


Abstract
Background Spinal fractures are among the most common traumatic injuries in elderly patients, with the odontoid process being frequently affected. As this patient group usually has high rates of comorbidity and chronic diseases, a nonoperative approach may offer a reasonable solution for a favorable fracture pattern.
Objective We modified the procedure by implanting a bilateral atlantoaxial joint spacer (model DTRAX) into the joint space and review our experience utilizing this technique for the treatment of patients with a fracture of the odontoid process.
Methods A retrospective evaluation was performed on patients treated surgically for unstable traumatic fractures of the odontoid process. The stabilization was performed using a dorsal rod and screw instrumentation of the lateral mass of the atlas and the pars interarticularis of the axis. The procedure was further modified by implanting a bilateral atlantoaxial joint spacer (DTRAX) into the joint space bilaterally after the removal of the articular cartilage. Patients older than 70 years with a traumatic fracture of the odontoid process were included. Pain was assessed pre- and postoperatively using the visual analog scale (VAS). To verify fusion during follow-up, either x-ray imaging of the cervical spine or magnetic resonance imaging or computed tomography were performed.
Results A total of 5 patients were included in our study. Four patients had an American Society of Anesthesiology score of 3 and 1 had a score of 4. The average duration of surgery was 187 ± 38.1 minutes. The average blood loss during the procedure was 340 ± 270 mL. The average radiological follow-up period was 21.2 ± 17.5 months. Preoperatively, the average VAS pain score was 2.3 ± 3.3. Postoperatively, the mean VAS decreased to 0.6 ± 0.9. The average follow-up period for pain was 27.2 ± 19 months. No patient showed neurological deficits before or after surgery. Follow-up demonstrated solid fusion in all cases.
Conclusion The fusion of the atlantoaxial joint with bilateral atlantoaxial joint spacers represents a suitable and feasible option for achieving high fusion rates in elderly patients with odontoid fractures.
Clinical Relevance A significant percentage of patients who are treated non-operatively will experience nonunion, which may cause instability of the atlantoaxial joint. Posterior fixation with screws and rods is a treatment option, but it leaves the cartilaginous joint surface in place, which can be an impediment to the fusion process. In other cases, degenerative collapse of the C1/C2 joint can cause compression of the C2 nerve root.
Level of Evidence 4.
- cervical fusion
- atlantoaxial fusion
- cage implantation
- facet cages
- DTRAX
- odontoid fracture
- odontoid non union
- odontoid pseudarthrosis
- elderly
- geriatric patients
Introduction
Spinal fractures are among the most common traumatic injuries in elderly patients.1 Due to the complex anatomy of the upper cervical spine, the odontoid process is frequently affected.1,2 The cause of injury in the elderly is most often incurred during low-energy traumatic events such as a fall from a standing position.3 Odontoid fractures can lead to a massive reduction in quality of life for those affected and are associated with high mortality and morbidity.4 The optimal treatment, however, in elderly patients with odontoid fractures remains controversial.3,5–7 In elderly patients, especially those with comorbidities or poor bone quality, conservative treatment may be the most appropriate solution if the fracture pattern is favorable.6,8–10 However, a significant percentage, ranging from 56% to 72% of patients treated nonoperatively, will experience nonunion, which may lead to permanent instability of the atlantoaxial joint.5,8,11–13 For these reasons, traumatic instability of the atlantoaxial joint may be an indication for surgical intervention by instrumented fusion.3,14
Several critical characteristics of elderly patients must be accounted for when considering a cervical stabilization surgery, such as the high rates of comorbidity and chronic disease, the occurrence of osteoporosis, and the frequently displayed low compliance rate to postoperative instructions.3,4,14–19 To meet this therapeutic challenge, a variety of surgical procedures have been developed, each with a unique risk profile.20–25 Presently, fixation with a C1 lateral mass and C2 pedicle screw and rod, also known as the Goel-Harms technique, has been widely used for atlantoaxial fixation with optimal stability and acceptable fusion rates.12,20,26 However, a distinct disadvantage of this procedure is that the cartilaginous joint surface is left in place, which can be an impediment to the fusion process.20,27 In other cases, cartilaginous destruction often leads to a collapse of the C1/C2 joint, which can cause compression of the C2 nerve root potentially causing long-term pain.28,29
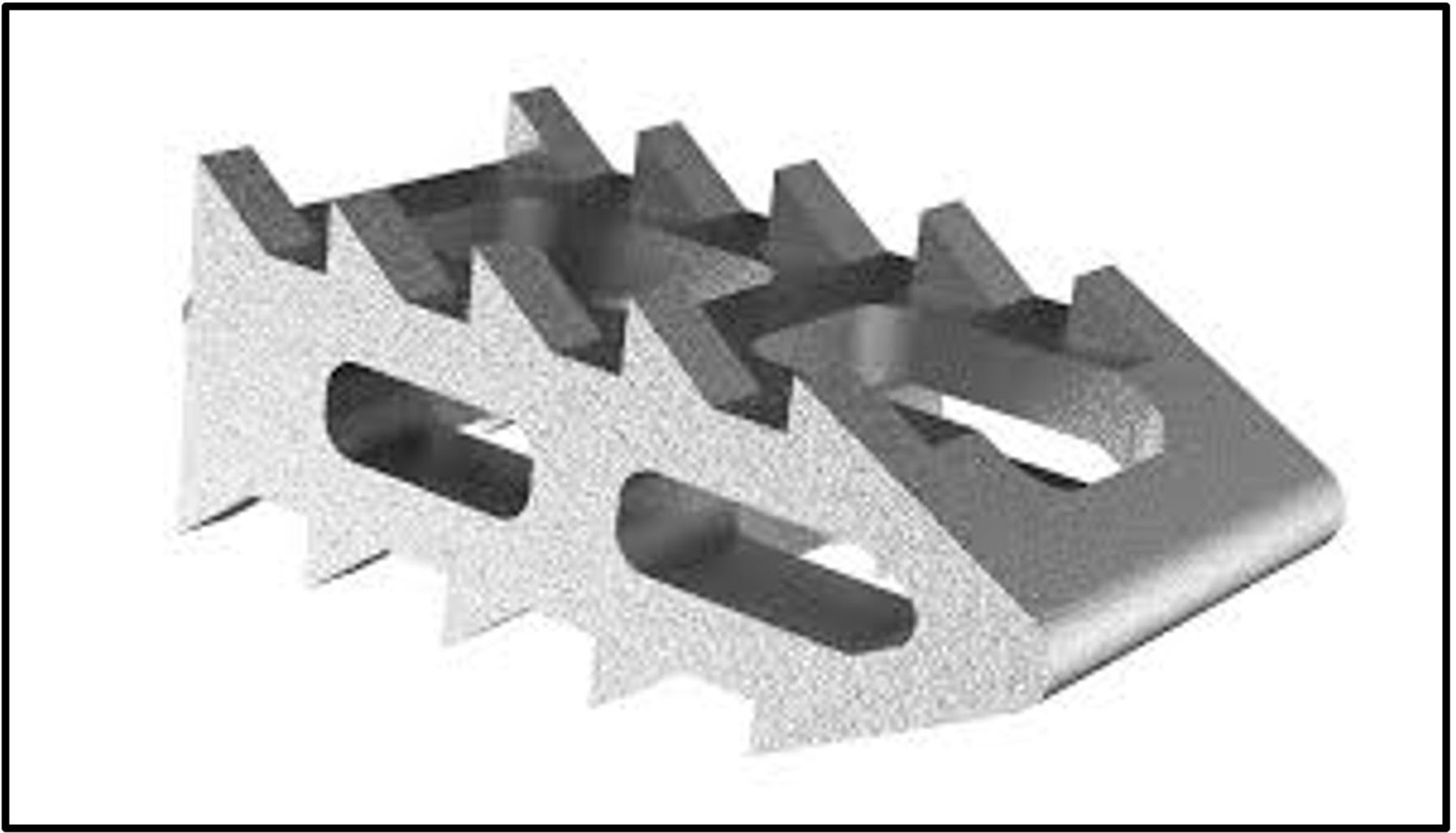
To address these shortcomings, we modified the procedure described by Goel-Harms by implanting a titanium or machined bone graft atlantoaxial joint spacer into the joint space after removing cartilage from the C1/C2 joint to augment fusion and simultaneously restore the height of the joint space (Figure 1). In the present article, we review our experience utilizing this technique for the treatment of patients with a fracture of the odontoid process. To our knowledge, this is the first report in the literature on the treatment of odontoid fractures in elderly patients using this technique.
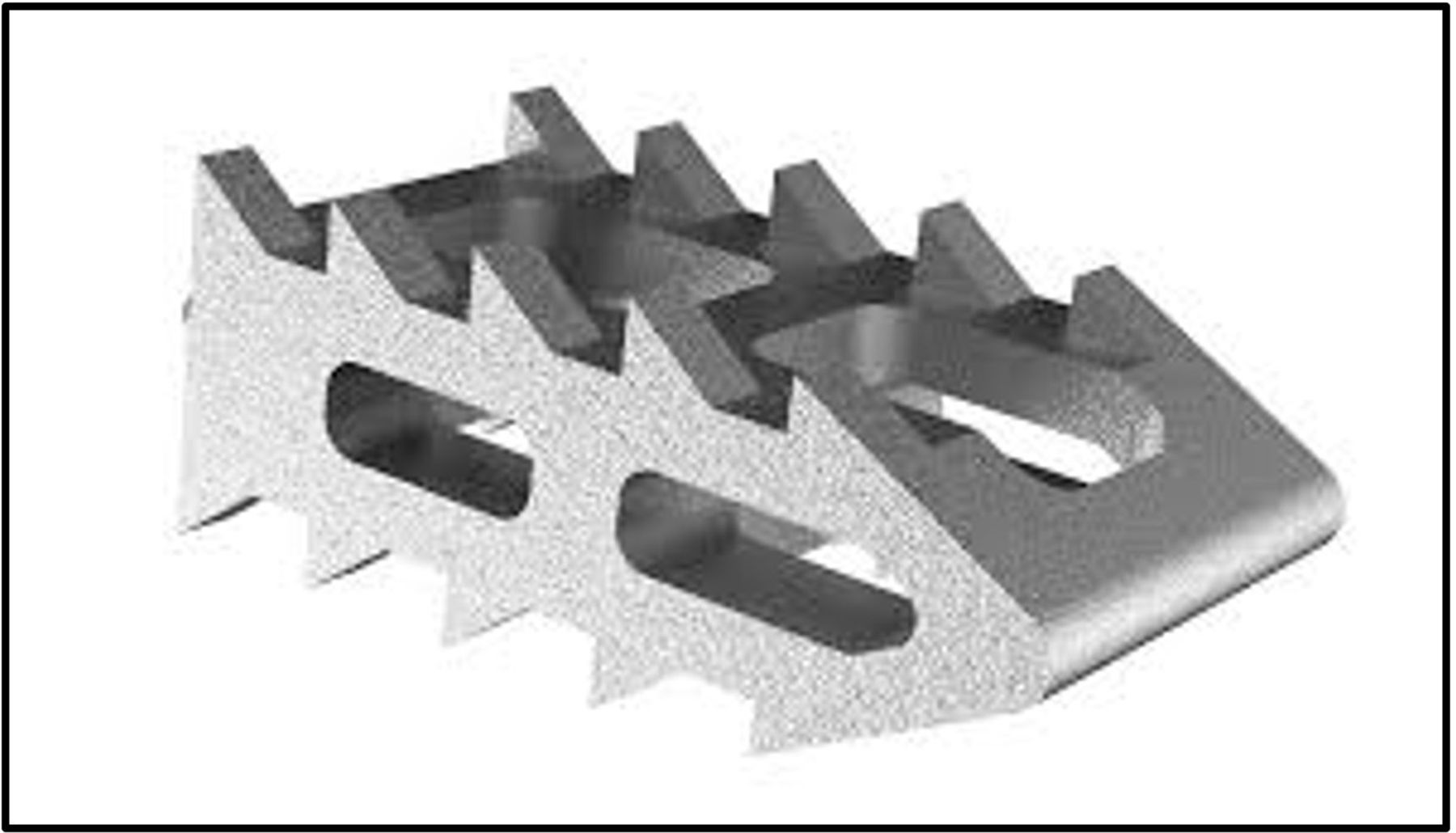
Illustration of a titanium interbody cervical spacer; length: 10 mm, wide: 5.5 mm, height: 2.5 mm (Fa. Stoeckli Medical; Oberkirch, Switzerland; graphics by Stoeckli medical).
Materials and Methods
A retrospective evaluation was performed on patients treated surgically for unstable traumatic fractures of the odontoid process (C2) (Figure 2). Stabilization was performed utilizing the Goel-Harms technique for dorsal rod and screw instrumentation of the lateral mass of the atlas and the pars interarticularis of the axis.20 We further modified the procedure by implanting a bilateral atlantoaxial joint spacer (DTRAX, Stoeckli Medical, Oberkirch, Switzerland) measuring 10 mm × 5.5 mm × 2.5 mm into the C1/C2 joint space bilaterally after removal of the articular cartilage. The spacer was additionally filled with demineralized bone matrix and autologous cancellous bone.

Preoperative computed tomographic image of an odontoid fracture (blue arrow) Anderson/D'Alonzo type 2, Eysel/Roosen type B with significant posterior dislocation.
Included in this case series were patients aged 70 years or older with a traumatic fracture of the odontoid process. Indications for surgery were instability of the fracture, dislocation in the fracture gap, or nonunion after initial conservative treatment.
Surgical Technique
All procedures were performed by experienced spine-dedicated surgeons, and all patients were treated using the same surgical technique. The procedure is performed in the prone position, with the patient’s head stabilized in a Mayfield head holder. Surgery was performed under general anesthesia with neuromonitoring performed during the entire procedure. Navigation was used (Brainlab AG, Munich, Germany) for assistance during the placement of screws and cages. Surgery is performed through a posterior skin incision in the midline, which is taken down to the atlas (C1) and the axis (C2) via subperiosteal dissection. After exposing the posterior lamina of the vertebrae, intraoperative computed tomography (CT) is performed (Brainlab AIRO, Brainlab AG, Munich, Germany). The accuracy of the navigation system is confirmed against anatomical landmarks. In none of the reported cases, a relevant inaccuracy of navigation was detected. Subsequently, the surgeon brings in the surgical microscope and proceeds to identify the C2 nerve root bilaterally.
To obtain better access to the atlantoaxial joint and to prevent nerve irritation by the C1 screw heads, the C2 nerve root on both sides proximal to the ganglion is first coagulated and then sharply transected using a scalpel. Afterward, the entry points of the C1 lateral mass screws and the C2 pars screws are visualized and marked via the navigation to obtain an optimal screw trajectory.30,31 The holes for the screws are then drilled and tapped using navigated instruments. Thereafter, the joint capsules of the C1/C2 joint are opened bilaterally and decorticated in preparation for insertion of the bilateral atlantoaxial joint spacer (DTRAX, Stoeckli, Feldkirch, Switzerland). For maximum fusion augmentation, an osteoconductive bone void filler demineralized bone matrix (Johnson and Johnson Medical Devices Company, New Brunswick, USA) together with autologous bone graft is also inserted into the joint space. These steps are performed prior to actual screw placement to prevent obfuscation of the C1/C2 joint. Screws are then placed into the prepared screw holes, and an intraoperative low dose CT is performed to verify the implant position. After confirmation of the correct implant position, rods are locked into place under slight compression of the joint space. After locking the rods, additional allograft bone material is added to support the posterior fusion. Finally, the surgical bed is irrigated and checked for hemostasis. Drains are then placed, and the wound is closed in a multilayer fashion. All patients receive a neck orthosis for 6 weeks followed by physiotherapy for an additional 6 weeks. Skin sutures are removed 10 to 14 days postoperatively.
Outcomes
The pain was assessed preoperatively using the visual analog scale (VAS) ranging from “0” (no pain) to “10” (worst pain imaginable). The physical examinations were repeated 14 days postoperatively and afterward depending on the individual course of healing and symptoms without a fixed interval.
To verify the fusion, imaging was performed during follow-up with follow-up intervals planned according to the patient’s symptomology and risk profile. The radiological imaging consisted either of x-rays of the cervical spine in 2 views as well as in flexion and extension or a magenetic resonance imaging (MRI) or CT.32 The criterion for a successful fusion was defined as a visible bony bridging as a direct radiological sign of the bone fusion. An indirect sign of stability was defined as the lack of movement (movement of <5°) in flexion and extension images, the fixed position of the implants, and the absence of radiological signs of loosening.33,34
Statistical analysis was performed using Rx64 version 4.1.1 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 5 patients (2 women and 3 men) were treated with C1/C2 fixation supplemented with a bilateral atlantoaxial joint spacer. The average age was 79.6 ± 5.4 years with an average body mass index of 24.8 ± 3.9. All patients presented with a fracture of the odontoid process as a result of low-energy trauma. Four cases were classified as Anderson D’Alonzo type 2 fractures, 3 of which were further classified as Eysel/Roosen type B fractures, and 1 of which was further classified as Eysel/Roosen type A. The fifth case was classified as Anderson D’Alonzo type 3 (Table 1).35,36
Cohort composition of fracture type and American Society of Anesthesiology (ASA) classification.
Four fractures were initially not dislocated and were therefore treated conservatively with a rigid neck orthosis. These patients eventually underwent surgery due to a significant increase in fracture dislocation during follow-up examination. The fifth case was an acute traumatic odontoid fracture with upfront dislocation. In all Anderson D’Alonzo type 2 fractures, surgical fusion was performed on the atlantoaxial joint only (C1/C2). In the Anderson D’Alonzo type 3 fractures, the surgical stabilization was extended to C3 (C1-C3) in order to reduce the load on the C2 vertebrae already affected by the fracture on the corpus as much as possible. Overall, the average duration of surgery was 187 ± 38.1 minutes, the average duration of all C1/C2 fusions was 184 ± 44 minutes, and the duration of the C1-C3 fusion was 196 minutes. The average blood loss during the procedure was 340 ± 270 mL. The longest follow-up period was 52 months with an average follow-up period of 21.2 ± 17.5 months. The average length of hospital stay was 6.0 ± 3.4 days (Table 2).
Cohort composition by fracture type according to Anderson D’Alonzo classification, fusion levels, blood loss, procedure time, and hospital stay.
Preoperatively, the average VAS for pain was 2.3 ± 3.3, which decreased to a mean of 0.6 ± 0.9 postoperatively. Pre- and postoperatively, no patient showed neurological deficits.
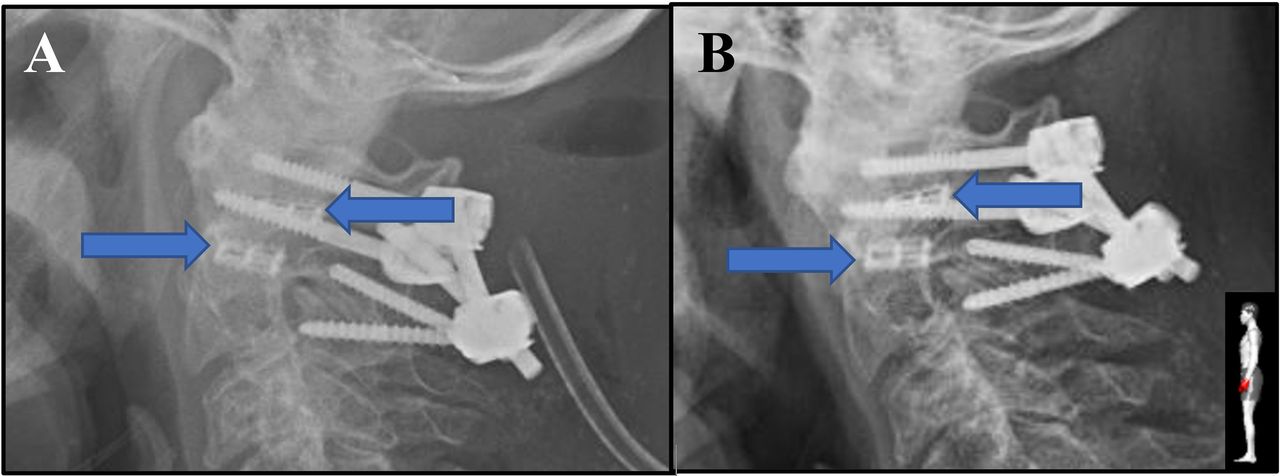
Follow-up imaging included cervical x-ray imaging, cervical CT, or MRI, which demonstrated solid fusion in all cases. None of the follow-up images showed instability, loosening, dislocation of the implants, or other implant failures. No instances of complication were recorded, and no revision surgery was required (Figures 3–6).
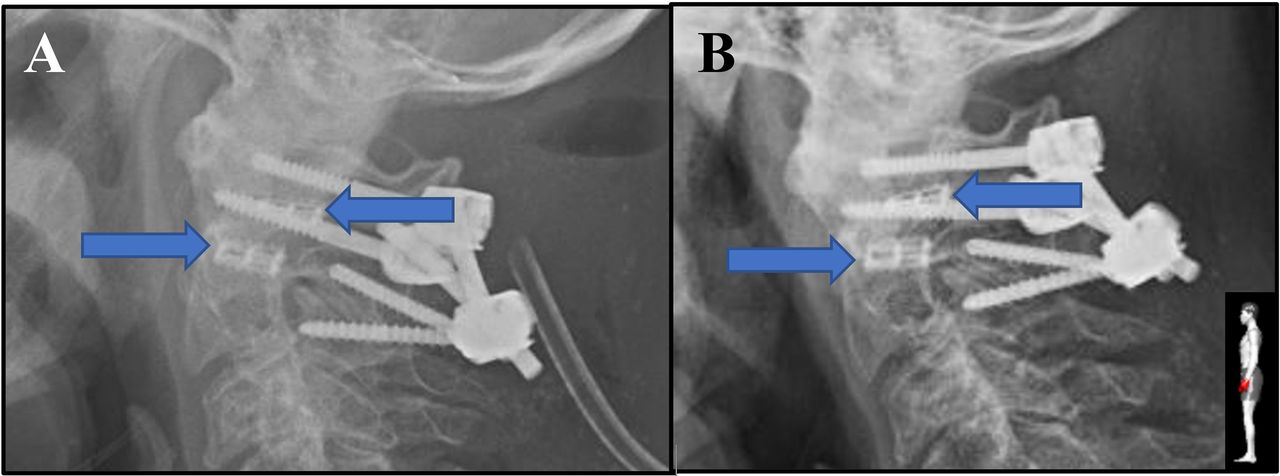
Lateral cervical x-ray images of a C1/C2 fusion with implanted titanium interbody cervical spacer (blue arrows) and posterior fusion; (A) first postoperative day and (B) 8 mo after surgery.

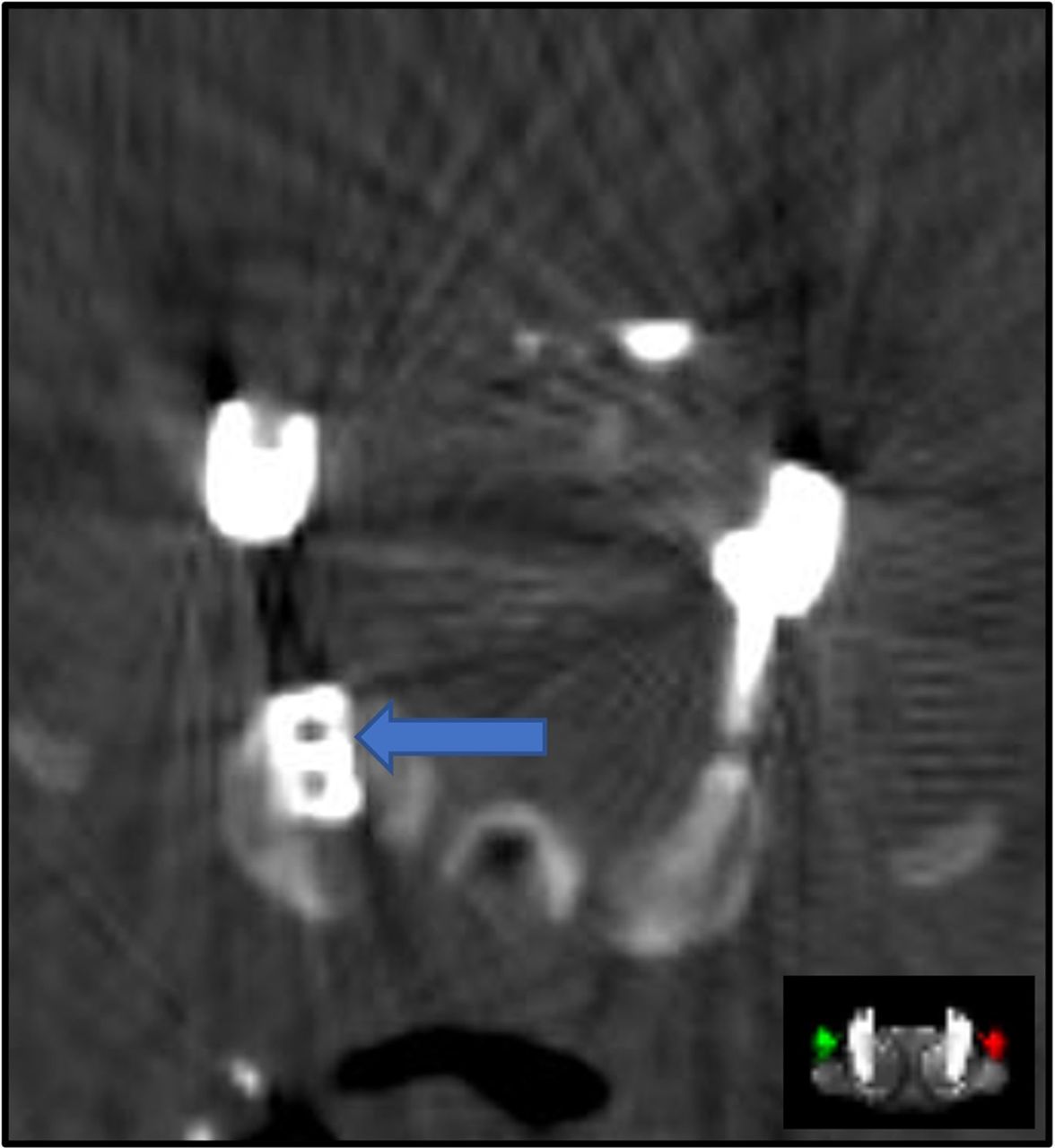
Axial computed tomographic image of C1/C2 fusion with titanium interbody cervical spacer (right side highlighted with blue arrow; left-sided implant not visible) and posterior fusion. The metal artifacts decrease the imaging quality.

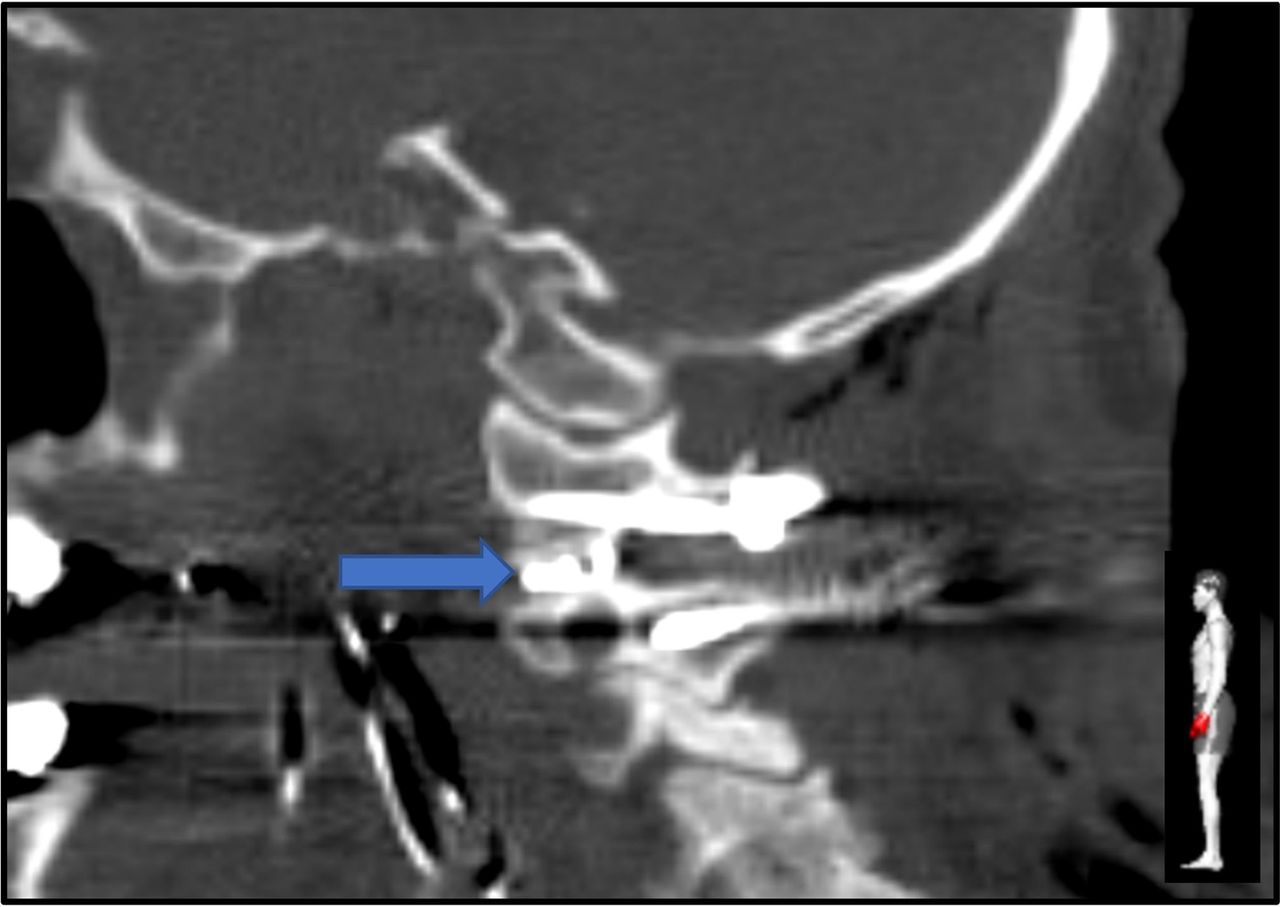
Sagittal computed tomographic image of C1/C2 fusion with titanium interbody cervical spacer (left side highlighted with blue arrow) and posterior fusion. The metal artifacts decrease the imaging quality.

Coronar computed tomographic image of C1/C2 fusion with titanium interbody cervical spacer (highlighted with blue arrows) and posterior fusion. The metal artifacts decrease the imaging quality.
Discussion
Odontoid fractures are a common traumatic disorder, particularly in the elderly.1 The most common cause is a low-energy trauma such as a tripping accident.3 In the past, these fractures were often immobilized with a halo brace as a conservative attempt to achieve bony fusion.37 This imposed significant restrictions on the patient’s lifestyle and represented a great burden, especially on elderly patients. In addition, this approach often resulted in suboptimal rates of fusion, which led to a tendency to avoid this procedure.38,39 With the development of new and improved implants and orthotics, this therapy has been increasingly replaced and is now reserved for only a few special indications.40
Anterior screw fixation remains a common treatment method for patients with nondisplaced Anderson and D'Alonzo type 2 odontoid fractures and favorable anatomy.3,13,41,42 Furthermore, a course of conservative treatment may also be legitimate in cases with favorable fracture patterns and elevated surgical risk.7,13,40,43 Older patients have unique clinical considerations that limit the utility of comparisons to younger patients with similar pathology.6,8–10 In addition, compliance can be limited in elderly patients with cognitive impairments, which enhances the value of treatment paradigms that are durable even in the face of limited compliance.17 Furthermore, studies have shown that longer immobilization in older patients significantly worsens outcomes and so upfront definitive treatment with progression to early rehabilitation should be prioritized.44
The common fusion techniques of the atlantoaxial joint have certain disadvantages in older patients. In the case of a delayed diagnosis or initial conservative treatment of an odontoid fracture that is now well corticated, trans-fracture screw fixation is contraindicated due to the low rates of fusion, especially in the setting of poor bone quality.3,45 Even with effective repositioning of the bone fragments, the chance of successful healing is relatively low and the complication rate is disproportionately high so that the risk profile of the procedure is debatable.46,47
A viable alternative in this case is the transarticular screw connection from anterior (Magerl) or posterior (Babour).46,48 One of the main disadvantages of these procedures is the risk of complications due to screw implantation near sensitive anatomical structures such as the vertebral artery and the risk of injuring them in case of anatomical variations.26,49 Furthermore, transarticular screw implantation is technically demanding and typically requires experienced surgeons. In addition, this procedure keeps the articular surface of the atlantoaxial joint intact, which can impede bony fusion. A further problem may result from the fact that the C1/C2 joint may be degenerated in older patients, and the reduced joint height may cause pain and nerve irritation.28,50 Moreover, the joint is additionally stabilized by sufficient capsule tension, for which reason a restoration of the original height of the joint space is recommended.28,29 This cannot be achieved with the transarticular screw fusion technique alone. There is also evidence from other spinal regions that screws have a reduced load-bearing capacity in poor bone quality and may loosen over time.51
Dorsal fusion in the Goel-Harms technique divides the load over a dorsal screw and rod system and appears to offer greater stability than screw-only constructs, particularly in flexion and extension extremes.26 However, the height of the joint space can be restored to a very limited extent. In addition, the articular surface of the atlantoaxial joint remains unaffected by the procedure, which presents a barrier to optimal fusion rates.20,27 To improve the rate of bony fusion for this challenging patient population, we modified the procedure described by Goel-Harms. The first modification is the transection of the C2 nerve root proximal to the ganglion. This procedure optimizes access to the C1/2 articular space while minimizing postoperative neuropathic pain and has previously been described with good clinical results.52–54 Aryan et al evaluated the procedure in a large study involving 102 patients and concluded that neuropathic pain occurred in only 1 case in the postoperative course.55 Turel et al came to a similar conclusion, investigating this procedure in a smaller cohort of 19 patients and also describing neuropathic pain in the further course in only 1 case.56 These results align with our experience in which no new neuropathic pain occurred postoperatively.
Another modification is the implantation of a spacer into the joint space. It is assumed that the loss of height of the atlantoaxial joint space can lead to the development of neck pain.28,50 In addition, the joint capsule is considered to be important for the stability of the joint and the development of pain.28,50 The implantation of spacers into the joint space has been described several times in the literature. An early description was provided in 2007 by Goel et al who implanted custom-made titanium spacers in a small case series.57 Turel et al published a study where a machined cortical allograft spacer was inserted into the atlantoaxial joint space. With this procedure, they described a fusion rate of 94%.56 Aryan et al also examined the fusion of the atlantoaxial joint after spacer implantation and found a high fusion rate of 98% in their whole cohort, but the subgroup with the spacer implantation was not examined separately.55 To our current knowledge, there is no published description of the implantation of a commercially available titanium implant for the C1/C2 joint in the literature. Titanium implants offer high mechanical stability combined with high biocompatibility.58,59 We considered the DTRAX bilateral atlantoaxial joint spacers, which were originally designed to be implanted minimally invasively into facet joints of the cervical spine, to be the most suitable in terms of size and shape.60
Adding a bilateral atlantoaxial joint spacers may also come with some potential disadvantages. One disadvantage could be that adding a bilateral atlantoaxial joint spacer may increase the procedure time. Depending on the technique, the literature reports procedure times from 144 to 219 minutes for an atlantoaxial fusion.61,62 Compared to the literature, the procedure time of our proposed technique with 187 ± 38.1 minutes does not seem to be that much different than the reported times. Furthermore, we expect the procedural time to decrease for the following cases as we become more proficient in performing this procedure and we pass the learning curve of placing the joint spacer.
Another proposed disadvantage may be that placing a cage would increase the length of hospital stay. The length of hospital stay in our case series was 6.0 days. When comparing these rates with the ones reported in the literature, it does not seem that adding the joint spacer will increase the length of hospital stay.6,63
Another disadvantage may be the increased costs as this procedure requires the implementation of an additional cage, which makes this technique more expensive to perform compared to the technique without the cage. However, our technique could result in a shorter hospital stay and a lower revision rate. The question remains if implementing this joint spacer would lead to an increase in either quality-adjusted life years or effectiveness to make this procedure a more cost-effective procedure. Therefore, further research should explore the cost-effectiveness of this technique as well.
Our case series indicates that fractures and fracture nonunions of the odontoid process in elderly patients can be treated safely and reliably by atlantoaxial fusion with implanting bilateral atlantoaxial joint spacer into the atlantoaxial joint. Our results are promising so far, but our study also has some limitations that need to be acknowledged. First is the sample size of the study. In this study, we presented only 5 cases in which we used the bilateral atlantoaxial joint spacer. This sample size is too low to determine efficacy. This case series does, however, show the safety and feasibility of this technique and therefore justifies further research with larger sample sizes. Another limitation is adhered to the retrospective nature of this study. No patient-reported outcome measures were regularly collected prior to and after surgery, and no prospective imaging protocols were established. This may be explored in further studies with comparative arms.
In our opinion, direct screw fixation of the odontoid process should only be attempted on recent odontoid fractures with good bone quality and without or slight dislocation of the fracture and a realistic prospect of healing. The procedure we described should be considered as an addition to the established fusion procedures of the lateral atlantoaxial joint. We believe this procedure would benefit elderly patients with an unstable odontoid fracture and dislocation in the fracture gap, as well as in cases with a fracture older than 6 weeks. Another proposed indication for our procedure is in patients with an odontoid fracture and either symptomatic atlantoaxial osteoarthritis, collapsed lateral atlantoaxial joint spaces to restore the joint space height, or both. To better quantify the benefit of our surgical procedure, further studies with a larger number of cases and a longer follow-up period are necessary.
Conclusion
Fusion of the atlantoaxial joint with the support of bilateral atlantoaxial joint spacers represents a suitable option for potentially achieving high fusion rates in elderly patients with odontoid fractures. This case series describes the safety and feasibility of this method and the preliminary clinical outcomes. Whether this procedure proves to be a superior alternative treatment for odontoid fractures in challenging patients over the long term will have to be investigated in future studies.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Roger Härtl is a consultant for Ulrich, Brainlab, and DePuy-Synthes and has royalties from Zimmer. The remaining authors have no disclosures.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.