


Abstract
Background There are many types of minimally invasive lumbar interbody fusion procedures. Among them is the recently introduced biportal endoscopic lumbar interbody fusion surgery. Biportal endoscopic transforaminal lumbar interbody fusion (TLIF) might combine the advantages of minimally invasive TLIF and endoscopic spine approaches. However, clinical evidence in support of biportal endoscopic TLIF remains insufficient.
Methods A comprehensive review of English-language literature on biportal endoscopic lumbar interbody fusion was performed. Articles on biportal endoscopic TLIF in PubMed, the Cochrane Library, and Web of Science were searched using the terms “unilateral biportal endoscopy,” “biportal endoscopic spine surgery,” “transforaminal,” and “lumbar interbody fusion” as well as their combinations. The clinical and radiological outcomes of biportal endoscopic TLIF were analyzed and are summarized here. The biportal endoscopic lumbar interbody fusion surgical techniques are then described.
Results There are 3 biportal endoscopic TLIF techniques. In the available literature, the postoperative 1-year outcomes of biportal endoscopic TLIF were comparable to those of posterior lumbar interbody fusion (PLIF) and minimally invasive (MIS)-TLIF. Clinical parameters were significantly improved after biportal endoscopic TLIF. Compared to PLIF or MIS-TLIF, biportal endoscopic-TLIF may have the advantage of a faster recovery. Biportal endoscopic TLIF showed no inferiority in fusion rates compared to PLIF or MIS-TLIF. The postoperative complications were usually minor.
Conclusions The postoperative 1-year clinical and radiological outcomes of biportal endoscopic TLIF were favorable compared to those of PLIF and MIS-TLIF. However, long-term outcomes should be investigated through prospective, randomized controlled trials in the future.
Clinical Relevance This review article outlines the most current evidence-based medicine with regard to spinal surgery with an aim to introduce a new technique.
INTRODUCTION
Lumbar interbody fusion is a surgical strategy to promote bony arthrodesis by inserting a structural graft into the intervertebral disc space. It can achieve stabilization of the 3-joint complex of the functional spinal unit through pedicle screw fixation.1 Lumbar interbody fusion is known to have better clinical outcomes, higher fusion rates, and lower reoperation rates than posterolateral lumbar fusion surgery because it has the advantages of a wider fusion bed space and biomechanical anterior column support.2,3
There are different types of lumbar interbody fusion procedures, including posterior lumbar interbody fusion (PLIF), transforaminal lumbar interbody fusion (TLIF), anterior lumbar interbody fusion, lateral lumbar interbody fusion (LLIF), and endoscopic lumbar interbody fusion. Among them, minimally invasive (MIS)-TLIF using the microscopic tubular technique can minimize surgical invasiveness, decrease pain, and achieve functional recovery earlier.4–6 Recently, endoscopic lumbar interbody fusion has been attempted as minimally invasive surgery.7 MIS-TLIF procedures may have better functional recovery for patients with spinal disabilities.8 Endoscopic lumbar interbody fusion procedures by uniportal or biportal endoscopic approaches have also been attempted for faster recovery after surgery.7,9
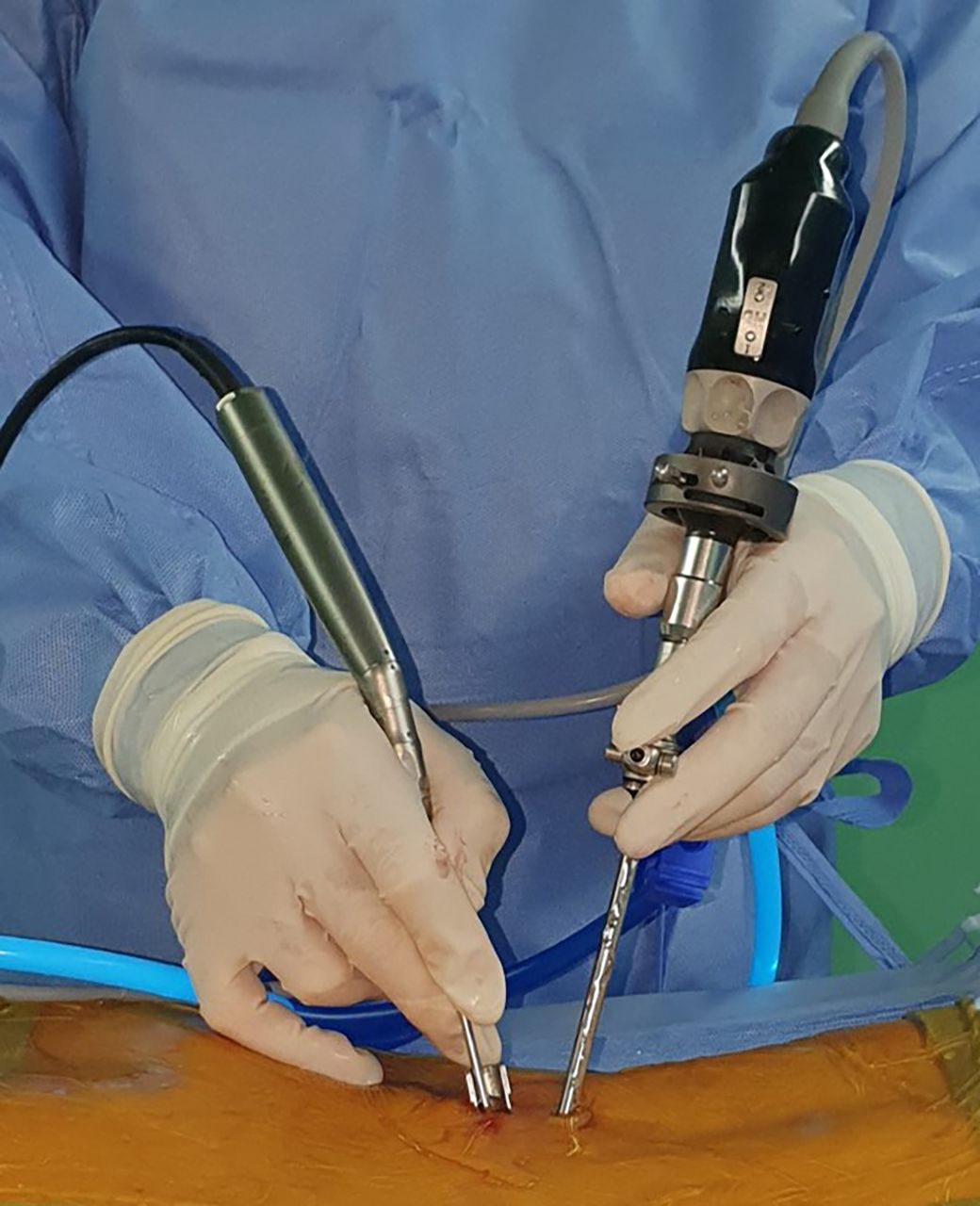
A biportal endoscopic approach can separate the viewing and working channels and allow continuous fluid irrigation through 2 independent surgical channels, unlike percutaneous uniportal full-endoscopic spinal surgery (Figure 1).10–12 In particular, using 2 independent transmuscular channels as the viewing and working portals has the advantage of free movement in the surgical view and the dynamic handling of surgical instruments, thus requiring a relatively shorter learning time than uniportal endoscopy.13–16 In the biportal endoscopic approach, all minimally invasive spinal surgeries such as lumbar discectomy, unilateral laminotomy for bilateral decompression, and lateral foraminotomy can be implemented with good clinical efficacy regardless of the phase of lumbar degenerative disc disease or the location of the primary pathology.17 Furthermore, the biportal endoscopic approach has evolved to the extent that it can be applied to lumbar interbody fusion surgery.7,9,10,18–25
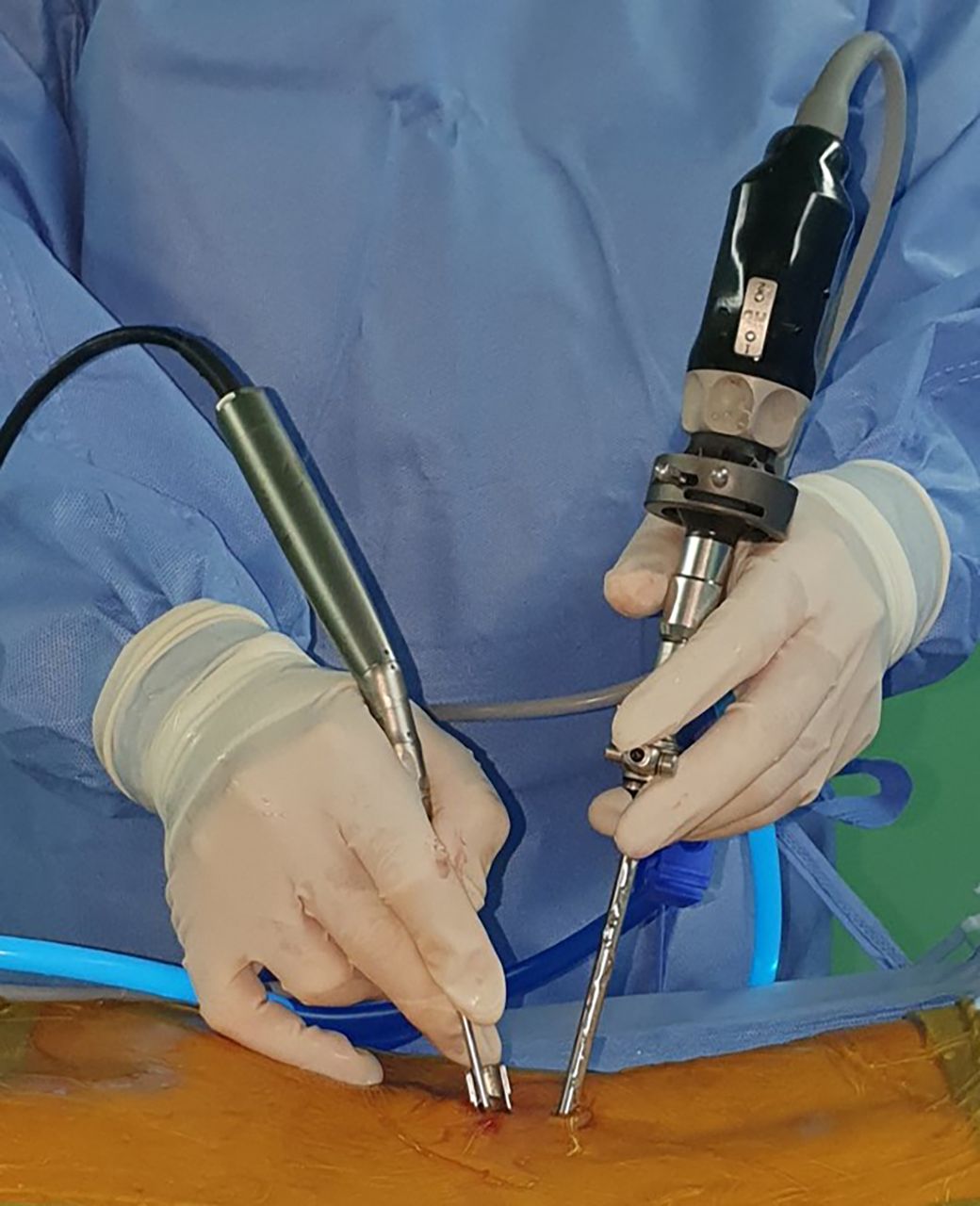
Overview of the biportal endoscopic approach for lumbar interbody fusion.
Early results of endoscopic lumbar interbody fusion surgeries using a biportal endoscopic technique (biportal endoscopic TLIF) have been reported.7,9,20 However, the clinical and radiological results of this surgery have not been accurately established. Therefore, the objective of this article is to describe the surgical technique of biportal endoscopic TLIF and discuss its clinical and radiologic results by reviewing previously published articles.
Surgical Technique of Biportal Endoscopic TLIF
Biportal endoscopic TLIF is performed using an arthroscopic surgical system (4 mm, 0° or 30°) and an automated pressure-controlled pump system set to a pressure of 30 to 35 mm Hg (or a gravity-fed system, which is set 1 m above the patient’s position) during surgery. While maintaining continuous fluid irrigation through each surgical portal, an arthroscopic tissue shaver system is used for tissue dissection, and a bipolar radiofrequency thermocontrolled ablator is used for tissue and vascular cauterization.
The biportal endoscopic TLIF technique is similar to minimally invasive TLIF using a tubular retractor (MIS-TLIF).6,10,20,22,24 Recently, 2 modified biportal endoscopic TLIF methods were introduced, including biportal endoscopic extraforaminal lumbar interbody fusion (biportal endoscopic-EFLIF) and modified far-lateral biportal endoscopic TLIF.25 There are also 2 surgical corridors of biportal endoscopic TLIF; biportal endoscopic TLIF through the trans-Kambin approach is also called biportal endoscopic-EFLIF) and is similar to uniportal full-endoscopic-TLIF.19,21,26–28 In summary, there are 3 biportal endoscopic TLIF methods (routine biportal endoscopic-TLIF, biportal endoscopic-EFLIF, and modified far-lateral biportal endoscopic-TLIF) and 2 corridors of biportal endoscopic-TLIF (the posterolateral and the trans-Kambin approaches).
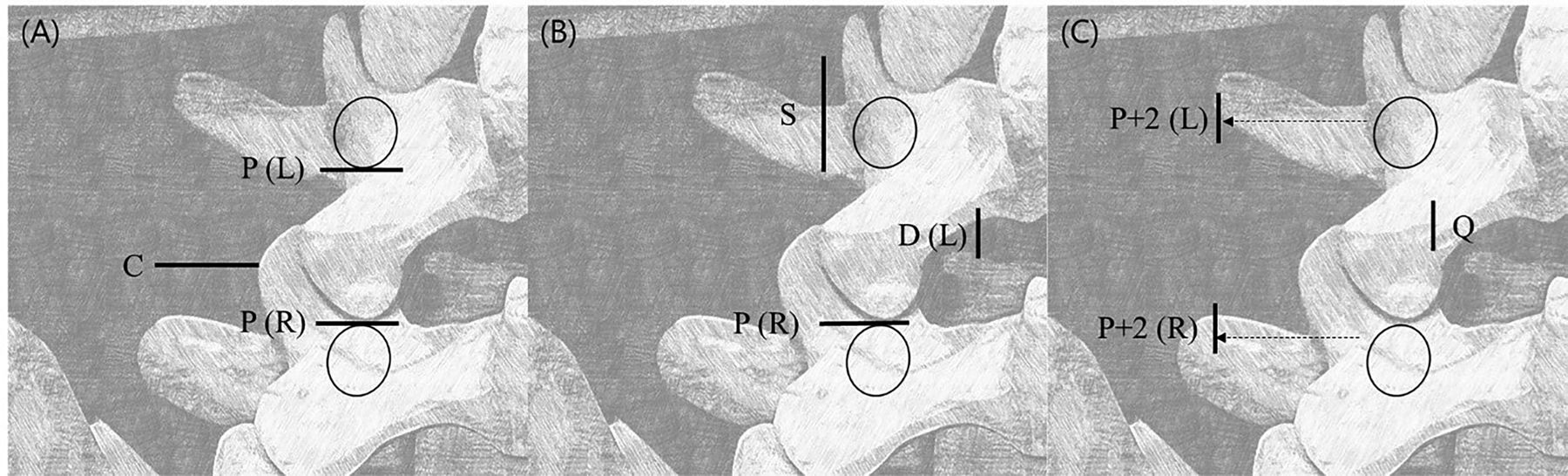
Three kinds of skin incisions are used in the biportal endoscopic TLIF methods. Two skin incisions are made for the 2 portals over the ipsilateral pedicles in modified far-lateral biportal endoscopic TLIF (Figure 2A). Sometimes, an additional far-lateral portal is made for cage insertion (Figure 2A). Two skin incisions for biportal endoscopic TLIF are also made around the ipsilateral pedicles and used for percutaneous pedicle screw insertion (Figure 2B). According to the surgeon’s preference, a medial skin incision may be made at the interlaminar disc level for an endoscopic portal (Figure 2B). For biportal endoscopic EFLIF, 2 skin incisions for 2 portals are made in the lateral area of the pedicles (Figure 2C). These lateral 2 portals may help with access using the trans-Kambin approach to biportal endoscopic EFLIF.
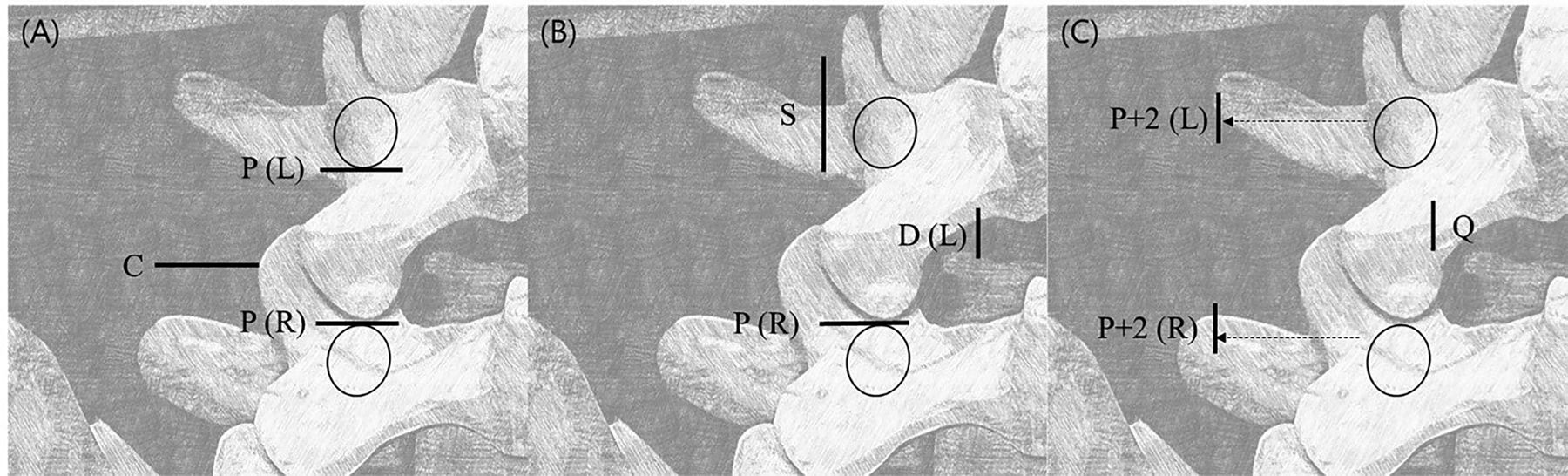
Location of the surgical portals for biportal endoscopic transforaminal lumbar interbody fusion using (A) the modified posterolateral approach, (B) the posterolateral approach, and (C) the extraforaminal approach. P(L): The cranial endoscopic portal located above the pedicle in the posterolateral approach. P(R): The caudal working portal located above the pedicle in the posterolateral approach. C: Additional portal for large interbody cage insertion in the modified far-lateral transforaminal approach. D(L): The cranial endoscopic portal located above the intervertebral disc in the modified posterolateral approach. S: Window for pedicle screw insertion in the modified far-lateral transforaminal approach. P+2(L): The cranial endoscopic portal located 2 cm from the outer lateral interpedicular line in the extraforaminal approach. P+2(R): The caudal working portal located 2 cm from the outer lateral interpedicular line in the extraforaminal approach. Q: Assistance portal located at the cross-section of the medial interpedicular line and the intervertebral disc line.
Biportal Endoscopic TLIF Through the Posterolateral Approach
There are 2 ways to make skin incisions for biportal endoscopic TLIF (video 1). First, 2 skin incisions are made over 2 superior and inferior pedicles spaced 1 cm above and below the intervertebral disc level22 (Figure 2). This allows ipsilateral decompression and contralateral sublaminar decompression through 2 independent skin incisions (Figures 1 and 3). Although there is no consensus that skin incisions for TLIF should be made longitudinally, this horizontal incision is different from that made for conventional percutaneous pedicle screw insertion in that a surgical drain is not inserted immediately after lumbar interbody fusion. The drain should be inserted after completing pedicle screw fixation.
Supplementary video

Two surgical corridors for biportal endoscopic transforaminal lumbar interbody fusion: (A) the posterolateral approach and (B) the trans-Kambin approach.
A second, modified skin incision can also be made. With this method, a 5-mm-long longitudinal skin incision for a viewing portal is made close to the disc space of the medial pedicular line, followed by another 2-cm horizontal skin incision on the working portal over the pedicle20 (Figure 2). This modified surgical port position may help optimize surgical visualization of the superior and inferior endplates during endplate preparation and interbody cage insertion, although an additional 2-cm-long longitudinal skin incision for superior pedicle screw insertion is required.
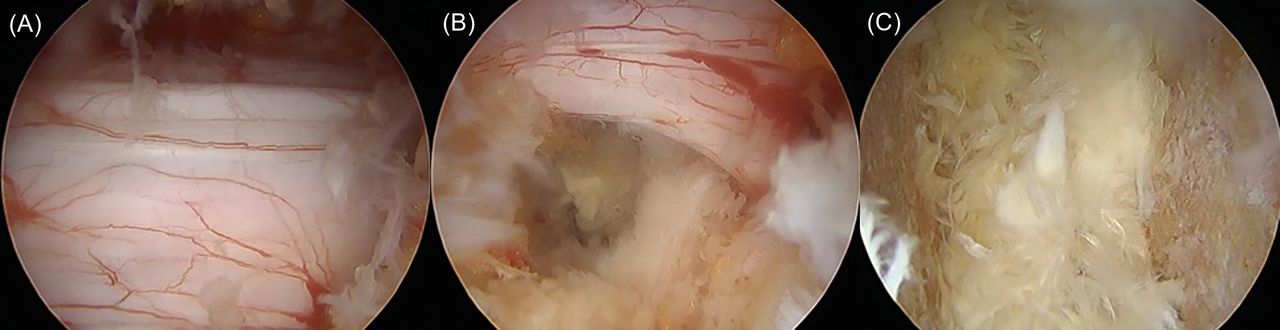
After obtaining endoscopic visualization of the posterior vertebrae, the surgical procedure is almost the same as MIS-TLIF. Central canal decompression is first performed by conducting a unilateral laminotomy with a bilateral decompression procedure (Figure 4A and B). An ipsilateral total facetectomy including inferior and superior articular processes is then performed. After performing an annulotomy, the disc material is removed. In the enlarged endoscopic field of view, only the cartilaginous endplate can be accurately removed without damaging the osseous endplate. Complete endplate preparation can be successfully performed (Figure 4C). After the dura is retracted medially using a root retractor, an interbody cage is inserted into the disc space under C-arm fluoroscopic guidance (Figures 4B and 5). A drainage catheter is placed in the epidural space. Percutaneous pedicle screw fixation is then performed after the interbody fusion procedure (Figure 5).

Optimization of the surgical field of view in biportal endoscopic lumbar interbody fusion surgery. Based on this, (A) sufficient contralateral sublaminar decompression, (B) ipsilateral total facetectomy, and (C) endplate preparation are possible.

Biportal endoscopic transforaminal lumbar interbody fusion through a posterolateral approach (Video 1). A 62-year-old female patient complained of bilateral radicular leg pain with back pain. Preoperative x-ray (A) and magnetic resonance imaging (B, C) depicted grade 2 degenerative spondylolisthesis with central stenosis of L4-5. We performed biportal endoscopic transforaminal lumbar interbody fusion at the L4-5 area. Postoperatively, the patient’s radicular pain was significantly improved. Postoperative magnetic resonance imaging and x-ray (D, E, F, G) revealed good reduction of spondylolisthesis and complete decompression of the central canal at L4-5.
Biportal Endoscopic TLIF Through the Trans-Kambin Approach
Kang et al19 have introduced biportal endoscopic EFLIF through the trans-Kambin approach (Figures 2 and 3). This technique proposes 3 skin incisions. Two 2-cm longitudinal skin incisions are made 2 cm lateral to the pedicle lateral margin [P+2(R) and P+2(L)] over the superior and inferior transverse processes. Another 1-cm longitudinal skin incision (Quarterback portal; Q) is made at the point where the intervertebral disc meets the pedicle medial margin. This positioning of surgical ports allows sufficient endoscopic visualization of the Kambin triangle with only partial lateral facetectomy. In particular, Q can be used as the secondary viewing portal while P(L) is used as the primary viewing portal, or Q can be used as the viewing portal to obtain a vertical surgical visualization for the Kambin triangle with P(L) and P(R) as working portals. In the implantation of the interbody cage, while using P(L) as a viewing endoscopic portal, the interbody cage was inserted through P(R), and the position of the interbody cage within the disc space could be more easily rearranged through Q. However, the disadvantage is that central canal decompression is limited because the main surgical portals are located too far outward. In cases requiring central canal or contralateral sublaminar decompression, unilateral laminotomy for bilateral decompression can be implemented by making one additional port in the distal direction of the Q port.
Modified Far-Lateral Biportal Endoscopic TLIF Using a Large Cage
This method may be used as a surgical fusion method combining the posterolateral approach and the trans-Kambin approach of biportal endoscopic TLIF. Two skin incisions are made for the endoscopic and working portals (Figure 6). Central canal decompression is first performed by conducting a unilateral laminotomy with a bilateral decompression procedure. A total facetectomy involving both the inferior and superior articular processes is then performed. With unilateral laminotomy and total facetectomy, sufficient space can be created to insert a large cage. The discectomy and endplate preparation are then performed after neural decompression.
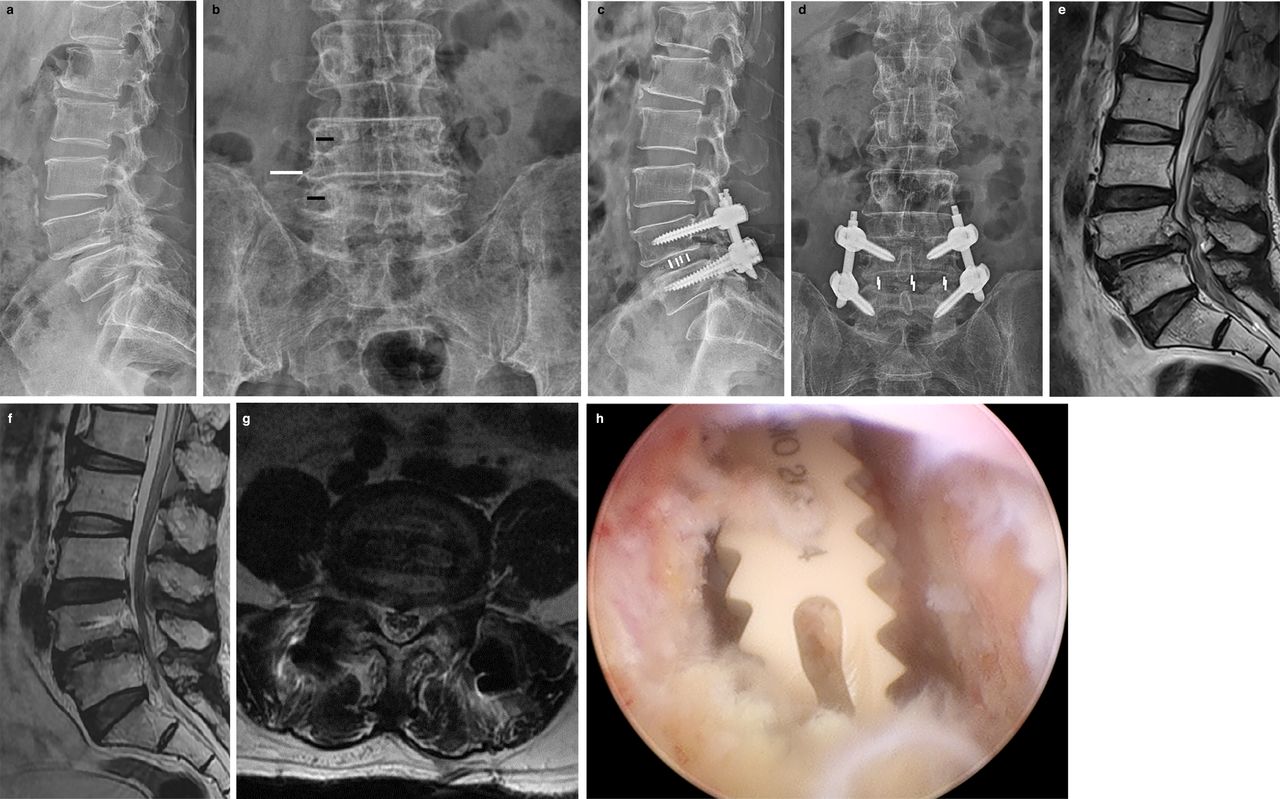
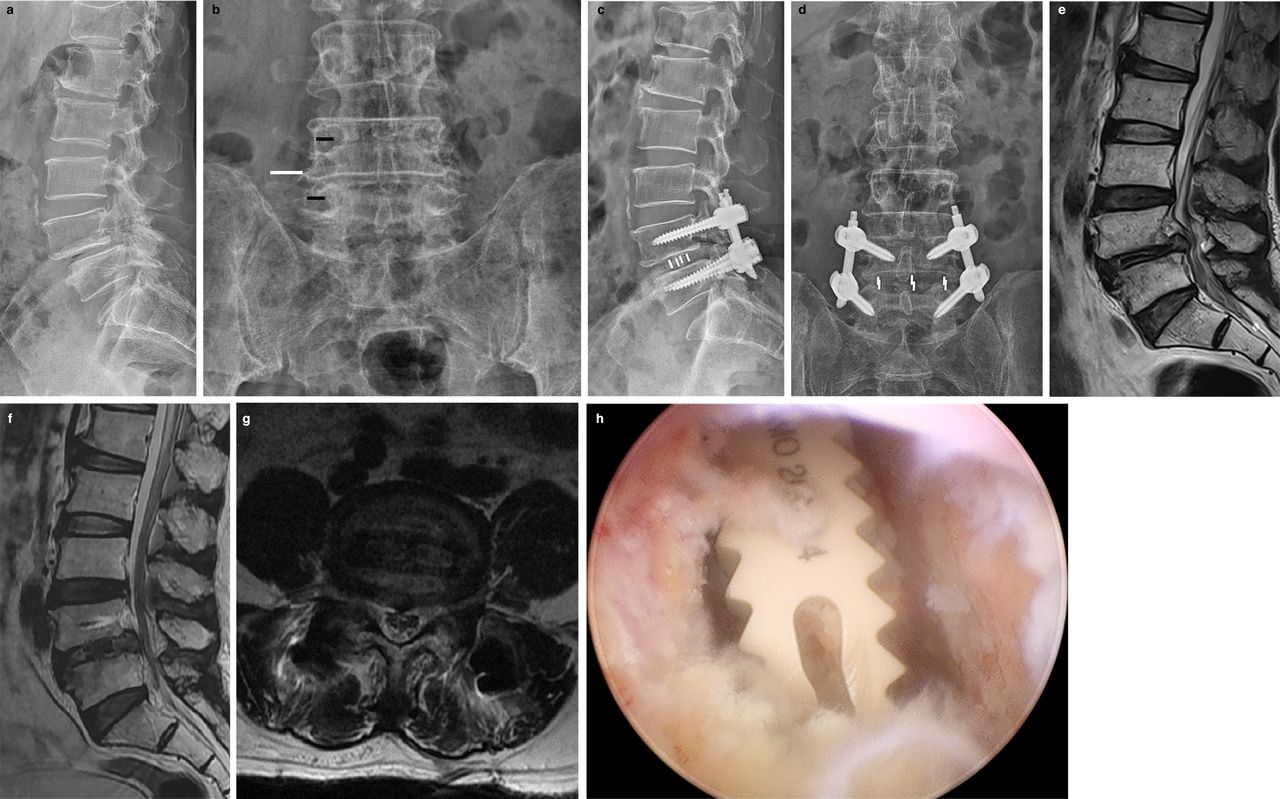
Case of modified far-lateral biportal endoscopic transforaminal lumbar interbody fusion. A 64-year-old male patient presented with bilateral leg pain and claudication. Preoperative x-ray showed isthmic spondylolisthesis of L4-5 (A). We performed modified far-lateral biportal endoscopic transforaminal lumbar interbody fusion at the L4-5 area. Two skin incisions over the pedicles were used for the endoscopic portal and the working portal (B, black lines). An additional lateral skin incision was used for cage insertion (B, white line). A large cage was inserted at L4-5 (C, D). After surgery, spondylolisthesis (E) was well resolved on the postoperative magnetic resonance imaging (F). A large cage was inserted at the L4-5 level (E, G). The intraoperative endoscopic image showed the transverse position of a large cage (H).
An independent additional port is made for the insertion of a large interbody cage on the outside of the lateral interpedicular line (Figure 6). A specially designed cage guide is inserted into the disc space through the additional surgical portal. Then, a large lordotic interbody cage is grafted into the disc space under C-arm fluoroscopic guidance. The cage can be inserted and reposited transversely using a cage impactor (Figure 6).
Review of Published Articles on Biportal Endoscopic TLIF
Four retrospective comparative studies and 3 retrospective case series have been published.9,18,22–25 The inclusion criteria for most studies were as follows: (1) patients who had lumbosacral radiculopathy and/or neurogenic intermittent claudication without responding to conservative treatment over 3 months, (2) single- or 2-level pathology, (3) low-grade degenerative or isthmic spondylolisthesis, (4) degenerative lumbar spinal stenosis with segmental instability, and (5) central stenosis with concomitant foraminal stenosis. The exclusion criteria were patients with infections, high-grade (slips greater than 50%) spondylolisthesis, trauma, tumorous conditions, coronal or sagittal deformities that required surgical correction, or previous spinal surgery at the same level.
Clinical and Perioperative Results
Among the 7 relevant articles that were included, 2 presented overall visual analog scale (VAS) scores, 5 presented VAS scores of back and leg pain, and 6 presented Oswestry Disability Index (ODI) scores (Table). The follow-up period was more than 12 months after biportal endoscopic TLIF in 6 of 7 articles. All operations were performed at or below the L3-4 level. The most frequent operative level was L4-5. The mean operation time reported ranged from 152.4 to 170.46 min. The mean estimated blood loss was 85.5 to 190.3 mL.
Summary of publications on biportal endoscopic transforaminal lumbar interbody fusion.
Although the assessment timing for VAS scores was heterogeneous in these studies, all studies reported significant improvements from preoperative VAS scores for overall, back, and leg pain at the final follow-up. In addition, the postoperative ODI and 36-Item Short Form Health Survey scores at 1 year were reported to show significant improvement compared to the preoperative scores.
Comparative Studies of PLIF, TLIF, and MIS-TLIF
Three comparative studies were reported. A retrospective review of biportal endoscopic TLIF and PLIF reported that biportal endoscopic TLIF had a significantly longer operation time (158.2 ± 26.7 min vs 136.6 ± 21.5 min, P < 0.001). However, PLIF had a significantly higher prevalence of blood transfusions (0% vs 18.6%, P < 0.001).23 In both groups, significant improvements in VAS scores for back and leg pain and ODI scores were observed compared to the preoperative values. However, the postoperative VAS scores for back pain at 1 week (3.8 ± 1.0 vs 5.2 ± 1.1, P < 0.001) and postoperative ODI scores at 1 year (32.7 ± 5.6 vs 29.2 ± 10.1, P < 0.001) were significantly lower in biportal endoscopic TLIF than in PLIF.
In 3 articles comparing biportal endoscopic-TLIF and MIS-TLIF, significant improvements in VAS scores for back and leg pain and ODI scores were reported in both groups at the final follow-up, showing no significant difference between the 2 groups.9,18,25 However, biportal endoscopic TLIF patients showed significantly superior VAS scores for back pain and 36-Item Short Form Health Survey scores in the early postoperative period, including at 1 day, 2 days, 2 weeks, 1 month, and 2 months after surgery. The mean estimated blood loss was significantly lower in biportal endoscopic TLIF in 1 study. In the other 2 studies, biportal endoscopic TLIF showed a significantly longer mean operation time than MIS-TLIF.
Radiologic Outcomes and Fusion Rate
One case-control study reported that there was no difference in radiologic measurements for segment disc height, sagittal Cobb’s angle, or the lumbar lordotic angle between biportal endoscopic TLIF and MIS-TLIF. Most studies reported fusion rates at a follow-up of 1 year after surgery. There were no reports of long-term fusion rate outcomes over 2 years. Short-term fusion rate outcomes in biportal endoscopic TLIF have been reported. Biportal endoscopic TLIF showed no inferiority in fusion rates compared to PLIF or MIS-TLIF (Table). To study the exact fusion rate of biportal endoscopic TLIF, a long-term follow-up study of more than 2 years is needed.
Complications
According to previous reports, there were no major complications related to biportal endoscopic TLIF. Most studies reported minor complications such as small incidental durotomy, nerve irritation, transient root palsy, and postoperative epidural hematoma. These complications usually improved after conservative management, including medication and bed rest. An epidural drainage catheter can be inserted for preventing epidural hematoma. The incidental durotomy site can be directly repaired by the application of TachoSil (an absorbable fibrin sealant patch) and nonpenetrating clips.
Advantages and Disadvantages
As mentioned, the clinical outcomes, complications, and radiological results were comparable 1 year after surgery for biportal endoscopic TLIF and PLIF or MIS-TLIF. However, within 2 months after surgery, early postoperative VAS scores for back pain were more greatly improved in biportal endoscopic TLIF patients.9,18,23,25 Although surgical incision size does not affect postoperative pain or disability, muscle retraction and relaxation time are closely related to paravertebral muscle damage.29 The biportal endoscopic technique, which uses more than 2 transmuscular channels, does not require even a short retraction of the paravertebral muscle. The bipolar radiofrequency thermocontrolled ablator, a new electrosurgical machine, can be used instead of electrocautery. It can cause less thermal injury to paravertebral muscles and neural elements. Therefore, it is expected that biportal endoscopic TLIF has potential advantages regarding crushing or thermal injury to the paravertebral muscle. In addition, it may lead to reduced back pain from an earlier stage after surgery.25
Several studies focusing on complications and poor prognosis after conventional posterior lumbar instrumented fusion surgery reported that longer operation time, greater blood loss, more extensive surgical levels (≥3 segments), and longer hospitalization duration were independent risk factors.30–33 Biportal endoscopic TLIF had the disadvantage of a longer mean operation time than PLIF or MIS-TLIF. However, it had significantly lower mean estimated blood loss and perioperative transfusions.9,23 These findings indicate that longer operation time, a risk factor for postoperative adverse events and poor prognosis, may not apply to biportal endoscopic TLIF.25
The biportal endoscopic technique uses at least 2 independent transmuscular ports: a viewing port and a working port. These 2 surgical ports allow for the dynamic handling of surgical instruments, optimization of the surgical field of vision, and continuous fluid irrigation. Unlike microscopic surgery in which the microscopic lens is located outside the patient’s body, biportal endoscopic surgery places the endoscopic lens inside the body. Therefore, sufficient neural decompression and complete removal of the ligamentum flavum can be obtained with minimal bone resection. In addition, complete endplate preparation can be achieved under a magnified endoscopic view without osseous endplate injury7 (Figure 5).
Disadvantages of the surgical biportal endoscopic TLIF technique are that it may be more difficult compared to conventional open surgery or MIS-TLIF, and the learning curve for endoscopic spine surgery is steep. Since biportal endoscopic-TLIF is technically difficult, performing this operation well requires ample experience in both biportal endoscopic spinal surgery and minimally invasive microscopic surgery.
CONCLUSIONS
This review found that the postoperative 1 year outcomes of biportal endoscopic TLIF may be favorable and are not inferior to PLIF and MIS-TLIF outcomes.
The VAS scores for back and leg pain and ODI scores were significantly improved after biportal endoscopic TLIF. Biportal endoscopic TLIF showed no inferiority in fusion rates compared to PLIF or MIS-TLIF, and postoperative complications were usually minor. The technical difficulty and a steep learning curve were disadvantages of biportal endoscopic TLIF. However, large-scale, long-term, and multicenter prospective randomized controlled trials are needed to determine the clinical relevance of biportal endoscopic TLIF.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The author(s) report no conflicts of interest or financial disclosures with respect to the research, authorship, and/or publication of this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.