


Abstract
Background Low back pain (LBP) is 1 of the most common problems that present in 80% of people. LBP can be caused by some pathologies, with discogenic pain being 1 source. Pain from LBP can become chronic and also cause disability. Treatment options for LBP varied from conservative to operative, and a novel treatment nowadays is using stem cells therapy to treat with pain from LBP.
Methods Database searches from Pubmed and ScienceDirect from inception to 13 September 2023. A total of 283 discogenic LBP cases from 8 articles. This study measured clinical outcomes using a visual analog scale (VAS) and Oswestry Disability Index (ODI) obtained from each study.
Results Functional outcomes in patients treated with stem cell therapy showed significant improvement ODI and VAS (P < 0.00001). Improvement also showed in Pfirrmann grade before and after treatment with stem cells (P = 0.005). Subgroup analyses using bone marrow aspirate concentrate also showed significant differences in both ODI and VAS (P < 0.00001).
Conclusion Stem cells therapy could be beneficial as an option of treatment for discogenic LBP in improving pain and activity of daily living.
Clinical Relevance Intradiscal stem cell therapy is a promising alternative for managing discogenic low back pain, offering improvements in pain and function.
Level of Evidence 4.
Introduction
Low back pain (LBP) is the most common musculoskeletal symptom caused by degenerative joint disease in the lumbar spine.1 LBP is defined as pain and discomfort between the costal margin and inferior gluteal fold with or without leg pain. An estimated 80% of the normal population will experience LBP in their lifetime, and this has enormous socioeconomic consequences.2 One of the conditions leading to degenerative joint disease in the lumbar spine is degenerative disc disease, in which this condition will lead to herniation of the intervertebral disc (IVD).1
Discogenic pain is a common source of LBP, with an overall prevalence of 26% to 42%. In younger populations, this increases to over 80%. Discogenic LBP is typically persistent with chronic pain and disability, and most treatment resources are directed toward refractory pain symptoms.3 The pathophysiology of discogenic back pain involves an imbalance in the anabolic and catabolic environments of the extracellular matrix in favor of catabolism. The resultant alteration in disc height affects the biomechanics of the involved spinal segment, which often results in segmental instability.4
It is estimated that the annual worldwide LBP incidence in adults is 15%, and the point prevalence is 30%.5 In 2020, LBP affected 619 million (95% uncertainty interval 554–694) people globally, with a projection of 843 million (759–933) prevalent cases by 2050.6 The high rate of LBP prevalence observed in all regions globally could have some important social and economic consequences, especially considering the substantial cost of care for this condition. For instance, from 2012 to 2014, the direct aggregate costs for all individuals with a spine condition in the USA were US$315 billion, with a substantial proportion of costs attributed to surgical procedures.6
Makkiyah et al said that the prevalence of LBP in middle-aged adults in Indonesia was 44.29% at 12 months.7 The Ministry of Health of the Republic of Indonesia stated that the number of LBP incidents in Indonesia in 2018 was 18%. Based on Indonesia’s 2017 national and subnational disease burden analysis data, LBP complaints were the main cause of loss of productive years due to disability due to illness and injury in Jakarta in 2017.8
Treatment modalities in the management of chronic lumbosacral pain include conservative management with physical therapy, pharmacological therapy, interventional and intradiscal, as well as surgical intervention through fusion or disc replacement.9 At present, nonsurgical treatment based on physiotherapy and pharmacological interventions remains the first-line treatment option for lumbar discogenic pain.10
In recent years, there has been an increasing shift toward regenerative therapies for several pathologies across the entire spectrum of medicine.11 Among the biological disc repair therapies, cell therapy has gained interest as it offers a disc regenerative potential while being minimally invasive.12 A cell therapy approach aims to address disc inflammation by inhibiting aberrant cytokine production and to promote disc rehydration and height restoration by initiating matrix anabolism, as well as repopulating and stimulating the native cells.12 As a result of these efforts, number of different regenerative modalities are being considered as treatment options for LBP due to DDD; these include platelet-rich plasma, stem cells, and bone marrow concentrate (BMC). Among these options, stem cell and BMC have shown promising results in the treatment of discogenic LBP.11
Based on all this, we conduct a systematic review of current literature on the role of stem cell therapy treatment for patients with discogenic LBP aiming to evaluate clinical improvement on LBP treated with stem cell therapy.
Methods
Search Strategy and Study Selection
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines.13 A comprehensive search across 2 databases (PubMed and ScienceDirect) from inception to 13 September 2023. The search terms used were “stem cell therapy” AND “discogenic LBP” (Figure 1). The inclusion criteria were (1) patients with discogenic LBP treated with stem cells therapy, (2) a study presents the effectiveness of intradiscal stem cell therapy, and (3) in English. Exclusion criteria were (1) patients had history of spinal fusion, (2) case report and review, and (3) incomplete data.

Preferred Reporting Items for Systematic Reviews and Meta-Analysis flowchart.
Eligibility Criteria and Quality Appraisal
The included studies were of any design reporting on the usage of stem cells for the treatment of discogenic LBP. The inclusion criteria used in this study were (1) published in English, (2) concerned discogenic LBP, and (3) patients had no history of prior surgery at the affected lower back. The exclusion criteria used in this study were (1) review articles, (2) animal studies, and (3) articles unavailable in English. Study quality was assessed with the Cochrane risk of bias tool for randomized controlled trials (RCTs) and the methodological index for non-randomized studies score for non-RCTs (Figure 2, Table 1).14 Each included study stated that there was no source of funding for their research.

Risk of bias of included randomized controlled trials.
Methodological index for non-randomized studies score.
Data Extraction
Three independent reviewers (R., K.Y., and A.G.) selected the articles included in the study through title and abstract screening and conducting full-text reviews of the selected articles. Any disagreements were resolved by a fourth, independent reviewer (N.P.H.). Initially, in the literature searching and cross-referencing, 86 articles were found, 19 articles were excluded before sceening because of duplication. After titles and abstracts were screened, 11 articles met the eligibility criteria. After a full-text review, 3 articles were excluded (prestudy protocol and nonusable data), and 8 articles were included in the systematic review.
Statistical Analyses
Mean difference and 95% confidence intervals were calculated using the inverse variance method, and study heterogeneity was assessed using I 2 with a value of >50% marked as significant heterogeneity. If the I 2 > 50%, subgroup analysis was carried out. Statistical significance was defined with a P value of <0.05. Statistical analyses were performed by Review Manager 5.4 analysis software.
Results
Patient Characteristics and Demographics
A total of 86 articles were identified, with 8 studies meeting the inclusion criteria after screening. Details of the studied, such as the number of patients, gender, study design, outcomes, and follow-up period, are presented in Table 2. Seven studies including a total of 283 patients were used in statistical analysis. One study was not included in statistical analysis because the results in the study were grouped. Patients’ ages ranged from 35 to 60 years. The follow-up period after stem cell therapy ranged from 12 to 36 months.
Characteristics of included studies.
Outcome Measurement and Results
The improvement in the Oswestry Disability Index (ODI) in 7 studies resulted in a significant difference (P < 0.00001) in patients treated with stem cell therapy. Subgroup analysis based on follow-up periods revealed significant reductions in ODI observed across all time points; however, heterogeneity was high (I 2 = 94%; Table 3; Figure 3).

Oswestry Disability Index forest plot.
Statistical analysis results.
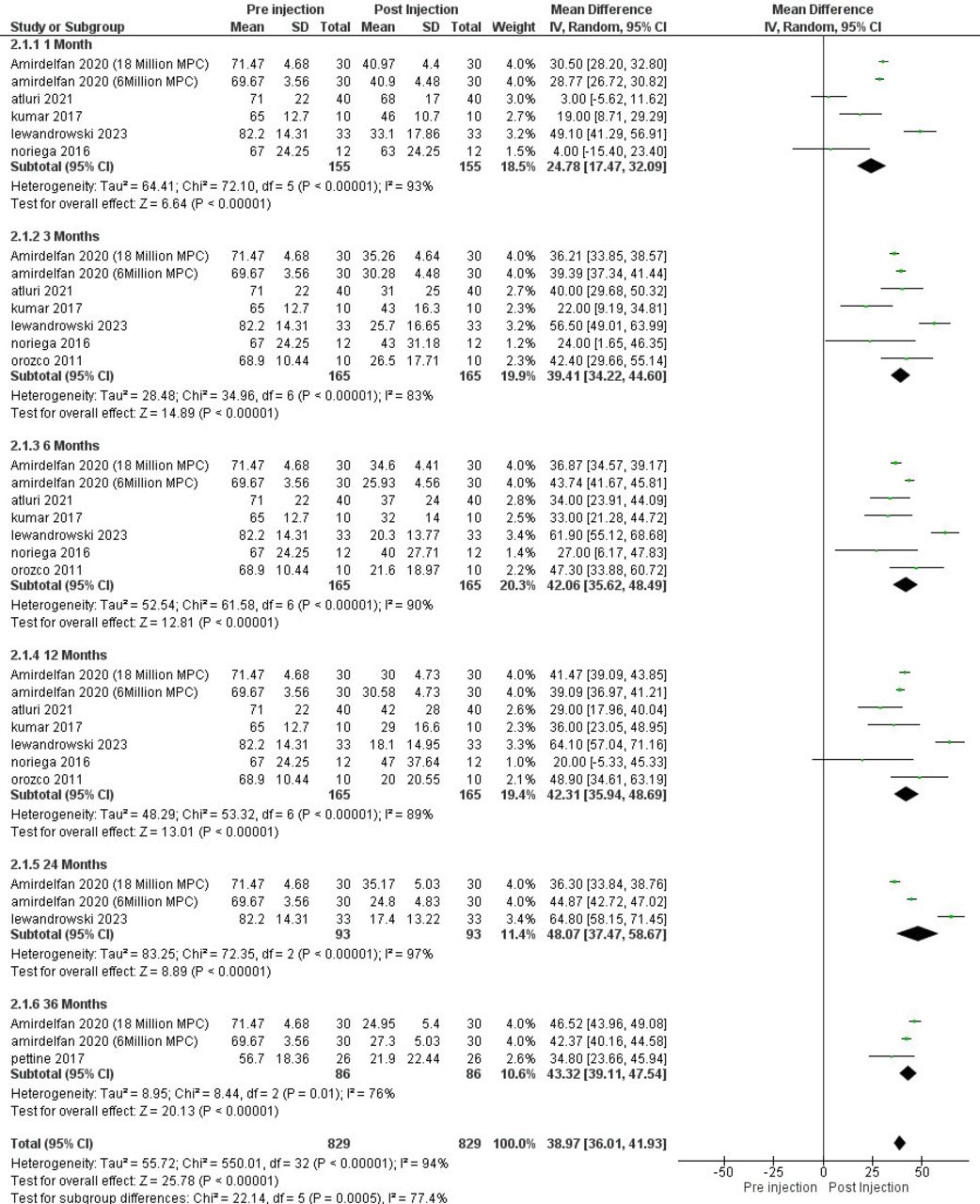
Pain scale using a visual analog scale (VAS) or numeric rating scale in 7 studies before and after treatment using stem cells therapy resulted in significant difference (P < 000001). Subgroup analysis by follow-up period similarly indicated consistent improvement across time points, though heterogeneity remained high (I 2 = 94%; Table 3; Figure 4).

Visual analog scale forest plot.
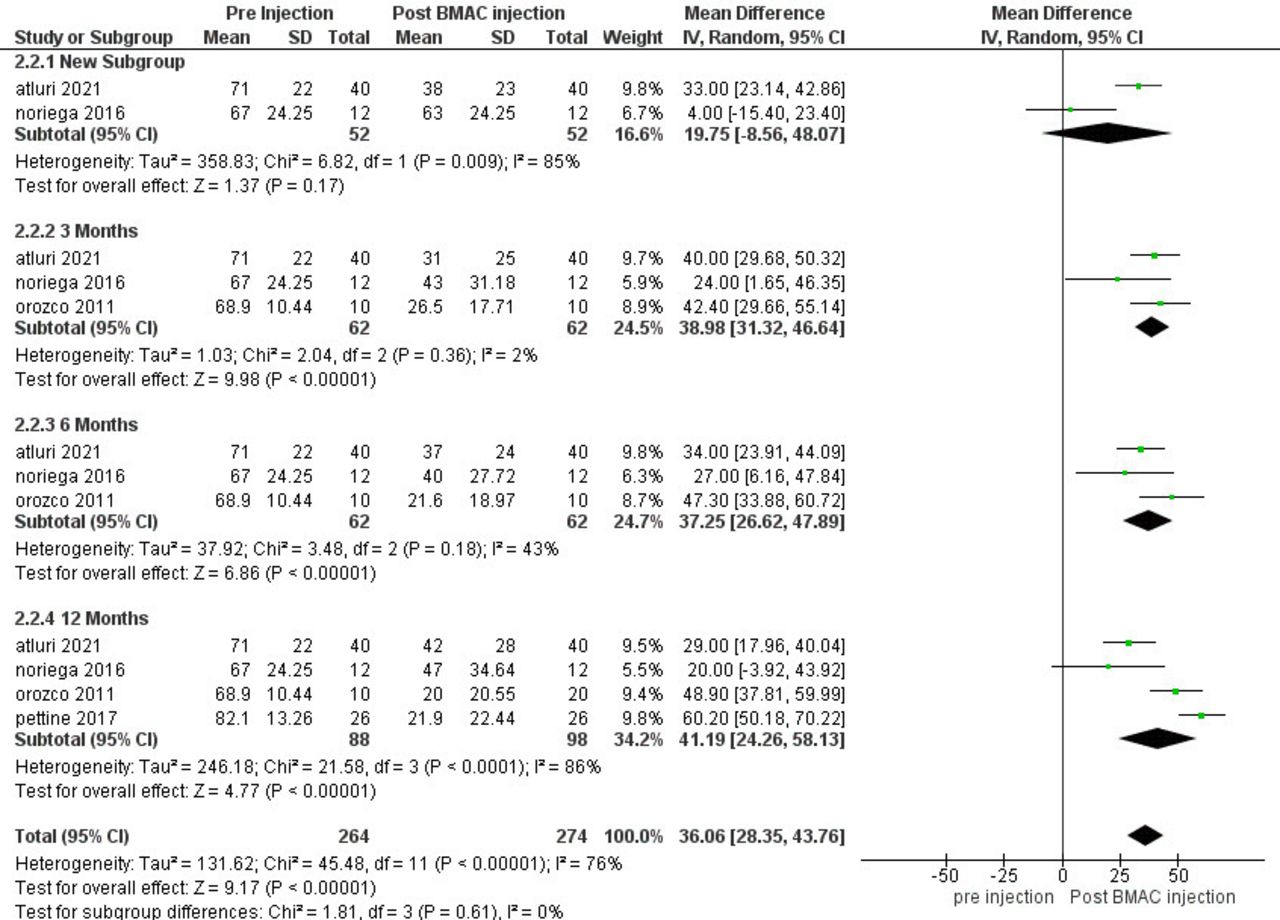
A subgroup analysis of ODI and VAS outcomes in studies using bone marrow aspirate concentrate was conducted across 4 studies. ODI improvement was significant across follow-up periods of 1, 3, 6, and 12 months, with moderate heterogeneity (I 2 = 58%; Table 3; Figure 5). For VAS, it was significantly different in follow-up periods 3, 6, and 12 months. In 1-month follow-up, it included 2 studies but was insignificant (P = 0.17), and the pooled heterogeneity was moderate (I 2 = 76%; Table 3; Figure 6).

Oswestry Disability Index improvement with bone marrow aspirate concentrate.

Visual analog scale improvement with bone marrow aspirate concentrate.
Magnetic resonance imaging assessments using Pfirrmann grading scale were available in 5 studies. Two studies included in the meta-analysis showed statistically significant improvement in Pfirrmann grade (P = 0.005) with low heterogeneity (I 2 = 0%; Table 3; Figure 7). Other studies showed varied results. In the study by Pettine et al, 8 of 20 patients showed improved Pfirrmann grade. In the study by Noriega et al,21 the control group had worsened Pfirrmann grade at the end of the follow-up. Although limited, these results suggest the potential of stem cell therapy to influence disc morphology, warranting further investigation with larger samples.

Pfirmann improvement.
Discussion
Regenerative treatments using stem cell therapy sourced from the human body are gaining popularity across medical fields. In orthopedics, it offers a promising alternative for patients with degenerative conditions who opt to avoid surgery. This therapy aims to stimulate the body’s natural regenerative mechanisms, especially in the IVDs, potentially alleviating pain in patients affected by degenerative disc disease over time.
Regenerative medicine therapies have shown potential for sustained relief and, in certain cases, may provide curative outcomes. In recent years, allogeneic stem cell transplantation has gained increasing interest as an alternative to autologous BMC transplantation.15 Another source of mesenchymal stem cells (MSCs) is BMC, which can be derived from either autologous or allogeneic bone marrow aspirate. BMC can be harvested from the posterior superior iliac spine of the patient16–18 or obtained from an allogeneic donor and subsequently processed following good manufacturing practice standards.21
Multiple studies3,4,9–11,23–25 investigating the potential of MSC therapy for degenerative disc disease have consistently concluded that MSCs may offer a promising treatment approach for this condition. Although the precise mechanisms by which MSCs can alleviate disc degeneration remain unclear, evidence suggests that intradiscal injection of MSCs could serve as a potential treatment option for patients with chronic LBP. MSCs are considered strong candidates for regenerating IVDs, as they aim to replenish disc tissue and rejuvenate its functionality by promoting matrix synthesis through the implanted cells. Furthermore, MSCs may exert positive effects on the surrounding native cells.26 Animal studies have shown that MSCs injected into the nucleus pulposus not only survive but also proliferate, potentially leading to improvements in the condition of degenerated discs.4
This systematic review and meta-analysis evaluated the effects of stem cell therapy on VAS, ODI, and disc morphology (Pfirrmann grade) in patients with discogenic LBP. Across studies, stem cell therapy showed statistically significant improvement in VAS/Numeric Rating Scale, ODI, and Pfirrmann improvement, suggesting substantial benefits for pain relief and functional outcomes in patients with discogenic LBP. High heterogeneity in overall analyses indicates variability in study outcomes, likely due to differences in intervention types, follow-up periods, and patient populations. Subgroup analyses by follow-up period and intervention type (bone marrow aspirate concentrate) reduced heterogeneity to some extent, suggesting the effects of stem cell therapy on disability may be durable over time.
The magnetic resonance imaging findings, although limited in scope, provide preliminary evidence that stem cell therapy may positively affect disc degeneration, as indicated by changes in Pfirrmann grade. However, varied results across studies underscore the need for standardization in imaging protocols and extended follow-up to ascertain the true impact on disc morphology. These findings, while promising, are derived from a small subset of studies, highlighting the need for more robust evidence with larger, standardized sample sizes.
Wu et al,24 Zhang et al,10 and Yolcu et al11 reported improvements in discogenic LBP after stem cell therapy. Yolcu et al observed improvement at 3 months, 6 months, and 12 months, although the quantitative gains were slightly lower at the 12-month follow-up. In contrast, Wu et al and Zhang et al compared only the baseline data with final follow-up outcomes.
The observed outcomes may be linked to the introduction of anabolic growth factors and stem cells into the degenerated IVD, effectively counteracting its catabolic environment. Increased levels of growth factors and cytokines have been shown to enhance cellular proliferation of both annulus fibrosus and nucleus pulposus cells, enhance glycosaminoglycan content, stimulate collagen synthesis, and upregulate gene expression related to extracellular matrix proteins that are essential for IVD function. This synergistic effect likely plays a significant role in improving the overall condition of the disc.16
Sanapati et al9 also stated in their study that regenerative therapies, including MSCs, may be effective in treating discogenic LBP, with the potential to decelerate or even halt the degenerative process of the IVD. However, they also suggested that the effectiveness of MSC injections could be improved by combining them with growth factors present in platelet-rich plasma.
Although no adverse events were reported following MSC injections, Meisel et al12 emphasized that evidence regarding the efficacy and safety of cell therapy remains limited due to potential biases and small sample sizes. Similarly, Schneider et al3 found that the quality of evidence for the effectiveness of intradiscal biological treatments was very low. This finding highlights the need for further research, particularly focusing on the efficacy and safety of MSC injections.
The authors acknowledge the limitations of this study. Variations in stem cell dose and cell types may influence the findings. Diverse reporting tools and follow-up times posed challenges in harmonizing results, and the small sample sizes in some studies may have contributed to bias. Different standards for patient selection across studies may potentially lead to a good outcome bias. Studies included in this review clearly stated no direct funding for their research, but several authors were affiliated with companies that manufactured the device used for their interventions, which may introduce a potential motivational bias. Future studies could benefit from more disclosure on author affiliations and potential conflicts of interest to further enhance objectivity.
Further research is necessary to compare the outcomes of stem cell therapy with standard treatments in long-term follow-up studies. Additionally, the optimal dose and variations in stem cell types required further investigation, as did establishing consistent patient selection criteria to ensure more accurate assessments of treatment efficacy.
Conclusion
Stem cells therapy could be beneficial as an option for the treatment for discogenic LBP in improving pain and activity of daily living. Future prospective studies with control subjects as a comparison of the effectiveness are strongly recommended to be conducted to verify this finding and also explore more effects regarding the use of stem cells.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.