


Abstract
Background Spinal cord tethering and syringomyelia after trauma are well-known pathologies in patients suffering from spinal cord injury (SCI). In symptomatic cases, various surgical options are available, but untethering and expansion duraplasty is the currently preferred treatment strategy. However, patient outcomes are usually limited by rather high rates of surgical revisions. The aim of the present study was to identify risk factors in SCI patients who underwent multiple surgeries for symptomatic spinal cord tethering and syringomyelia.
Methods We retrospectively investigated 25 patients who received at least 2 untethering surgeries of the spinal cord. All patients were treated by untethering and expansion duraplasty and/or clinically followed between 2012 and 2022 at the Swiss Paraplegic Center.
Results A higher location of SCI correlates with a more rapid development of symptomatic spinal cord retethering in need of surgical revision (r = 0.406 and P = 0.044). Interestingly, the extent of spinal cord tethering is lower in those patients who underwent an early surgical intervention (r = 0.462 and P = 0.030), which points toward an increased vulnerability of the spinal cord at higher levels. Ninety-two percent of the patients displayed a potentially chronic inflammatory condition with a mean level of C-reactive protein of 28.4 ± 4.1 mg/L, while the white blood cell count was identified as an independent predictor for surgical interventions in symptomatic cases.
Conclusions Revision surgery in posttraumatic spinal cord tethering and syringomyelia patients is associated with the location of SCI and the extent of spinal cord tethering. It appears that chronic inflammatory conditions might play an important role in promoting spinal cord retethering and thus warrant further investigation.
Clinical Relevance SCI patients with chronic inflammatory conditions and SCI at upper levels should be clinically monitored more carefully as they appear to be more susceptible to progressive forms of posttraumatic spinal cord tethering and syringomyelia.
Level of Evidence 3.
Introduction
Posttraumatic spinal cord tethering and syringomyelia are rare and disabling pathologies in spinal cord injury (SCI) patients1–5 with an overall incidence of approximately 7%.6 In symptomatic and deteriorating cases, a surgical strategy is indicated, typically favoring the approach of spinal untethering and expansion duraplasty.7–9 However, surgical outcome is often frustrating, and complication rates are rather high.10 In particular, revision rates due to retethering in progressive disease account for up to 50%, with surgical reinterventions becoming increasingly demanding and time consuming. At present, the understanding of the pathophysiological mechanisms of progressive posttraumatic spinal cord tethering and syringomyelia is limited. Moreover, strategies to reduce revision rates like expansion duraplasty and/or placement of drainages are unspecific measures that are only partially successful.11
The process of spinal cord tethering is considered a progressive scarring of the meninges due to an inflammatory cascade, frequently triggered by a traumatic event.12 The arachnoiditis and the subsequent tethering of the spinal cord gradually lead to an impairment of pulse pressure waves of the cerebrospinal fluid (CSF), which disturbs central nerve conduction. To some extent, this might additionally alter the vascular resistance of spinal cord vessels.13 As a consequence, intravascular fluid eventually starts to leak from the vascular structures and accumulates within the spinal cord. This phenomenon is known as myelomalacia or “soft cord” and can evolve into syringomyelia as an end point of this process.
Different studies have focused on regenerative capacities and neuroprotective effects of neural precursor cells for SCI patients.14,15 Indeed, improved functional outcome was observed in experimental animal models. These promising results might partially be explained by neuromodulation through differentiated astrocytes (and other regulatory cells) involved in the immune response of the injured central nervous system.16 However, results in clinical trials are less encouraging with conflicting results.17 Nevertheless, as inflammation after trauma appears to play a critical role in SCI patients and in the development of posttraumatic spinal cord tethering and syringomyelia, a chronic inflammatory state could possibly be associated with retethering and thus disease progression. As a consequence, we investigated a cohort of patients suffering from posttraumatic spinal cord tethering and syringomyelia who underwent multiple untethering surgeries. The indication to perform surgery followed the recommendations stated by Bonfield et al11 and was based on both magnetic resonance evaluation and failure to preserve the patient’s function (ie, achieve a stable neurological level). The aim was to identify outcome predictors to select patients at risk for spinal retethering and thus personalize and improve patient care. The hypothesis was that chronic inflammatory conditions might be a risk factor for progressive forms of posttraumatic spinal cord tethering and syringomyelia in need of surgical revisions.
Materials and Methods
Patient Population and Data Collection
In this investigation, we retrospectively included 25 patients (22 men and 3 women) who underwent surgical revisions (spinal untethering and expansion duraplasty) out of a larger cohort of patients with surgical treatment of symptomatic spinal cord retethering and syringomyelia after trauma.9 Only patients with recurrent surgeries (n ≥ 2) were included, while all the other patients with only 1 surgical intervention (n < 2) were excluded from further investigations (n = 42).
All patients were initially treated by untethering and expansion duraplasty and/or clinically followed up between 2012 and 2022 at the Swiss Paraplegic Center. The clinical and imaging data were electronically retrieved by the available patient’s medical and imaging records. The indication to perform surgical interventions in symptomatic spinal cord tethering and syringomyelia followed the recommendations by the consensus panel in 2010.11 All patients have been evaluated by the same criteria that arose from the best available evidence as well as practice preference. Syringoperitoneal shunts were either newly introduced or revised whenever the intraoperative collapse of the syringomyelia (as controlled by ultrasound) was less than 50% of its initial size after concluding the surgical untethering. To estimate potential chronic inflammation, all available C-reactive protein (CRP) and white blood cell (WBC) counts were collected from each patient over the whole follow-up period.
The study was approved by the local ethics committee (Ethikkommission Nordwest- und Zentralschweiz, EKNZ; KEK-2021–00890). The need for written informed consent for further use of patient’s medical records for research purposes was waived by the local ethics committee. All investigations were performed in accordance with the Declaration of Helsinki (as revised in 2013) and thus respect ethical principles for medical research involving human subjects.
Statistical Analysis
Quantitative parameters are expressed as mean ± SE and categorical variables as frequencies or percentages. As test for normal distribution of the data, the Shapiro–Wilk test was used. Pearson’s correlation analysis was applied to identify a relationship between the parameters of interest. Furthermore, step-wise multivariate linear regression models were used to determine independent predictor variables. Due to the explorative nature of this investigation, no prespecified level of significance was selected. Therefore, the level of evidence was graded on a continuous scale as previously recommended,18 and P values were quantified according to their level of evidence. All statistical investigations were conducted using SPSS 28 (SPSS, Chicago, IL, USA).
Results
Of the investigated 25 patients (22 men and 3 women), the mean ages at the time of SCI and at first and second surgical interventions were 27.7 ± 2.3 years, 41.6 ± 2.3 years, and 47.9 ± 2.2 years, respectively. The mean intervals between the SCI and the first surgery and the first and the second surgery were 13.9 ± 2.8 years and 6.3 ± 1.5 years. Almost all included patients had 2 surgical interventions (n = 20, 80%), while 5 patients had 3 or more surgeries (n = 5, 20%). The mean follow-up of patients after the last surgical intervention was 6.3 ± 1.2 years. Most patients had an ASIA Impairment Scale grade of A (n = 18, 72%), and 92% (n = 23) of patients were initially classified as polytrauma at the time of SCI. The majority of the patients displayed a potentially chronic inflammatory condition (n = 23, 92%), while most frequently, a chronic prostatitis or urinary tract infection (n = 23, 92%) and/or pressure ulcers (n = 14, 56%) were present. Some patients (n = 12, 48%) suffered from other chronic inflammatory disorders like dermatological, neoplastic, and/or rheumatological diseases. Finally, patients showed mildly elevated levels of CRP of 28.4 ± 4.1 mg/L with a WBC count of 7.7 ± 0.4 × 109/L over the whole follow-up period. Fourteen of the 25 patients (56%) received either a new syringoperitoneal or a revision of the already implanted shunt system. An overview of the available patient baseline characteristics is given in Table 1. As only 3 of the 25 patients in this cohort were women, a statistical comparison of the demographics between men vs women was not possible.
Patient baseline characteristics.
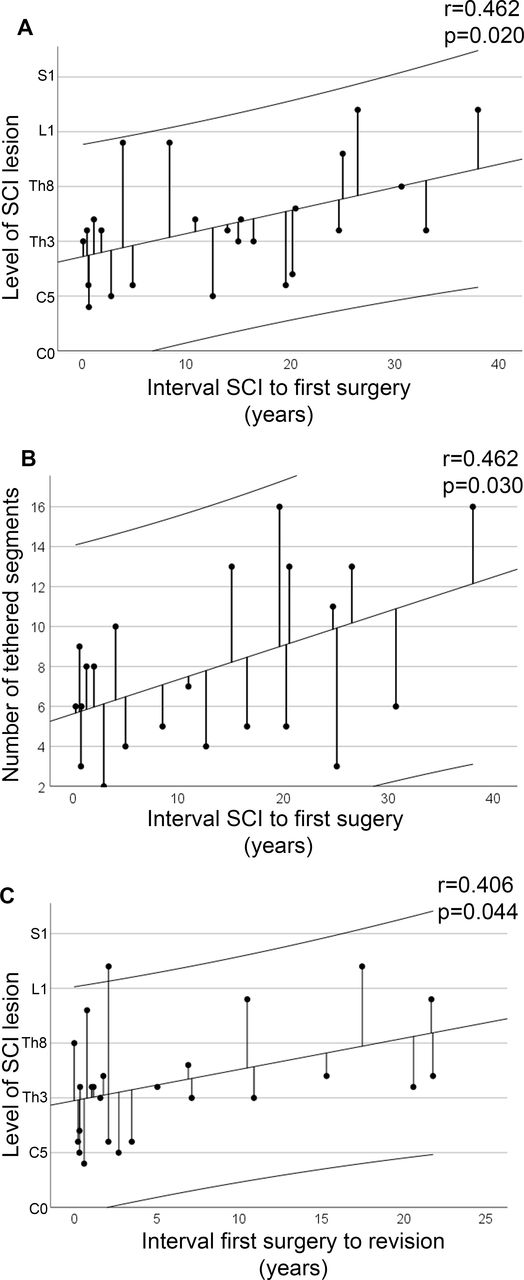
The higher the location of SCI, the more rapid was the development of symptomatic spinal cord tethering in need of surgical intervention (r = 0.462; P = 0.020; Figure A). Interestingly, the extent of spinal cord tethering was less severe in patients who underwent early untethering surgery (r = 0.462; P = 0.030; Figure B), pointing toward an increased vulnerability of the spinal cord at upper levels for the development of symptomatic spinal cord tethering and syringomyelia. In accordance with these findings, the level of SCI positively correlated with the interval between the first surgical intervention and revision surgery (r = 0.406; P = 0.044; Figure C). Therefore, SCI lesions at higher levels appear to be more prone to develop symptomatic spinal cord tethering in need of surgical intervention and might be a risk factor for surgical revisions. Subgroup analysis by various anatomic groups (cervical, C0–C7; cervicothoracic, C6–Th2; thoracic, Th1–Th12; thoracolumbar, Th10–L2; lumbar, L1–L5) did not allow any statistically robust conclusions due to lack of both sample and effect sizes.

Rate of development of symptomatic spinal cord tethering and syringomyelia in patients with surgical revisions. The interval between spinal cord injury (SCI) and the first surgical intervention correlated with the location of the SCI lesion (panel A; P = 0.020) and with the extent of spinal cord tethering (panel B; P = 0.030). Furthermore, the velocity of development of spinal cord retethering was correlated to the segmental height of the SCI lesion (panel C; P = 0.044). The 95% confidence interval of the linear line fitting including the SE of regression is given for panels A–C. Regarding the location of SCI lesion, the vertebral segments are displayed in anatomical order from C0 to S1, while the displayed locations refer to the middle of the respective SCI lesion.
In the first stepwise multivariate linear regression model adjusted for risk factors that potentially promote arachnoiditis, including age, the extent of spinal cord tethering/syringomyelia, and location of SCI, both age (B-coefficient 0.478 and P = 0.013) and extent of spinal cord tethering/syringomyelia (B-coefficient 0.396 and P = 0.034) were independent predictors for the rate of development of a symptomatic tethered cord and syringomyelia (Table 2, Model 1). In the second stepwise multivariate linear regression model including age, location of SCI, CRP, and WBC, both location of SCI (B-coefficient 0.621 and P = 0.002) and WBC (B-coefficient 0.357 and P = 0.048) were selected as independent predictors for the rate of development of a symptomatic tethered cord and syringomyelia (Table 2, Model 2). In the final stepwise multivariate linear regression model, which included age, type of duraplasty, and location of SCI as risk factors for developing retethering, the location of SCI was selected as an independent predictor (B-coefficient 0.406 and P = 0.044; Table 3).
Stepwise linear regression models for the development of symptomatic spinal cord tethering and syringomyelia after trauma in need for surgical intervention (n = 25).
Stepwise linear regression model for the development of symptomatic spinal cord retethering and syringomyelia after trauma in need for surgical revision (n = 25).
Discussion
Surgical revisions due to retethering in SCI patients with symptomatic spinal cord tethering and syringomyelia are a great challenge in the treatment of this disabling pathology. It appears that patients with SCI lesions located in the upper spinal cord are more susceptible in developing symptomatic spinal cord tethering and syringomyelia in need for surgery. Interestingly, minor or circumscribed adhesions situated at higher levels of the spinal cord are already sufficient to deteriorate the patients’ condition. In particular, the location of SCI has been identified as an independent predictor for surgical revisions. Moreover, it seems that almost all patients in this study most likely displayed a chronic inflammatory condition with high rates of chronic prostatitis and/or urinary tract infections and pressure ulcers. Therefore, low-grade inflammatory processes might promote arachnoiditis and spinal cord scaring and impose a potential risk factor for surgical revisions. This is additionally supported by the selection of WBC count as an independent predictor for the velocity of development of spinal tethering in need for surgery. Consequently, chronic inflammatory conditions may be perceived as a trigger for the high revision and retethering rates in patients with posttraumatic spinal cord tethering and syringomyelia.
There are several challenges regarding the treatment of posttraumatic spinal cord tethering and syringomyelia. First, the selection of patients who should be treated surgically is demanding. A consensus panel by Bonfield et al11 proposed to treat patients who demonstrate a motor deterioration with surgery, while there is evidence against surgery in patients suffering solely from sensory loss, neuropathic pain, and/or asymptomatic but expanding syringomyelia. Second, once the indication for a surgical intervention is given, disagreement exists concerning the most suitable surgical technique. Nevertheless, a weak recommendation exists toward untethering and expansion duraplasty for the treatment of spinal cord tethering and syringomyelia with the aim to diminish the rate of retethering.7,8,11 Finally, the surgical outcome, and consequently the benefit of surgery, is intensively debated.10 In particular, the high retethering and complication rates of up to 50% or more are a great challenge following surgical treatment. However, in SCI patients with progressive neurological loss endangering activities of daily life and thus failure of conservative measures, the evaluation of a surgical strategy as the last line option to improve the patient’s condition is usually justified. Unfortunately, any kind of conservative or surgical measures are presently perceived to be palliative with the aim to stop or slow down a progressive arachnoiditis resulting from a probable autoinflammatory disease of the meninges.12 As a consequence of usually frustrating clinical outcomes, independent of the applied therapeutic measures, the validity of a surgical strategy is seen critically. Nevertheless, by performing a spinal cord untethering and expansion duraplasty, neurological deterioration can frequently be arrested in approximately 80% of cases, while in at least 50% of cases, a functional improvement has been documented.1,5,8,9,19
Chronic inflammatory processes or conditions are generally acknowledged to negatively impact various body functions, thus rendering the human organism prone for adverse reactions like autoimmune responses.20 Considering that SCI is usually accompanied by polytrauma, the body is entering a state of systemic inflammatory reaction (systemic inflammatory response syndrome [SIRS]).21 Heterogeneous biomechanical forces on the spinal cord resulting from traumatic fractures and/or dislocations in SCI patients lead to damage of the cord and the meninges, thus resulting in subarachnoid inflammation (arachnoiditis).12 Indeed, inflammatory cytokines like tumor necrosis factor α, interleukin 1β, and interleukin 6 reach abnormal levels for several days after SCI22,23 before returning to baseline levels. Moreover, the systemic inflammatory response appears to be more robust if SCI is located in the upper part of the spinal cord. This is supported by the fact that the hepatocellular damage as a secondary effect of SCI at higher levels is more intense.24 Considering that not all patients develop symptomatic spinal cord tethering and syringomyelia after traumatic SCI, either arachnoiditis is cleared before significant scarring occurs or the trauma severity inducing parenchymal alterations is rather mild. However, in SCI patients with more severe degrees of trauma, the development of symptomatic spinal cord tethering and syringomyelia might be more likely due to extensive SIRS for several days or weeks. This goes along with the finding that younger patients with SCI in the upper part of the spinal cord and thus usually higher trauma severity appear to develop symptomatic spinal cord tethering and syringomyelia in need of surgical intervention more rapidly.9 Thus, the formation of fibrous scarring within the spinal cord parenchyma and thus disturbance of nerve conduction and CSF flow seems to be related to trauma severity, location of SCI, and the consecutive inflammatory response. Indeed, proliferating meningeal cells are able to enter the spinal cord parenchyma following SCI.25,26
Unfortunately, no long-term investigations of parenchymal tissue surrounding the spinal cord after trauma are available so far. Thus, it must be hypothesized that in those SCI patients developing symptomatic spinal cord tethering and syringomyelia several years or even decades after SCI, a low-grade or potentially chronic (probably autoimmune) inflammatory process of the arachnoid tissue has to persist. To some extent, this might lead to a clinically relevant impairment of CSF flow and/or nerve conduction with the development of symptomatic spinal cord tethering. Interestingly, this fits with the findings in our study in which the WBC count was an independent predictor for the velocity of development of symptomatic spinal cord tethering and syringomyelia in need for surgery. Moreover, a high rate of most likely chronic inflammatory pathologies of 92% in those SCI patients undergoing surgical revisions for retethering additionally supports our findings. Furthermore, in our patient cohort, the mean levels of CRP as an acute phase response protein are slightly elevated, which underlines the hypothesis that a low-grade or chronic inflammatory process might be predictive concerning surgical outcome in patients with retethering. Although only the location of SCI has been identified as an independent predictor for retethering cases in need of surgical revision, our data show that the rate of development of symptomatic spinal cord tethering and syringomyelia in need of surgery is faster in those patients with traumatic lesions in the upper part of the spinal cord. Conclusively, as trauma severity is usually more severe in upper parts of the spinal cord and inflammatory parameters might play an important role in the development of posttraumatic spinal cord tethering and syringomyelia, a major SIRS and thus a persistent chronic inflammatory reaction could be a plausible explanation in progressive spinal cord tethering cases with surgical revisions.
Limitations
As with any study, we acknowledge that the present study has some limitations. This is a retrospective and single-center cohort trial of a rare pathology with a low number of patients and no control group. This limitation was due to the fact that the available data were limited, and no standardized comparison between patients with 1 surgical intervention (excluded from this investigation) to those with multiple surgeries was feasible. As a consequence, the statistical power of this investigation is limited. In our opinion, larger investigations should be performed with additional measurement of more sensitive and representative inflammatory parameters such as blood sedimentation rate, high-sensitivity CRP, and/or procalcitonin of affected patients.
In addition, the shown relationships between “level of SCI lesion” and “number of tethered segments” to “interval between SCI to first surgery” or “interval between first surgery to revision” have to be regarded critically. Statistically, a relationship is present when a change of 1 variable leads to an increase or decrease of the other variable. To understand the strength of this relationship, the r-value plays an important role. While a positive/negative r-value of 1 means a perfect positive/negative linear correlation, a positive/negative r-value of 0.8 ≤ 1, 0.4 ≤ 0.8, and 0 ≤ 0.4 refer to a strong, moderate, or weak positive/negative linear correlation, respectively. Our data showed only a moderate positive linear correlation with r-values between 0.4 and 0.8, and thus, the suggested relationships should be perceived with caution.
Furthermore, as expansion duraplasty, both synthetic (expanded polytetrafluoroethylene [Gore-Tex] or polyesterurethane [Neuro-Patch]) and organic (bovine pericardium [Dura-Guard]) products were applied. Although various studies state high biocompatibility for all of these products,27–30 and our multivariate regression model excluded the different types of patches as independent predictors for surgical revisions, we cannot completely exclude retethering due to a potential adverse immune reaction against the patch material. In particular, inflammatory events and adverse reactions such as ossification have been associated with the use of Gore-Tex as dural substitutes.31,32 To avoid local inflammatory response against synthetic or xenograft patch material, autologous tissue (ie, patient’s harvested fascia lata or pericranium) should still be considered as a safe and well-established alternative for expansion duroplasty.33
Additionally, the size of the syrinx could not be reliably estimated due to limited imaging data with regard to standardized measurements. Also, the conduction of surgical techniques might vary among the cases as different surgeon teams were involved in the treatment of the reported patients. Thus, this explorative and noncontrolled investigation has to be considered as concept generating with the aim of laying the basis for further prospectively designed investigations with appropriate size and control groups to confirm our findings. Thus, our results cannot be generalized to the whole population of SCI patients suffering from spinal cord tethering and syringomyelia. Finally, it is also clear that the value of the retrospectively available parameters is limited, and multivariate analysis integrating all potential confounders was not feasible.
Conclusions
Revision surgery in posttraumatic spinal cord tethering and syringomyelia patients is associated with the location of SCI and the extent of spinal cord tethering. In particular, in SCI patients with lesions located in the upper spinal cord, the development of symptomatic spinal cord tethering and syringomyelia in need for surgery is more rapid, with an increased susceptibility for retethering and thus surgical revisions. It further seems that chronic or low-grade inflammatory conditions might play an important role in promoting spinal cord tethering and, thus, inflammatory pathways, in particular within the spinal cord, need to be further investigated. Conclusively, SCI patients with chronic inflammatory conditions and SCI at upper levels should be clinically monitored more carefully as they might possess the tendency to develop progressive forms of posttraumatic spinal cord tethering and syringomyelia with an increased risk for symptomatic retethering in need of surgical revisions.
Acknowledgments
We thank the medical staff of rehabilitation and radiology for being involved in routine patient care of the investigated SCI patients and as such in the generation of the necessary clinical data included in this investigation. Furthermore, we thank Dr. Raoul Heilbronner, former senior neurosurgeon at the Swiss Paraplegic Center, for being involved in both conservative and operative care of the included patients. There was no specific funding concerning this study; however, we are grateful to the Swiss Paraplegic Center, the Swiss Paraplegic Research, and the Swiss Paraplegic Foundation for their support.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval The study was approved by the local ethics committee (Ethikkommission Nordwest- und Zentralschweiz, EKNZ; KEK-2021-00890). The need for written informed consent for further use of patient's medical records for research purposes was waived by the local ethics committee. All investigations were performed in accordance with the declaration of Helsinki (as revised in 2013) and thus respect ethical principles for medical research involving human subjects.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.