


Abstract
Background This study presents a single surgeon’s experience comparing 1-year outcomes of endoscopic transforaminal lumbar interbody fusion (E-TLIF) vs minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) in an Asian population.
Methods Retrospective review of consecutive patients who underwent single-level E-TLIF or MIS-TLIF by a single surgeon in a tertiary spine institution from 2018 to 2021 with 1-year follow-up. Inclusion criteria for both procedures were degenerative disc disease with grade I or II spondylolisthesis and mild to moderate central canal stenosis. Clinical outcomes assessed included surgery duration, blood loss, and length of stay. Patient-reported outcomes assessed included the visual analog score for back pain and lower limb pain, Oswestry Disability Index, and North American Spine Society Neurogenic Symptom Score. Radiographic parameters assessed included segmental lordosis, posterior disc height, listhesis, and the presence of cage migration or subsidence.
Results Twelve E-TLIF and 34 MIS-TLIF patients were identified. E-TLIF had shorter surgery duration (165 ± 15 vs 259 ± 43 min for E-TLIF and MIS-TLIF groups, respectively; P < 0.001), reduced blood loss (83 ± 75 vs 181 ± 225 mL; P = 0.033), and decreased length of stay (1.8 ± 0.9 vs 4.7 ± 2.9 days; P < 0.001) compared with MIS-TLIF. E-TLIF and MIS-TLIF patients had significant improvements (P < 0.05) at 1 year in all patient-reported outcomes scores and radiographic parameters assessed. Both E-TLIF and MIS-TLIF patient groups also had similar postoperative patient-reported outcomes scores and radiographic parameters. No complications were recorded for E-TLIF, while MIS-TLIF had a case of dura tear and another case of meralgia paresthetica. There were no instances of cage subsidence, cage migration, or implant loosening in either group at 1 year.
Conclusions Although the study size was limited because E-TLIF is a relatively new technique in our institution, 1-year results demonstrate that E-TLIF can be a safe and efficacious option that achieves clinical and radiological results similar to MIS-TLIF with the additional benefits of decreased surgical duration, blood loss, and length of hospital stay.
Clinical Relevance The results of this study support the effectiveness and potential advantages of endoscopic TLIF compared with MIS-TLIF.
Level of Evidence 3
- Endoscopic transforaminal lumbar interbody fusion
- minimally invasive transforaminal lumbar interbody fusion
- lumbar degenerative disc disease
- spinal stenosis
Introduction
Endoscopic spine surgery has seen significant advancements over the past few decades with technological improvements in optics and the design of surgical instruments. Endoscopic transforaminal lumbar interbody fusion (E-TLIF) represents the latest generation of endoscopic spine surgery, and early results are promising.1 E-TLIF can be performed via the transforaminal approach or the posterior-lateral approach using either a uniportal or a biportal technique.2 In this study, E-TLIF was performed via a uniportal transforaminal approach under general anesthesia and neuromonitoring. E-TLIF involves a smaller skin incision and decreased soft tissue disruption compared with conventional minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF).3 Unlike MIS-TLIF, E-TLIF largely depends on indirect decompression, which can be facilitated through the use of expandable cage technology. There is limited literature evaluating E-TLIF in Asians with a smaller surface area for interbody fusion. This study presents a single surgeon’s experience comparing 1-year outcomes of E-TLIF vs MIS-TLIF in an Asian population.
Methods
Patient Population
A retrospective review was conducted on all consecutive patients who underwent single-level E-TLIF or MIS-TLIF by a single surgeon in a tertiary spine institution from 2018 to 2021 with at least 1-year follow-up. This study was reviewed and approved by our institution’s ethics committee. Inclusion criteria for both procedures were patients who experience persistent neurological symptoms or intermittent claudication and do not respond to appropriate conservative treatment with concordant imaging evidence of single-level mild to moderate spinal stenosis or degenerative disc disease with grade I or II spondylolisthesis. Exclusion criteria were severe spinal stenosis causing cauda equina syndrome or footdrop, trauma, infection, high-grade spondylolisthesis, and previous lumbar spine surgical treatment or radiofrequency ablation. The choice of technique was dependent on the availability of endoscopic technology in later years, surgeon, and patient preference.
Surgical Technique
Both E-TLIF and MIS-TLIF techniques were done under general anesthesia and neuromonitoring. Patients were positioned prone on a Jackson table.
MIS-TLIF was performed through a paramedian Wiltse plane approach and the use of tubular retractors to expose the posterior elements. This is followed by facetectomy, discectomy, interbody cage insertion, packing of the bone graft, laminectomy, and finally nerve root decompression to ensure that all affected neural elements at that level are thoroughly decompressed.
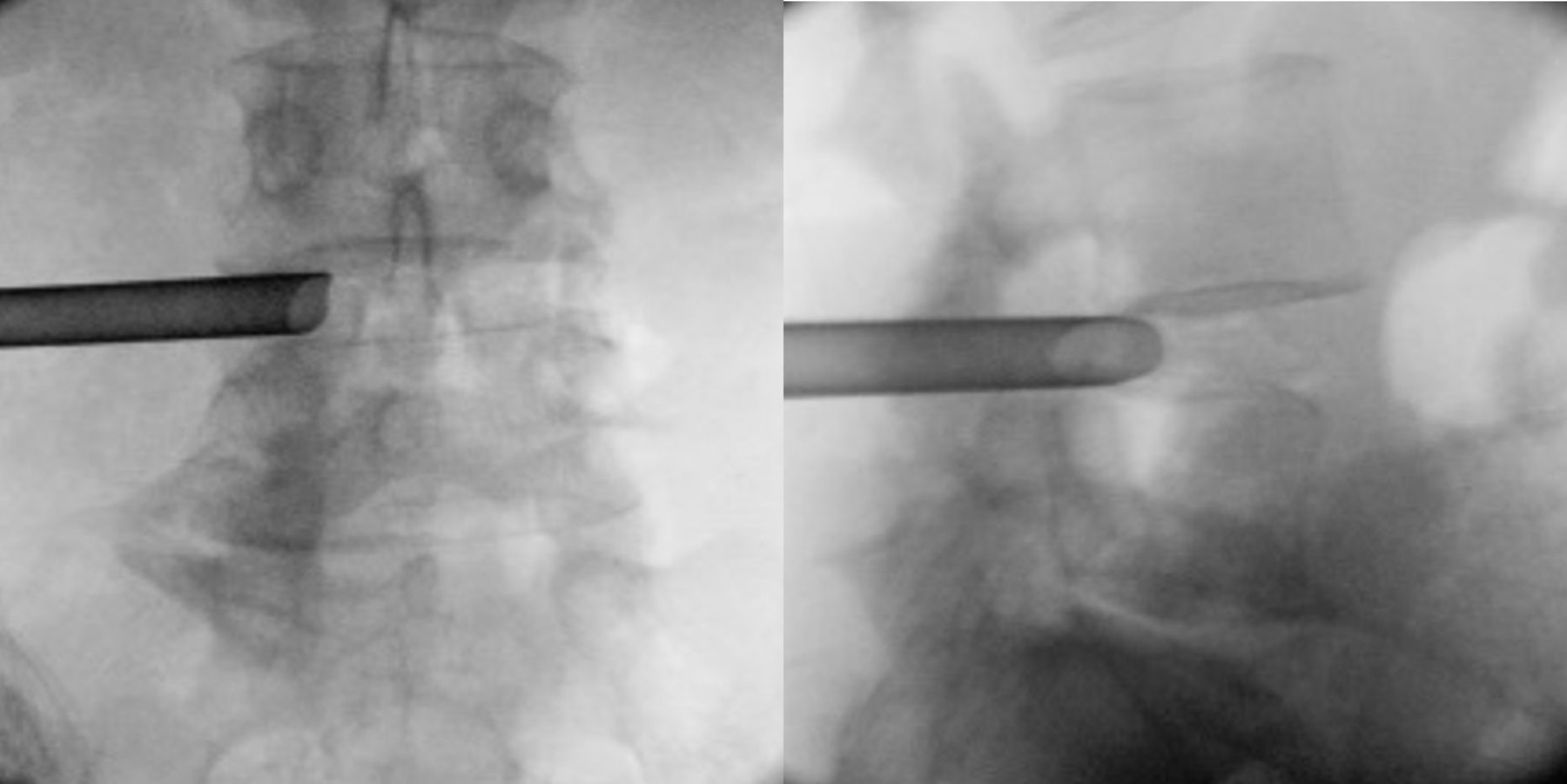
In E-TLIF, a small skin incision is made about 8 to 13 cm from the midline with the aid of fluoroscopic localization. The disc space is initially accessed through Kambin’s triangle with an 18G spinal needle. A Nitinol wire is inserted through the spinal needle (Figure 1), which is used to guide a series of dilators into the disc space, followed by a 7-mm working cannula (Figure 2).

Nitinol wire inserted through 18G spinal needle into the disc space after fluoroscopic confirmation of correct positioning.

Working cannula inserted after sequential dilation.
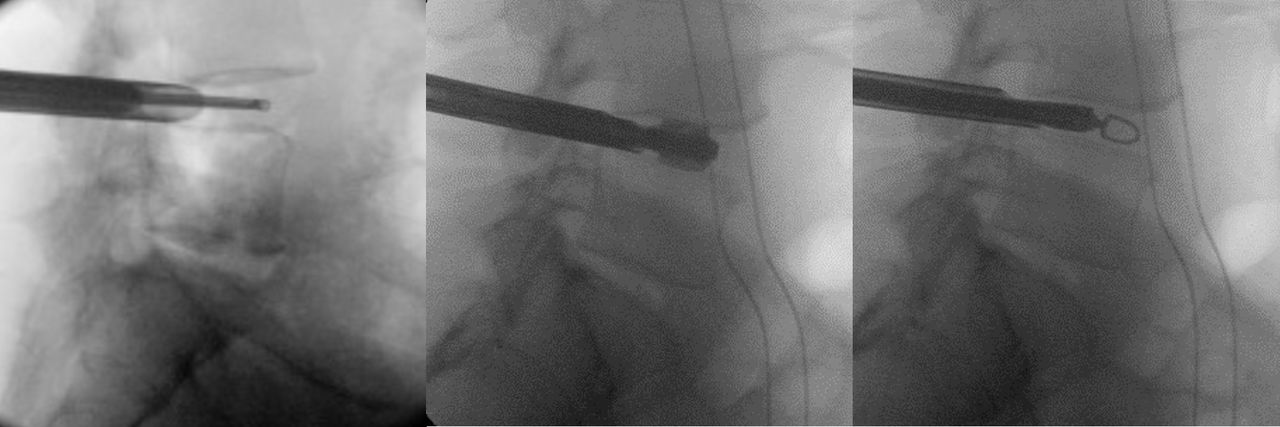
An endoscope is then introduced to visualize the interbody disc and other anatomical landmarks. Discectomy is achieved using specialized tools specifically designed for E-TLIF, including micropituitary rongeurs (Figure 3), expandable shavers (Figure 3), back-biting curettes (Figure 3), electrocautery, and stainless-steel brushes on a powered drill system. The endoscope is reintroduced to the disc space directly to visualize the adequacy of endplate preparation.

Discectomy and endplate preparation performed through working cannula with aid of fluoroscopy using micropituitary rongeurs (left), expandable shavers (middle), and back-biting currettes (right).
The working cannula is subsequently changed to a larger 8.5-mm diameter cannula. Cage height and length are templated using an adjustable trial with fluoroscopic aid. Allogenous bone grafts are packed into the disc space together with recombinant human bone morphogenetic protein-2. This is followed by the insertion of an expandable titanium interbody cage (Figure 4).

Expandable titanium interbody cage before expansion (left) and after expansion with a torque-limiting handle (middle). Final height and position of the expandable cage was confirmed with intraoperative fluoroscopy (right).
The titanium interbody cage is then expanded in situ (Figure 4). The amount of expansion is first estimated by preoperative templating and subsequently confirmed with expansion under lateral view fluoroscopy. The use of a torque-limiting handle prevents expansion beyond the safety threshold.
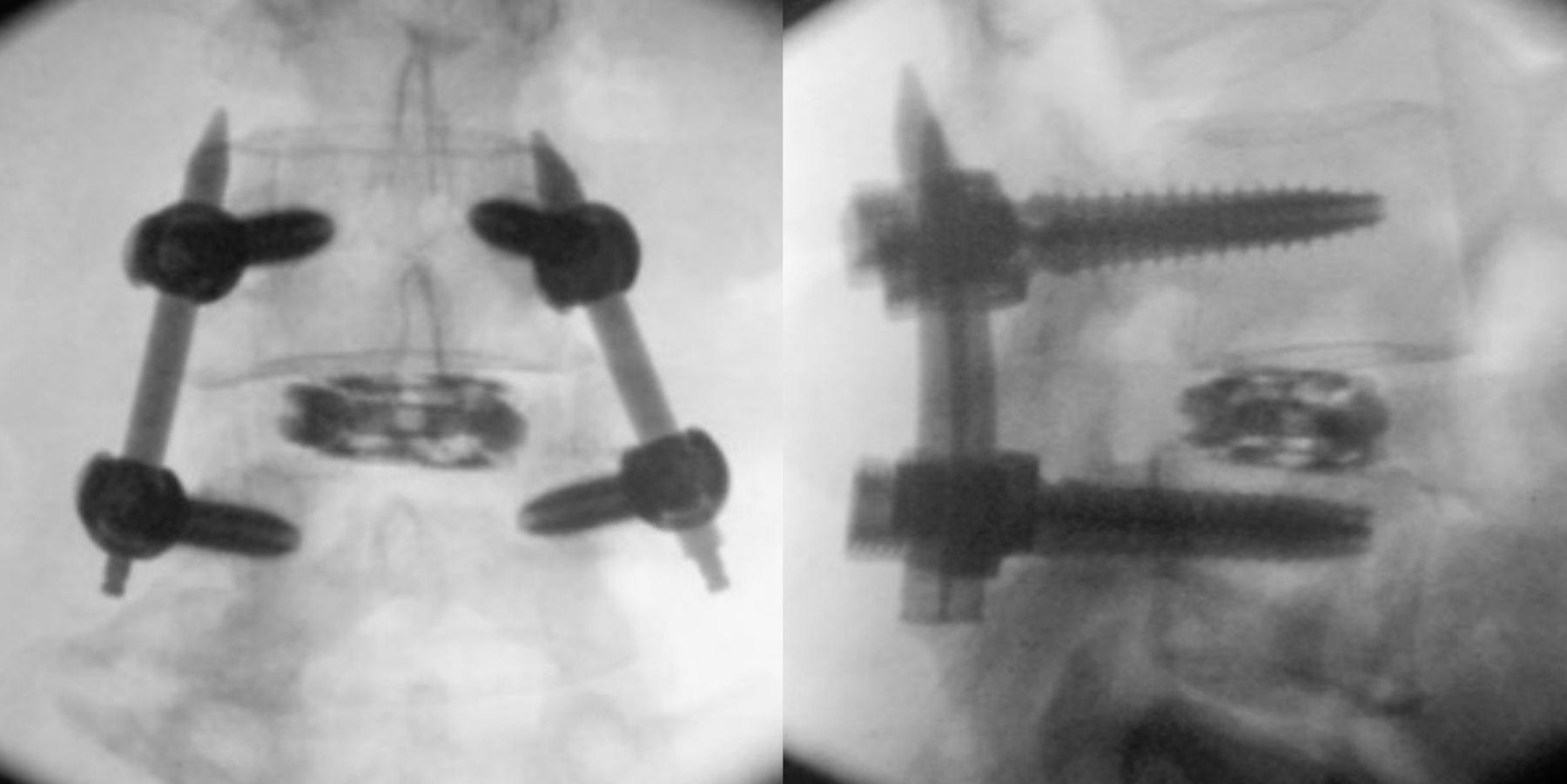
For both E-TLIF and MIS-TLIF, the surgery is completed with the instrumentation of bilateral pedicles with screws and rods (Figure 5).

Final intraoperative fluoroscopic images following insertion of expandable titanium interbody cage and instrumentation of bilateral pedicles with screws and rods.
Clinical and Radiological Outcomes
This study assessed clinical outcomes including surgery duration, blood loss, length of stay, and patient-reported outcomes, as well as radiological outcomes. Patient-reported outcomes included the visual analog score (VAS) for back pain and lower limb pain, Oswestry Disability Index (ODI), and North American Spine Society (NASS) Neurogenic Symptom Score (NSS). All clinical assessments were performed by third-party independent health care professionals not involved in the study within our institution’s Orthopedic Diagnostic Center using a standardized procedure at routine time intervals.
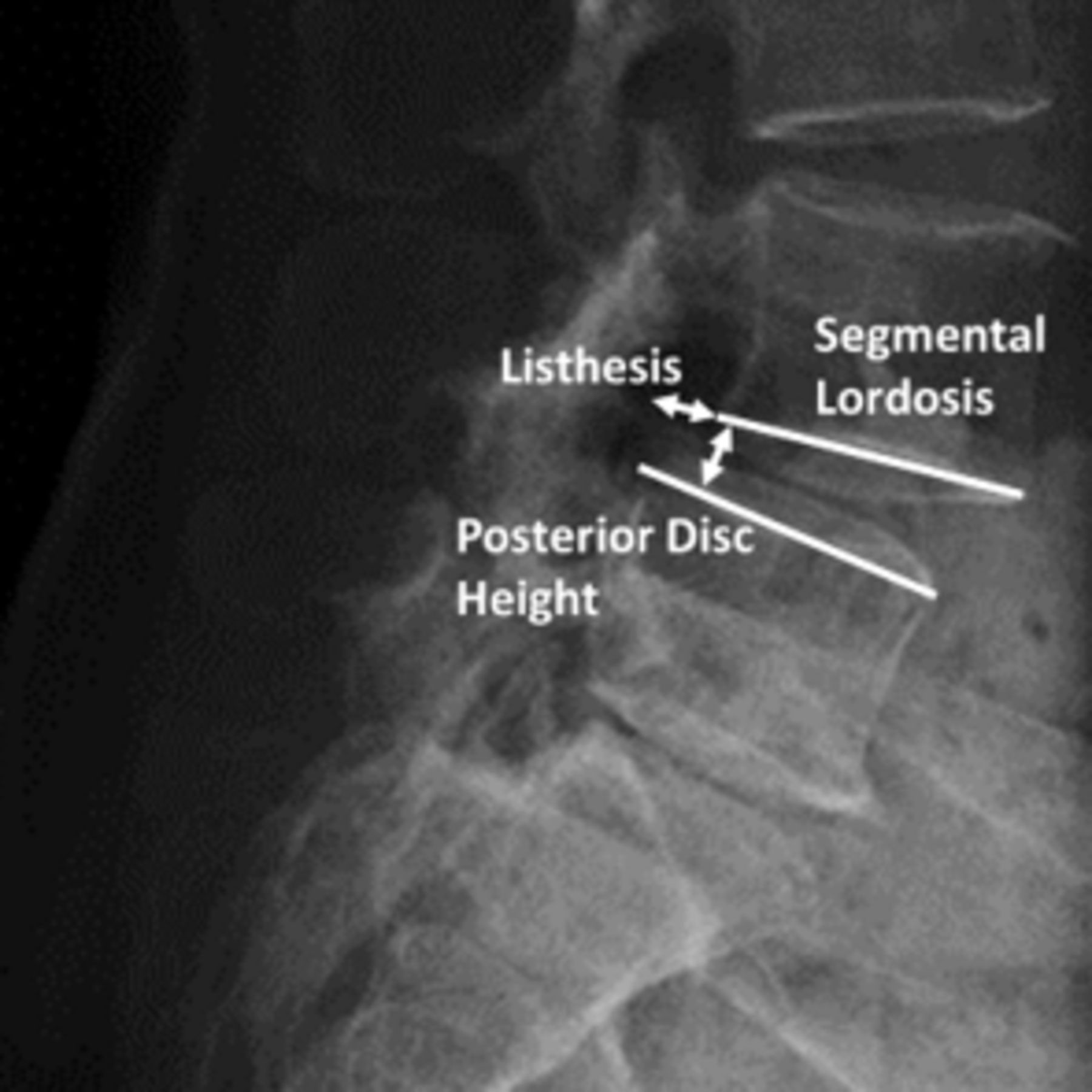
Radiographic parameters assessed included segmental lordosis, posterior disc height, and amount of listhesis (Figure 6). Standard anterior-posterior and lateral radiographs of the lumbar spine were also taken at routine time intervals, including preoperatively and at final follow-up. Segmental lordosis was defined as the angle between the inferior endplate of the cephalad vertebral body and the superior endplate of the caudal vertebral body. Posterior disc height was defined as the distance between the inferior endplate of the cephalad vertebra and superior endplate of the caudal vertebra at the posterior vertebral body line, as described by Hsieh et al.4 The amount of listhesis was measured by calculating the horizontal distance between the posterior vertebral body line of the cephalad vertebral body and that of the caudal vertebral body. Radiographs were also evaluated for cage migration or subsidence as defined in previous studies.5,6

Lateral lumbar radiograph demonstrating the measurement of segmental lordosis, posterior disc height, and amount of listhesis.
Statistical Analysis
Descriptive statistics were reported as means and SDs. Statistical analyses were used to compare the above outcome measures. A paired t test was used to compare continuous variables between the same group of patients, while an unpaired t test was used to compare continuous variables between different groups of patients. The χ2 test was used to compare dichotomous variables. Statistical significance was determined at P < 0.05. Data analysis was conducted using SPSS Statistics for Windows version 22.0 (IBM Corp., Armonk, NY).
Results
Twelve E-TLIF and thirty-four MIS-TLIF patients were included in this study. Both groups were similar in age, body mass index (BMI), gender, and levels at which surgery was performed (Table 1). The average BMI for both groups was overweight according to World Health Organization Asian BMI standards, and the E-TLIF group had 5 overweight patients and 3 obese patients.
Patient demographics.
E-TLIF had shorter surgery duration (165 ± 15 vs 259 ± 43 minutes for E-TLIF and MIS-TLIF group, respectively; P < 0.001), reduced blood loss (83 ± 75 vs 181 ± 225 mL; P = 0.033), and decreased length of stay (1.8 ± 0.9 vs 4.7 ± 2.9 days; P < 0.001) compared with MIS-TLIF (Table 2).
Comparison of postoperative outcomes between endoscopic TLIF and minimally invasive TLIF.
E-TLIF and MIS-TLIF patients had significant improvements at 1 year in all patient-reported outcomes assessed, comprising VAS for back pain, VAS for lower limb pain, ODI, and NSS (Table 3). E-TLIF and MIS-TLIF patients also had significant improvements in the radiographic parameters assessed, comprising segmental lordosis, posterior disc height, and amount of listhesis (Table 3).
Endoscopic TLIF clinical and radiological outcomes.
Between the E-TLIF and MIS-TLIF groups, there was no significant difference in postoperative VAS for back pain (0.6 ± 1.5 vs 0.7 ± 1.8; P = 0.777), VAS for lower limb pain (0.8 ± 1.9 vs 0.3 ± 1.1; P = 0.355), ODI (19.2 ± 10.0 vs 15.9 ± 13.1; P = .378), or NSS (11.1 ± 16.9 vs 14.6 ± 16.4; P = 0.673; Table 2). There was also no significant difference in the change in segmental lordosis (2.9 ± 1.9 vs 2.3 ± 2.6; P = 0.444), posterior disc height (2.7 ± 1.2 vs 2.0 ± 1.4; P = 0.145), or listhesis (−4.4 ± 2.8 vs −3.1 ±2.4; P = 0.157) between the E-TLIF and MIS-TLIF groups (Table 2), making both groups comparable.
No complications were recorded for E-TLIF, while MIS-TLIF had a case of dura tear and another case of meralgia paresthetica. There was no cage subsidence, cage migration, or implant loosening in either group at 1 year.
Discussion
This study demonstrates that E-TLIF performed through a uniportal transforaminal approach can treat degenerative spine conditions successfully with significant improvement in patients’ symptoms and a reduction in VAS for back pain and lower limb pain, ODI, and NSS. This echoes the findings of similar studies that demonstrate the effectiveness of E-TLIF.7,8 This study also shows that E-TLIF can lead to similar improvements in clinical patient-reported outcomes as compared with MIS-TLIF following surgery. Recent reviews confirm no significant differences between the 2 procedures in clinical efficacy.2,9
Compared with MIS-TLIF, E-TLIF had significantly decreased surgery duration, blood loss, and length of hospital stay. The benefits of decreased blood loss and length of hospital stay with E-TLIF have also been reported in recent studies.9,10 A decreased length of hospital stay is likely due to less postoperative pain from a smaller incision and decreased soft tissue violations, resulting in earlier ambulation and rehabilitation (Figure 7).3 In our experience, decreased surgical time is because E-TLIF depends on indirect decompression as opposed to MIS-TLIF, which requires direct decompression of neural elements.11 E-TLIF performed through Kambin’s triangle avoids the need to perform a facetectomy to access the disc space for the insertion of an interbody fusion device. Nevertheless, a recent meta-analysis comparing E-TLIF and MIS-TLIF shows that E-TLIF has a longer operating time compared with MIS-TLIF, suggesting that our results may not be replicated in other institutions.2

Postoperative and 1-year photographs of stab incisions following single-level endoscopic transforaminal lumbar interbody fusion.
This study demonstrates that E-TLIF can restore posterior disc height and correct listhesis (Figure 8), thereby indirectly resulting in neuroforaminal and lateral recess decompression. Despite the fact that E-TLIF requires operating through an even smaller surgical window compared with MIS-TLIF, we have shown in this section that the degree of posterior disc height restoration and listhesis correction after E-TLIF is not inferior to that of MIS-TLIF. The use of expandable titanium interbody cages is essential to achieving this goal, as the interbody cages, which are inserted through an 8.5-mm working cannula, can reach a final height of up to 14 mm after in situ expansion. Overexpansion of the cage can be prevented by preoperative templating, using a torque-limiting handle, and finally confirmation with lateral view fluoroscopy to prevent the risk of future subsidence. Additional correction of spondylolisthesis and stabilization of the operated spinal segments were obtained through the reduction of pedicle screws to rods. Lv et al12 also reported in their study that E-TLIF, though the posterior-lateral approach, can achieve similar reduction of spondylolisthesis as MIS-TLIF.

Preoperative (top) and postoperative (bottom) lumbar spine radiographs of a patient who underwent successful endoscopic transforaminal lumbar interbody fusion for treatment of lower limb radiculopathy and lower back pain with significant improvement of symptoms at 1 year. Postoperative radiographs demonstrate reduction of L4-L5 anterolisthesis and improvement of posterior disc height.
This study also demonstrates that E-TLIF can be performed safely on overweight and obese patients with good results. Five overweight and 3 obese patients underwent E-TLIF without complications or significantly increased surgical difficulty and had improvement in their symptoms. Given this positive early experience with E-TLIF in patients with high BMI, there may be a further role for E-TLIF in these patients. MIS-TLIF has previously been demonstrated to be safe in obese patients and has better outcomes compared with open TLIF with regards to decreased blood loss, shorter hospitalization, reduced dural tear, and wound infection rates.13 Nevertheless, performing conventional MIS-TLIF using METREx tubes in obese patients is technically more challenging as longer tubes must be utilized due to the thickness of subcutaneous fat, resulting in a greater working distance. However, this technical challenge is not present when performing E-TLIF in obese patients, as the endoscopic view during endoscopic lumbar spine surgery is independent of the working distance between skin and intervertebral disc.14 Further studies will be useful to further elucidate the benefits of E-TLIF in patients with a high BMI.
Previous systematic reviews suggest similar complication rates between the 2 procedures.2,9 In this study, no complications were recorded for E-TLIF, while the MIS-TLIF group had a case of dura tear and another case of meralgia paresthetica. The E-TLIF approach avoids direct decompression of neural elements, and the thecal sac is not exposed directly, thus reducing the incidence of dura tear. The second patient who underwent MIS-TLIF developed paresthesia over her right thigh—likely due to compression of the lateral femoral cutaneous nerve that occurred due to positioning on the surgical table during the MIS-TLIF procedure. Patients who lie prone on the Jackson table for a prolonged period have a risk of compression of the lateral femoral cutaneous nerve at the level of the anterior superior iliac spine, resulting in meralgia paresthetica, and this is an unfortunate complication of positioning. This also highlights an advantage of E-TLIF, which is shorter operative duration, as decreased surgical time has been associated with lower rates of postoperative meralgia paresthetica.15
This study assessed all consecutive E-TLIF and MIS-TLIF cases performed by a single surgeon from a tertiary spine institution. All patients had at least a 1-year follow-up. Another advantage of this study is that the surgical technique is consistent for all patients since it is performed by the same surgeon. While patients who underwent E-TLIF had good results postoperatively in our study, we concede that E-TLIF may not be suitable in certain cases. Extremely narrow Kambin’s triangle due to collapsed foramen or intervertebral disc height is a relative contraindication for the endoscopic technique. Anatomical limitations can restrict the application of the transforaminal endoscopic approach.16 A smaller working space through a narrow Kambin’s triangle can also cause technical difficulties for thorough disc preparation and safe cage insertion, leading to complications such as exiting nerve root injury, nonunion, or case migration.8
Conclusion
While study size was limited as E-TLIF is a relatively new technique in our institution, 1-year results are encouraging and demonstrate that in an Asian population, E-TLIF can be a safe and efficacious option that achieves similar clinical and radiological results to MIS-TLIF, with the additional benefits of decreased surgical duration, blood loss, and length of hospital stay.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethical Standards Approval was obtained from the institution’s ethics committee. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.