


Abstract
Background Anterior cervical discectomy and fusion (ACDF) at 3 or more levels remains challenging, with reported high pseudarthrosis rates and implant-related complications. Porous surface polyetheretherketone (PEEK) interbody cages are newer implants for ACDF with limited data available for their use in ACDF procedures at 3 or more levels. The objective of this study was to assess the clinical and radiographic outcomes of porous PEEK devices for ACDF at 3 or more levels.
Study Design Retrospective case series.
Methods Consecutive patients who underwent primary ACDF for degenerative cervical disc disease at 3 or more levels with porous PEEK cages with anterior plate instrumentation were included. Clinical outcome scores, radiographic parameters, pseudarthrosis rates, and cage subsidence rates were assessed. Preoperative and postoperative clinical outcomes and radiographic measures were compared using paired t tests.
Results A total of 33 patients with ACDF at 3 or more levels with porous PEEK cages were included, with minimum 1-year follow-up. Two patients had cage subsidence (6.1%), and 1 patient had pseudarthrosis (3.0%). There were significant postoperative increases in overall cervical lordosis, sagittal vertical axis, fusion segment lordosis, T1 slope, and disc height. Clinical outcomes showed significant improvement from the preoperative visit to the final postoperative follow-up.
Conclusions High rates of fusion (97.0%) were observed in this challenging patient cohort, which compares favorably with previously published rates of fusion in ACDF at 3 or more levels.
Clinical Relevance The optimal management of cervical spinal pathology regarding approach, technique, and implants used is an active area of ongoing investigation. The high levels of radiographic and clinical success utilizing a relatively novel implant material in a high-risk surgical cohort reported here may influence surgical decision making.
Level of Evidence 3.
Introduction
Anterior cervical discectomy and fusion (ACDF) demonstrates reliable improvement in symptoms of radiculopathy and myelopathy associated with anterior spinal pathology in appropriately selected patients.1–5 Patients with multilevel disease may require multilevel discectomy and fusion. However, ACDF involving multiple levels has been associated with increased risk of pseudarthrosis with rates of up to 56% reported for ACDF at 3 or more levels.6 Pseudarthrosis may result in mechanical axial pain as well as recurrence of index level symptoms and necessitate revision surgery.6,7
A myriad of implants, biologics, and techniques have been described and developed to promote fusion and reduce risk of pseudarthrosis in ACDF procedures. While strut autograft demonstrates high fusion rates, numerous alternatives, including machined allograft, titanium, and polyetheretherketone (PEEK) cages, were developed to reduce donor-site morbidity associated with structural autograft.8 Titanium cages provide structural integrity, and porous surface promotes osseointegration, though they are limited by radiopacity and risk of subsidence.9 Conversely, smooth PEEK has a modulus of elasticity similar to that of bone, theoretically reducing the risk of stress shielding, endplate fracture, and subsidence; however, it has a hydrophobic inert surface. A recent study demonstrated a 5-fold increased rate of pseudarthrosis for a single-level ACDF using smooth PEEK cages technique.7 Smooth PEEK cages in multilevel ACDF have also demonstrated higher rates of pseudarthrosis compared with structural allograft.10
Recently, porous surface PEEK cages have been developed to promote surface bony ingrowth, enhance osseointegration, and improve fusion rates.11–13 Porous PEEK is manufactured by extruding PEEK through sodium chloride crystals, followed by leaching of embedded sodium chloride crystals in water to leave behind a porous surface layer.14 Initial biomechanical and in vitro studies have demonstrated bony ingrowth and improved fusion rates in the near term.15 There are limited data regarding the clinical outcomes and fusion rates of porous PEEK interbody cages.12–14,16 To our knowledge, the present study is the first to evaluate the clinical outcomes of patients undergoing ACDF procedures of 3 or more levels using these novel porous PEEK interbody implants.
Materials and Methods
A multicenter retrospective case series was performed at 3 institutions. Patients undergoing multilevel ACDF with porous PEEK cages for symptoms of degenerative cervical disc disease (radiculopathy or myelopathy) at 3 or more levels from January 2016 to October 2018 were included. All included patients had at least 1 year of clinical and radiographic postoperative follow-up. Patients were excluded from study if at the time of surgery, they were younger than 18 years, or were being treated for malignancy, trauma, or an infection.
Three fellowship-trained spine surgeons performed all procedures. Porous PEEK ACDF cages (COHERE, NuVasive, San Diego, CA) were filled with bioactive graft material according to surgeon preference. One surgeon used nanOss Bioactive 3-dimensional bone void filler (RTI Surgical, Marquette, MI), 1 surgeon used BioSphere Putty (Synergy Biomedical, Wayne, PA), and 1 surgeon used Osteocel (NuVasive, San Diego, CA). The Rush University Institutional Review Board granted approval for this study (Office of Research Administration No. 18080303) with a waiver of informed consent due to the retrospective nature of the study, usage of deidentified data, and minimal risk to subjects. The 3 surgeons who performed the procedures receive consulting fees/royalties from NuVasive (San Diego, CA), which manufactures porous PEEK cages. These authors who received royalties performed final review of the manuscript; however, they were not involved in data collection, radiographic assessment (including fusion assessment), clinical outcome assessment, or statistical analysis of data. No funding was received for this study.
Preoperative data collection included age, sex, body mass index (BMI), presence of diabetes mellitus, smoking status, and number of fusion levels for all included patients. Preoperative patient-reported outcome scores collected included visual analog scale (VAS) neck pain, VAS arm pain, and Neck Disability Index (NDI) scores. Preoperative radiographic data collected included C2-C7 lordosis, cervical sagittal vertical axis (SVA), planned fusion segment lordosis, T1 slope, lordosis proximal/distal to planned fusion segment, and disc height on neutral lateral radiographs.
The surgical technique in all cases involved a traditional anterior approach to the cervical spine and thorough discectomy at each of the fused levels. After initial disc release and removal, caspar pins are used to distract the disc space and provide access to perform the decompression. A high speed burr is utilized to remove cartilaginous endplate and posterior osteophytes as well as to plane flat any endplate deformity to facilitate uniform cage fit. This technique is applied sparingly, so as to maintain the endplate’s structural integrity and minimize the risk of implant subsidence.
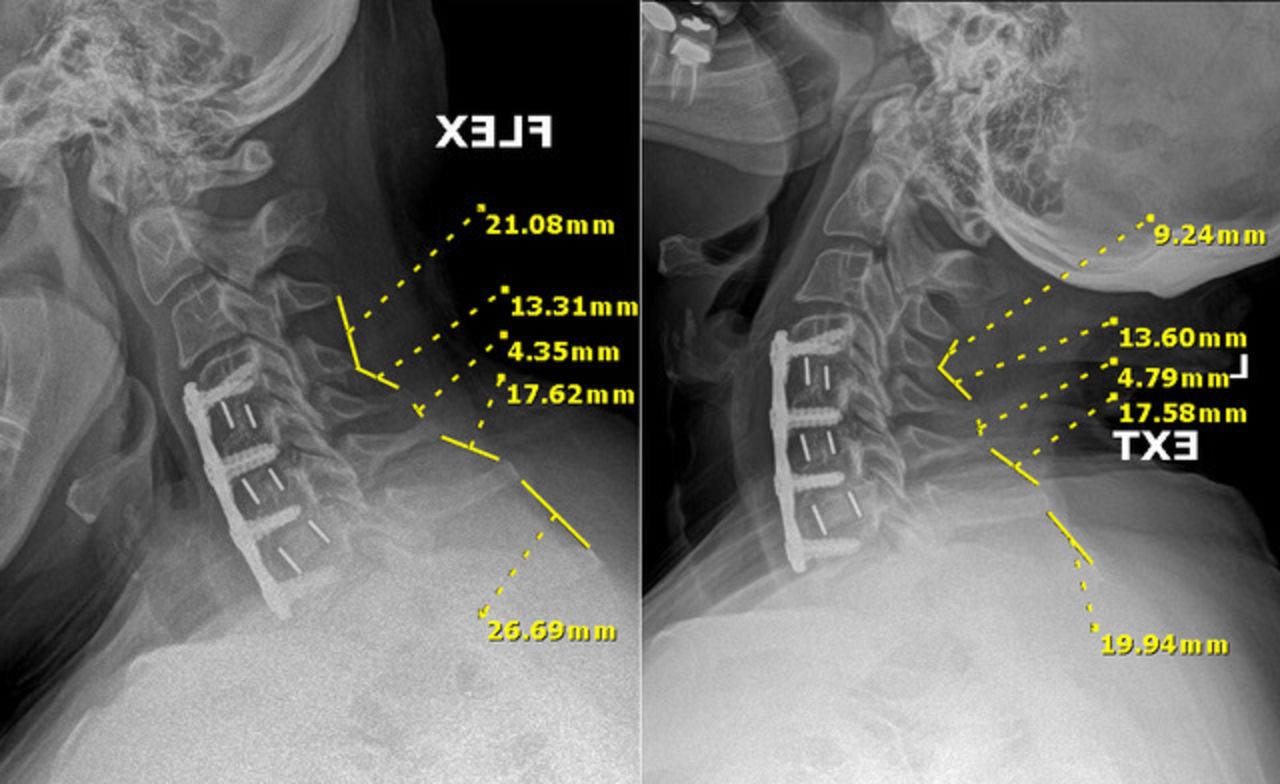
Postoperatively, clinical outcome scores and radiographic outcomes were again assessed. At the first postoperative visit, radiographic outcomes of C2-C7 lordosis, SVA, fusion segment lordosis, T1 slope, lordosis proximal/distal to fusion segment, and disc height were assessed on neutral lateral radiographs. At the final postoperative visit, the above radiographic outcomes were again assessed, along with clinical outcomes (VAS neck, VAS arm, and NDI). Evidence of pseudarthrosis and graft subsidence was assessed on final follow-up radiographs by 2 independent reviewers. Pseudarthrosis was defined as the lack of bony bridging between fused segments, motion greater than 1 mm per fused level between spinous processes on flexion and extension views,6 or the lack of bridging bone in 2 planes on computed tomography image, when available.17 Patients demonstrating fusion by the above criteria had images magnified >150% and had at least 4 mm of motion at an adjacent unfused segment to ensure appropriate effort consistent with Cervical Spine Research Society criteria (Figure 1).17 Subsidence was defined as the loss of disc height ≥2 mm from immediate postoperative to final follow-up radiograph.

Postoperative lateral radiograph in flexion (left) and extension (right) demonstrating measurments made to assess fusion at the addressed levels. Cervical Spine Research Society critera were utlized.
Statistical analysis was performed using Stata version 13.1 (StataCorp LP, College Station, TX). Baseline patient characteristics were compared using χ 2 and analysis of variance tests for categorical and continuous data, respectively. Two-sided t tests were used to compare differences in clinical and radiographic outcomes. Statistical significance was set at P < 0.05.
Results
A total of 33 patients met inclusion criteria (Table 1), with a mean age of 58.8 ± 8.7 years and mean BMI of 31.3 ± 7.2 kg/m2. Of that, 60.6% of patients were women, 29.2% had a smoking history, and 25.9% were current smokers. The mean follow-up time was 16.8 months with a minimum of 1-year follow-up. Out of these patients, 22 patients (66.7%) had a 3-level procedure, 10 patients (30.3%) had a 4-level procedure, and 1 patient (3.0%) had a 5-level procedure for a total of 111 fused levels.
Demographics of included patients (N = 33).
Two patients demonstrated cage subsidence (6.1% of patients, 1.8% of fused levels), and 1 patient had radiographic evidence of pseudarthrosis (3.0% of patients, 0.9% of fused levels) who required reoperation (3.0% of patients). The 1 pseudarthrosis case was observed in a 55-year-old female smoker with BMI 35 who underwent C3-C7 ACDF and, subsequently, underwent a C3-T2 posterior spinal fusion 6 months postoperatively due to ongoing neck pain consistent with nonunion. When comparing radiographic measurements (Table 2), there was a significant increase in preoperative-postoperative and preoperative-final C2-C7 cervical lordosis (pre-post 1.1–10.4°, P < 0.001; pre-final 1.1–9.6°, P = 0.001). Furthermore, there were significant increases in SVA (pre-post 23.1–28.1 mm, P = 0.002; pre-final 23.1–28.7 mm, P = 0.008), fusion segment lordosis (pre-post −1.7 to 8.7° P < 0.001; pre-final −1.7 to 8.7°, P < 0.001), T1 slope (pre-final 24.5–29.1°, P = 0.022), and disc height (pre-post 2.6–3.5 mm, P = 0.008; pre-final 2.6–3.2 mm, P = 0.019) following ACDF. All clinical outcomes (Table 3) showed significant improvements from the preoperative to final follow-up visits (NDI 22.3–9.6, P < 0.001; VAS neck 3.5–1.0, P < 0.001; VAS arm 5.2–0.6, P < 0.001).
Differences in radiographic outcomes between preoperative, postoperative, and final follow-up.
Preoperative and postoperative patient-reported outcomes.
Discussion
While numerous implants and techniques have been described to promote fusion and eliminate structural autograft donor-site morbidity associated with ACDF procedures, ACDF involving multiple levels has historically been associated with a high risk of pseudarthrosis, particularly with 3 or more levels.6 In many instances, concomitant supplemental posterior instrumentation has been recommended, adding considerable morbidity and cost to the procedure.18 To the authors’ knowledge, this is the first study to report on the outcomes of patients undergoing ACDF procedures of 3 or more levels using porous PEEK interbody cages. This study demonstrates successful clinical outcomes with a 97% fusion rate and low reoperation and subsidence rates in patients with at least 1 year of postoperative follow-up. Radiographically, use of a porous PEEK cage led to significant improvements in disc height, T1 slope, SVA, and C2-C7 and fusion segment lordosis.
The goal of intervertebral cages in ACDF is to maintain disc height after discectomy while bony fusion occurs across the disc space. However, due to performance trade-offs in currently available biomaterials, the ideal intervertebral cage design has been elusive. Metallic implants with various surface architectures provide high strength and facilitate bony ingrowth; however, they are associated with imaging artifacts that make fusion assessment challenging. Metallic implants also may lead to bone resorption and subsidence due to high modulus of elasticity relative to bone and stress shielding. Smooth PEEK cages do not interfere with imaging and have favorable mechanical properties, such as a modulus of elasticity that is similar to bone; however, these devices have been shown to be associated with a lack of bony ingrowth due to their hydrophobic and chemically inert surfaces. Porous surface PEEK cages were recently developed to combine the beneficial mechanical and imaging properties of PEEK with the favorable bony ingrowth capacities of surface porosity to improve fusion rates.11–13 Porous PEEK is associated with improved osteogenic differentiation in vitro and greater implant fixation in vivo when compared with smooth PEEK and titanium-coated PEEK.15
In this study, patients with ACDF at 3 or more levels with porous PEEK interbody graft experienced low rates of pseudarthrosis (3.0%), suggesting acceptable rates of osseointegration 1 year after surgery. This pseudarthrosis rate is lower than has been previously reported in the literature for ACDF at 3 or more levels with traditional autograft, allograft, titanium cages, or smooth PEEK cages (6–42%).6,19–22
Laratta et al retrospectively assessed 46 patients who underwent 3- or 4-level ACDF with smooth PEEK or titanium cages with plate fixation and found a 24% reoperation rate for nonunion.21 In a different retrospective single-institution study, De la Garza-Ramos et al used structural autograft or allograft and found a 5.6% pseudarthrosis rate in 3-level ACDF patients and 15.4% in the 4-level ACDF patients.20 Wewel et al retrospectively assessed 72 patients who had 3- and 4-level ACDF with structural allograft and found a 42% pseudarthrosis rate in 3-level ACDF patients and 56% in 4-level ACDF patients.6 Chen et al compared stand-alone PEEK cages vs PEEK cages with plate fixation in 54 three-level ACDF patients and found cage subsidence in 13 and 5% of segments, respectively, with pseudarthrosis rates of 14 and 8%, respectively.19 The reported increase in pseudarthrosis seen in multilevel ACDF is due to greater graft-bone interfaces required for fusion and altered biomechanics at several segments.21 Pseudarthrosis in multilevel ACDF may also be related to technical factors, and in ACDF cases at 4 or more levels, plate fixation and positioning can be especially challenging. While no complications were noted in the present study specifically in terms of fixation failure, the authors recommend thorough removal of anterior vertebral osteophytes, wide exposure of the disc spaces, and initial screw fixation at the proximal and distal ends of the plate to facilitate plate positioning.
While the use of a composite interbody cage in anterior cervical fusion comes with the risk of stress shielding, endplate microfracture, subsequent cage subsidence, and loss of clinical outcome durability,23–25 the favorable modulus of PEEK may reduce this risk.13,26–29 In this study, when combined with anterior plating, porous PEEK cages had radiographic evidence of subsidence in only 5.1% of cases. In reports of 1- or 2-level ACDFs using smooth PEEK cages and anterior plating, subsidence has been reported in 9.7 to 38.5% of cases between 6 and 24 months of follow-up.30 Additionally, in the present study, porous PEEK cages had acceptable improvements and relative maintenance in disc height, SVA, C2-C7 lordosis, and fusion segment lordosis, postoperatively (Figure 2). These outcomes remained significant at the time of final follow-up, 1 year after surgery. While the numerical mean C2-C7 cervical lordosis at final follow-up was less than mean C2-C7 cervical lordosis at final follow-up, this difference was within 1° and was not statistically significant. This was likely due to minor variability in radiographic measurements. Additionally, while the numerical mean proximal adjacent segment lordosis decreased at final follow-up, this difference was not statistically significant and is well within the margin of measurement error and not likely a complication from the procedure. Last, while the mean disc height was less at final follow-up compared with mean disc height at the immediately postoperative visit, this difference was quite small (0.29 mm) and while statistically significant, it did not meet the threshold for subsidence and was therefore likely clinically insignificant.

Preoperative (left) and postoperative (right) lateral radiographs of an exemplary case indicating achievement of multilevel lordosis and restoration of disc space height without subsidence. Robust interbody fusion is demonstrated at the operated levels.
This study has several limitations. First, this is a retrospective study and is limited by the number of included patients. Similarly, this study also lacked a specific control group, and conclusions on the effectiveness of porous PEEK models are limited to comparisons between historical studies. Additionally, 3 different biologic agents were used in our cohort based on surgeon preference; this factor may have affected fusion rates. Longer-term follow-up may have elucidated more significant outcomes. However, despite these limitations, to the authors’ knowledge, this is the first report of porous PEEK cages for ACDF at 3 or more levels.
Conclusion
The present study assessed porous PEEK cages for ACDF procedures at 3 or more levels and supports that these devices are a clinically viable alternative for achieving successful outcomes. High rates of fusion (97.0%) were observed in this challenging patient cohort, which compares favorably with previously published rates of fusion in ACDF at 3 or more levels. While these implants show promise, additional studies are needed to further validate the efficacy of porous PEEK interbody cages in multilevel ACDF procedures.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Gilberto Gomez reports consulting fees, royalties/licenses, and stock/stock options and patents planned, issued, or pending from Orthopedic Designs North America. Frank Phillips reports royalties/licenses from NuVasive and SI Bone; consulting fees from NuVasive, Globus, Spine Art, Spinal Kinetics, Medtronic, and Stryker; leadership or fiduciary role with Theracell, Edge Surgical, SMISS, ISASS; and stock/stock options from Surgio, NuVasive, Providence, Spinal Simplicity, Mainstay, and Augmedics. The remaining authors have no disclosures.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.