


Introduction
Chile is a country with an area of 756,102 km2.1 It spans a distance of 4270 km (2653 miles) of coastline from north to south, which creates problems in delivering sophisticated health care in rural areas. It is the 38th largest country in the world by size.2 It was founded in 1810 as an independent republic.3 In addition to Spanish (the official spoken language), Chile has 6 indigenous languages. However, only 20% of the indigenous populations speak their native tongue. About 40% of Chile’s population of 19 million lives in the region of Santiago.
Chile is traditionally considered a model in Latin America in terms of political and financial transparency.4 It has also been one of the fastest growing economies in Latin America in the past decade, allowing the country to reduce poverty significantly.5 However, the World Bank estimates that the impacts of the COVID-19 crisis could reverse years of growth in the Chilean middle class.5 Despite recent efforts to diversify its economy, Chile’s economy relies heavily on copper exporting; thus, the country remains vulnerable to international copper prices and global demand (mainly from China).6 Within Latin America, Chile ranks fourth in gross domestic product after Brazil, Mexico, and Argentina with $331,250 billion.7 According to figures provided by the International Monetary Fund in April 2021, the most developed economies in Latin America in terms of gross domestic product per capita are Panama with $30,390 and Chile with $24,930.8
Spine-Related Disease Burden in Chile
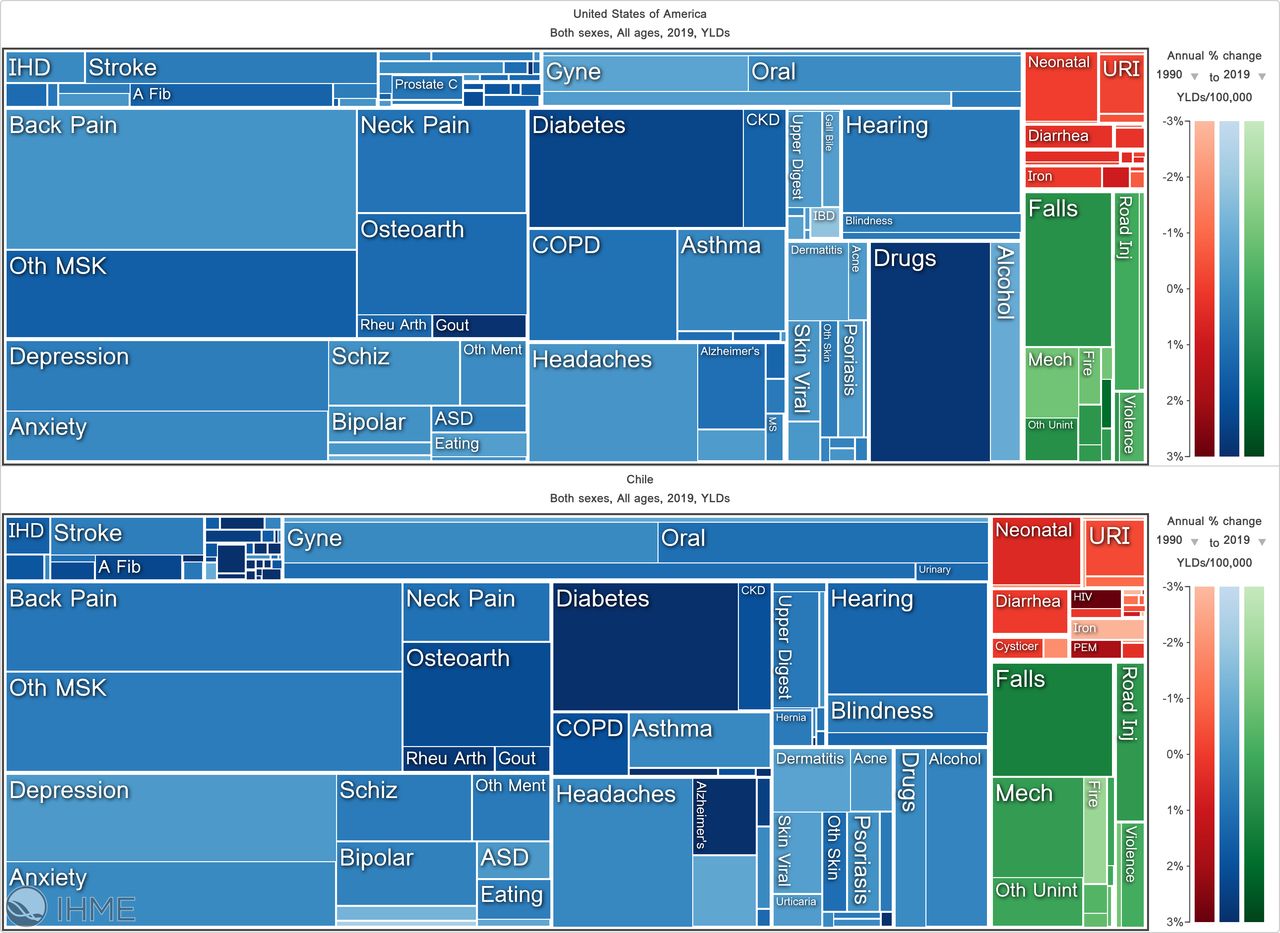
According to the Institute for Health Metrics and Evaluation, the disease burden expressed in years lived with disability (YLDs) data from Chile for all genders and ages is substantial (Figure 1). The Chilean YLDs due to low back pain were 7.7% of total YLDs (6.37%–9.16%) in 2019, with an annual change rate of −0.83%. In comparison, the US 2019 low back pain percentages were 10.38% of total disability-adjusted life years (9.38%–12.1%) with an annual change rate of 0.077%. The 2019 YLDs numbers were 5697152.11 (4114138.91–7474689.77) for the United States and 166912.76 (570421.30–435002.97) for Chile. The disease burden due to musculoskeletal disorders increased in Chile from 1990 to 2019 by 33.7%, making it the number 1 condition with the highest 2019 YLDs numbers: 2658.78 (1896.19–3543.16; Figure 2). The increasing socioeconomic status of the Chilean population is reflected by the changes in developmental assistance for health (DAH). After 2010, DAH resources were shifted from Latin-American countries to Sub-Saharan Africa (Figure 3). In 2018, only $1.3 (4.22%) of the $39 billion DAH money was allocated to Latin-American and Caribbean countries (Figure 4). Instead of infectious and communicable conditions, which remain the focus of global DAH expenditures in third world countries, chronic diseases, such as musculoskeletal and cardiovascular conditions, are the focus of today’s modern Chilean national health service (Figure 5). Management of spinal conditions plays out in this context of a change in modern Chilean society’s socioeconomic demographics.

Illustrative tree map of causes and disease burden expressed in years lived with disability (YLDs) comparing 2019 data from Chile and the United States for all genders and ages. The Chilean YLDs for low back pain were 7.7% of total YLDs (6.37%–9.16%) with an annual change rate of −0.83%. The US 2019 low back pain percentages were 10.38% of total disability-adjusted life years (9.38%–12.1%) with an annual change rate of 0.077%. The 2019 YLDs numbers were 5697152.11 (4114138.91–7474689.77) for the United States and 166912.76 (570421.30–435002.97) for Chile. Source: Institute for Health Metrics and Evaluation (IHME). Used with permission. All rights reserved. A fib, atrial fibrillation; ASD, autism spectrum disorder; COPD, chronic obstructive pulmonary disease; CKD, chronic kidney disease; IBD, inflammatory bowel disease; IHD, ischemic heart disease; MS, multiple sclerosis; MSK, musculoskeletal; Oth, other; URI, upper respiratory infection; PEM, post-exertional malaise.

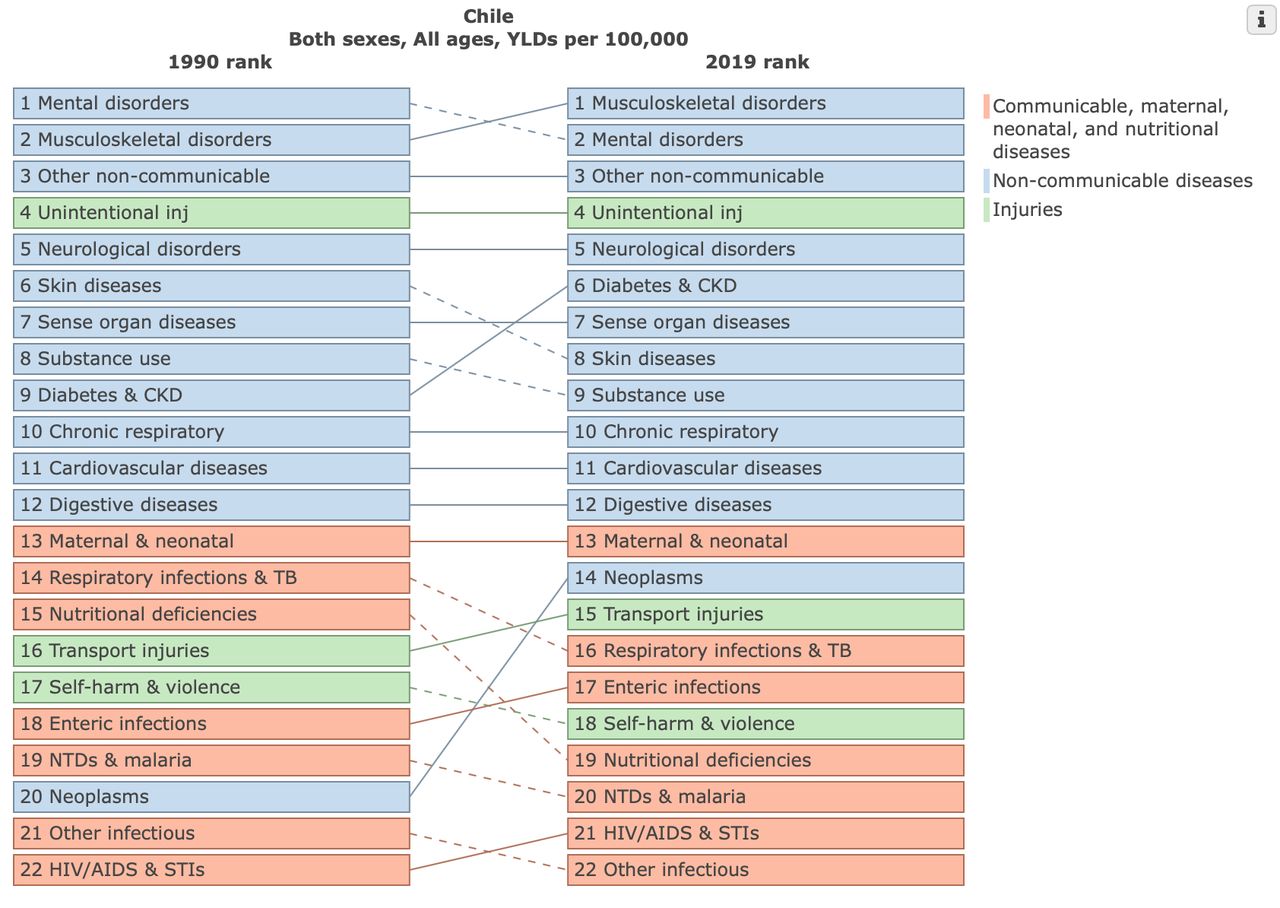
Comparative ranking of disease groups expressed in years lived with disability (YLDs) per 100,000 comparing 1990 with 2019 data from Chile for all genders and ages. There was a 33.7% increase in YLDs of musculoskeletal disorders from 1990 to 2019. They were ranked as the number 1 condition with the highest 2019 YLDs numbers: 2658.78 (1896.19–3543.16). Source: Institute for Health Metrics and Evaluation. Used with permission. All rights reserved. CKD, chronic kidney disease; inj, injury; NTDs, neglected tropical diseases; inj, injury; STIs, sexually transmitted infections; TB, tuberculosis.

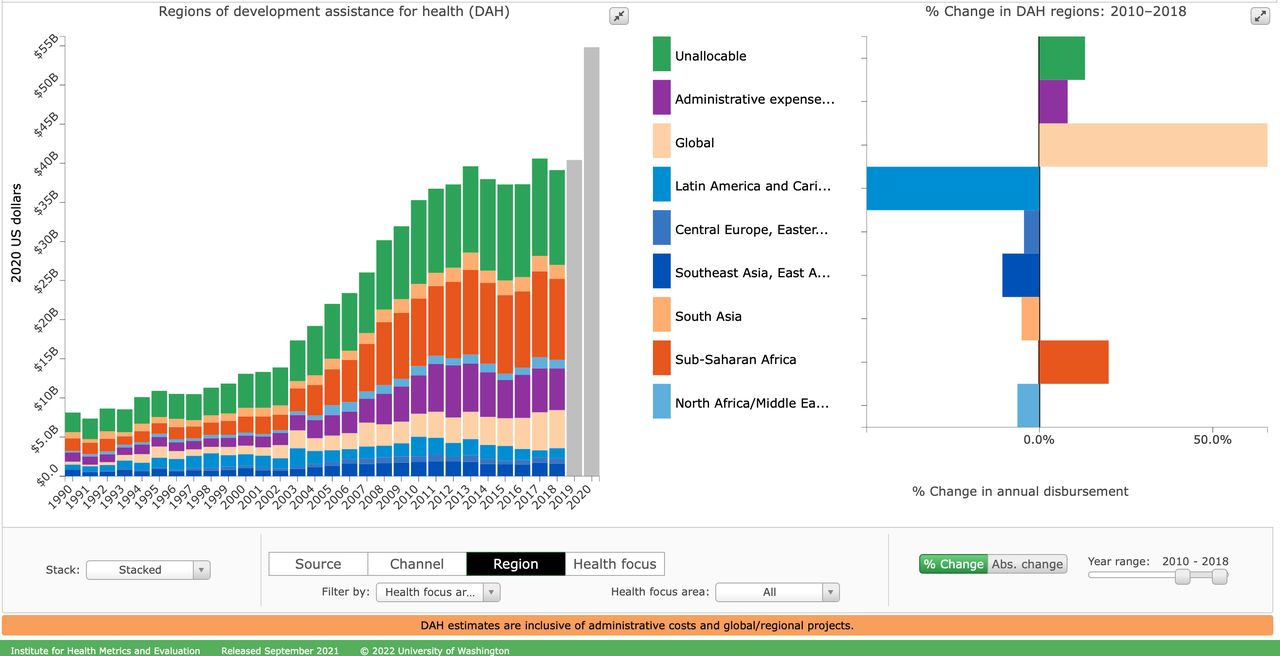
Changes in developmental assistance for health (DAH) by region to 2020 show an increase from $620 million to $2.5 billion in 2010. After 2010, DAH resources were shifted to sub-Saharan Africa with an absolute increase of $1.7 billion in 2018. During the same time frame, DAH spending in Latin-American countries decreased by $1.2 billion. Source: Institute for Health Metrics and Evaluation. Used with permission. All rights reserved.

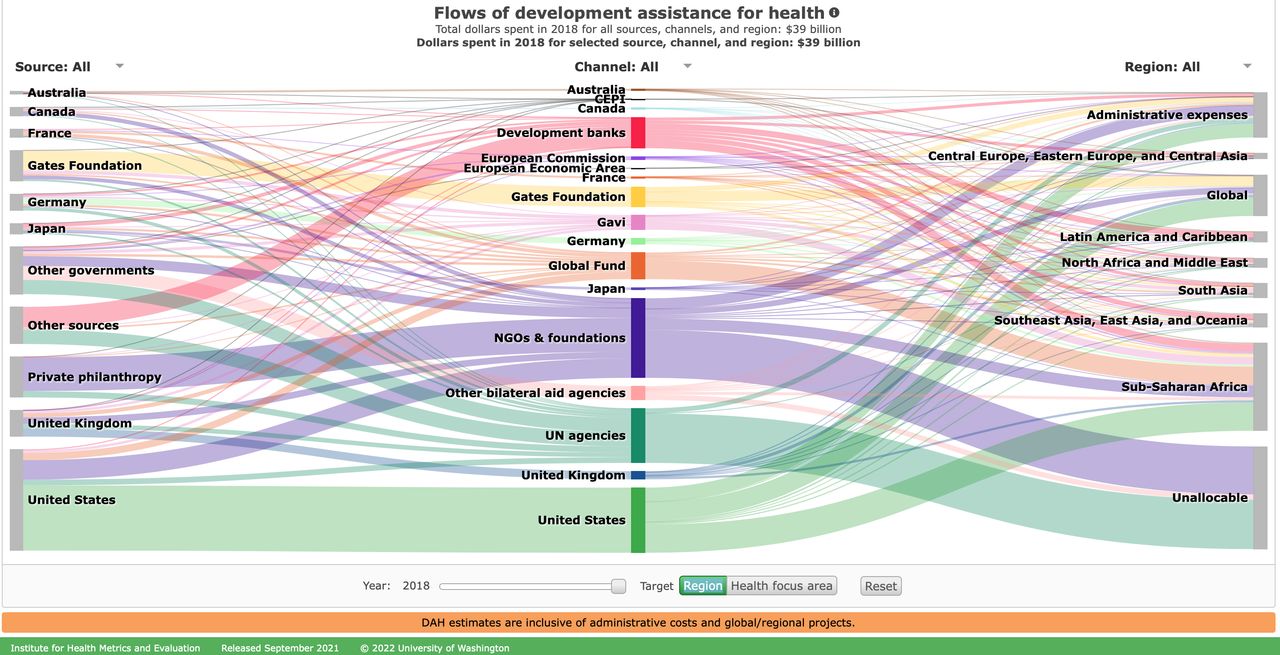
Flows of developmental assistance for health (DAH) spent in 2018 by region are shown. Total dollars spent for all sources, channels, and health focus areas were $39 billion. Only $1.3 billion (4.22% of DAH) was allocated to Latin-American and Caribbean countries. The majority of DAH dollars went to Sub-Saharan Africa ($10 billion; 26.51%). Source: Institute for Health Metrics and Evaluation. Used with permission. All rights reserved. NGOs, nongovernmental organizations; CEPI, Coalition for Epidemic Preparedness Innovations.

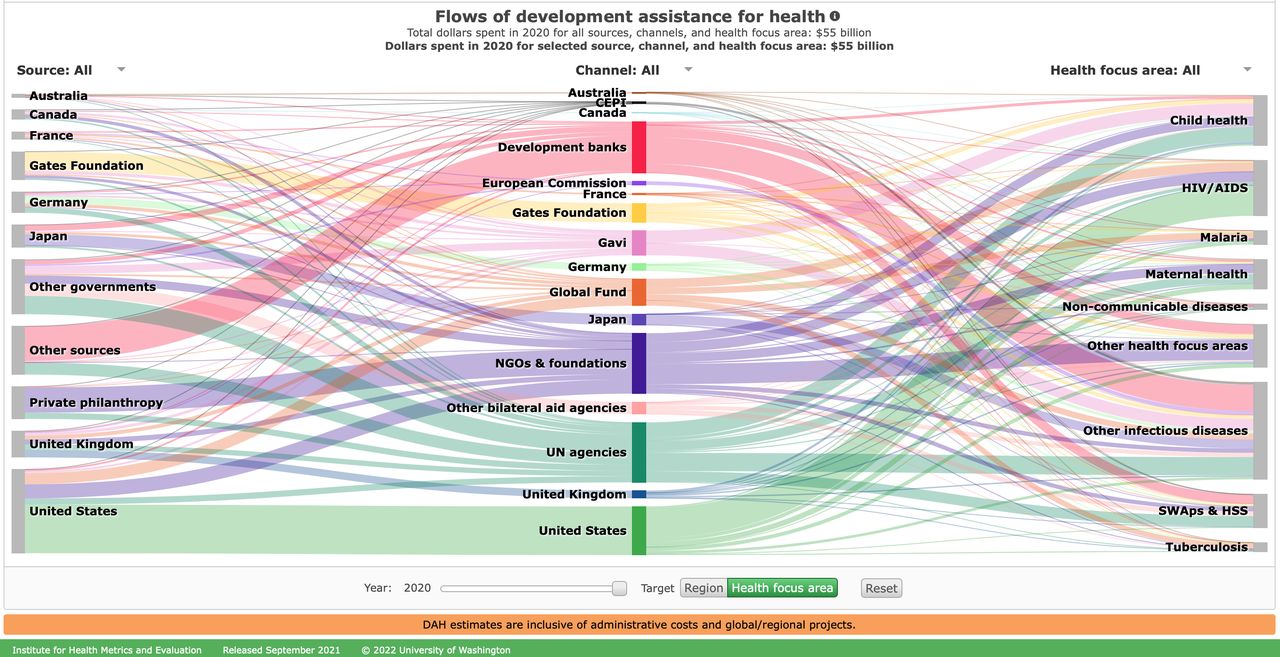
Flows of development assistance for health (DAH) globally in 2020 are shown. Total dollars spent for all sources, channels, and health focus areas were $55 billion. The majority of DAH spending was for infectious diseases: HIV/AIDS, $9 billion (16.37%); other infectious diseases, $16 billion (28.65%); malaria, $2.3 billion (4.14%); and tuberculosis, $1.5 billion (2.78%). Source: Institute for Health Metrics and Evaluation. Used with permission. All rights reserved. NGOs, nongovernmental organizations; CEPI, Coalition for Epidemic Preparedness Innovations; HSS, health systems strengthening; SWAP, sector-wide approaches.
Orthopedic and Spine Surgery in Chile
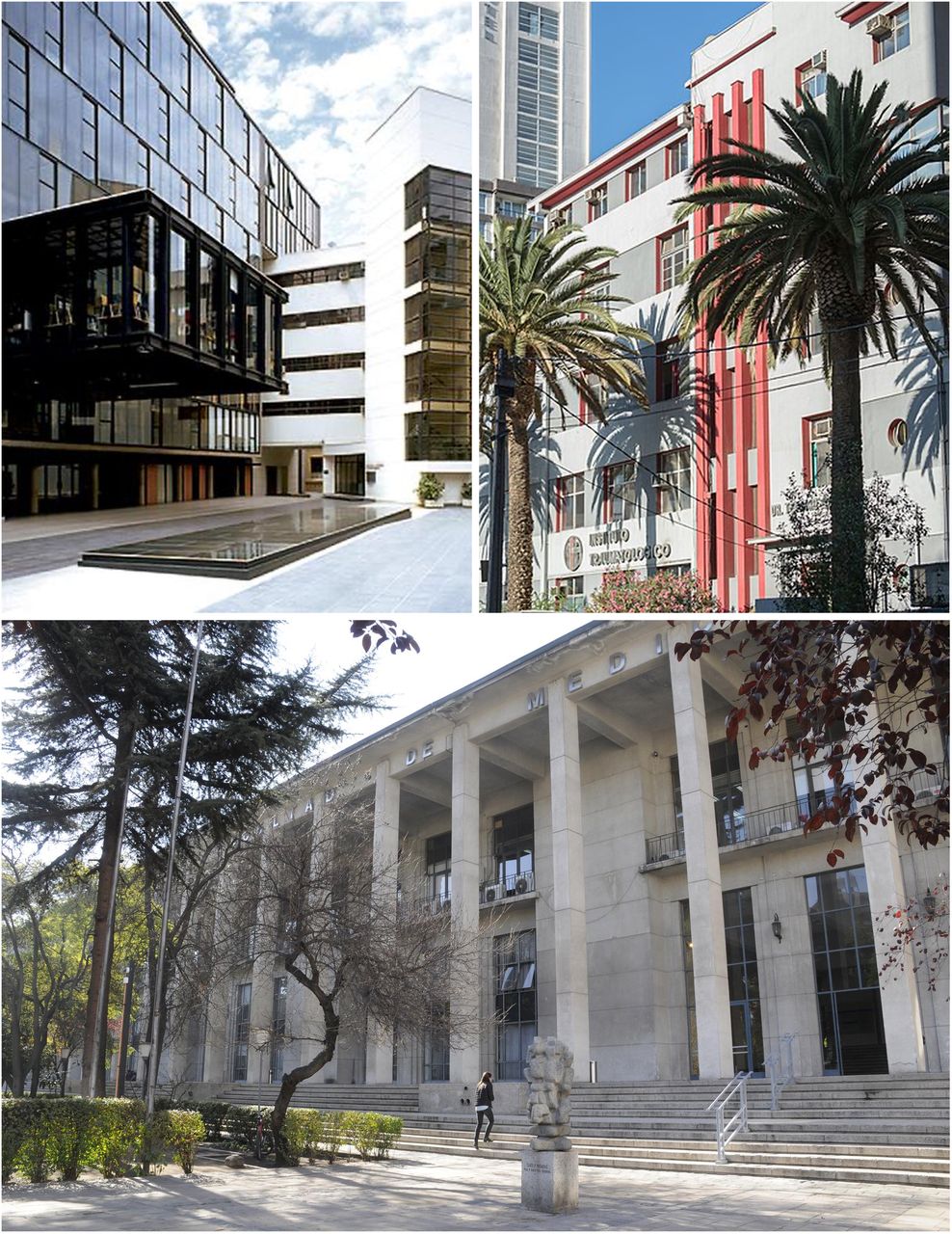
Orthopedic surgery in Chile began to develop as a discipline in the 1920s. It was established as a specialty with the inauguration of the Traumatology Institute in 1937 under the direction of Dr. Teodoro Gebauer, where musculoskeletal pathology began to be treated regularly.9 The Society of Orthopedics and Traumatology was founded in 1949 under the leadership of Dr. Ernesto Prieto to create a scientific society that would promote the study, teaching, and research of musculoskeletal pathology.9 The first university in Chile was the University of Chile, founded in 1843.10 In the past 30 years, there has been an explosion in the number of new universities, going from 6 in 1990 to 55 today, of which 22 have a medical school (Figure 6).

Chile’s leading medical institutions include the Instituto Traumatológico (top left), the University of Chile Medical School (top right), and the Medical School of the Universidad Catolica (bottom).
Just as the number of physicians has increased in Chile, the number of orthopedic surgeons and specialists in spinal surgery has also increased. In the 1990s, there were about 20 surgeons who performed spine surgery on a regular basis. Currently, the number of spine surgeons is around 120 in Chile (including orthopedics and neurosurgery). There is no accurate record of the number of spinal surgeries in the country. However, there is no doubt that the number of surgeries has increased substantially in recent years.
Chilean Spine Registry—Registro de Columna en Santiago
In 2019, a spine registry (Registro de Columna en Santiago) was started. This registry records spine surgeries performed in 9 Santiago hospitals, which include public and private institutions. To date, some 1255 surgeries have been registered. Of these, 72% were completed for degenerative pathology, 9% for traumatic injuries, 9% for deformities, 8% for tumor, and 2% for infectious causes. The most frequent diagnoses were herniated nucleus pulposus with 34%, spinal stenosis with 17%, fracture with 7%, and scoliosis with 5%. Fusions were performed in 54% of surgeries, and 46% were noninstrumented surgeries. Minimally invasive surgery has gained popularity in Chile within the past 10 years. Five years ago, endoscopic spine surgery started to replace tubular retractor-based minimally invasive surgeries, amounting to 5.4% of all Registro de Columna en Santiago registered surgeries to date. The endoscopic method is increasingly replacing traditional translaminar lumbar decompression techniques for herniated disc and spinal stenosis. The Traumatological Hospital of Santiago established an endoscopic training program consisting of hands-on clinical and cadaver training sessions. Clinical research in spine surgery in Chile, such as the recent article on short-segment vs long-segment posterior fixation in unstable spine fractures by Cabrera et al,11 is focused on common problems encountered in a community-based spine care model under a single-payer system.
Spine Surgery and The Chilean National Health Fund
On 7 September 2019, a decree approving the Explicit Health Guarantees (GES) was published in the Official Gazette (El Mercurio), and it has been enforced since 1 October 2019. It guarantees coverage of 85 diseases through the National Health Fund (Fonasa) and the Health Insurance Institutions (ISA). Scoliosis surgery in those younter than 25 years and surgery for herniated discs remain within them, but unfortunately, spinal stenosis and other degenerative diseases, which have been associated with high inpatient health care expenditures, have been omitted. GES guarantees a quick solution after the initial consultation by aiding the public or private health provider. Despite these assurances, waiting lists have grown to several months for lumbar disc herniations. With the prioritization of these GES problems in the spine, the public system neglected surgical treatment of other degenerative spine pathologies, causing patients to have to wait for more complex spinal deformity surgeries. This dynamic causes many patients to seek alternative access to spine care in the private sector as patients recognize that private health care providers have a more efficient way to treat patients for cash.
Endoscopic spine surgery is perceived by many of the 120 Chilean spine surgeons as a solution to the higher disease burden associated with musculoskeletal diseases and low back pain in particular by offering a cost-effective alternative to traditional spine surgery without the need for hospitalization, less postoperative pain, complications, and need for analgesia. To the many patients who are overwhelming Chile’s public health system, which is notoriously slow in assessing the value of surgical innovation and implementing new technology advances, private care outside the single-payer system is the only viable alternative.
Conclusions
Chile is a highly developed, industrialized country in Latin America with a disease burden similar to other first world countries, including the United States. The single-payer public health care system is strained even though well-intended treatment guarantees for some 85 chronic conditions have been implemented. The most common painful conditions of the spine are excluded from this guaranteed coverage, prompting an increasing number of patients to seek help in the private sector. Innovation is carried out mainly by private practice spine surgeons who work with established university centers to implement validated innovations supported by peer-reviewed articles.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests This manuscript is not meant for or intended to endorse any products or push any other agenda other than the clinical utilization data associated with the presented research. The authors declare no conflict of interest, and there was no personal circumstance or interest that may be perceived as inappropriately influencing the representation or interpretation of reported research results. This research was not compiled to enrich anyone. It was merely intended to highlight the common problems encountered in community spine care in Chile.
Disclaimer The views expressed in this article represent those of the authors and no other entity or organization. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data Availability Statement The data presented in this study are public record and available at www.healthdata.org.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.