


Abstract
Background Tubular spine surgery has emerged as a hallmark of minimally invasive spine (MIS) procedures. In recent years, thanks to technological advances, tubular dilators and retractors have been integrated with digital cameras to allow for ergonomic, high-definition visualization of the surgical field.
Objective To detail the evolution, ergonomics, economics, and outcomes of camera-based tubular spine surgery, spanning the origins of MIS tubular techniques to the current use of operative microscopes and tube-mounted digital cameras (TMDCs).
Methods This is a narrative review of studies examining the evolution of tubular spine surgery as well as its most recent advances, with a particular emphasis on advances in visualization of the surgical field.
Results Despite early resistance to tubular techniques due to a steep learning curve, minimally invasive tubular approaches are being increasingly adopted by the mainstream spine surgical community, which has resulted in an expansion of both indications and procedural modalities. This can largely be attributed to the increased quality of visualization, as evidenced by improvements in microscopes as well as emerging technologies like exoscopes and TMDCs. Tubular MIS procedures have also achieved superior efficacy compared with open surgical approaches for the treatment of several spinal pathologies while allowing for improved ergonomics, which may have lasting consequences on surgeon longevity.
Conclusions Advances in visualization technologies have allowed tubular surgery to become an effective, ergonomic, and muscle-sparing alternative to open spine surgery. Further research is necessary to quantify the true costs and outcomes associated with nascent TMDC technology.
Clinical Relevance This work elucidates developments in visualization for tubular spine surgery.
Level of Evidence 5.
Introduction
Spine surgery has undergone tremendous change over the past few decades, especially in the realm of minimally invasive surgery (MIS) procedures. MIS was initially introduced with the goal of achieving proper decompression of the neural elements while minimizing iatrogenic damage to musculature and surrounding tissue.1 Tubular surgery, which involves inserting a hollow tube into the paraspinal musculature and gradually dilating it to create a direct pathway to the spine, was proposed as a minimally invasive technique to reduce muscle damage.2,3 In recent years, thanks to technological advances, tubular dilators and retractors have been integrated with a variety of novel visualization modalities, ranging from operative microscopes (OMs) to exoscopes to miniature cameras, ultimately allowing for ergonomic, high-definition visualizations of the surgical field.3–5 Moreover, these technologies have achieved increasing adoption by the mainstream spine surgical community despite encountering early resistance due to a steep learning curve.3,6,7 In this comprehensive review, we detail the evolution, ergonomics, economics, and outcomes of these visualization technologies for tubular spine surgery, spanning the origins of MIS tubular techniques to the current use of OMs, exoscopes, and tubular-mounted digital cameras (TMDCs).
Evolution of Tubular Spine Surgery
To appreciate the significance of tubular spine surgery, it is helpful to review the origins of MIS. Spine surgery at the beginning of the 20th century was primarily performed in an “open” manner which decompressed the thecal sac and nerve roots through subtotal or total laminectomy. This required extensive dissection of paraspinal musculature and ligamentous structures, often leading to suboptimal postoperative clinical outcomes.3 This led to an interest in less invasive surgical approaches, culminating in 19788 with the introduction of interlaminar approaches to removing disc herniations. Interlaminar approaches, especially those using microscopy, conferred significantly less damage to surrounding paraspinal soft tissues. These approaches were not perfect, though, as they were still associated with iatrogenic injuries to the facet joint as well as to some surrounding tissue.3 Nonetheless, for decades, the use of the OM became the gold standard for the treatment of lumbar disc herniations, as it allowed for spine surgery to be performed with smaller incisions, less blood loss, and greatly enhanced visualization.1
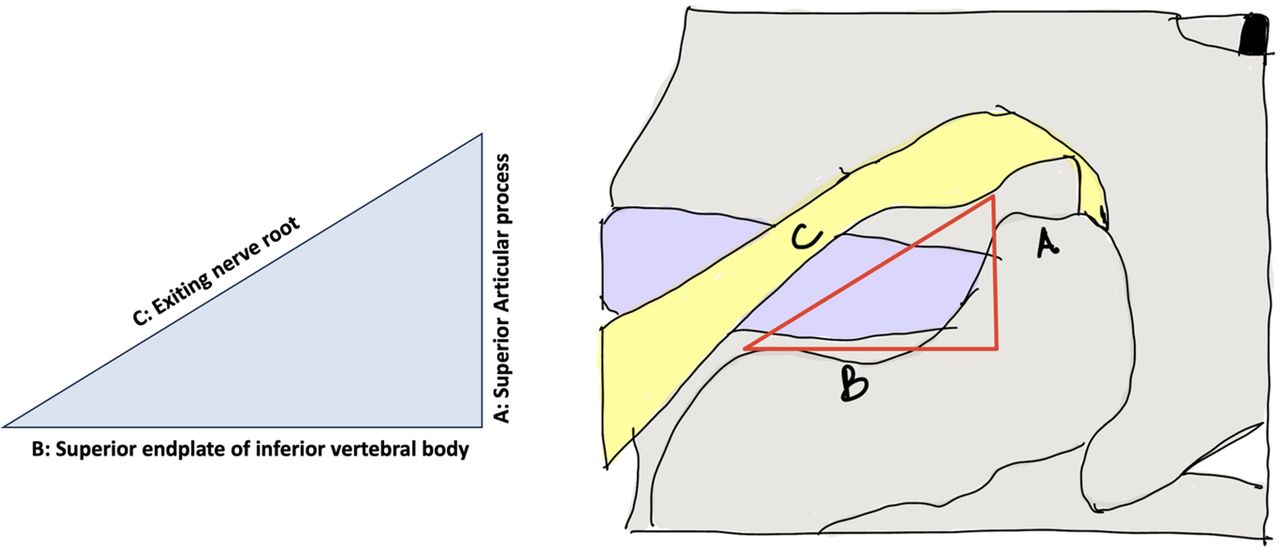
The next major development in spine surgery was marked by the introduction of the “Kambin triangle”3,9 (Figure 1), an anatomic space that could be used as a safe working area to treat lumbar disc pathology. This space later became the catalyst for the original tubular spine surgical approaches. In 1999, Foley and Smith10 introduced a novel technique, termed the microendoscopic discectomy, which used both a tubular retractor and a disposable endoscope to treat far-lateral disc herniations. As described in this seminal study, a 15-mm paramedian incision was made, followed by the placement of an endoscopic tubular retractor with the goal of treating unilateral, single-level radiculopathy secondary to disc herniation. All 11 procedures described in the study were performed in an outpatient setting under epidural anesthesia, and improvement was shown in all patients postoperatively.10

Borders of Kambin triangle.
Despite the success of this study, endoscopy did not become widely implemented in the immediate aftermath of these findings, primarily due to the poor image quality of the endoscope,5 as well as the steep learning curve associated with its use.3 Nonetheless, spine surgeons saw the value of tubular surgery and started utilizing larger tubular retractors while replacing the endoscope with OMs for enhanced visualization.1,3
Tubular Surgery Utilizing Microscopes
When tubular retractors and dilators were first introduced in spine surgery, they were criticized for providing a narrower field of vision compared with open surgical approaches, which disoriented surgeons and led to confusion regarding the exact location of various anatomic structures.3 Furthermore, there appeared to be no ideal tube size; narrow and longer tubes were more difficult to operate in sufficient space, while wider tubes demonstrated more potential to damage muscles surrounding the posterior arch of the spine.2
Thanks to improvements in surgical tools as well as a general increased exposure to MIS, microscope-based tubular retractors are now commonly applied to a variety of spine procedures. In 2002, Foley and Lefkowitz modified the conventional transforaminal lumbar interbody fusion (TLIF) procedure to employ tissue-sparing mechanisms, termed “MIS-TLIF.”11–13 As the authors describe, this technique involves the insertion of a tubular retractor to the facet joint for facetectomy, discectomy, and placement of an interbody implant and bone graft. The tubular retractor is then removed, followed by pedicle screw fixation using a percutaneous screw-rod system.11
Paramedian tubular approaches soon gained popularity among spine surgeons, and several studies described the use of these approaches for lumbar discectomy, thoracic discectomy, tumor removal, and infection treatment, among others.14–18 Today, there is great variability between surgeons in the type of retractors used to access the facet joint for spine procedures. Different options include nonexpendable tubular tractors, expendable retractors, or both.11 Nonetheless, the use of tubular retractors is consistent throughout various MIS paradigms, including for MIS-TLIF.
During microscope-assisted tubular procedures, the OM may be introduced into the field after a tubular retractor has been placed over serial dilators and the paraspinal musculature has been dilated, as described above. MIS procedures that utilize tubular retractors, such as MIS-TLIF as well as MIS microdiscectomy, have consistently demonstrated superior outcomes to their “open” surgical counterparts. More specifically, the use of the microscope in MIS tubular procedures has been associated with improved outcomes compared with the “naked eye” approach. In a 2024 study comparing the efficacy of microscope-assisted MIS-TLIF to naked-eye MIS-TLIF, Zhang et al found that microscope-assisted surgeries were associated with less trauma, less bleeding, shorter postoperative stay, and faster recovery.19 In a similar study comparing microscope-assisted MIS-TLIF to conventional “open” TLIF, Peng et al found that the former was associated with less injury, less blood loss, and faster postoperative recovery. Tubular approaches using microscopes have also been described for other parts of the spine, such as cervical foraminotomy.20 Despite the visualization advantages provided by the microscope, however, OMs have been associated with poor ergonomics, high initial capital cost, and reduced operative space (such that only unit can be used at a time).21 Cumulatively, these shortcomings have led to the development of additional visualization modalities for tubular spine procedures.
Alternatives to Microscopes for Visualization
Although microscopes have traditionally been the gold standard means of operative visualization, tubular procedures performed through an OM have received criticism for difficult ergonomics, as mentioned earlier. Successful decompression of the neural structures using a microscope often requires extreme microscope positional angles, which force surgeons to adopt nonergonomic positions for extended periods of time.22 To align with the microscopic eyepiece, surgeons may adopt unnatural positions that make it nearly impossible for other operating room (OR) staff or trainees to properly assist in these situations. Loupes and headlights, other modes for surgical visualization, have also been associated with poor ergonomics, as these technologies increase the weight of the head and can increase the load on the cervical spine.23
A variety of novel technologies have been introduced to address the ergonomic deficiencies that are inherent to microscopic spine surgery. One of these is the exoscope, a visualization modality that is placed approximately 20 cm or farther above the operative field, thereby facilitating an unobstructed working space.24 A particular advantage of exoscope is that it can be seamlessly integrated with tubular spine procedures. In a nonspine context, the use of tubular retractors with exoscopes has been described for minimally invasive resection of intracranial lesions, including cavernous hemangiomas, meningiomas, gliomas, and pilocytic astrocystomas.25,26 In a spine-specific context, Ariffin et al described the use of exoscopes for tubular microdiscectomy and tubular decompression. The authors found that the exoscope had a short learning curve, and no cases required conversion to open surgery or change of exoscope to microscope due to poor visualization or image quality.22
More broadly, in a systematic review comparing the image quality of exoscope-assisted spine surgery to OM-assisted spine surgery, Iqbal found that the exoscope was consistently associated with improved image quality, illumination, and ergonomics,24 though not all studies were specific to tubular surgery. The exoscope has also been associated with notable disadvantages, however, including reduced stereopsis, bulky setup, and high capital costs which may exceed $400,000.27
Thanks to advancements in enabling technologies such as miniature digital cameras, novel drills, and real-time intraoperative navigation, the past decade has also been marked by an explosion in interest in endoscopic spine surgery.3 Advances in endoscopic cameras include improvements in resolution (the number of pixels contained in a display), color representation, and lighting.28 However, the endoscope has been shown to have an extremely steep learning curve, which may make it challenging for established surgeons to incorporate into their practice. Moreover, the literature has demonstrated mixed results regarding the efficacy of endoscopic surgery compared with tubular-based spine surgery.29 Due to the limitations of these technologies, a need has emerged for small cameras with improved depth of visualization, improved ergonomics, and little or no learning curve.
Emergence of TMDC
TMDCs represent the most recent example of camera-based technology for tubular retractors and dilators. As the name suggests, TMDC relies on the mounting of high-definition digital cameras on tubular retractors (Figure 2). Notably, the camera is not a part of an endoscope but is rather an independent device that can be mounted to the retractor. Cases of TMDC described in the literature have so far incorporated the Viseon MaxView System and have been utilized for a variety of spinal procedures, including cervical foraminotomy, minimally invasive lumbar decompression, TLIF, corpectomy, and thoracic discectomy.4,30–32

High-definition digital camera mounted to a tubular retractor (Viseon MaxView Posterior).
One notable advantage of TMDC is its ability to facilitate a seated operation which is ergonomically favorable for the surgeon. Although seated operations offer technical and anatomic advantages to surgeons (including easier retraction of soft tissues and improved visualization), these operations are ergonomically challenging when performed with microscopes.30 To reach the microscope, surgeons must extend their arms in front of them at shoulder height for the duration of the operation, which may lead to increasing fatigue. In a 2023 study, Boudreaux et al performed a posterior cervical foraminotomy using TMDC.30 A sterile digital camera was brought into the field to perform the foraminotomy (with the patient in a seated position) through the tubular retractor at C6 to C7 and C7 to T1 levels. Surgeon economics were independently scored intraoperatively through the Rapid Entire Body Assessment (REBA). The REBA scoring criterion identifies the ergonomic “risk” associated with specific body positions, with increasing scores indicating a need for change in body positioning. Interestingly, not only did the authors compare REBA scores of TMDC to microscopes, but these scores were also compared between surgeons of differing statures. When a microscope was placed, the “tall” surgeon and the “short” surgeon achieved similar REBA scores, placing them both in a “medium-risk” category. When the TMDC was introduced, however, the repeated REBA scores for both surgeons were 3, placing them in the “low-risk” category. The authors therefore demonstrated the potential of TMDC to greatly improve the ergonomics of seated spine surgery, especially for surgeons of shorter stature.30
In a separate study, Louie et al retrospectively compared operative times, ergonomics, and workflow between consecutive single-level minimally invasive lumbar decompression surgeries in a TMDC cohort and a matched, historic cohort of OM cases.4 Compared with the OM group, the TMDC cohort had significantly shorter operative times, while OR staff indicated improved safety, setup time, and workflow in surveys. In terms of complications, durotomy rates were similar between the 2 cohorts despite incidental durotomy being a criticism of MIS tubular spine procedures.4 Similar to the aforementioned Boudreaux study,30 Louie et al4 utilized the REBA system to score surgeon ergonomics during the initial laminotomy phase of consecutive cases of both TMDC and OM cohorts. The average REBA score was 3 (indicating “low risk”) using the TMDC, which was significantly lower than the average REBA score when using the microscope (4.1; “medium risk”).
TMDC has also been utilized for MIS-TLIF, as described in technical notes by Yun et al21 and by Leroy et al.32 As the latter authors explain, the digital camera allows improved visualization and an expanded field of view which was conveyed on multiple monitors. The camera was also able to rotate in every direction, thereby reducing the need for constant irrigation, and the surgeon in this case achieved an ergonomically favorable setup, with the monitor facing directly across from his visual field. The utility of TMDC may also extend beyond operative outcomes and ergonomics. In a case report,21 Yun et al describe the utility of TMDC for enabling a dual-surgeon workflow for performing a 2-level TLIF. As the authors write, this allows for a significant reduction in OR time compared with single-surgeon TLIFs, as well as a reduction in fluoroscopy time since only a single fluoroscopy exposure could be used to perform arthrodesis at both levels.
An additional benefit of TMDCs is their relative low cost compared with microscopes, which may cost hundreds of thousands of dollars. Indeed, OMs are not always available in resource-poor settings, especially in low- and middle-income countries. In these situations, portable cameras may be a much more practical and readily available solution for spine surgeons.33 Similarly, TMDCs are projected onto a large monitor and may therefore be feasibly presented to a large audience (including both trainees and OR staff), unlike an OM. This may facilitate improved teaching ability as well as a “team environment” in which everybody in the OR can see what is happening in the surgical field.
The Importance of Surgeon Ergonomics
As detailed by Louie et al,4 TMDCs enable ergonomic ability which exceeds that of microscopes. In the long term, this ergonomic improvement may prevent surgeons from experiencing debilitating disability. Two-thirds of spine surgeons in one study admitted to experiencing neck pain, with 17.5% taking sick leave due to debilitating neck pain.4,34 In a separate survey study, 31% of spine surgeons reported lumbar disc herniation, 28% reported cervical disc herniation, and 24% reported rotator cuff disease.35 TMDC has been proposed as an ergonomic solution to these musculoskeletal problems. Since TMDCs allow surgeons to maintain a neutral neck position when performing spine surgery, they may lessen the prevalence of these debilities.4 Moreover, in contrast to OMs and their associated angular limitations, TMDCs can be projected onto a fixed visual screen, which allows surgeons to maintain neutral positioning of their shoulders.4,30 This is relevant because shoulder pain has been reported in 24% to 49% of spine surgeons, with an increasing prevalence among surgeons performing endoscopic spinal procedures.23,36,37 Moreover, since ergonomics have been shown to influence the longevity of a surgeon’s career, this directly impacts patient care.4
The relationship between ergonomics and surgeon well-being is an understudied topic in the literature. Nonetheless, as more surgeons incorporate TMDC into their regular practice, such analysis will likely become more prevalent.
In addition to improving ergonomics, advanced visualization also has the potential to reduce the learning curve associated with the use of tubular retractors, which have historically been their biggest barrier to widespread implementation.33,38 The literature reports dozens of cases that must be performed in order to achieve reliable technical competence for tubular procedures, ranging up to 50 or more for MIS-TLIF, for instance.39 ,40 Thanks to TMDC’s enhanced visualization of the surgical field, however, there is potential to alleviate this learning curve.
Outcomes and Economics
Compared with open approaches, MIS tubular surgery has been shown to be associated with decreased hospital length of stay41–44 and operative times.41–43 Moreover, tubular procedures have also demonstrated potential for cost savings in comparison to their open counterparts. In the case of MIS-TLIF, for example, several studies have compared the costs and efficacy of MIS-TLIF in relation to open TLIF.45–47 One study found that MIS-TLIF was associated with reduced costs over 2 years while providing equivalent improvement in postoperative outcomes. Likewise, patients undergoing MIS-TLIF had shorter hospital lengths of stay, faster narcotic independence, as well as faster return-to-work rates.48 Likewise, Cahill et al demonstrated significantly lower costs for tubular microdiscectomy compared with open microdiscectomy.49 A separate randomized controlled trial comparing the cost-effectiveness of tubular discectomy to conventional microdiscectomy found no significant differences in quality-adjusted life years and costs.50
Scant literature exists comparing costs and outcomes of the various visualization modalities for tubular retractors, making it difficult to ascertain direct comparisons of cost-effectiveness. In a systematic review, Li et al compared outcomes between tubular discectomy using microscopes and conventional microdiscectomy.51 Ultimately, the authors found no significant differences between the 2 modalities in terms of operative times, complications, or long-term patient-reported outcomes.51 Cost, however, was not captured in this review study. In a separate study, Sarikonda et al found no differences in intraoperative costs between exoscope- and microscope-assisted anterior cervical discectomy and fusion, though tubular retractors were not used in these cases. Many studies have also compared the cost-effectiveness of endoscopic procedures to tubular procedures,52 though endoscopic surgery is a distinct category from camera-based tubular surgery.
Further research is warranted to identify the specific costs associated with microscope-assisted tubular surgery, especially in relation to other visualization modalities like exoscopes or TMDCs. Due to the novelty of TMDCs, no studies have been published studies assessing the cost-effectiveness of this technology. This is a gaping hole in the literature that requires further research going forward.
Conclusions
Advances in tubular spine surgery—whether in the form of microscope-based tubular retractors, exoscopes, or TMDC—have allowed for improvements in the visualization and ergonomic capacity of spine surgery. Further research is needed to quantify the true costs of these technologies, especially with regard to how they compare to each other. In the meantime, training programs may consider standardizing early education of tubular surgery and incorporating nascent digital camera technology, so that surgeons are equipped to perform these muscle-sparing techniques without fear of a daunting learning curve.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.