


Abstract
Background Anterior column realignment is an attractive minimally invasive treatment for sagittal imbalance. Expandable spacers offer controlled tensioning of the anterior longitudinal ligament (ALL) during release, which could optimize correction and anterior column stability. This study investigated the biomechanical and radiographic effects of single-level anterior-to-psoas lumbar interbody fusion (ATP-LIF) with expandable spacers and sequential ALL release.
Methods In vitro range of motion tests were performed on 7 fresh-frozen cadaveric spines (L2–L5) with a ±7.5 Nm load applied in flexion-extension (FE), lateral bending (LB), and axial rotation (AR). After testing intact spines, single-level (L3–L4) ATP-LIFs were performed and supplemented with posterior screws, rods, and integrated lateral screws and tested after (1) no ALL release (ATP-LIF); (2) resection of 1/3 the ALL’s width (1/3 ALL release); (3) resection of 2/3 the ALL’s width (2/3 ALL release); and (4) complete ALL resection (3/3 ALL release). Following each partial ALL release, rods were removed, and spacers were expanded until the torque limit was reached. Rods were then reapplied, and lateral radiographs were taken to analyze changes in intervertebral angle (IVA), foraminal height, foraminal area, and posterior and anterior disc height (PDH and ADH).
Results In ATP-LIF constructs, range of motion decreased in FE (18% intact), LB (14% intact), and AR (30% intact), while IVA, PDH, ADH, foraminal height, and foraminal area increased. PDH and ADH increased linearly with sequential ALL release and spacer expansion, while LB and AR remained stable. FE increased slightly (+15%–16% intact, <1°) following 2/3 ALL release but remained stable afterward. IVA increased exponentially with sequential ALL release, gaining 8.8° ± 3.2° with complete release.
Conclusions The present study found improved biomechanics and radiographic parameters following ATP-LIF with intact ALL, minimal biomechanical differences between partial and complete ALL release, and greater correction and height restoration with complete release. Future clinical testing is necessary to determine the impact of this finding on patient outcomes.
Clinical Relevance Controlled tensioning of the ALL before and after ligament release allows for potential optimization between restoring sagittal balance and maximizing construct stability in a minimally invasive approach.
Level of Evidence 5.
Introduction
Adult spinal deformities (ASD) requiring surgical correction are expected to increase in the United States as a result of the growing elderly demographic, increasing life expectancy, and rising patient expectations from their healthcare system.1–4 The prevalence of ASD in the United States is reported to lbe as high as 68% for patients older than 60 years.1,5 Correction of sagittal imbalance is of particular clinical interest in ASD patients because it is a common comorbidity and has a strong correlation to health-related quality of life measures.1,4,6–8 Sagittal imbalance is a condition characterized by a change in the natural curve of the spine. It can be caused by a variety of factors such as trauma, metabolic disease, previous surgery, and degenerative disc disease.3 Sagittal imbalance due to degenerative disc disease destabilizes the spine due to an anterior shift in the center of gravity that occurs as a result of a loss in lumbar lordosis. This can lead to increased stress at neighboring discs and detrimental compensatory mechanisms that work to restore sagittal balance.9–11 Such compensatory mechanisms include reduced thoracic kyphosis, lumber hyperextension, knee flexion, ankle extension, and muscle compensation. These cascades can ultimately lead to back pain, adjacent segment degeneration, additional deformities, and reduced patient functionality.7,9
Restoration of lumbar lordosis is a primary goal for correcting sagittal imbalance. This has been traditionally achieved using 3-column osteotomies supplemented with posterior pedicle fixation and/or interbody spacers.1,9 Three-column osteotomy techniques such as pedicle subtraction osteotomy (PSO) use an open approach to shorten the posterior column to restore lumbar lordosis.1,4,6,7 These procedures are capable of restoring lumbar lordosis up to 30°to 40°.7,12 While effective, 3-column osteotomies are invasive, carrying high risks of intra- and postoperative complications such as pain, nonunion, infection, vascular injury, dysesthesia, paresthesia, and significant blood loss.1,4,6,9 Previous studies have reported complication rates as high as 46% to 50% for primary and 70% for revision surgeries.1,4
Recently, anterior column realignment (ACR) has been proposed as a minimally invasive alternative to osteotomies such as PSO.2,8,13 ACR relieves tension on the anterior column by sacrificing the anterior longitudinal ligament (ALL), via anterior or transpsoas lateral access, to allow for the extension of the anterior column via lateral lumbar interbody fusion or anterior-to-psoas lumbar interbody fusion (ATP-LIF) to restore lumbar lordosis.1,4,6–9,13 Previous clinical and biomechanical studies have shown lower or similar instances of postoperative complications, as well as significantly decreased blood loss and improved radiographic parameters using ACR compared with 3-column osteotomies for sagittal imbalance.1,2,4,6,7,14 Greater lordosis correction (30°–40°)9,12 is achievable with single-level PSOs compared with single-level ACRs (10.6°–13.1°),15 which has prompted the use of combination techniques (ACR + posterior osteotomy).1,8,16 However, ACR could potentially achieve comparably high correction as PSO without the need for posterior osteotomies by treating multiple levels,9 thereby retaining the benefits of a less invasive lateral/anterior approach.7 Additionally, the more oblique ATP-LIF approach offers the added benefits of reducing the need for the neuromonitoring that is required to transverse the psoas in a lateral approach and provides access to the entire lumbar spine.17,18
The majority of previously published research has focused on ACR with static spacers, but wider adoption of expandable spacers presents opportunities for further improving patient outcomes. Static spacers are theoretically at greater risk of anterior instability, which can lead to spacer migration, nonunion, endplate fracture, and adjacent segment failure.7,9 Expandable spacers offer minimally invasive treatment for patients with ASD and have demonstrated improved disc and foraminal height (FH) restoration with favorable lordosis restoration in single- and multilevel fusions compared with their static counterparts.19 Compared with PSO, ACR with hyperlordotic expandable spacers has been reported to achieve comparable sagittal correction with significantly less blood loss and shorter hospitalizations.14 Expandable spacers also have the potential for more controlled tensioning of the ALL with expansion during sequential release, which could optimize lordosis restoration and anterior column stability; however, it is currently unknown how much of the ALL must be sacrificed to achieve maximal correction and how this influences biomechanics of the spine. Therefore, the aim of this cadaveric study was to investigate the biomechanical and radiographic effects of single-level ATP-LIF with expandable spacers and sequential ALL release.
Methods
Specimen Preparation
Seven fresh-frozen human cadaveric lumbar spine specimens (L2–L5) were used in this study, with a single operative level (L3–L4). The medical history of each donor was reviewed to exclude any specimens with previous spinal trauma, malignancy, deformity, or vertebral fractures that would otherwise unduly influence the outcomes of the tests. Anteroposterior (AP) and lateral radiographs were taken to evaluate the presence of any osseous pathology. Dual-energy x-ray absorptiometry scans were taken using a Lunar Prodigy Scanner 8743 (GE Medical Systems, Waukesha, WI, USA) and a water-bath protocol to assess bone mineral density (BMD; T-score).20 Specimens were thawed to room temperature (25°C) and carefully denuded, leaving only ligaments, bones, and intervertebral discs of the desired vertebral levels. Prior to testing, specimens were potted in a 1:1 mixture of Bondo Auto Body Filler (Bondo/MarHyde Corp., Atlanta, GA, USA) and fiberglass resin (Home Solutions All Purpose, Bondo/MarHyde Corp.). Specimens were potted at the L2 and L5 vertebrae, such that the L3 to L4 mid-disc plane was aligned horizontally in the coronal, sagittal, and transverse planes. Specimens were wrapped in surgical gauze and periodically sprayed with saline (0.9%) throughout testing to preserve viscoelastic properties.21 Prior to testing, all specimens were double-wrapped in plastic bags and stored at –20°C.
Surgical Constructs
A total of 5 constructs were used in this study: (1) Intact: intact specimens that served as controls; (2) ATP-LIF: ATP-LIF at L3 to L4 supplemental with posterior fixation (PF), integrated lateral fixation (LF), and intact ALL; (3) 1/3 ALL release: ATP-LIF, PF, LF, and partial (1/3) ALL release, leaving 2/3 of the ligament’s width intact; (4) 2/3 ALL release: ATP-LIF, PF, LF, and 2/3 ALL release, leaving 1/3 of the ligament’s width intact; (5) 3/3 ALL release: ATP-LIF, PF, LF, and complete ALL release.
ATP-LIF Procedure
Prior to pedicle screw insertion, the physiological range of motion (ROM) of each intact specimen was measured using a custom-built 6-degrees-of-freedom (6DOF) motion simulator. Pedicle screws (CREO, Globus Medical Inc., Audubon, PA, USA) were then placed bilaterally at L3 to L4 in each specimen using the Weinstein approach. Screws (6.5 mm diameter) were inserted until 60% to 75% of the vertebral body was occupied in the lateral view, and screw trajectory was verified via AP and lateral fluoroscopy.22
A single-level ATP-LIF was performed at L3 to L4 of each specimen beginning with a partial annulotomy to create a window in the anterolateral annulus for disc removal. A Cobb elevator was inserted through this window to release the contralateral annulus, leaving the posterior annulus intact. A discectomy was performed, and the appropriately sized expandable interbody spacer (ELSA-ATP, Globus Medical Inc.) was selected based on specimen anatomy. ATP-LIF spacers were inserted laterally with a 30° anterior-to-posterior offset, aimed at the midline of the L3 to L4 disc space, and oriented with the longitudinal axis 90° from the sagittal plane. Spacers were expanded to fill the disc space and tension the ALL until the torque limit of the spacer was reached. Caution was taken during this step to ensure that the implant was not over expanded to the point of ALL damage. Integrated screws (5.5 × 30 mm) were then inserted and oriented laterally at the same 30° anterior-to-posterior offset to provide supplemental LF.
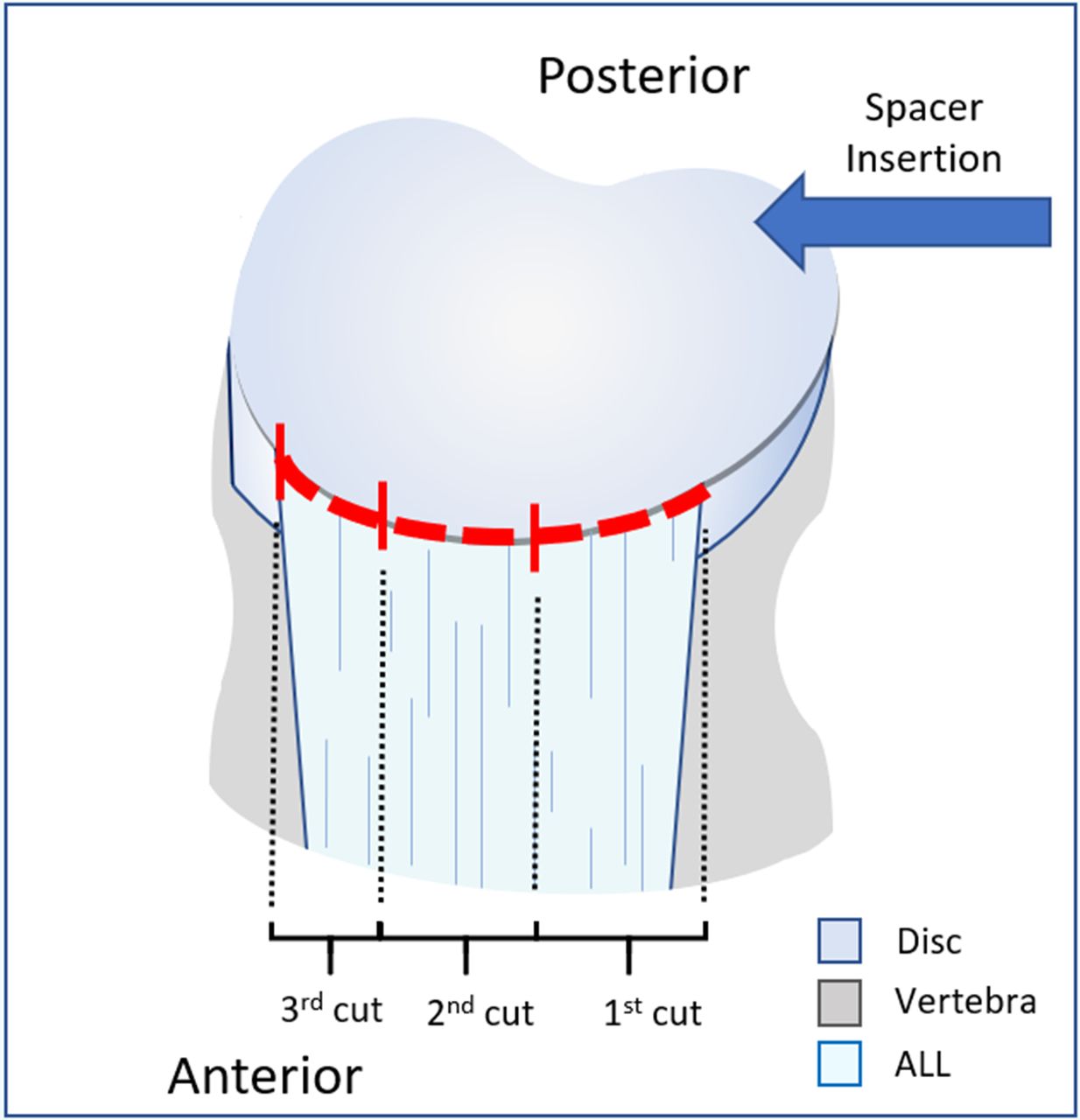
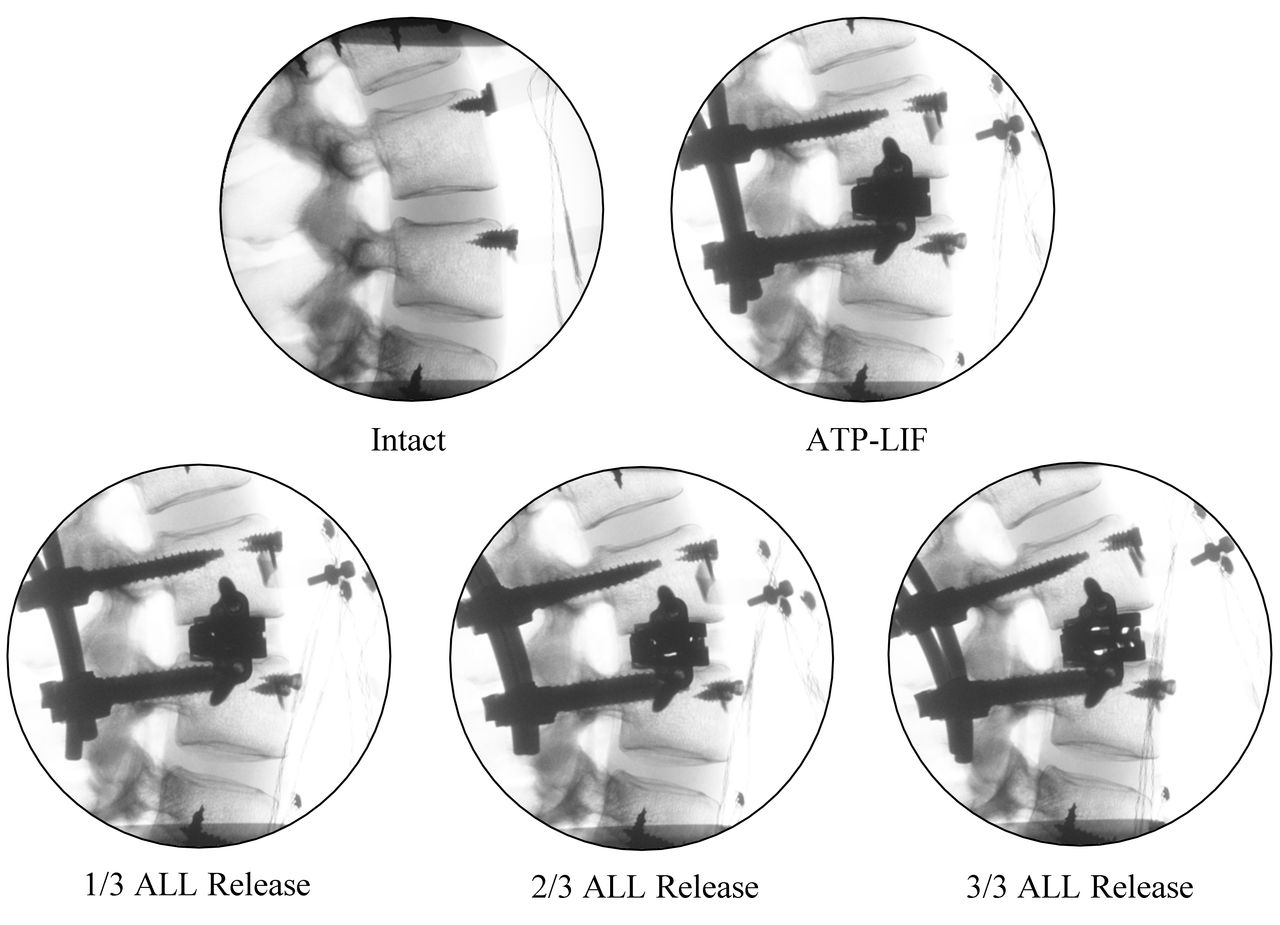
Spacer placement was confirmed with AP and lateral fluoroscopy utilizing anatomical markers from the preprocedure fluoroscopy shots. Ti6AL4V (TAV) rods (5.5 mm diameter) were inserted into the tulips of the pedicle screws and secured with locking caps to create the ATP-LIF construct. After testing, rods were removed, and sequential ALL release was performed using a scalpel to release the ligament, starting on the side of spacer insertion, in an ipsilateral-to-contralateral fashion (Figure 1).7 For each partial release, 1/3 of the total width of the ALL and anterior annulus was severed (Figure 1), and the spacer was further expanded until the torque limit was reached or damage to the ALL was observed. Rods were reinserted before ROM, and radiographs were taken. This process was repeated to create ATP-LIF constructs with 1/3, 2/3, and complete ALL release (Figure 2).

Diagram of L4 vertebra with inferior half of L3 to L4 disc. The dashed red line indicates the trajectory of the cut to completely release the anterior longitudinal ligament (ALL). The rightmost red hash perpendicular to the trajectory indicates the first cut, resecting 1/3 of the width of the ALL (1/3 ALL release). The middle red hash indicates the second cut, resecting another 1/3 of the width of the ALL (2/3 ALL release). The left hash indicates the starting point for the cut to achieve complete ALL release (3/3 ALL release).

Representative anterior-to-psoas lumbar interbody fusion (ATP-LIF) constructs with sequential anterior longitudinal ligament (ALL) release.
Multidirectional Testing
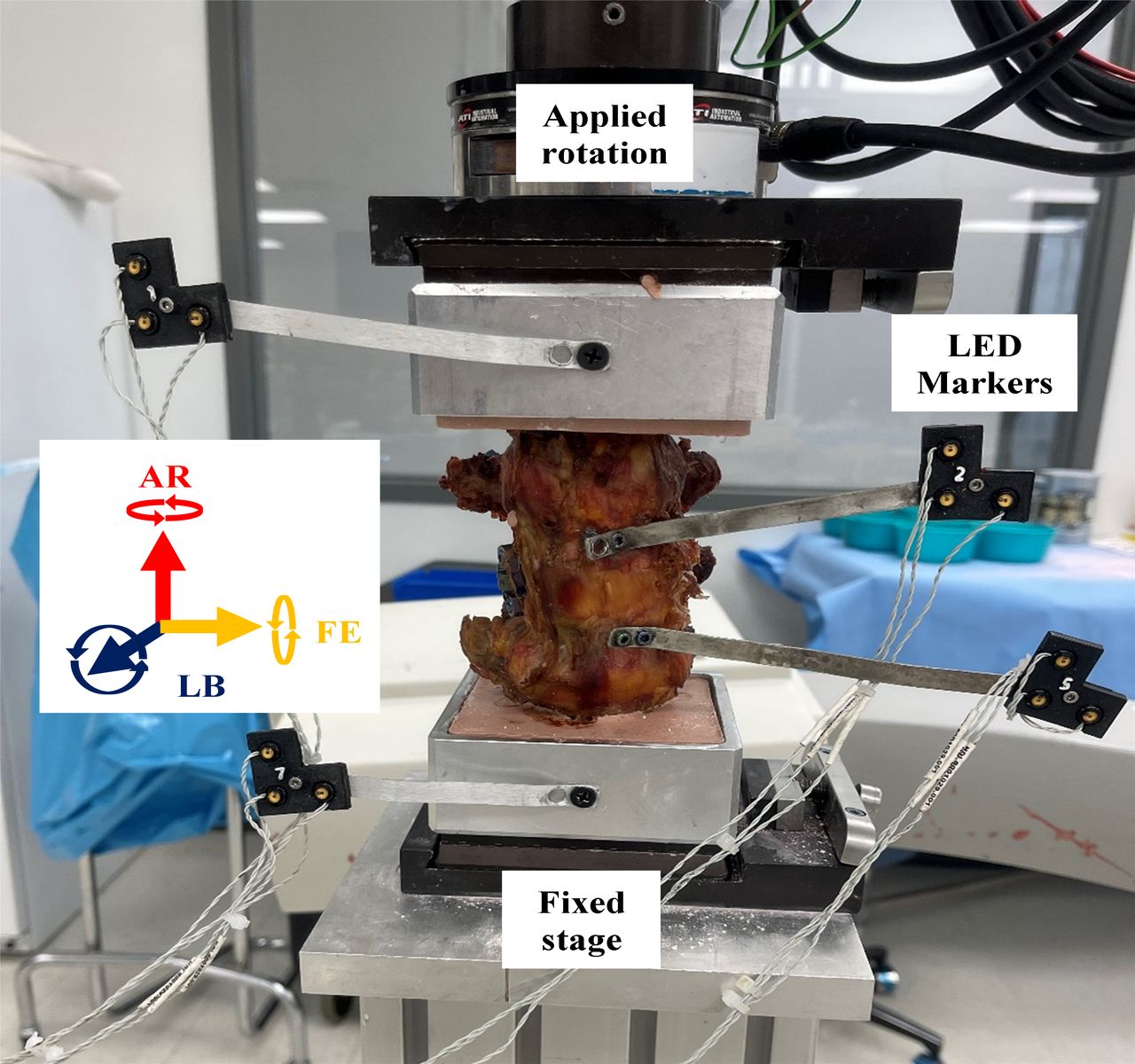
ROM was measured using a custom-built 6DOF motion simulator and commercial motion analysis software (Optotrak Certus Northern Digital Inc., Waterloo, Canada). Proximal and distal portions of the specimen were mounted to the 6DOF motion simulator (Figure 3). This system is supported by near frictionless air bearings and uses 3 orthogonal, cephalad servomotors to apply unconstrained, pure moments in all 3 physiological rotation axes; flexion-extension (FE), lateral bending (LB), and axial rotation (AR). Using these servomotors, a load control protocol was used to apply a pure moment of ±7.5 Nm at a velocity of 1.5°/s. Three loading and unloading cycles were performed for each rotation axes per test. The first 2 cycles preloaded the specimen to account for tissue viscoelasticity, while the data from the third cycle was analyzed.21 Motion was tracked with 4 plexiglass markers, each containing 3 light-emitting diodes, secured rigidly to L2 to L5. Data were collected through the Optotrak Certus motion capture system, which superimposes a system of coordinates onto each rigid body to determine relative Eulerian rotations of the vertebral bodies in all 3 rotational axes. Raw ROM at the operative level (L3–L4) was analyzed for statistical comparisons.

L2 to L5 specimen on the 6-degrees-of-freedom motion simulator. Applied bending movements are indicated as flexion-extension (FE), lateral bending (LB), and axial rotation (AR).
Radiographic Evaluation
Radiographic parameters were evaluated in the lateral view by 2 independent observers. Lateral radiographs of each construct were analyzed using ImageJ (ImageJ, U.S. National Institutes of Health, Bethesda, Maryland, USA) with measurements of only the operative level (L3–L4). The parameters of interest included intervertebral angle (IVA), anterior disc height (ADH), posterior disc height (PDH), and FH. IVA was defined as the angle between the flat endplates of the operative level (L3–L4). ADH and PDH were defined as the distance between endplates of the L3 to L4 disc at their most anterior and posterior points, respectively. FH was defined as the distance between the vertically oriented concavities of the intervertebral foramen, while foraminal area (FA) was defined as the area of the foramen devoid of bone.1,7,9,23
Statistical Methods
Statistical analysis was performed using SPSS Statistics (version 22, IBM Corp., Armonk, NY, USA). A 1-way analysis of variance test with repeated measures was used to assess the main effects of sequential ALL release on biomechanics and radiographic parameters. Significant main effects were followed up with Bonferroni post-hoc analysis, and significance was defined as P < 0.05. For the radiographic parameters, interobserver agreement was evaluated via intraclass correlation coefficients. Additionally, the mean differences between interobserver measurements were calculated and used to quantify absolute agreement. Regression analysis was also performed to evaluate trends in average values in response to constructs with and without sequential ALL release as well as spacer expansion.
Results
Specimen demographics, BMD, and spacer angle (°) are presented in Table 1.
Demographics, donor information, and spacer sizes of specimens.
Spacer Expansion
For each construct, the cumulative spacer expansion was calculated. Sequential ALL release had a significant effect on spacer expansion (P < 0.001). Expanded spacer height increased significantly following 1/3 ALL resection (P = 0.007) compared with ATP-LIF, then proceeded to further increase following 2/3 ALL resection (P = 0.029) compared with 1/3 ALL release. Spacer height also increased from 2/3 to 3/3 ALL resection; however, this was not statistically significant (P = 0.068). This resulted in a linear trend between average spacer height and sequential ALL release (R 2 > 0.99, P = 0.001) with each partial resection resulting in a 1.1 mm increase in spacer height (Table S1).
Range of Motion
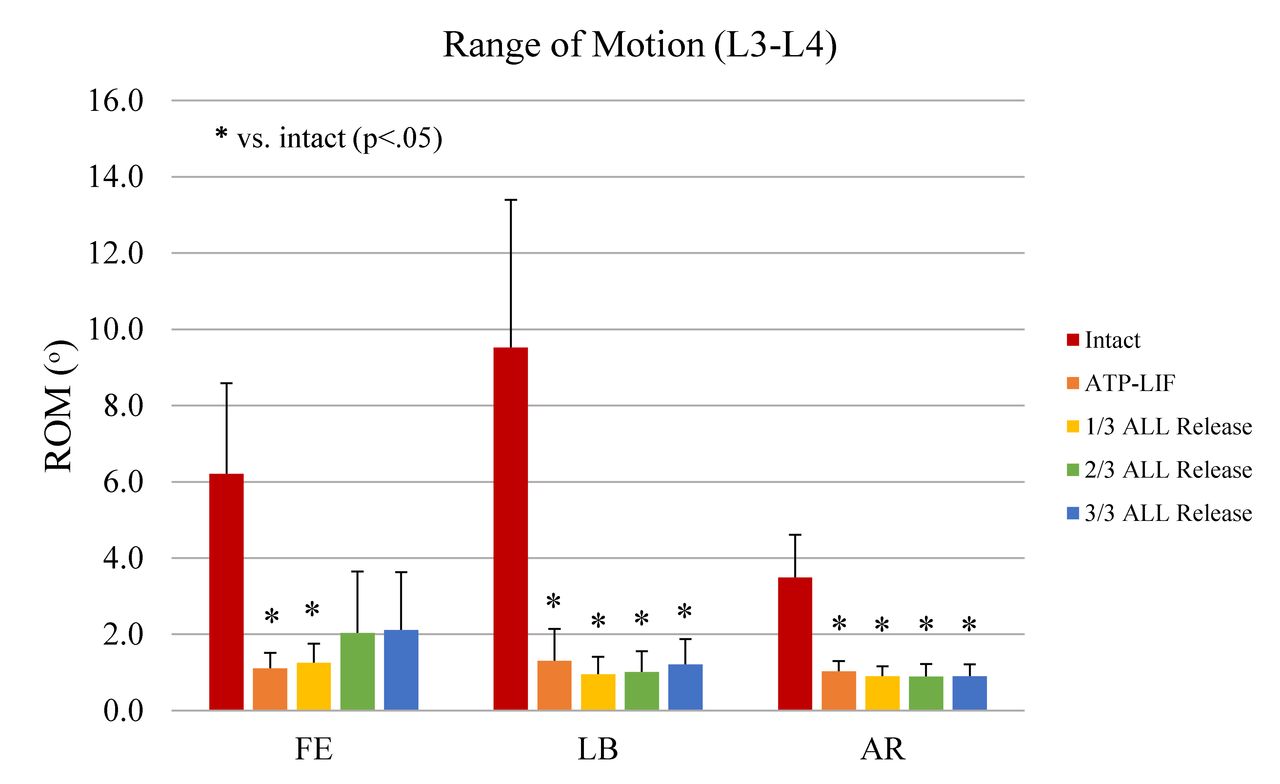
Raw ROM was used for statistical comparisons (Tables 2 and S2). Constructs were found to have a significant effect (P = 0.002) on ROM. ROM decreased significantly following ATP-LIF in FE (18% intact, P = 0.017), LB (14% intact, P = 0.016), and AR (30% intact, P = 0.005; Figure 4 & Table S2).
ROM following sequential ALL release.

Range of motion (ROM) at L3 to L4 in flexion-extension (FE), lateral bending (LB), and axial rotation (AR) following sequential anterior longitudinal ligament (ALL) release. * P < 0.05 vs intact.
Motion did not increase in LB and AR following sequential ALL resection. Instead, LB and AR motion remained stable at 10% to 14% intact and 26% to 30% intact, respectively, in constructs with intact ALL, partial ALL release, and complete ALL release.
Motion also did not increase in FE following 1/3 ALL release (20% intact) but did increase (<1°) following 2/3 ALL release (33% intact). However, this was not significant compared with ATP-LIF (P > 0.999) or 1/3 ALL release (P > 0.999). FE motion then remained stable between 2/3 ALL release and 3/3 ALL release (34% intact), and both constructs still had substantially less motion than Intact.
Radiographic Parameters
Angles (IVA), heights (ADH, PDH, and FH), and areas (FA) at L3 to L4 were measured by 2 independent observers. Intraclass correlation coefficient values were calculated as measures of interobserver agreement. The absolute agreement was moderate-to-excellent between observers, ranging from 0.67 to 0.98, and consistency was high-to-excellent, ranging from 0.77 to 0.97, indicating agreement of exact measurement values and highly consistent changes in each parameter following spacer insertion, expansion, and sequential ALL release. Additionally, there were low mean differences between observer measurements (IVA: 1.0° ± 0.8°; ADH: 1.1 ± 1.2 mm; PDH: 0.6 ± 0.6 mm; FH: 1.5 ± 1.1 mm; FA: 25.0 ± 21.9 mm2). These results indicate good interobserver consistency with negligible differences in absolute values (Table S3).24 Radiographic parameters were averaged between observers for statistical comparisons (Table S4).
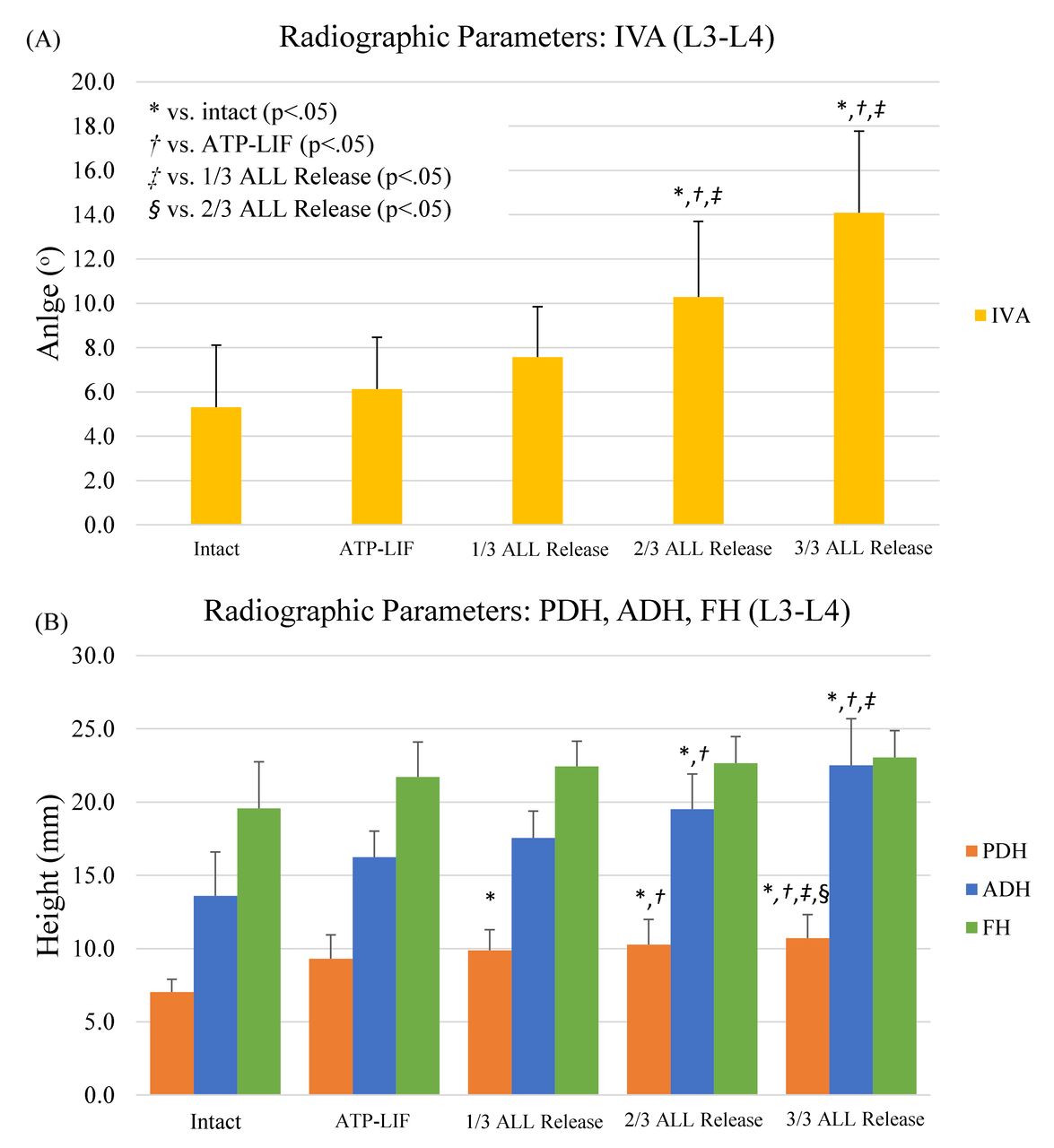
ATP-LIF with sequential ALL release had a significant effect on IVA (P < 0.001), PDH (P < 0.001), ADH (P < 0.001), and FH (P = 0.005), but not FA (P = 0.064). On average, IVA increased exponentially with spacer expansion (R 2 = 0.99, P = 0.007) and sequential ALL release (R 2 = 0.98, P = 0.001), as shown in Figure 5a and Table S1. On average, IVA increased with each procedural step, gaining 0.8° following spacer insertion with intact ALL (P = 0.141 vs intact), 1.5° following 1/3 ALL release (P = 0.291 vs ATP-LIF), 2.7° following 2/3 ALL release (P = 0.033 vs 1/3 ALL release), and 3.8° following complete ALL release (P = 0.092 vs 2/3 ALL release). This resulted in a total of 8.8° correction that was achievable primarily due to ALL release (P = 0.001 vs ATP-LIF). ADH and PDH also increased linearly with spacer expansion (R 2 = 0.98–0.99, P < 0.05) and sequential ALL release (R 2 = 0.83–0.98, P < 0.05; Table S1), gaining an average of 2.1 and 0.5 mm per partial ALL release, respectively (Figure 5b and Table 3). FH and FA both had a sharp initial gain of 2.1 mm and 17.3 mm2, respectively, following spacer insertion that then plateaued despite sequential ALL release.

Radiographic trends of (A) intervertebral angle (IVA) and (B) intradiscal heights (posterior disc height [PDH], anterior disc height [ADH], and foraminal height [FH]) following sequential anterior longitudinal ligament (ALL) release. *P < 0.05 vs intact. †P < 0.05 vs anterior-to-psoas lumbar interbody fusion (ATP-LIF). ‡P < 0.05 vs 1/3 ALL release. §P < 0.05 vs 2/3 ALL release.
Radiographic parameters following sequential ALL release (mean ± SD).
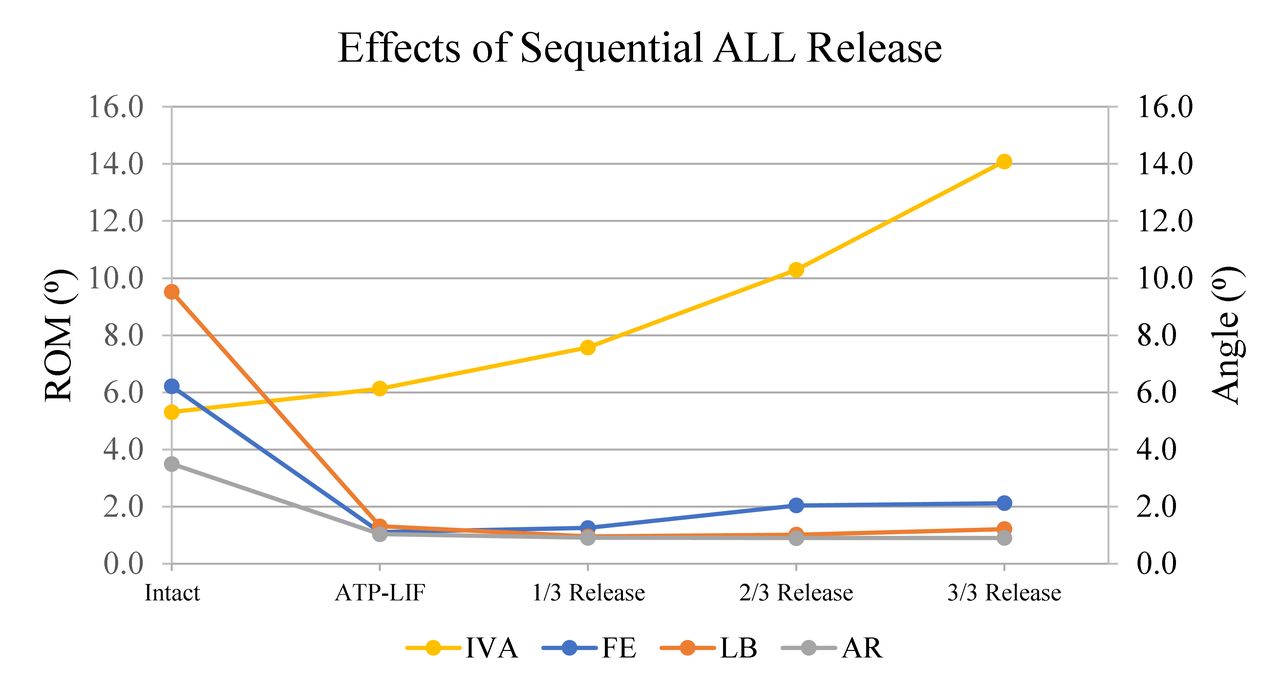
Radiographic and ROM trends were analyzed between constructs to investigate the interaction of sagittal alignment and biomechanics of the lumbar spine following sequential ALL release (Figure 6). As expected, spacer insertion and supplemental fixation resulted in decreased ROM in all directions (14%–30% intact). Interestingly, there appears to be an inflection point at 2/3 ALL release, where a large increase in IVA (2.7°) was accompanied by a small increase in FE motion (+15% intact, <1°), while LB and AR motion remained stable (Figure 6). From 2/3 to 3/3 ALL release IVA increased even more (3.8°), while FE motion was stable (33% vs 34% intact).

Average range of motion (ROM; flexion-extension [FE], lateral bending [LB], and axial rotation [AR]) and intervertebral angle (IVA) following sequential anterior longitudinal ligament (ALL) release.
Discussion
The restoration of sagittal balance is recognized as a primary goal of ASD surgery with clinical benefits to patients;1,25,26 however, corrections greater than 30° can be challenging.7 PSOs have been shown capable of achieving up to 40° of correction but at the cost of high complication rates.1,4,6,9,12,27 ACR has gained popularity as a minimally invasive alternative to PSO for sagittal imbalance caused by lumbar disc degeneration. Traditionally, PSOs offer greater correction at the expense of higher blood loss compared with ACR with static hyperlordotic spacers.4 Expandable spacers present an opportunity to further improve patient outcomes through shorter hospitalizations and comparable corrections to PSOs14 as well as the possibility to optimize lordosis and anterior column stability via controlled expansion and sequential ALL release. Therefore, this study investigated the biomechanics and radiographic parameters of single-level ATP-LIF constructs with expandable spacers following sequential ALL release.
The present study found a linear relationship between spacer expansion and sequential ALL release, with spacers gaining an average of 1.1 mm in height per every 1/3 of the ALL that was released. This led to linear trends in ADH (2.1 mm/each partial release) and PDH (0.5 mm/each partial release). Meanwhile IVA increased exponentially with sequential ALL release and spacer expansion, gaining a total of 8.8° correction with complete ALL release. These findings were in line with previous studies.15,28,29
Following spacer insertion with supplemental fixation, ROM dropped in all bending moments (FE: 18% intact; LB: 14% intact; AR: 30% intact) with LB and AR remaining stable after sequential ALL release. Meanwhile, FE increased following 2/3 ALL release (33% intact) but remained stable between 2/3 and complete ALL release. The loss in stability between 1/3 and 2/3 ALL release was expected due to the role of the ALL as a tension band to resist hyperextension.2 The largest increase in correction occurred between 2/3 and 3/3 ALL release (3.8°) and resulted in only a slight change in stability during FE (+1°) compared with ATP-LIF with intact ALL. This was particularly interesting because ACR is often considered to be a more destabilizing procedure than other biomechanical studies.2,7,9 The authors attributed this stability to the use of posterior fixation, integrated LF, and expandable spacers.2,9,13,30 FH and FA also increased following spacer insertion, but unlike other alignment parameters, these had a small response to sequential ALL release, possibly due to the already large foraminal space of the intact specimens. The authors hypothesize that different trends could potentially be observed in cases of foraminal stenosis.
The ability to customize lordosis and other radiographic parameters in a minimally invasive technique such as ACR is an attractive alternative to many surgeons who seek to avoid more invasive osteotomies. In this study, less correction was achieved with partial ALL release with no significant changes in stability, but near-complete-to-complete ALL release achieved greater correction and disc height restoration with only a slight increase in FE. While this amount of segmental correction is lower than what is achievable with a PSO, this procedure can be augmented with combination approaches like the Ponte osteotomy, hyperlordotic spacers, and multiple spacers at adjacent levels.7–9 These findings provide insight into the trade-offs between stability and sagittal correction that can help surgeons weigh the benefits between partial and complete ALL release in ACR. Furthermore, these findings demonstrate the potential of expandable spacers as tools to achieve more controlled correction and height restoration with ALL release.
Limitations
While this study provides useful biomechanical and radiographic insight into the effects of sequential ALL release in ACR, there are a number of limitations. This was a biomechanical study performed in a controlled environment that may not be directly applicable to those in clinical settings, which must consider factors such as patient age, comorbidities, prior surgery, and BMD. Additionally, this study focused on sequential ALL release in single-level ATP-LIF constructs, so these interpretations are not necessarily applicable to multilevel constructs. This study also did not investigate the effects of hyperlordotic spacers (20°–30°) and instead used expandable spacers with less extreme profiles (6°–10°) due to the anatomical constraints of specimens, which could have limited the amount of correction achieved. Finally, fatigue testing, spacer migration, and load distribution were also not investigated because these were outside the scope of this study but should be explored in future studies.
Conclusions
The restoration of lumbar lordosis remains a primary goal for the treatment of sagittal imbalance. ACR has become an attractive minimally invasive alternative to PSOs for the treatment of sagittal imbalance; however, it is currently unknown how much of the ALL must be sacrificed to achieve maximal correction and how this influences spinal biomechanics. In this cadaveric study, improvements in biomechanics and sagittal alignment were observed in ATP-LIF constructs with intact ALL and posterior elements. There were minimal changes in the biomechanics between constructs with partial and complete ALL release, but those with complete ALL achieved greater correction and disc height restoration. Expandable spacers allow the decision between partial or complete ALL release to be left to the discretion of the surgeon via controlled implant expansion. Future clinical testing is necessary to determine the impact of these findings on patient outcomes.
Supplementary material
TABLE S1.
TABLE S2.
TABLE S3.
TABLE S4.
Footnotes
Funding Funding and materials for this study were provided by Globus Medical, Inc. Globus also paid the journal's article processing charge for the publication of this article.
Declaration of Conflicting Interests J.P.H. receives consulting fees from Globus Medical and received support for travel for this study. J.P.M., J.M.M., and B.S.B. are paid employees of and also receive stock options from Globus Medical. J.W. was a full-time co-op at the time of this study from Drexel University and was paid by Globus Medical for this role.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.