


Abstract
Background Antibiotic treatment of spondylodiscitis is influenced by antibiotic stewardship; specifically, empirical antibiotic therapy is avoided in favor of—delayed—targeted antibiotic therapy after microbiological diagnosis. Only patients with neurological deficits or clinical signs of sepsis should be treated by empirical antibiotic therapy. However, the level of evidence for this treatment concept is weak.
Purpose The aim of this study was to investigate whether patients who were treated with a nontargeted antibiotic therapy show a worse outcome than patients who were exclusively treated with targeted antibiotic therapy.
Study Design/Setting A retrospective single-center data analysis.
Patient Sample We included 201 patients with spondylodiscitis who were treated at the authors’ institution between 2013 and 2020.
Outcome Measures Mortality rate, time in hospital, development of laboratory parameters, and development of pain (visual analog scale).
Methods We performed a retrospective data analysis of patients who were treated for spondylodiscitis from January 2013 to March 2020. Clinical and demographic data as well as outcome and complications were recorded and analyzed. We investigated whether patients who were treated by a nontargeted antibiotic therapy had a worse outcome than patients who were exclusively treated by targeted antibiotic therapy and which other clinical factors had an impact on clinical outcome.
Results A total of 201 patients were included, 37 of whom developed sepsis during their hospital stay, and 14 of these 37 patients died. The 14 patients who died represented (10.0%) of the subgroup who received an empirical antibiotic treatment before the targeted antibiotic therapy (n = 141). There were 0 deaths in the subgroup who did not receive an empirical antibiotic treatment (P < 0.05). The time to diagnosis since admission to the hospital was 10.5 (2.2) days in patients with sepsis; in patients without sepsis, it was 5.2 (0.9) days (P < 0.05).
Conclusions Based on the results of this investigation, the authors recommend delaying antibiotic therapy until targeted antibiotic therapy is possible. Furthermore, early diagnosis of spondylodiscitis and prevention and early detection of sepsis are essential to reduce the mortality rate of patients with spondylodiscitis.
Level of Evidence 3.
INTRODUCTION
Spondylodiscitis is an infectious disease of the spine, which usually shows unspecific clinical symptoms.1–3 The incidence of spondylodiscitis varies between 1:100,000 and 1:250,000 and represents around 3% to 5% of all cases of osteomyelitis.3,4
Due to the unspecific clinical symptoms of patients with spondylodiscitis, there is a delay of 2 to 6 months between the beginning of the first symptoms and the diagnosis.1–3,5,6 This delay may be the main reason why spondylodiscitis is a severe and potentially life-threatening disease. The mortality rate of spondylodiscitis has been reported to be between 2% and 20%.7
The key component of a successful treatment for spondylodiscitis is to treat the infection with adequate antibiotic treatment.8,9 Additional surgical treatment might be necessary as an internal fixation if instability of a spinal segment is detected7,10,11 or if an operative debridement and decompression of the spinal canal is necessary.12,13
The most commonly detected microbiological pathogen in spondylodiscitis is Staphylococcus aureus6,14–16 followed by Gram-negative pathogens in 4% to 30% of the cases and streptococci or enterococci in 5% to 30% of the cases.17 Polymicrobial infections are unusual, occurring in about 2.5% of the total number of cases.7
Pathogen detection is mostly performed by blood culture, percutaneous biopsy, or intraoperative tissue sampling.2,4,15,18 However, identification of the pathogen is only successful in 49% to 83% of cases.5,10,15,16,18,19 One of the main reasons for the failure of pathogen identification is a prior empiric antibiotic therapy.4
Antibiotic stewardship programs are becoming more widely implemented and therefore strongly influence the treatment of spondylodiscitis.16,20,21 To avoid ineffective or unnecessarily toxic or expensive treatments, empirical antibiotic therapy is avoided in favor of delayed targeted antibiotic therapy after microbiological diagnosis. For this reason, it is particularly important that the antimicrobial treatment is not commenced until the exact pathogen is identified. An exception from this procedure is mandatory in patients with severe sepsis, which should be treated by an empirical antibiotic regimen.9
The level of evidence for this treatment concept is still weak.3,9,22 Therefore, we conducted an investigation on this topic. The primary objective of this study was to analyze whether there are significant differences in the outcome of patients with spondylodiscitis who received a target antibiotic therapy compared with the outcome of those who received empirical antibiotic therapy.
MATERIALS AND METHODS
This study was designed as a single-center retrospective cohort study and was performed in cooperation with the local Institute for Medical Microbiology and Hospital Hygiene.
Patients who needed to be treated for spondylodiscitis as an inpatient in our institution between January 2013 and March 2020 were identified in the clinical documentation system by diagnostic code. Inclusion and exclusion criteria are listed in Table 1.
Inclusion and exclusion criteria.
Clinical and demographic data as well as outcome and complications were recorded and analyzed. As potential outcome parameters, we collected data on the duration of the hospital stay, need for surgery, development of laboratory parameters of the infection, development of pain, and level of mobility for each patient as well as the mortality rate. Furthermore, we noted whether patients developed sepsis during the hospital stay. Sepsis was defined according to the 2016 updated guidelines from Singer et al with an increase in the Sequential Sepsis-related Organ Failure Assessment score of 2 points or more. The score is based on 6 different scores, 1 each for the following systems: respiratory (ratio between PaO2/FiO2), cardiovascular (mean arterial pressure or administration of vasopressors required), hepatic (bilirubin level), coagulation (number of plates), renal (creatinine or urine output), and neurological (Glasgow Coma Scale) systems.23 Surgery was normally performed in patients with neurological deficit, sepsis, epidural abscess, instability, or failure of the conservative treatment.
We documented the performed antibiotic treatment protocols and the identified pathogens for each patient. If antibiotic therapy was commenced before a pathogen was identified, it was classified as empirical antibiotic treatment. All patients received at least 6 weeks of antibiotic treatment with a minimum of 2 weeks of intravenous administration of antibiotics. We investigated whether patients who received nontargeted (empirical) antibiotic therapy had a worse outcome compared with patients who received targeted antibiotic therapy and which other clinical factors had an impact on clinical outcome.
Statistical analysis was performed by SPSS 25 (IBM, Armonk, USA). Descriptive data are given as mean and SEM. We tested all continuous variables for normal distribution by Kolmogorov-Smirnov tests. None of the variables showed normal distribution. Thus, we performed χ2 tests and Mann-Whitney U tests.
This study was approved by the local ethics committee of a university hospital (Register number 2020–914) and was conducted according to the revised Declaration of Helsinki.
RESULTS
We identified 253 patients who were treated for spondylodiscitis as inpatients in our institution between January 2013 and March 2020. After the application of the inclusion and exclusion criteria, we enrolled 201 patients to our investigation. Thirty-one patients were excluded due to an incomplete set of data, 11 patients were excluded due to severe neurological deficits at the time of admission to the hospital, and 10 patients were excluded due to severe clinical signs of sepsis at the time of admission to the hospital.
Eighty-seven patients were women (43.3%) and 114 were men (56.7%). The mean age of the patient was 65.5 (0.99) years. Seventy-four (36.8%) patients were classified as multimorbid.
The mean duration of the hospital stay was 33.63 (1.78) days. The time to diagnosis since admission to the hospital was 6.3 (0.8) days for all patients. In patients with sepsis, it was 10.5 (2.2) days, and in patients without sepsis, it was 5.2 (0.9) days (P < 0.05, effect size 0.63).
Overall, 123 (61.2%) patients received conservative treatment, and 78 (38.8%) patients needed an operative treatment for spondylodiscitis. Fourteen (7%) patients died, and 187 (93%) were discharged from the hospital. In 66 (32.8%) of the 201 patients, complications such as sepsis, intraspinal abscess, or unstable fracture occurred. Of the 14 patients who died, 13 (92.9%) patients were multimorbid. Approximately 40% (74 of 184) of the successfully treated patients underwent surgery during the hospital stay, whereas only 28.6% (4 of 14) of the patients who died underwent surgery.
In 140 patients (69.7%), the type of pathogen could be identified. The identified pathogens are shown in Table 2. In 22 (10.9%) patients, more than one pathogen could be identified. S aureus was most commonly detected. From the 74 cases of S aureus, 13.5% were methicillin-resistant S aureus (MRSA). Overall, MRSA was detected in 5% of our study population. Pathogens summed up under “others” were Fusobacterium nucleatum, Klebsiella pneumoniae, Parvimonas micra, Proteus vulgaris, Streptococcus pneumoniae, Pseudomonas aeruginosa, Serratia marcescens, and Salmonella enteritidis.
Type of detected pathogen.
S aureus was also the most common pathogen in all the patients who died. The rate of patients in whom S aureus was detected was higher in the patients who died than in the overall collective (57.1% vs 36.8%). Escherichia coli is another pathogen that was more frequently detected in the patients who died. Escherichia coli was detected in 5.5% in the overall collective of patients and in 21.4% of the patients who died. All patients in whom a pathogen was detected and who died were from the subgroup of patients who received empirical antibiotic treatment prior to targeted antibiotic treatment.
The methods of pathogen identification are shown in Table 3. The method of pathogen identification had no effect on time-to-treatment with targeted antibiotics or on the patients’ outcome.
Type of specimen for identification of the pathogen.
In every patient in whom a pathogen could be detected, the targeted antibiotic treatment started within a mean of 0.95 (0.2) days. Time-to-treatment with targeted antibiotic treatment after identification of the pathogen in blood cultures was a mean of 0.9 (0.3) days; after detection in an intraoperative specimen, 1.1 (0.3) days; after detection in probes from a percutaneous puncture, 1.0 (0.1) days; and after simultaneous detection in multiple probes, 0.9 (0.2) days. The method of pathogen identification in the subgroups of patients who developed sepsis or died during the hospital stay showed no significant impact on the time to treatment of targeted antibiotic therapy (Table 3).
Every patient in whom a pathogen could be identified received targeted antibiotic therapy. Mean time-to-treatment with a targeted antibiotic was 13.5 (4.0) days in patients who survived and 1.8 (1.7) days in patients who died (P < 0.05, high statistical power of 0.95). An additional infection other than spondylodiscitis was suspected in 80 (39.8%) of the patients. Endocarditis was diagnosed in 16 of these 80 patients. An iatrogenic origin of the spondylodiscitis was found in 27 (13.4%) patients.
Every patient who died during the hospital stay had a nonvertebral infection site in addition to the spondylodiscitis. Six of the 14 patients who died had pneumonia in addition to the spondylodiscitis, and 3 of the 14 patients who died had endocarditis.
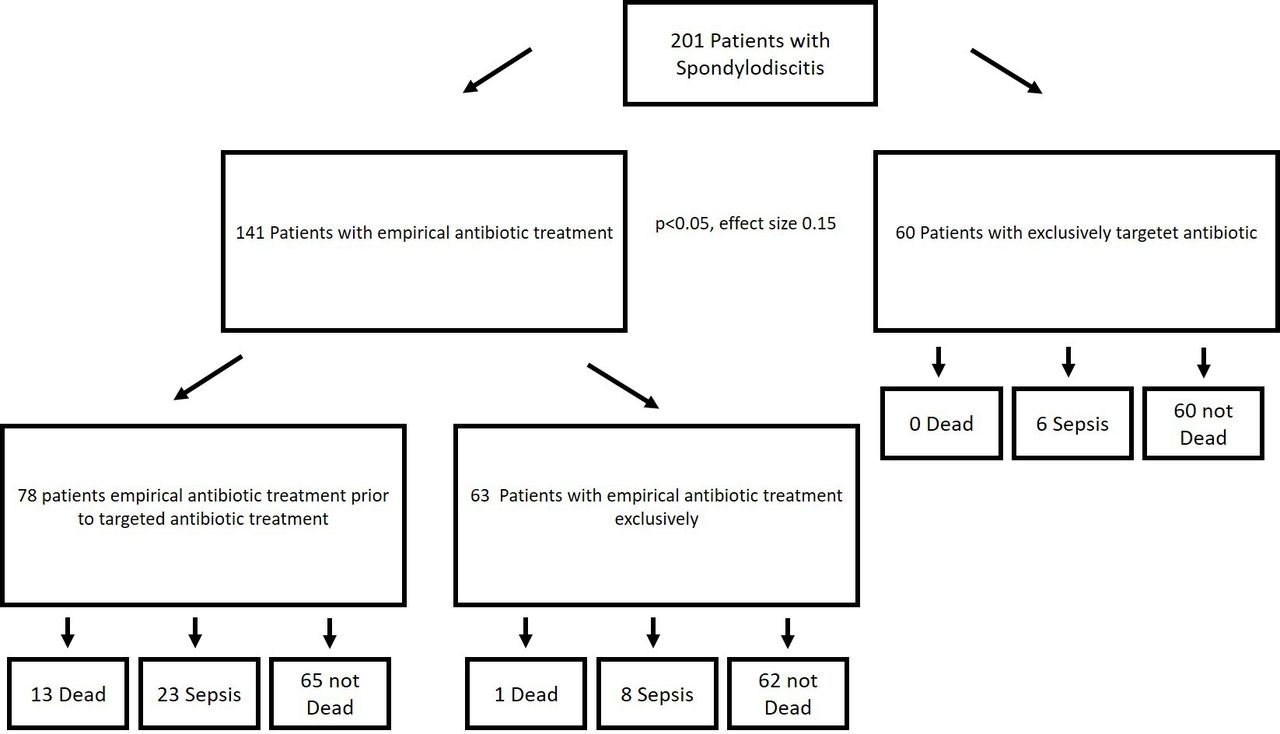
Fourteen of 141 patients (10.0%) who received empirical antibiotic treatment with or without a following targeted therapy died. One of these 14 patients received empiric antibiotic therapy because no pathogen could be isolated. Thirteen of the 14 patients who died received targeted antibiotic therapy after the empiric treatment. Out of all the patients who did not receive empirical antibiotic treatment, 0 died (P < 0.05). The outcome of the patients and the development of sepsis depending on the antibiotic treatment regime is shown in the Figure.

Outcome of the patients according to the subgroup analyzis.
Thirty-seven of 201 patients developed sepsis during their hospital stay, and 14 of these 37 patients died. None of the patients without sepsis (0 of 164) died (P < 0.001, effect size 0.61 [high]). The mean duration between hospital admission and diagnosis of spondylodiscitis was 10.5 (2.17) days in cases of sepsis and 5.2 (0.85) days in cases without sepsis (P < 0.025, effect size 0.77 [high]). The mean duration for identification of the pathogen in patients with sepsis was 1.8 (1.7) days.
In the patients who developed sepsis during the hospital stay, the rate of patients in whom S aureus (56.7% vs 36.8%) or E coli was detected (8.1% vs 5.5%) was higher than in the overall collective. In both subgroups (empirical antibiotic treatment prior to targeted antibiotic treatment and targeted antibiotic treatment only), there was a predominance of S aureus in the patients who developed sepsis during the hospital stay. E coli was only predominant in the subgroup of patients who received empirical antibiotic treatment prior to targeted antibiotic treatment. The differences between these subgroups were not significant. The rate of patients with sepsis in whom no pathogen could be detected was less than in the overall group of patients (21.6% vs 30.3%).
DISCUSSION
In this investigation, we analyzed the data of 201 patients to examine whether there were significant differences in the outcome of patients who received a targeted vs an empirical antibiotic treatment due to spondylodiscitis. The demographic data of our group of patients with a mean age of 65.5 years and a male predominance are comparable to data reported in other investigations.4,7,24,25 This suggests that our study population was representative.
Sobottke et al reported a successful pathogen detection in 49% up to 83% of the cases.4 In our group of patients, we were able to detect the pathogen in 69.7% of the cases. The most successful method of pathogen detection in our group of patients was through blood cultures, followed by operative biopsies and computer tomography-guided needle biopsies. None of these latter techniques of pathogen detection were more effective than the others in our group of patients. Thus, we recommend combining the different techniques of pathogen detection. This recommendation is comparable to that of other studies.2–8,13,16,18,21
The spectrum of pathogens in our group of patients is different compared with the reported data from other study groups. As in former reports, S aureus was the most commonly detected pathogen in our group of patients with spondylodiscitis.4,6,7,15,16,26 However, we also found a significantly lower number of Gram-negative pathogens and a significantly higher number of patients with multiple pathogens.
When looking at the subgroups of patients who developed sepsis or died during the hospital stay, the rate of patients in whom S aureus or E coli was detected was higher than in patients who did not die or develop sepsis. This finding suggests that these 2 pathogens are more aggressive than others. Patients in whom these pathogens are detected should, based on these results, be observed even more carefully for potential signs of sepsis. In our investigation, we did not explicitly analyze the virulence of the detected pathogen, which is known to have an important influence on the patient’s outcome and the risk of developing sepsis.
Spondylodiscitis is often transferred hematogenously—because of bacteremia—from either the skin, the respiratory tract, the genitourinary tract, the gastrointestinal tract, or the oral cavity.16,27–29 In our group of patients, we found another nonvertebral site of infection in 40% of the patients. An iatrogenic origin for spondylodiscitis was found in 13.4% of the cases. Every patient who died had a nonvertebral infection site in addition to spondylodiscitis. This is potentially caused by the fact that every patient who died developed sepsis. Developing additional infection sites is more likely in patients with sepsis, presumably because of bacteremia, than in patients without sepsis. However, we were not able to discern whether the patient’s spondylodiscitis was the primary or the secondary infection site.23
Our data showed that the most severe complication in patients with spondylodiscitis was sepsis. None of the patients without sepsis died. In our group of patients, sepsis occurred in 18% of the cases. In patients who developed clinical signs of sepsis, the diagnosis of spondylodiscitis had been established significantly later than in those patients without sepsis. This fact shows that an early diagnosis of spondylodiscitis is essential for a successful treatment. Spondylodiscitis should always be considered when a patient presents with general signs of an infection of unknown origin. Due to generalized pain and lack of movement in these patients, back pain as a key symptom of spondylodiscitis could stay undetected under the veil of the multitude of symptoms.
Our data showed that only patients with sepsis died. This may indicate that it is safe to postpone antibiotic treatment for patients without sepsis until successful pathogen detection.
If there are no signs of sepsis but clinical symptoms of infection are still present, we recommend taking blood cultures every second day for a period of 10 to 14 days. If no pathogen is detected in this period, we recommend beginning an empirical antibiotic treatment. Patients with sepsis need an immediate start of an empirical antibiotic treatment, if possible directly after the first blood culture or biopsy has been taken. Based on recent literature, we recommend at least 6 weeks of antibiotic treatment.16,25
Navarro-Navarro et al showed that biopsies had significantly more often positive results if no antibiotic treatment was given before the biopsy, which also suggests clinical benefits for the patient if no empiric antibiotic treatment is given before the pathogen could be identified.18
The mean duration between hospital admission and the beginning of targeted antibiotic treatment was significantly longer (13.5 vs 1.8 days) in patients who did not die than in patients who died. However, the earlier onset of targeted antibiotic therapy in patients who died might be due to a positive blood culture of critical patients, who have bacteremia, in contrast to noncritical patients, who contained the infection locally.30
Patients who died during inpatient treatment of spondylodiscitis received empirical antibiotic therapy significantly more often than patients who did not die. No patient who did not receive empirical antibiotic therapy died. A bias of this investigation is that we did not perform a separate analysis of patients who exclusively had an empiric antibiotic treatment and patients who had empiric antibiotic treatment prior to targeted antibiotic therapy. This subanalysis could not be performed due to issues with multiple testing (determined during the prior power analysis for the study design) and because of the different sizes of the groups. However, due to the high statistical power of the result and because the timing of the beginning of the targeted antibiotic therapy did not show any significant influence on patient outcome, our data seem to indicate that empirical antibiotic therapy should be avoided if possible (no clinical signs of sepsis, no neurological deficits).
Several investigations report a poorer outcome for patients if a nonsensitive antibiotic treatment (ie, an antibiotic treatment to which the pathogen is immune) is administered.4,8,9,16,20,21 The group of patients who received exclusively an empirical antibiotic treatment without a change of the antibiotic regimen after identification of a pathogen consisted—naturally—of patients in whom no pathogen could be identified. Since the type of empirical antibiotic treatment is selected with the aim to be effective on the most likely pathogens, by “luck” or by a careful selection of the antibiotic treatment, effective empirical antibiotic treatment will in most cases prevent identification of the pathogen because a high percentage of the pathogens are effectively eliminated. Those patients in whom a pathogen could be detected after administration of an empirical antibiotic treatment have, in most cases, received a noneffective—or less effective—(for “their” pathogen) empirical antibiotic treatment, which led to persistent bacteremia and made identification of the pathogen possible. These patients, in our investigation, showed an inferior outcome than patients who exclusively received targeted antibiotic treatment. Considering that there are many possible confounding factors for the other analysis, we decided, prior to the investigation, to analyze the 2 latter groups.
Comparable to the literature, our data showed that dying from spondylodiscitis was significantly associated with multimorbidity.16,25 Patients who died underwent surgery less often (28.6% vs 39.6%) during the hospital stay. This may result from the fact that these patients had medical conditions that did not allow for surgical procedures under general anesthesia.
A limitation of our investigation is that we performed retrospective data analysis and that there was no official study protocol for the treatment of the patients. However, due to a standard operating procedure in our department according to the treatment of spondylodiscitis, the treatment of the patients was comparable without an official study protocol.
CONCLUSION
Based on the results of our investigation, we recommend delaying antibiotic therapy until targeted antibiotic therapy is possible. Furthermore, our data suggest that an early diagnosis of spondylodiscitis, along with prevention and early detection of sepsis, is essential to reduce the mortality rate of patients with spondylodiscitis.
Acknowledgments
From 2009 to July 2018, patients were treated in the Department of Orthopedic Surgery by Dr R. Kraupse. Patients included between August 2018 and March 2020 were treated in the Department of Orthopedic and Trauma Surgery by Dr J. Windolf.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests M.R.K. reports personal fees from Globus Medical outside the submitted work.
Data Availability Statement The datasets generated during and/or analyzed during the current study are not publicly available due data protection but are available from the corresponding author on reasonable request.
Authors Contributions M.P.: conception and design, administrative support, collection and assembly of data, provision of study materials or patients, data analysis and interpretation, manuscript writing, and final approval of manuscript. M.E.R.: administrative support, collection and assembly of data, provision of study materials or patients, data analysis and interpretation, manuscript writing, and final approval of manuscript. M.K.V.: administrative support, collection and assembly of data, manuscript writing, and final approval of manuscript. J.W.: administrative support, provision of study materials or patients, manuscript writing, and final approval of manuscript. M.R.K.: administrative support, collection and assembly of data, provision of study materials or patients, data analysis and interpretation, manuscript writing, and final approval of manuscript.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.