


Abstract
Background We aimed to synthesize the latest evidence on the efficacy and safety of decompression alone compared to decompression with fusion in patients with lumbar spondylolisthesis. We also aimed to evaluate factors affecting the efficacy and complications.
Methods A systematic literature search was conducted using PubMed, Scopus, Europe PMC, Cochrane Central Database, and ClinicalTrials.gov. The main outcome was improvement in Oswestry Disability Index (ODI). The secondary outcome was back pain and leg pain improvement, complications, reoperation rate, duration of surgery, length of hospital stay, and blood loss.
Results There were 3993 patients from 13 studies. Decompression with fusion was associated with greater reduction in ODI (mean difference 4.04 [95% CI 0.95, 7.13], P = 0.01) compared to decompression alone. Greater reduction in back (standardized mean difference [SMD] 0.27 [95% CI 0.00, 0.53], P = 0.05) and leg pain (SMD 0.13 [95% CI 0.06, 0.21], P < 0.001) was observed in the decompression with fusion group. Complications were similar in the 2 groups (OR 0.60 [95% CI 0.34, 1.04], P = 0.07). The reoperation rate was similar in both groups (P = 0.54). Decompression alone resulted in shorter duration of surgery (mean difference −85.18 minutes [95% CI −122.79, −47.57], P < 0.001), less blood loss (mean difference −262.65 mL [95% CI −313.45, −211.85], P < 0.001), and shorter hospital stay (mean difference −2.64 days [95% CI −3.58, −1.70], P < 0.001). Empirical Bayes random-effects meta-regression showed that the rate of complication was influenced by age (coefficient 0.172, P = 0.004).
Conclusion Decompression with fusion had greater efficacy than decompression alone but was associated with more blood loss, lengthier surgery, and hospitalization. In terms of complications, decompression alone may be beneficial in younger patients. (PROSPERO CRD42020211904)
Level of Evidence 2A.
INTRODUCTION
Lumbar spondylolisthesis is a degenerative condition in which one vertebra slips forward relative to the vertebra below, resulting in a spondylotic and narrowed spinal segment. This pathology typically causes low back pain, radiating to the buttocks and lower extremities, and neurogenic claudication due to concomitant lumbar spinal stenosis.1,2 As lumbar spinal stenosis symptoms stem from the dural sac or nerve root compression, the need for decompressing the neural structures becomes apparent.3 Conservative treatment is initially offered to symptomatic patients, but if the nonsurgical approach is no longer successful, surgical management in the form of decompression alone or decompression in combination with a spinal fusion is considered.4
To date, the selection of a surgical technique for lumbar spondylolisthesis remains debatable. Many studies comparing the outcomes of 2 different surgical procedures have often had conflicting results. In this systematic review and meta-analysis, we aimed to synthesize the latest evidence on the efficacy and safety of decompression alone compared to decompression with fusion in patients with lumbar spondylolisthesis. We also aimed to evaluate factors affecting the efficacy and complications.
METHODS
This study follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guideline. The protocol was registered in PROSPERO database (CRD42020211904; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=211904).
Eligibility Criteria
We included research articles including randomized controlled trials (RCTs) and observational studies (prospective or retrospective cohorts) that investigate the outcome of interest between patients with degenerative lumbar spondylolisthesis that underwent decompression alone or decompression with fusion with at least 12 months follow-up. Only published studies have been included in this study. We excluded abstract-only publications, letters, preprints, review articles, editorial/commentaries, case reports/case series/studies <20 patients, animal/cadaveric studies, nonEnglish language articles, and studies that did not report key exposures or outcomes of interest.
Search Strategy and Study Selection
A systematic literature search was conducted using PubMed, Scopus, Europe PMC, Cochrane Central Database, and Clinicaltrials.gov with keywords ((decompression alone) OR (decompression only) OR (decompression)) AND ((decompression plus fusion) OR (fusion)) AND (spondylolisthesis)) for records published from inception up until September 29, 2020. Duplicates were removed, and the titles and abstracts of the remaining articles were independently assessed by 2 authors using the inclusion and exclusion criteria.
Data Extraction
Two authors performed data extraction independently using standardized extraction forms that included author, year, study design, age, gender, body mass index, baseline Oswestry Disability Index (ODI), length of follow-up, and the outcome of interest.
The main outcome of interest was the improvement in ODI postoperatively, reported as the mean change from baseline or ODI at the last follow-up. If a study reported both, mean change from baseline was preferred for analysis. Minimal clinically important difference (MCID) in the ODI improvement was ODI improvement above the cut-off point that the respective studies used.
The secondary outcome of interest includes improvement in back pain and leg pain, measured as improvement in either Numerical Rating Scale (NRS) or visual analog scale (VAS) postoperatively. Complications and reoperation rate were reported in the number of events per total sample. Duration of surgery was the length of the procedure which was reported in minutes. The length of hospital stay was the number of hospitalization days before the patient was discharged. Blood loss was the volume of intraoperatively blood loss in milliliters.
The between-group differences in ODI, length of hospital stay, duration of surgery, and blood loss were reported in mean differences. Back pain and leg pain were reported as standardized mean differences (SMDs), because they include 2 different scale, NRS and VAS. MCID, complications, and reoperation rate were reported in odds atios (ORs).
Risk of Bias Assessment
Risk of bias assessment was performed by 2 independent authors. Cochrane risk of bias assessment tools was used to evaluate RCTs and the Newcastle-Ottawa Scale (NOS) was used to assess observational studies.
Statistical Analysis
Review Manager 5.3 (Cochrane Collaboration) and Stata 16 (StataCorp LLC, Texas, USA) were used to perform meta-analysis in this study. We used the inverse variance method to pool continuous variables and obtain mean differences/SMD along with its standard deviations (SDs). To obtain OR along with its 95% confidence intervals (CIs), we used the Maentel-Haenszel formula. Random-effects model was used to pool the effect estimates regardless of heterogeneity. P values in this study were two-tailed, and a value of ≤0.05 was considered statistically significant. Chi-squared and Cochrane Q test were used to assess heterogeneity, I squared (I 2) value of >50% and/or a P value of <0.10 was statistically significant for substantial heterogeneity. We performed regression-based Egger’s test to evaluate the presence of small-study effects for the outcomes. The risk of publication bias was assessed using inverted-funnel plot. Empirical Bayes random-effects meta-regression analysis was performed using age, female sex, and ODI as covariates. Subgroup analyses were performed for RCTs, grade I spondylolisthesis, and single-vertebral level surgery.
RESULTS
Study Selection and Baseline Characteristics
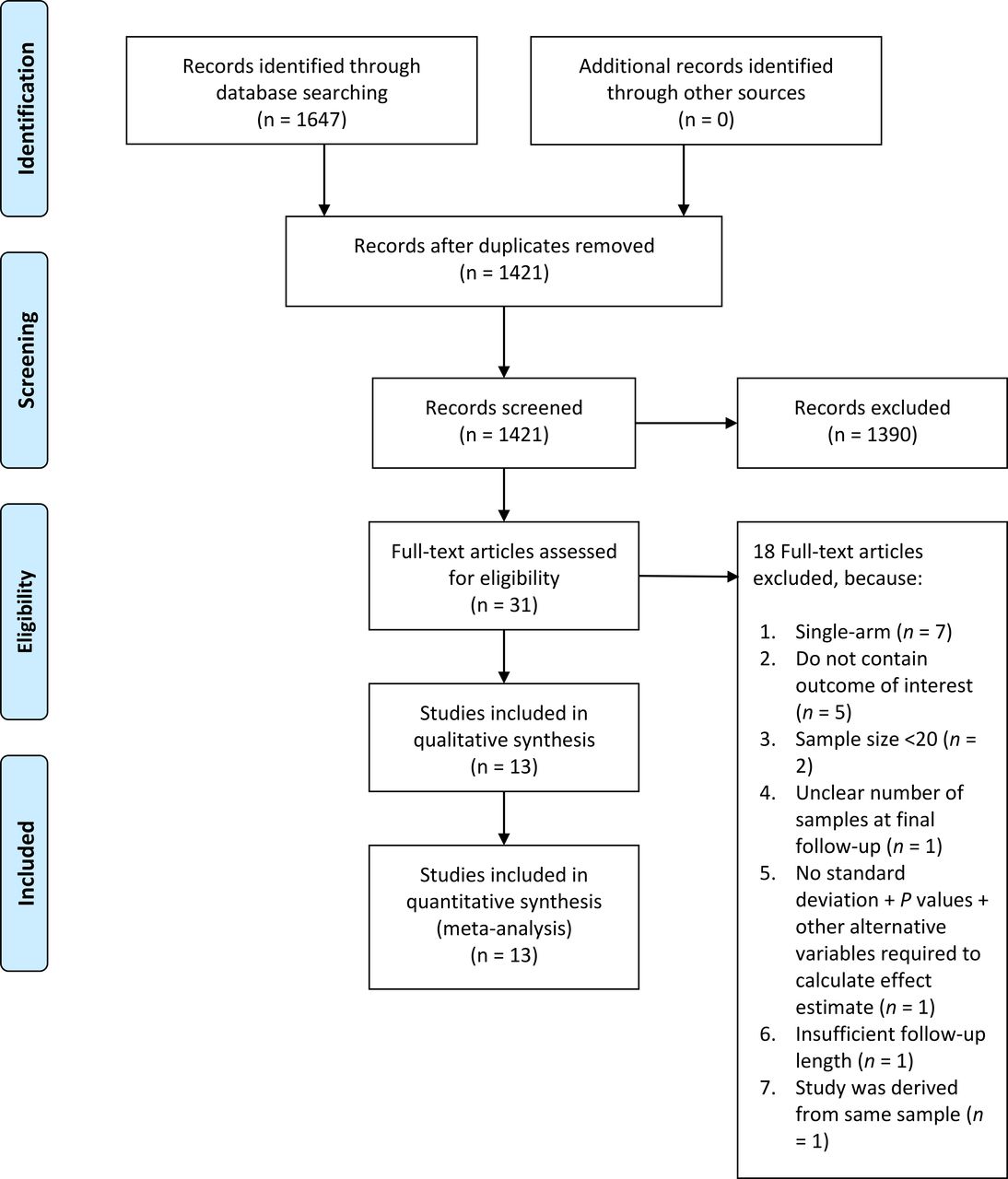
The PRISMA flowchart is presented in Figure 1. We included 13 studies comprising 3993 patients in the qualitative and quantitative syntheses.1–15 Three studies were RCTs, and 10 studies were cohorts. The baseline characteristics of the studies can be seen in Table 1 and Table 2. The mean age of the pooled analysis was 67.85 ± 18.93.

PRISMA flowchart.
Baseline characteristics of included studies.
Inclusion criteria and types of operation of included studies.
Oswestry Disability Index
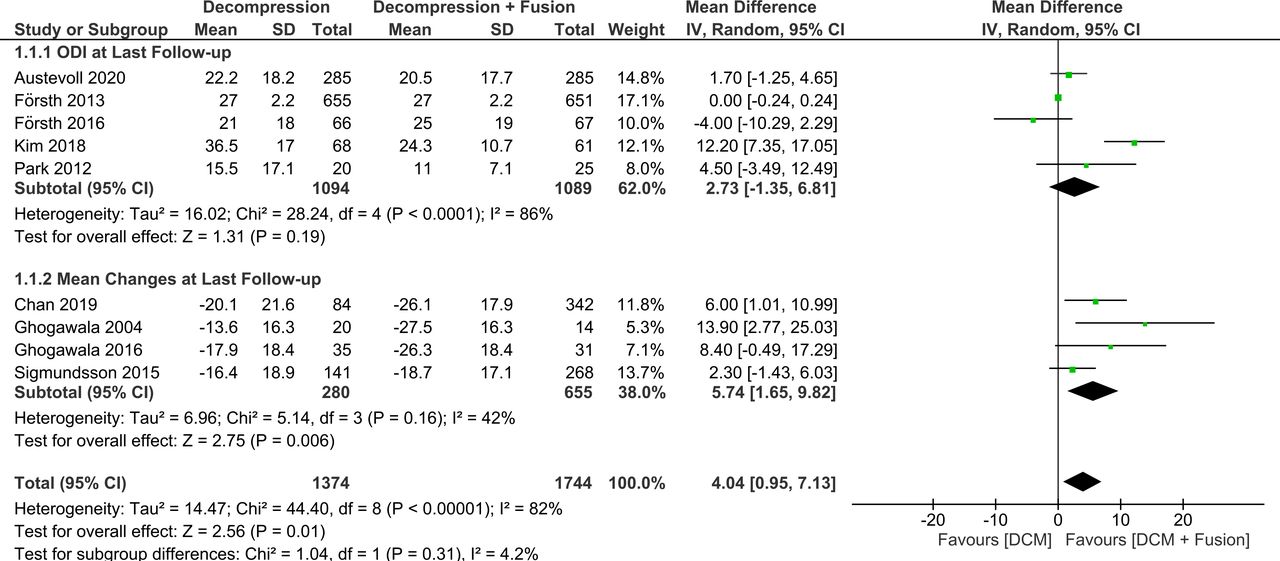
Decompression with fusion was associated with greater reduction in ODI (mean difference 4.04 [95% CI 0.95, 7.13], P = 0.01; I 2: 80%, P < 0.001) compared to decompression alone (Figure 2). The mean changes in ODI at the last follow-up was greater in the decompression with fusion group (mean difference 5.74 [95% CI 1.65, 9.82], P = 0.006; I 2: 42%, P = 0.16). The MCID for ODI improvement was similar (OR 0.76 [95% CI, 0.57, 1.07], P = 0.12; I 2: 0%, P = 0.40).

Oswestry Disability Index (ODI) outcomes. DCM, decompression.
Pain Scores
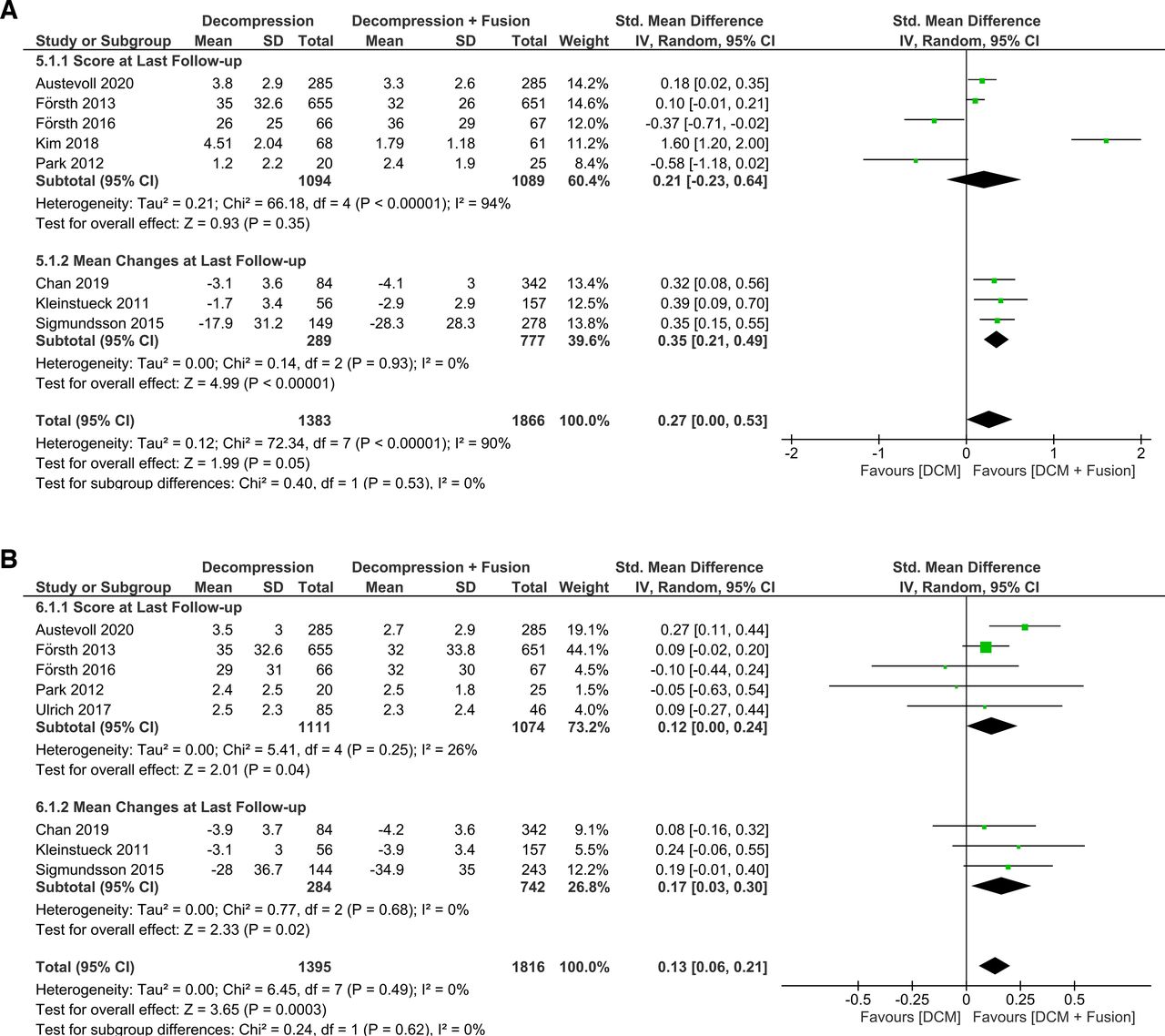
Meta-analysis showed that a greater reduction in back pain (SMD 0.27 [95% CI 0.00, 0.53], P = 0.05; I 2: 90%, P < 0.001) (Figure 3A) and leg pain (SMD 0.13 [95% CI 0.06, 0.21], P < 0.001; I 2: 0%, P = 0.49) (Figure 3B) was observed in the decompression with fusion compared to decompression alone.

(A) Back pain and (B) leg pain outcomes. DCM, decompression.
Complications
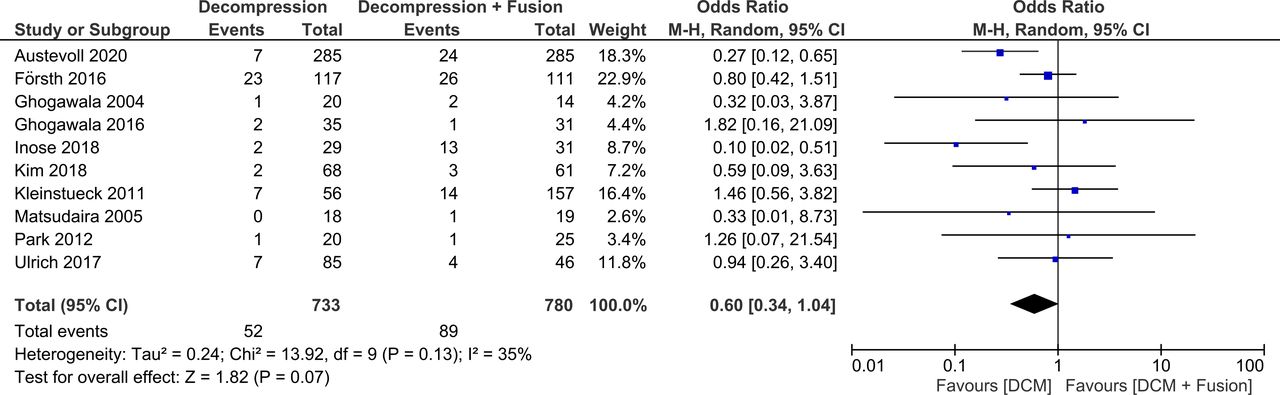
The rate of postoperative complications was similar (OR 0.60 [95% CI 0.34, 1.04], P = 0.07; I 2: 35%, P = 0.13) (Figure 4) compared to the decompression with fusion group. The reoperation rate was similar in both groups (OR 1.17 [95% CI 0.71, 1.93], P = 0.54; I 2: 52%, P = 0.08).

Complications. DCM, decompression.
Duration of Surgery
The duration of surgery was shorter in the decompression alone group (mean difference −85.18 minutes [95% CI −122.79, −47.57], P < 0.001; I 2: 99%, P < 0.001) compared to decompression with fusion group. Decompression alone group was associated with less blood loss (mean difference −262.65 mL [95% CI −313.45, −211.85], P < 0.001; I 2: 87%, P < 0.001).
Length of Hospital Stay
The length of hospital stay was shorter in the decompression alone group (mean difference −2.64 days [95% CI −3.58, −1.70], P < 0.001; I 2: 91%, P < 0.001).
Risk of Bias Assessment
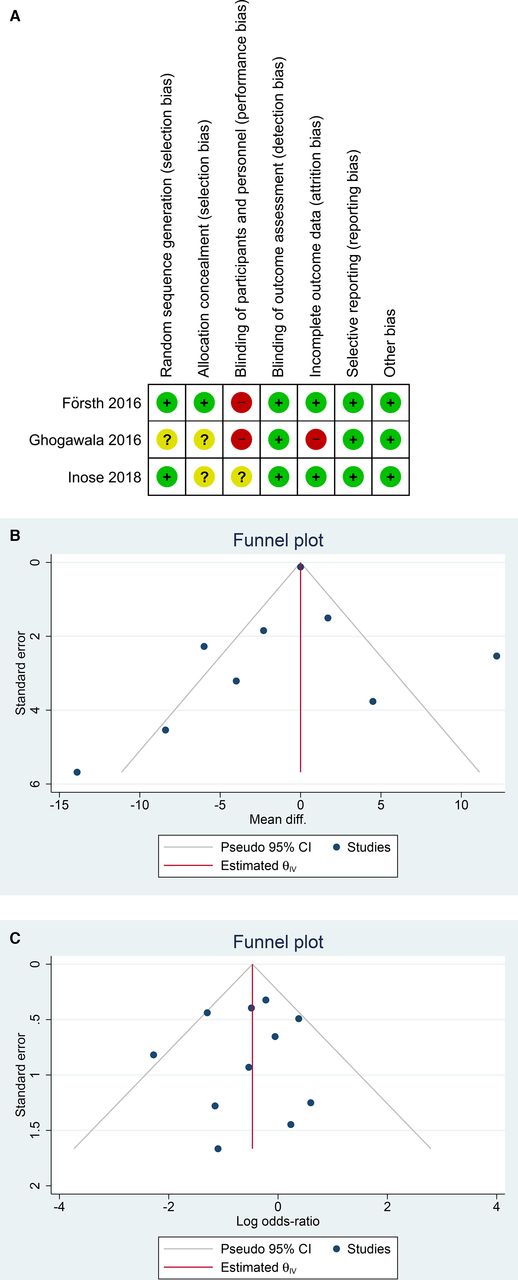
The risk of bias assessment for RCTs can be seen in Figure 5A, and the NOS for observational studies can be seen in Table 1. Funnel plot analysis showed a relatively symmetrical distribution for the ODI (Figure 5B) and complications (Figure 5C). Regression-based Egger’s test showed no indication of small-study effects for the ODI (P = 0.219), leg pain (P = 0.257) improvement, and number of complications (P = 0.810). Back pain improvement was statistically significant for small-study effects (P = 0.009).

Risk of bias assessment. Risk of bias assessment for randomized controlled trials (A). Funnel plot analysis for Oswestry Disability Index (B) and complications (C).
Meta-Regression
Empirical Bayes random-effects meta-regression showed that the difference in ODI improvement between decompression alone and decompression with fusion group was not influenced by preoperative ODI (coefficient −0.31, P = 0.322), age (coefficient −0.519, P = 0.619), and female sex (coefficient 0.309, P = 0.352). Age (coefficient −0.533, P = 0.411), female sex (coefficient −0.174, P = 0.449), and preoperative ODI (coefficient −0.022, P = 0.948) did not significantly influence the difference in back pain improvement between the 2 groups. Difference in leg pain improvement was not significantly affected by age (coefficient −0.020, P = 0.904), female sex (coefficient −0.026, P = 0.672), and preoperative ODI (coefficient 0.005, P = 0.974). Meanwhile, the rate of complications varied significantly by age (coefficient 0.172, P = 0.004) but not by female sex (coefficient 0.041, P = 0.115). We further performed subgroup analysis in studies with mean age less than 67.8 years old (the mean age of the pooled analysis) and found that complications were significantly decreased in the decompression alone group (OR 0.46 [95% CI 0.23, 0.92], P = 0.03; I 2: 36%, P = 0.15).
Subgroup Analysis for RCTs
Decompression alone and decompression with fusion resulted in a similar rate of ODI improvement (mean difference 1.78 [95% CI −10.34, 13.91], P = 0.77; I 2: 80%, P = 0.03), reoperation (OR 1.39 [95% CI 0.33, 5.93], P = 0.66; I 2: 80%, P = 0.03), complications (OR 0.49 [95% CI 0.11, 2.23], P = 0.36; I 2: 68%, P = 0.04). Decompression alone was associated with reduced blood loss (mean difference −345.00 mL [95% CI −458.89, −231.11], P < 0.001; I 2: 71%, P = 0.03), length of surgery (mean difference −104.40 [95% CI −168.75, −40.04], P = 0.001; I 2: 96%, P < 0.001), and length of stay (mean difference −2.14 d [95% CI −3.12, −1.16], P < 0.001; I 2: 49%, P = 0.14). There was only one RCT that evaluated back and leg pain improvement; hence, it was not included in the subgroup analysis.
Subgroup Analysis for Grade I Spondylolisthesis
Meta-analysis showed that decompression with fusion was associated with greater ODI improvement (mean difference 6.48 [95% CI 1.17, 11.79], P < 0.001; I 2: 72%, P = 0.003). There was similar improvement in terms of back (SMD 0.26 [95% CI −0.58, 1.10], P = 0.55; I 2: 95%, P < 0.001) and leg pain (SMD 0.02 [95% CI −0.17, 0.20], P = 0.86; I 2: 0%, P = 0.68). Both have similar complications (OR 0.77 [95% CI 0.45, 1.33], P = 0.35; I 2: 0%, P = 0.92) and reoperation rate (OR 1.35 [95% CI 0.56, 3.23], P = 0.50; I 2: 61%, P = 0.08). Decompression alone was associated with reduced blood loss (mean difference −267.15 mL [95% CI −326.17, −208.14], P < 0.001; I 2: 90%, P < 0.001), length of surgery (mean difference −81.21 minutes [95% CI −129.40, −33.03], P = 0.001; I 2: 98%, P < 0.001), and length of stay (mean difference −2.09 days [95% CI −2.69, −1.49], P < 0.001; I 2: 62%, P = 0.05).
Subgroup Analysis for Single-Vertebral Level Surgery
Subgroup analysis showed that decompression with fusion was associated with greater ODI improvement (mean difference 4.15 [95% CI 1.48, 6.82], P = 0.002; I 2: 0%, P = 0.50) compared to decompression only. Similar improvement in terms of back (SMD 0.15 [95% CI −0.20, 0.51], P = 0.39; I 2: 76%, P = 0.01) and leg pain (SMD 0.13 [95% CI −0.02, 0.28], P = 0.08; I 2: 0%, P = 0.65) was observed. The 2 procedures have similar complications (OR 0.42 [95% CI 0.09, 1.94], P = 0.27; I 2: 37%, P = 0.19) and reoperation rate (OR 2.05 [95% CI 0.94, 4.45], P = 0.07; I 2: 10%, P = 0.29). Decompression alone resulted in less blood loss (mean difference −277.09 mL [95% CI −395.15, −159.03], P < 0.001; I 2: 89%, P < 0.001), shorter length of surgery (mean difference −115.38 minutes [95% CI −160.05, −70.71], P < 0.001; I 2: 91%, P < 0.001), and shorter length of stay (mean difference −2.03 days [95% CI −2.62, −1.44], P < 0.001; I 2: 70%, P = 0.04).
DISCUSSION
This meta-analysis showed that decompression with fusion resulted in a more significant improvement in ODI and pain scale compared to decompression alone. However, the duration of surgery, operative blood loss, and the length of hospital stay were lesser in the decompression alone group. Although the trend for complications was lower in decompression alone group, it was not statistically significant. The summary of meta-analysis is available in Table 3.
Summary of findings.
Consideration remains regarding the extent of surgery required in each individual case and whether analysis of the preoperative symptoms can assist in selecting the most appropriate procedure. Currently, there is no clear guidelines about which surgery is best for any given patient. In a clinical practice, patient selection is typically based on the symptoms arising from mechanical low back pain and radiating buttock and leg pain and their relationship with each other. A patient presenting with nerve compression due to stenosis as the main symptom, without the presence of major low back symptoms, may be advised to undergo a simple decompression rather than a more extensive fusion procedure even though there is an underlying slippage, which may indicate an inherent instability.10
Decompression has become the treatment of choice for severe spinal stenosis and provides better outcomes than nonoperative management, but it is often associated with postoperative instability.16 Several factors may increase the likelihood of instability after laminectomy for spondylolisthesis, such as facet angle, disc height, and motion on flexion-extension radiographs.8 Some surgeons consider spondylolisthesis with a 3-mm translation as a sign of instability; therefore, some facilities recommend performing instrumentation surgery regardless of the severity of spondylolisthesis. Decompression with fusion technique has since become the standard treatment for degenerative spondylolisthesis.3
Many believe that adding fusion to decompression will result in a systematically better outcome. One plausible explanation for this assumption is that decompression alone does not adequately help patients with predominantly stenotic symptoms, because the underlying cause of the stenosis, such as instability, is left untreated. Another explanation is that more stenosis would present due to the slippage, and this condition requires more extensive resection, which is often impossible without creating more instability, and therefore this cannot be resolved by decompression alone.10
Performing simultaneous fusion in elderly population, who generally have multiple comorbidities, may lead to a greater risk of life-threatening perioperative complications (ie, pneumonia, respiratory failure, and acute myocardial infarct) and a higher rate of death.10,16 Osteopenia or osteoporosis is a condition that commonly coexists in the elderly that increases the risk of screw loosening and sinking of the intersomatic cage.15 Although age may be a factor limiting the effectiveness of lumbar surgery, it is not associated with worse outcomes when fusion is used to complement decompression compared to decompression alone.7
Even though the use of pedicle screws may result in higher fusion rates, it does not necessarily lead to improvements in low back pain and radiculopathy; this raises the question of which procedure is superior to others, and also whether localized spinal instability due to spondylolisthesis causes lower back pain and/or decreased quality of life.3 Decompression alone is performed with less resection of the bony elements and thus in a more limited space compared to decompression with fusion, where the exposure is usually more extensive and resection can be carried out more freely without the risk of creating increased instability.10 Our meta-analysis showed that the improvement in ODI and pain scale is better in patients receiving decompression with fusion. However, the need for instrumentation in fusion surgery carries the risk of infection due to osteosynthesis material and the risk of hardware malposition and failure, necessitating reoperation.4,15 Our study showed that the reoperation rate was similar in the 2 groups. The longer duration of decompression with fusion procedure compared to decompression alone also increases the risks of anesthesia and their consequences in the elderly population.15 Furthermore, there is a risk of accelerated degenerative changes adjacent to a lumbar fusion in elderly individuals.16
Meta-regression analysis showed that in terms of complications, decompression alone may be beneficial in younger patients. Increasing age, although controversial, has been shown to affect the prognosis in lumbar spinal surgery negatively.14,17–20 One of the plausible explanations for the possible benefit in the younger age is the rate of complication is higher in the elderly due to age or other medical comorbidities. Thus, the complications are more avoidable in the younger groups.
One study provided no standard deviation, P values, or other alternative variables required to calculate effect estimate; the study reported that both methods result in satisfactory clinical outcomes.21 One study was excluded because of the unclear number of samples at final follow-up; it showed that both decompression alone and decompression with fusion resulted in similar 5-year reoperation rates.22 Studies showed that both surgical modalities resulted in similar improvement in quality of life measured by EuroQol 5-dimensions (EQ-5D) and Short Form-36 (SF-36).1,6–9,12,13,16 However, Kleinstueck et al reported that the improvement in Core Outcome Measures Index was significantly greater in the decompression with fusion group.10 In terms of expense, Yagi et al showed that both decompression alone and decompression with fusion is equally cost-effective.23
Clinical Implications
This meta-analysis indicates that decompression with fusion has greater efficacy than decompression alone but was associated with lengthier surgery and hospitalization. In terms of complications, decompression alone may be beneficial in younger patients. Thus, decompression alone might be more valuable in younger patients, although further RCT in younger patients is needed. Nevertheless, in the presence of instability, decompression alone may have limited success. Thus, in this subset of patients, decompression with fusion might be a procedure of choice. The studies included involvement of 1–3 vertebral levels, patients with >3 vertebral involvements may benefit more from the decompression with fusion as opposed to decompression alone.
Limitations
The primary limitation of this meta-analysis is that the several included studies have a moderate-high risk of bias. Additionally, there were only 3 RCTs available for analysis. Several studies did not report their spondylolisthesis grade, which may influence the surgical outcome.
CONCLUSIONS
Decompression with fusion results in a greater improvement in ODI and pain scale compared to decompression alone. Duration of surgery, operative blood loss, and the length of hospital stay were lesser in the decompression alone group. In terms of complications, decompression alone may be beneficial in younger patients.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript.
Disclosure The authors report no financial disclosures related to this article.
Contributors Raymond Pranata conceived and designed the study and drafted the manuscript. Raymond Pranata and Rachel Vania acquired the data and drafted the manuscript. Raymond Pranata and Michael Antonius Lim performed data extraction and interpretation. All authors contributed to the writing of the manuscript. Raymond Pranata performed the statistical analysis.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}