


ABSTRACT
Background: Anterior lumbar interbody fusion (ALIF) has been well established as an effective surgical intervention for chronic back pain due to osteoporotic vertebral collapse. Historically, ALIF has consisted of an anterior approach to disc height restoration with a subsequent posterior pedicle screw fixation. Although the applications of cement augmentation with posterior fixation have been previously reported, treatment of patients with both isthmic spondylolisthesis and decreased bone mineral density using a stand-alone ALIF is controversial because of concerns for decreased fusion rates and increased subsidence risk, respectively. We report a case of stand-alone ALIF used to treat a low-grade isthmic spondylolisthesis in the setting of idiopathic thoraco-lumbar scoliosis in a patient with secondary degenerative changes and discuss the benefits of this surgical technique in a patient with several comorbidities.
Methods: An osteopenic 66-year-old woman with multiple medical comorbidities and 2 years of left radicular leg pain was found to have a Myerding grade I isthmic spondylolisthesis in the setting of idiopathic thoraco-lumbar scoliosis with secondary changes. The patient underwent an L5-S1 stand-alone ALIF with anterior cement augmentation without posterior pedicle screw fixation.
Results: The patient experienced immediate relief of radicular leg pain postoperatively and had an uneventful course. At 2 years follow-up, she remained symptom free, and radiographs showed excellent fusion and maintenance of intervertebral disc height.
Conclusions: The use of stand-alone ALIF with anterior cement augmentation of the vertebral bodies is a surgical technique that could produce excellent improvement in patients with low-grade isthmic spondylolisthesis in the setting of osteopenia. The use of the all-anterior approach in similar patients with multiple medical comorbidities can also be a useful technique, as it decreases associated morbidity of surgery and complication risks associated with prolonged operative times.
- anterior lumbar interbody fusion
- osteopenia
- osteoporosis
- anterior cement augmentation
- isthmic spondylolisthesis
INTRODUCTION
Isthmic spondylolisthesis is the result of a defect in the pars interarticularis that leads to the forward slippage of a vertebra, causing foraminal compression of nerve roots. Many surgical options exist to correct spinal pathology, including anterior lumbar interbody fusion (ALIF), posterior lumbar interbody fusion, transforaminal lumbar interbody fusion, posterolateral fusion, and circumferential fixation, with numerous case-specific factors affecting the surgeon's preferred approach.1 Among the available techniques, however, there remains no consensus for optimal surgical management.2,3 Compared with other fixation techniques, ALIF provides improved access to the anterior spinal column, allowing for better sagittal and coronal correction of the index segment deformity. This procedure relies upon restoration of disc height to provide for direct and indirect decompression of the neural elements.4 It also allows for increased surface area for fusion that in general results in less implant subsidence, provided there is adequate disc removal, endplate preparation, and removal of the posterior longitudinal ligament to allow for distraction.
Osteoporosis is a common disorder caused by a perturbation in the regulatory mechanisms that govern cellular bone formation and resorption. The end result is the creation of bone that has less structural support and is comparatively weaker than non-osteoporotic bone.5 For this reason, use of stand-alone anterior spinal fusion procedures in patients with severe osteoporosis remains controversial because of increased risk of endplate or vertebral body fracture. Augments such as polymethyl methacrylate (PMMA), colloquially known as bone cement, act as a mechanical interlock between the irregular bone surface and the implant, thereby improving strength of the construct and reducing the incidence of subsidence.6 Prior studies have described ALIF with cement augmentation and supplemental posterior fixation for these osteoporotic patients, but the two-site approach when using traditional techniques to place posterior instrumentation has been associated with longer operative time, increased blood loss, and increased complication rates.7–9 Specifically with percutaneous pedicle screw placement, there is greater radiation exposure and violation of cranial facet joints, which can lead to altered biomechanics at the adjacent level.10 Other studies have shown pseudoarthrosis rates from 0% to 49% in ALIFs without supplemental posterior fixation.11,12 If sufficient fixation can be provided by a single surgery, then the additional risks associated with combined anterior and posterior approaches can be avoided.13 In this report, we describe an L5-S1 ALIF with anterior cement augmentation without supplemental posterior fixation in an osteopenic patient for Myerding grade I isthmic spondylolisthesis in the setting of thoraco-lumbar scoliosis with secondary degenerative changes.
CASE REPORT
History, Physical Exam, and Diagnostic Workup
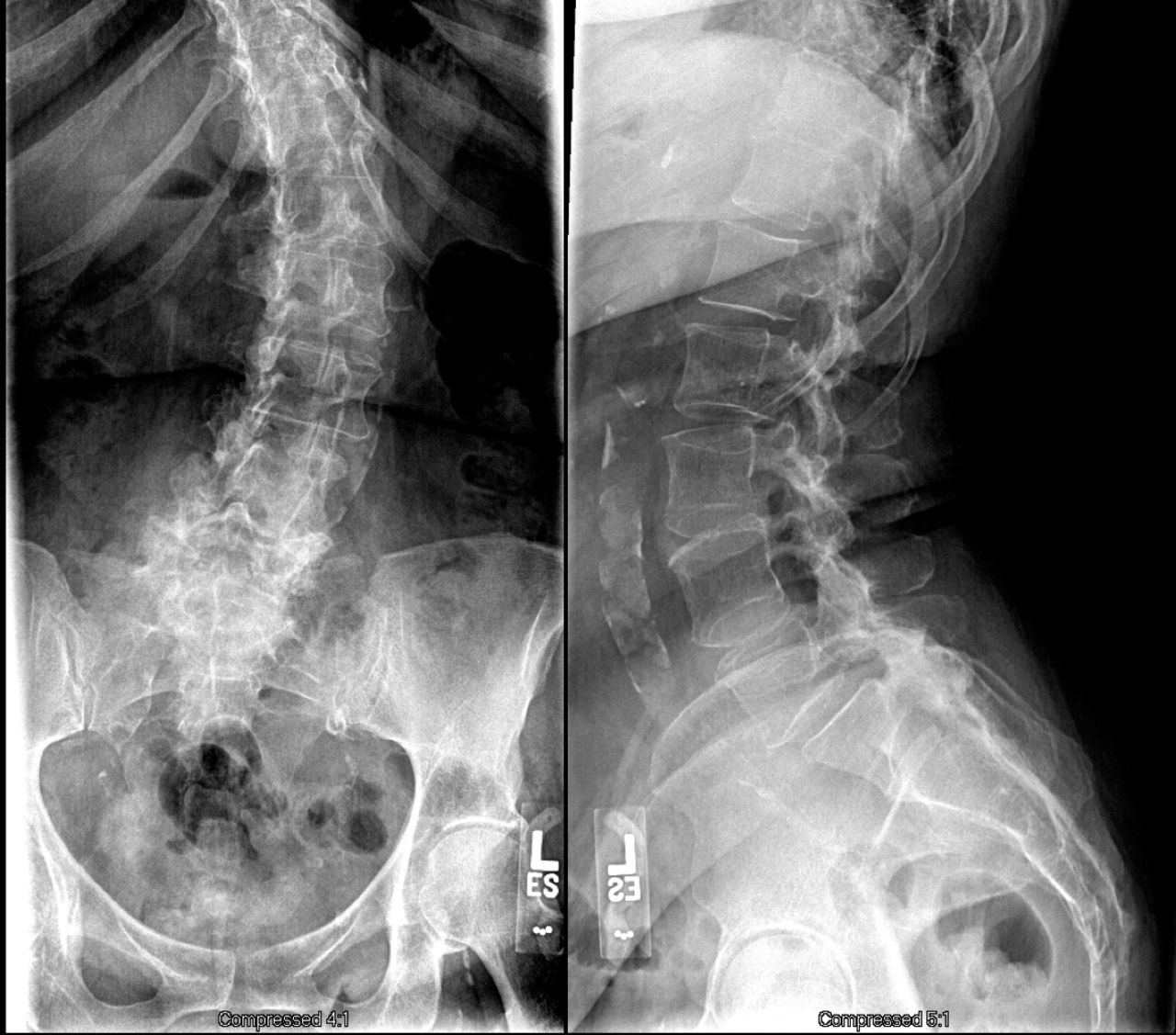
A 66-year-old woman with chronic persistent left leg radicular pain resistant to conservative treatment presented in June 2013. Neurological examination findings were unremarkable; the patient had full sensation and strength in the lower extremity. She required use of a significant amount of narcotics to control her pain. Plain radiographs and magnetic resonance imaging showed a 41° left lumbar scoliosis curve with a grade I L5-S1 anterolisthesis with bilateral pars defects (Figure 1). Imaging also showed lumbosacral spondylosis most severe at L5-S1, including advanced facet arthropathy, and disc osteophyte complexes resulting in foraminal stenosis and impingement of the left L5 and S1 nerve roots. The dual-energy x-ray absorptiometry scan showed osteopenia with a T-score of −2.1. The use of posterior instrumentation was deemed undesirable because of her attendant scoliosis and lateral listhesis at L4-5.
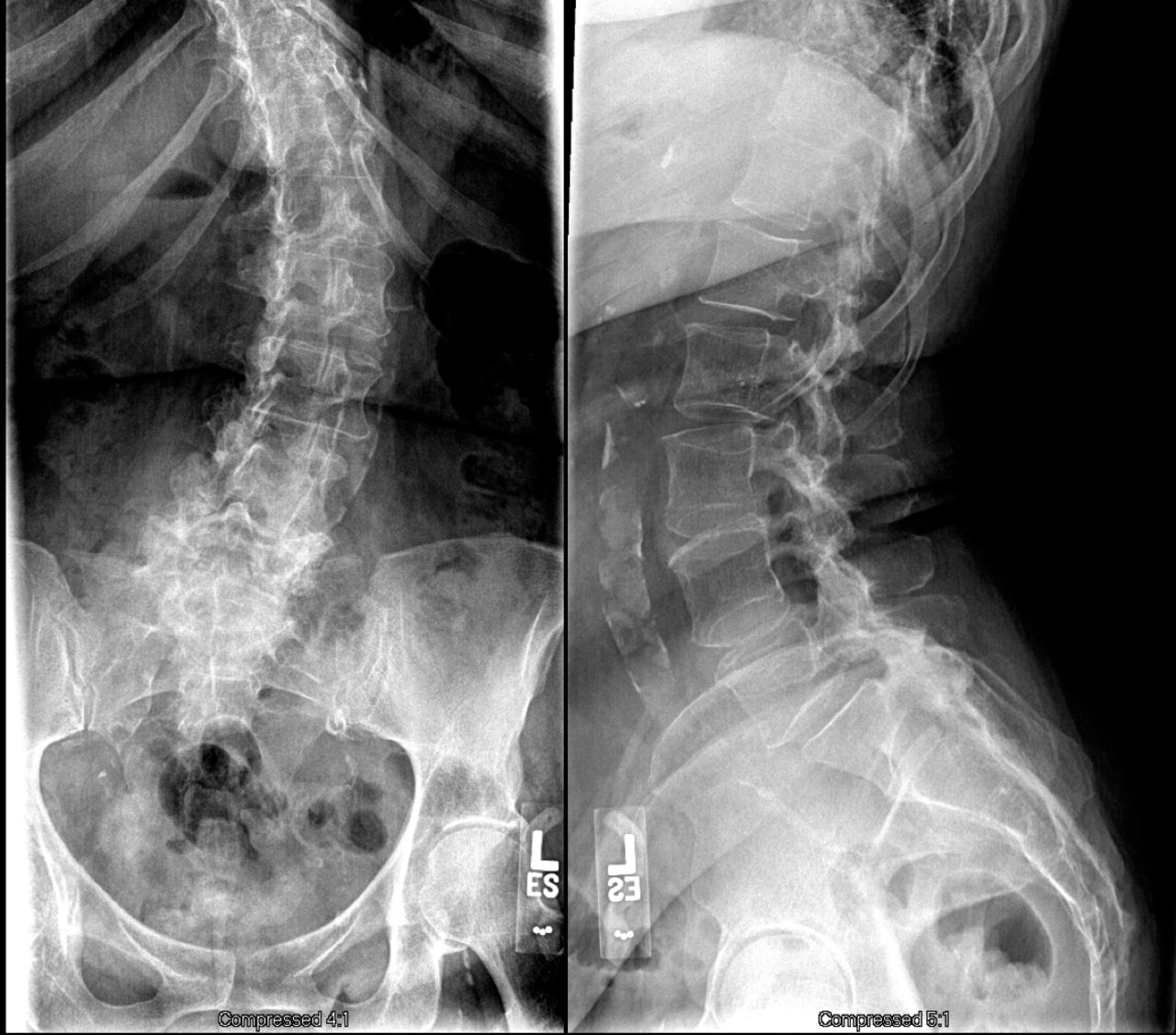
Preoperative anterior posterior (left) and lateral (right) lumbar radiographs showing spondylosis, lumbar scoliosis curve, and a grade I L5-S1 anterolisthesis.
Technique for ALIF With Anterior Cement Augmentation Without Supplemental Posterior Fixation
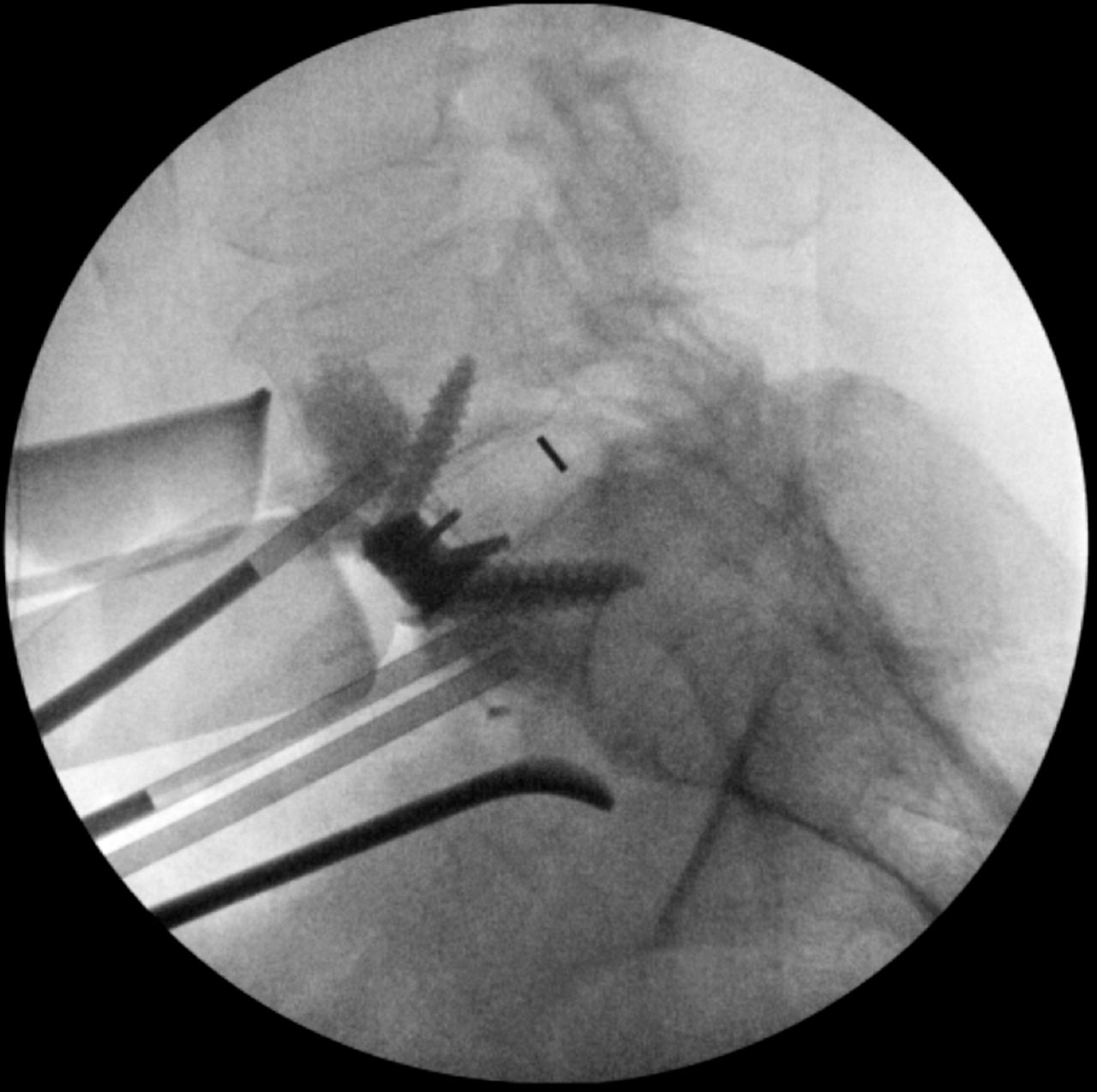
An anterior, paramedian, left-sided, retroperitoneal approach localized over L5-S1was performed. C-arm fluoroscopy was used to localize the L5-S1 level. An L5-S1 total discectomy was performed with removal of the cartilaginous endplates and posterior annulus. A medium-footprint 13-mm, 15° interbody cage (Globus, Aubudon, Pennsylvania) packed with recombinant human bone morphogenic protein-2 (Medtronic, Minneapolis, Minnesota) and collagen/ceramic strip (Globus, Aubudon, Pennsylvania) was tapped into the disc space with interference fit observed. Integral fixation of the interbody cage was achieved with 25-mm screws caudal and cephalad. Vertebroplasty was then performed by placing 2 cannulas 10 mm deep into S1 and 1 cannula into L5. Three milliliters of PMMA was injected into both the S1 and L5 vertebral bodies with the use of neuromonitoring and C-arm fluoroscopy throughout. Final confirmation under C-arm flouroscopy (Figure 2) showed appropriate placement of PMMA. A standard wound closure was performed.
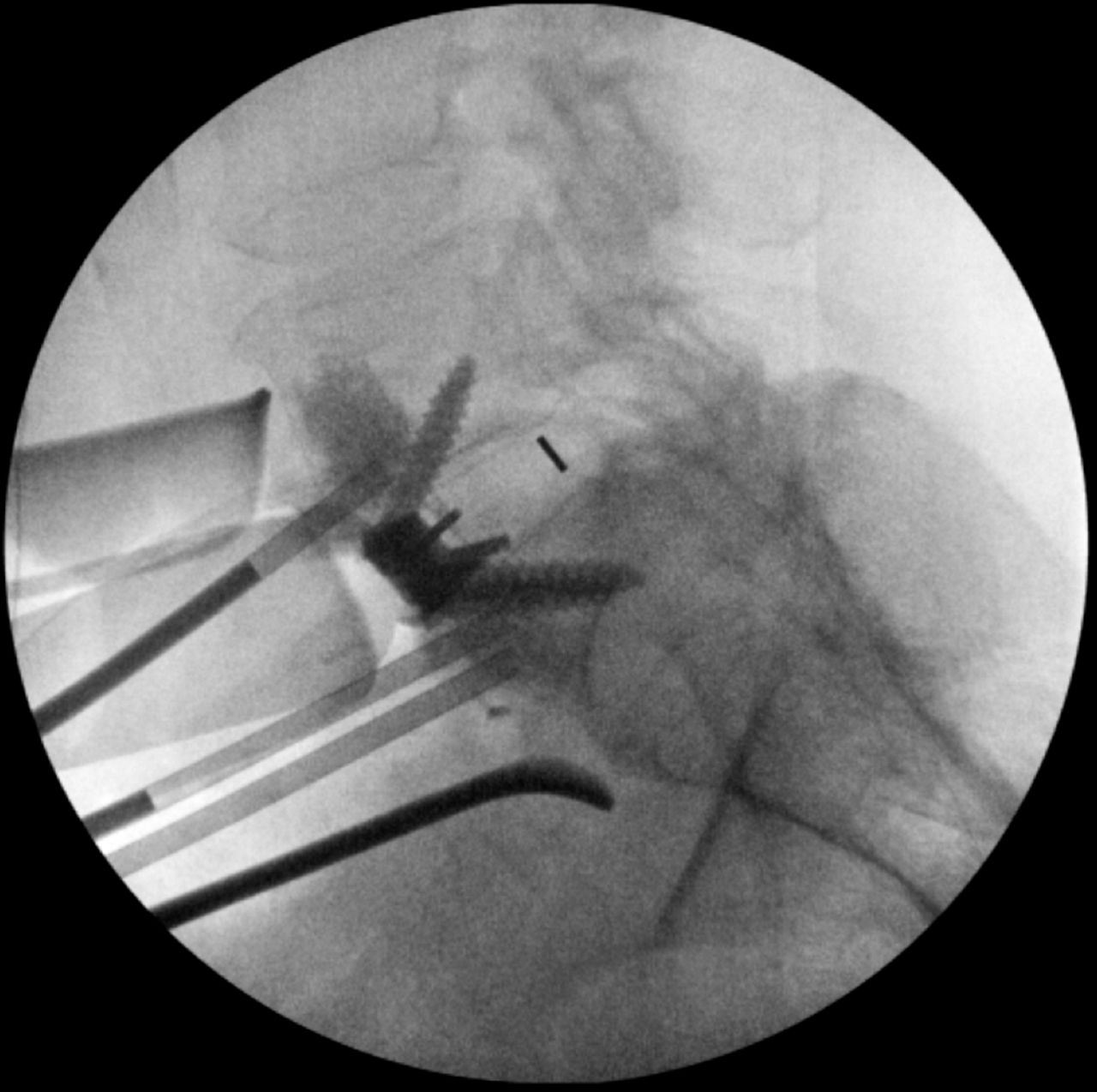
Intraoperative final C-arm fluoroscopy image with cannulas in place after polymethyl methacrylate augmentation of L5 and S1 vertebral bodies.
Postoperative Course
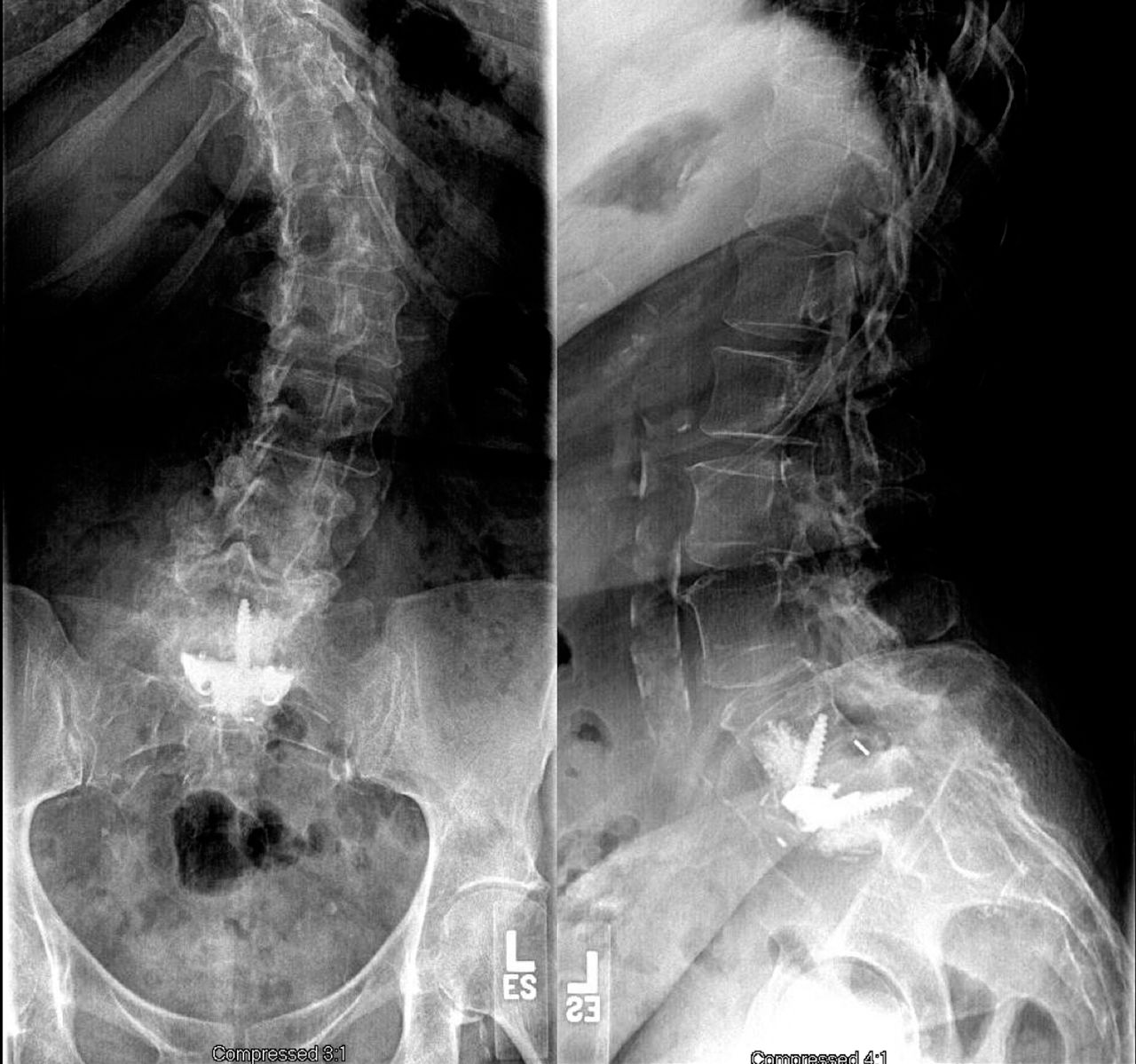
Postoperative day 1, the patient experienced immediate relief of preoperative left leg radicular pain and was completely neurologically intact. She was discharged home on postoperative day 3 on postoperative pain medication and weekly alendronate for 8 weeks to decrease subsidence.14 At 2 years follow-up, she was symptom free and no longer required use of any narcotic pain medication. Lumbar radiographs showed stable fusion at L5-S1 without subsidence, hardware loosening, or vertebral body height loss (Figure 3).
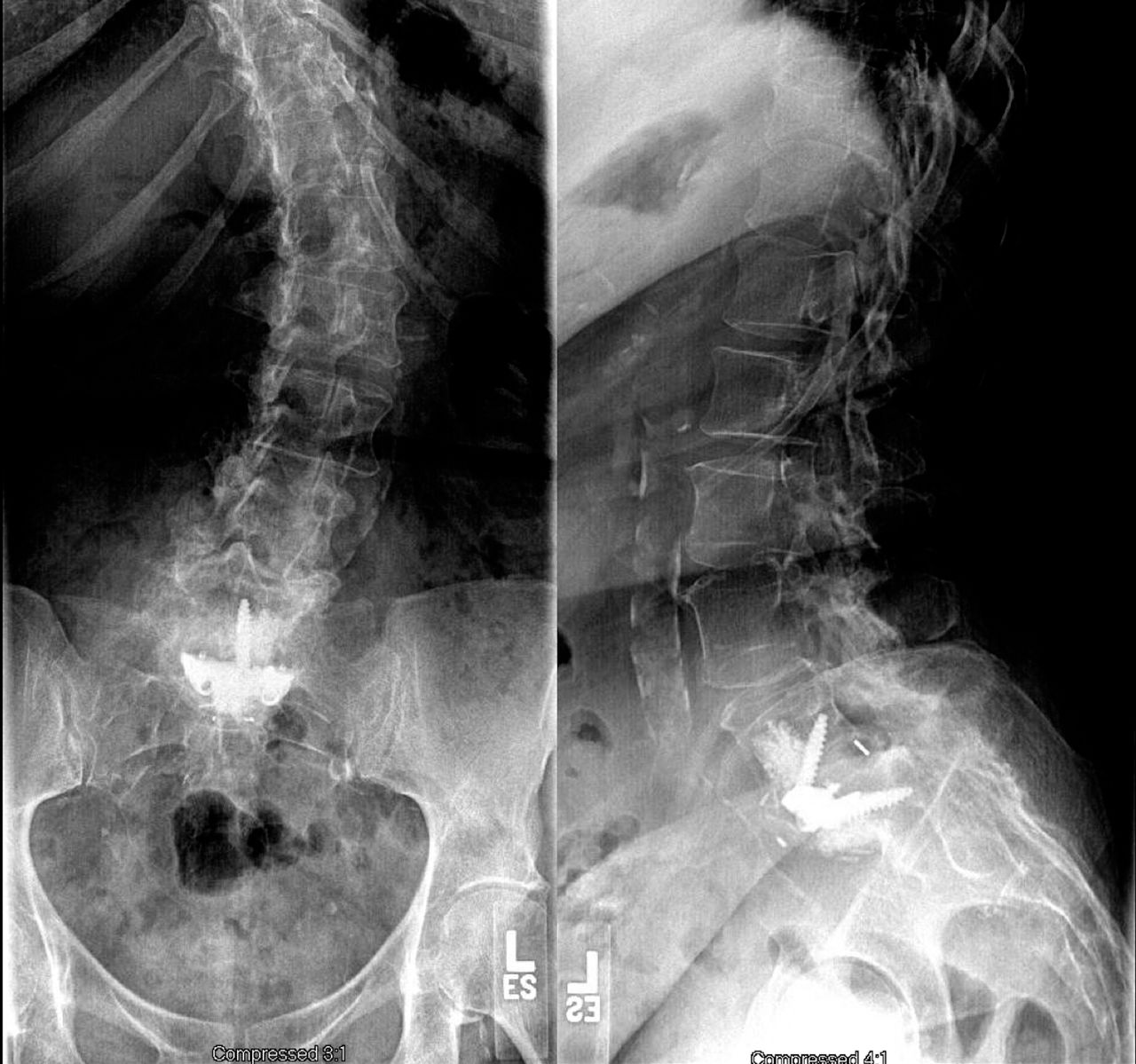
Anterior posterior (left) and lateral (right) lumbar radiographs at 2 years showing excellent interbody fusion without any hardware loosening or loss of vertebral body height.
DISCUSSION
Operative treatment of isthmic spondylolisthesis lacks a definitive consensus, with many fusion techniques having been used in these patients, including ALIF, posterior lumbar interbody fusion, transforaminal lumbar interbody fusion, posterolateral fusion, and circumferential fusion. Significant research has been done to determine the superiority of each technique with still no consensus.2,3 Circumferential fusion in the form of ALIF with posterolateral fusion produces the highest fusion rates but also results in the most complications.3,15 Strube et al16 compared the clinical results of patients who underwent fusion with stand-alone ALIF and those of patients receiving ALIF with pedicle screw fixation and found that pain assessed through both visual analog scales and Oswestry Low Back Pain Disability Index improved more significantly among patients treated with stand-alone ALIF, which questions the clinical relevance of radiographic fusion in patients' postoperative functional improvement. Long-term clinical follow-up of patients treated with ALIF for isthmic spondylolisthesis confirms the satisfactory results at 10 years after surgery.17,18
While there are many surgical options for the treatment of spondylolisthesis, comorbid osteoporosis or osteopenia complicates the management of these patients.12,19 With both osteoporosis and osteopenia, the decrease in bone mineral density correlates to reduced screw pullout strength and increased risk of interbody subsidence.1,19–23 Previously, osteoporosis was a contraindication for instrumented spinal fusion due to increased rates of failure, but advancements in cement augmentation and spinal fixation have changed this outlook.24 Multiple studies have shown the efficacy of PMMA augmentation in instrumented posterior spinal fusion.22,25,26 Kim et al8 evaluated anterior cement augmentation of ALIF in osteoporotic patients, but they did so in patients receiving simultaneous instrumented posterior spine fusion because of the theoretically superior strength and fusion rates of circumferential stabilization. In a cadaveric biomechanical analysis, however, Choi et al13 demonstrated that an anterior stand-alone cage compared with circumferential fixation provides sufficient stability and better simulates anterior-posterior load distribution of a normal intact spine, ultimately leading to significantly less adjacent segment stress and facet joint deterioration. The all-anterior approach described in this report allows for decreased operative times, decreased risk of neurologic damage, and retention of intact posterior muscular and ligamentous support structures.7,9 As compared with percutaneous pedicle screw placement, the all-anterior lumbar approach without posterior fixation also leads to reduction in radiation exposure and avoids damage to the cranial facet joints that can lead to worsening of postoperative pain.10 Vertebroplasty has long been utilized in the treatment of osteoporotic vertebral compression fractures to strengthen the vertebral body, but this procedure has significant risks associated with cement extravasation.27,28 Leakage of the cement, either by way of migration across fractured vertebral body cortex or into external venous plexus, can cause severe complications, including neural compression and cement embolus, respectively.29,30 The use of effective prophylactic vertebroplasty in the form of cement augmentation, however, is associated with a far lower complication rate than that for osteoporotic vertebral compression fracture because the vertebral bodies remain intact.9,31,32 The use of PMMA cement augmentation has also been shown to improve initial screw fixation as well as drastically increase pullout strength.20,25,33 Furthermore, the use of prophylactic anterior cement augmentation has been shown to decrease cage subsidence following ALIF and PSF in osteoporotic patients.8
Cement augmentation does have associated risks that are particularly prone to occur in osteoporotic patients. Reports of failed cement-augmented instrumentation exist, and potential consequences can be more drastic than nonaugmented screws, as the intact cement-screw complex can be displaced through compromised bone.34 These reports warn surgeons against becoming too reliant on cement augmentation, as the underlying disease must be evaluated for operative risk. Vertebroplasty has also been implicated in higher rates of adjacent segment degeneration because improving the structural integrity of an osteoporotic vertebra at one level increases the force placed on and decreases the load to failure of adjacent vertebrae.26,35–37 Prophylactic cement augmentation, however, has been shown through both biomechanical analysis and clinical studies to confer no additional risk of adjacent segment degeneration.8,38
In conclusion, stand-alone ALIF with anterior cement augmentation without posterior supplemental fixation is a potential surgical treatment option for patients with isthmic spondylolisthesis and comorbid osteoporosis or osteopenia. The technique provides adequate fixation while avoiding complications associated with posterior pedicle screw fixation.
Footnotes
Disclosures and COI: No funds were received in support of this work. The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper. This study was approved by the Institutional Review Board of George Washington University Hospital in Washington, DC.
- ©International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}