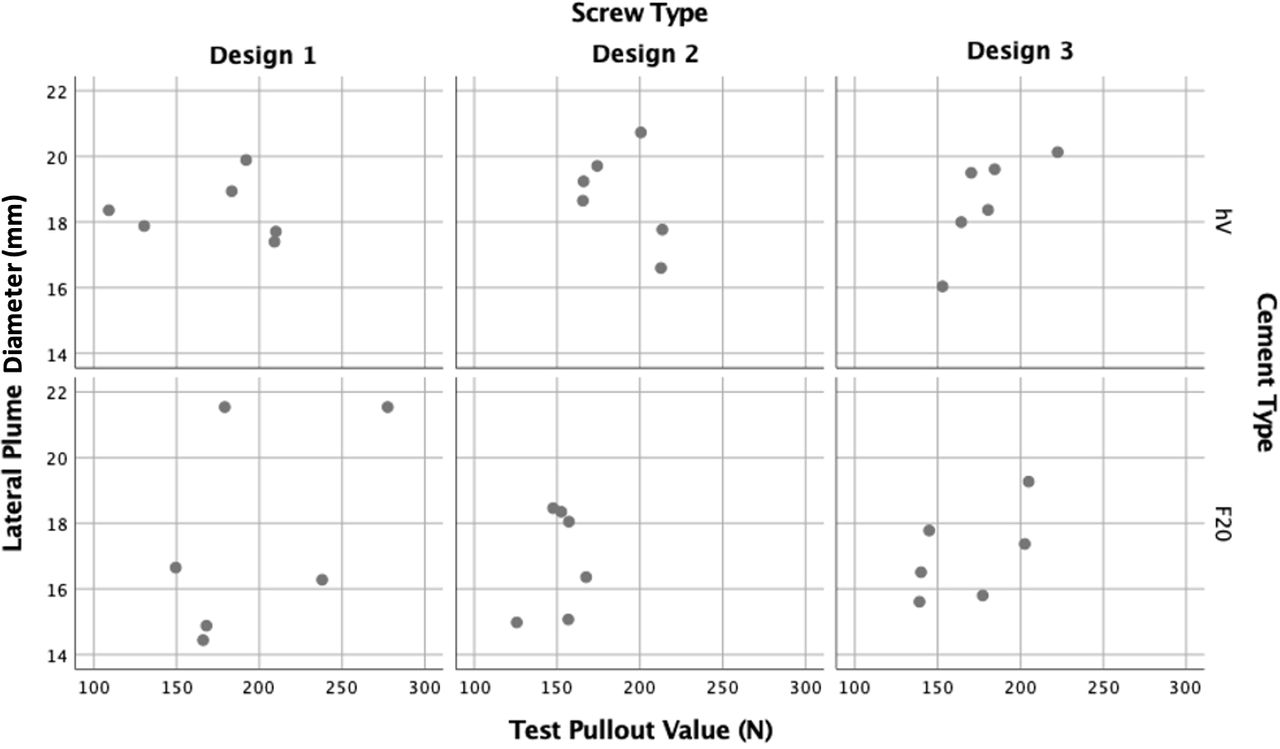
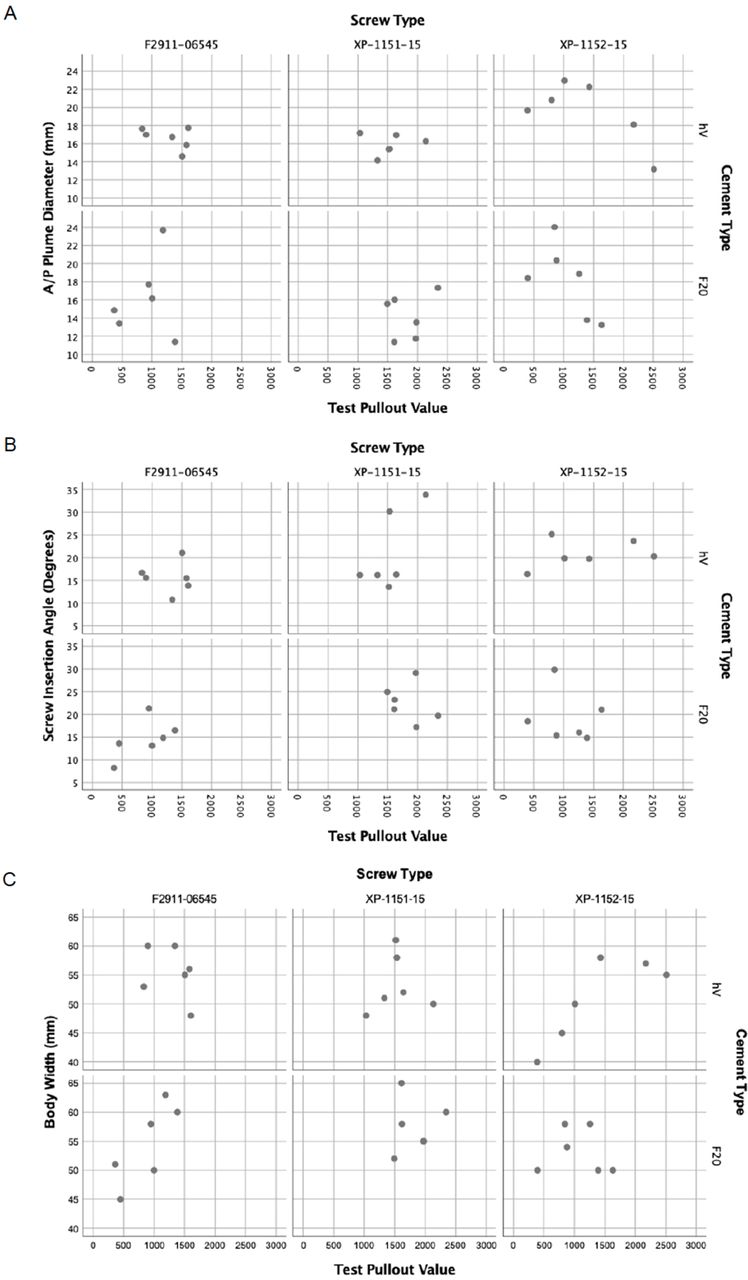
Dimensions and relationships of the cement plumes formed within the instrumented vertebra are presented in Supplemental Table 3. Results of correlation testing between plume geometry and pullout are presented in Figure 7. Only the A/P plume diameter was found to significantly correlate with pullout strength (coefficient = −0.420, P = 0.011) (see Figure 7A).

Vertebral testing: Correlation scatterplots of variables in pedicle screw instrumentation of 3 different screw designs, anterior-posterior (A/P) plume diameter, screw insertion angle, and vertebral body width were found to significantly correlate with pullout strength. (A) A/P plume diameter and pullout strength (coefficient = −0.420, P = 0.011); (B) screw insertion angle and pullout strength (coefficient = 0.381, P = 0.022); and (C) body width and pullout strength (coefficient = 0.395, P = 0.017).
Other measures that were found to significantly correlate with pullout strength were the screw insertion angle (Figure 7B: coefficient = 0.381, P = 0.022) and the body width of the vertebra (Figure 7C: coefficient = 0.395, P = 0.017). No statistically significant correlation was observed to exist between the BMD and pullout strength.
Vertebra: Distribution Pattern of the Cement Plume
Fenestration pattern was found to influence the distribution of the cement plume within the cortical bone of the vertebra. Illustrative examples of computed tomography-guided plume geometry analysis are presented in Figure 8. Of the 3 configurations, design 3 with the largest distance between fenestrations demonstrated a 22% incidence of cement extrusion into the pedicle and a 28% incidence of cement extrusion anterior to the tip of the screw. Design 1 with the most distal holes demonstrated a 28% incidence of cement extrusion anterior to the screw, but no cement within the pedicle. Design 2 with its intermediate pattern of fenestration distribution was found to confer a centrally distributed cement plume within the vertebral body but with purchase toward the root of the pedicle, without evidence of anterograde or retrograde cement leak in any instrumented specimen.
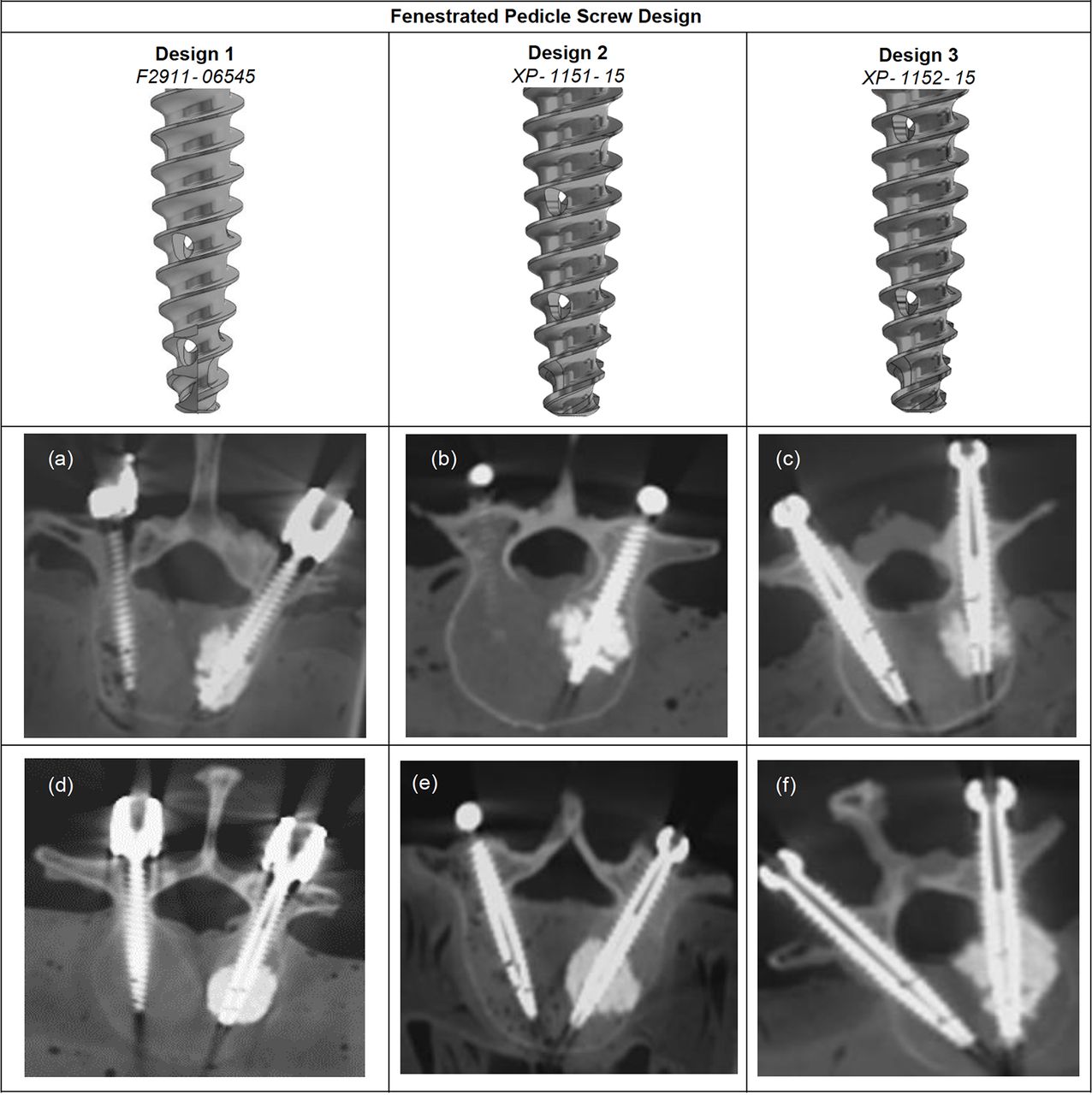
Illustrative examples of computed tomography-guided dimensional analysis of cement plume geometry formed with 3 different Everest fenestrated screw designs and 2 viscosities of Teknimed polymethylmethacrylate cement. Medium-viscosity (F20) plumes are represented in the top row (A–C); high-viscosity plumes (hV) are shown in the bottom row (D–F). Only design 2 demonstrated a consistently confined cement plume, with purchase toward the cortical bone of the vertebra, without anterograde or retrograde leak. Cement viscosity was not found to influence the plume distribution.
Vertebra: BMD
The mean BMD of the vertebral specimens was found to be 1.10 ± 0.27 g/cm2, with T scores ranging from −5.1 to 2.9, reflecting a mix of both healthy and osteoporotic specimens Supplemental Table 1.
Discussion
Cement augmentation is increasingly being conducted through injectable pedicle screws, particularly in osteoporotic patients.10 While it is widely accepted that PMMA augmentation results in superior fixation strength and outcomes,22 there is a lack of consensus in the literature regarding the optimal screw design,21,23,24,26–29 cement viscosity, volume,8 or mode of cement delivery.21,30–32
The importance of these interacting variables is undermined by the incidence of cement leak during augmented spinal instrumentation, where iatrogenic distribution of the cement plume results in adverse outcomes, ranging from clinically silent lesions to cement emboli and compressive radiculopathies, necessitating secondary intervention.16
Effect of Cement Augmentation on Pullout Strength
In both foam blocks and cadaveric vertebra, cement augmentation conferred a significant increase in the overall pullout strength of the construct. Our data align with the current literature of experimental ex vivo models, in which pedicle screw-cement augmentation significantly enhances axial pullout forces.27,31–34 A parallel and near identical experimental design by Charles et al35 demonstrated a 51.8% increase in median pullout forces with cement augmentation of fenestrated screws, which was comparable with the 63.8% increase observed with our study. A similar study by Goost et al36 demonstrated that cementation conferred a 110% increase in pullout strength in osteoporotic specimens, compared with the 50% increase seen in normal vertebra. While this supports the intrinsic finding of our study that cement augmentation enhances the strength of the bone-screw interface, no correlation between BMD and pullout strength was observed in this study.
Correlation Between Plume Geometry and Pullout Strength
In the foam block model, the lateral diameter of the cement plume was shown to correlate with the pullout strength. This finding reflects the principle that the resistance to pullout is related to the surface area normal to the direction of pull. Conversely, the lack of correlation between the A/P plume diameter and pullout strength in the foam blocks was unexpected, as the A/P diameter would be reflective of the length of interface between the cement and the cancellous bone. Given the linear direction of axial pullout force, it is perhaps expected that the perpendicular purchase afforded by the lateral plume diameter would thus result in a stronger counterforce to pullout.
These findings were unexpectedly reversed in the vertebral tests, in which pullout force was found to be significantly correlated with only the A/P plume diameter, and not lateral plume diameter (Supplemental Figure 3A). Given the difference in densities between the foam blocks and the vertebral specimens, with the latter representing a mix of healthy to osteoporotic specimens (Supplemental Table 1), we hypothesize that bone with poor density relies on the lateral plume diameter, while healthier bone is more dependent on the A/P plume dimension.
Other significant correlations with pullout strength were noted between vertebral body width and screw insertion angle, with increasing strength associated with larger body width and steeper insertion angles. The extent to which these findings may be extrapolated is limited by the small sample sizes of this study and highlights the need for further biomechanical studies in order to explore these relationships.
Of interest, we were unable to demonstrate a meaningful correlation between the pullout strength and the differing cement viscosities, nor the design of the screw in either the foam blocks or the vertebral specimens. This is a confounding result that is difficult to explain, as one would expect cement distribution throughout subcortical bone to be enhanced by its exit track, its inherent fluid properties, and the porous quality of the bone. In a similar study by Choma et al,24 a low-viscosity PMMA cement was found to enhance pullout strength when compared with a high-viscosity cement. These discordant findings warrant further investigation and repetition.
Distribution of Cement Plume in Relation to Fenestration Design
As described in the methodology and appendix, all 3 screw designs were assessed according to the distribution pattern of the cement plume. An important finding of this study is the consistent cement plume geometry formed by the XP-1151–15 (design 2) screw (Figure 1B). Previous studies have noted the variation of the cement plume formation across differing screw designs,12 and it is the opinion of the authors that an ideal plume would be wholly confined to the vertebral body, providing the greatest purchase strength and resistance to axial pullout, without retrograde or anterograde leakage (Figure 8B and E). Thus, a centrally distributed fenestration pattern is most likely to confer a predictable and favorable plume pattern.
A recent, robustly designed experiment by Liu et al8 examined the relationship between the material variables and determined that an optimal profile of 3 mL of PMMA through a 4-hole fenestrated screw would confer the greatest fixation stability. Of interest, they noted that the fenestration distribution favored a plume toward the cancellous bone of the pedicle conferred the greatest fixation strength. While our study was not able to replicate this finding, we note that the design 2 (Everest XP-1151–15) screw resulted in a similarly distributed plume, with purchase toward the pedicle. Taken together, these findings suggest a trend for a centrally distributed pattern of fenestrations being capable of conferring the most predictable plume pattern, which may confer the greatest biomechanical advantage from cement augmentation. Further studies are required to investigate this inference.
Limitations
The key limitation of this experimental study is the small sample size of test specimens. While some interesting and statistically significant patterns emerged during post hoc analysis, our ability to extract meaningful trends and subtle differences between the different screw-cement groups is limited by the small sample sizes (n = 6).
Of importance, we were unable to detect the effect of varying cement viscosity on plume geometry and pullout strength, nor did we observe a correlation between the BMD and pullout strengths. As this experimental design would ideally be conducted in purely osteoporotic vertebra where cementation is considered most relevant, the varying densities of the specimens present a limitation to this study due to the difficulty of procuring purely osteoporotic specimens (Supplemental Table 1). Nonetheless, the variability in the cohort was not found to influence the strength of pullout forces (Supplemental Figure 2J).
In an initial pilot test of the vertebral specimens, pullout of the control screw caused failure of both pedicles. The spinous process was therefore excised in order to decouple the instrumented pedicles during testing. However, this may have resulted in artificial weakening of the specimens. The results may have been further confounded through the use of wire and spacers to help secure the specimens. This is likely to have contributed to the large SD observed in the pullout values of the vertebral test group.
It is important to note that the pullout test itself presents a limitation on the clinical application of our experimental findings. While used in the literature as a means of standardizing tests of fixation integrity,37 studies have noted that the linear, unidirectional pullout force used in these studies fails to reflect the biomechanical reality of in vivo screws. In view of this, there is a growing appreciation for the need to develop dynamic, translational testing methods of implant fixation strength.37,38
Conclusion
We examined 3 different fenestration patterns and the resulting plume distribution following injection of both medium- and high-viscosity PMMA cements. In addition to biomechanical testing, radiographic analysis was conducted to clarify the distribution profiles that might provide the optimal profile for fenestrated pedicle screw fixation within osteoporotic spines.
In accordance with the literature, we demonstrated that cement augmentation confers a significant increase in the stability of pedicle screw fixation of osteoporotic vertebra, when tested by axial pullout. However, this biomechanical advantage was not able to be attributed to either the fenestration pattern of the screws or the viscosity of the injected cement. Pullout strength was found to correlate with some geometric measures of the cement plume. Lateral plume diameter, AP diameter, and screw insertion angle appear to be measures that influence the fixation strength of augmented specimens and warrant further investigation as potential targets for further optimizing methods of spinal fixation.
In assessing the effect of fenestration distribution on cement plume formation, a centrally distributed pattern conferred the greatest predictability with the least leak. While no particular screw-cement group demonstrated a clear biomechanical advantage, the design 2 screw was shown to result in a cement plume formation likely to be associated with fewer complications due to unpredictable cement leak. Given the growing use of fenestrated pedicle screws in osteoporotic spine instrumentation, larger biomechanical studies are required in order to develop consensus regarding the optimal profile for cement augmentation of fenestrated pedicle screws.
Footnotes
Funding Funding was obtained via institutional support from Macquarie University, K2M, Life Healthcare, DepuySynthes and Medtronic.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval All experimentation was granted ethical approval and were conducted in accordance with institutional policies.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}