


Abstract
Background Persistent pelvic compensation following adult spinal deformity (ASD) corrective surgery may impair quality of life and result in persistent pathologic lower extremity compensation. Ideal age-specific alignment targets have been proposed to improve surgical outcomes, though it is unclear whether reaching these ideal targets reduces rates of pelvic nonresponse following surgery. Our aim was to assess the relationship between pelvic nonresponse, age-specific alignment, and lower-limb compensation following surgery for ASD.
Methods Single-center retrospective cohort study. ASD patients were grouped: those who did not improve in Scoliosis Research Society-Schwab pelvic tilt (PT) modifier (pelvic nonresponders [PNR]), and those who improved (pelvic responders [PR]). Groups were propensity score matched for preoperative PT and assessed for differences in spinal and lower extremity alignment. Rates of pelvic nonresponse were compared across patient groups who were undercorrected, overcorrected, or matched age-specific postoperative alignment targets.
Results A total of 146 surgical ASD patients, 47.9% of whom showed pelvic nonresponse following surgery, were included. After propensity score matching, PNR (N = 29) and PR (N = 29) patients did not differ in demographics, preoperative alignment, or levels fused; however, PNR patients have less preoperative knee flexion (9° vs 14°, P = 0.043). PNR patients had inferior postoperative pelvic incidence and lumbar lordosis (PI-LL) alignment (17° vs 3°) and greater pelvic shift (53 vs 31 mm). PNR and PR patients did not differ in rates of reaching ideal age-specific postoperative alignment for sagittal vertical axis (SVA) or PI-LL, though patients who matched ideal PT had lower rates of PNR (25.0% vs 75.0%). For patients with moderate and severe preoperative SVA, more aggressive correction relative to either ideal postoperative PT or PI-LL was associated with significantly lower rates of pelvic nonresponse (all P < 0.05).
Conclusions For patients with moderate to severe baseline truncal inclination, more aggressive surgical correction relative to ideal age-specific PI-LL was associated with lower rates of pelvic nonresponse. Postoperative alignment targets may need to be adjusted to optimize alignment outcomes for patients with substantial preoperative sagittal deformity.
Clinical Relevance These findings increase our understanding of the poor outcomes that occur despite ideal realignment. Surgical correction of severe global sagittal deformity should be prioritized to mitigate these occurrences.
Level of Evidence 3.
- adult spinal deformity
- SRS-Schwab modifiers
- pelvic tilt
- pelvic nonresponders
- postoperative alignment targets
Introduction
The pelvis and its movement about the femoral heads is key in regulating the alignment of the sagittal plane. In the spine literature, the rotation of the pelvis around the femoral heads is commonly assessed using the radiographic parameter of pelvic tilt (PT). For patients diagnosed with adult spinal deformity (ASD), evaluation of PT allows for an effective assessment of the pelvis’ compensation for truncal inclination.1 Often, in the setting of high anterior sagittal malalignment, ASD patients will compensate with pelvic retroversion, resulting in high PT.2 When pelvic compensation for deformity is exhausted, compensatory mechanisms may then extend to the lower extremities, resulting in pelvic shift, knee flexion, and ankle flexion.3 As multiple studies show a relationship between greater lumbopelvic malalignment and inferior health-related quality of life, appropriate postoperative reduction of pelvic compensation is an important goal of ASD corrective surgery.4,5
To better optimize surgical planning for operative ASD patients, Lafage et al proposed patient-specific spinopelvic realignment thresholds.6 The formulas published by Lafage et al use patient age and US normative back pain scores to generate ideal postoperative age-adjusted sagittal alignment targets. Their research suggests that to achieve satisfactory clinical outcomes, older patients may not need to meet the same rigorous alignment standards as younger patients. For patients undergoing ASD corrective surgery, more aggressive correction relative to ideal age-specific postoperative alignment has been associated with higher rates of proximal junctional kyphosis, and undercorrection has been associated with greater postoperative recruitment of compensatory pelvic retroversion and lower limb flexion, as well as suboptimal postoperative health-related quality of life.7–9
Despite the increased use and recognition of age-specific alignment targets in ASD corrective surgery, persistent postoperative lumbopelvic malalignment remains a problem, with some studies reporting insufficient PT correction in up to 41% of patients.10 Additionally, other reports suggest that ASD patients may show pelvic nonresponse following surgery, or residual postoperative PT malalignment despite improvements in lumbar lordosis (LL) or sagittal balance.11 To date, it remains unclear whether reaching ideal age-specific postoperative alignment is associated with lower rates of pelvic nonresponse following ASD corrective surgery. This study aims to assess the relationship between ideal pelvic nonresponse, age-specific alignment, and lower limb compensation following ASD corrective surgery.
Materials and Methods
Data Source and Collection
This analysis is a retrospective cohort study of nonconsecutive surgical spine patients visiting a single academic tertiary hospital from 2013 to 2017. All patients underwent standing, biplanar, full body stereoradiographic imaging (EOS imaging, Paris, France), as previously described in the literature, per standard of care.12 The authors obtained approval from the local Institutional Review Board to review and analyze patients in the retrospective database. The Institutional Review Board approved a waiver of consent, due to the minimal study risk and appropriate deidentification and storage of patient data.
Inclusion Criteria
Only adult patients (>18 years) undergoing >4-level fusion for kyphosis, scoliosis, or symptomatic deformity were included for analysis. Patients with missing baseline or early postoperative (<6 months) radiographic imaging, trauma patients, and patients undergoing surgery for spinal tumors, cervical spine pathologies, vertebral fractures, infection, instrumentation failure, pseudarthrosis, or disc herniation were excluded.
Radiographic Assessment
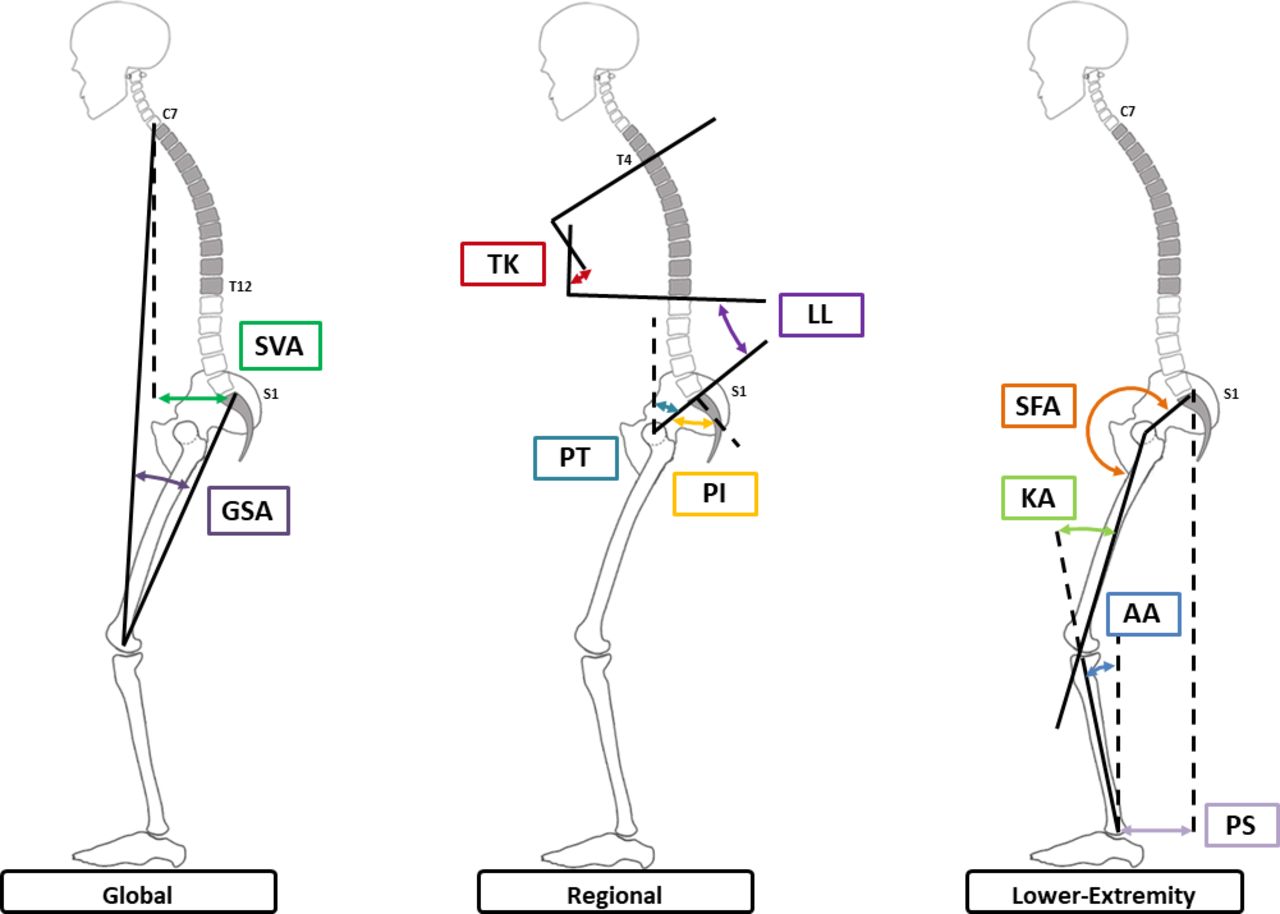
Measurement of all radiographic parameters was conducted using validated software (Surgimap, Nemaris Inc., New York, NY) at a single research center.13 Figure 1 presents a schematic of the global, regional, and lower extremity alignment parameters assessed in this study, measured as previously described in the literature.14 Global alignment parameters included C7-S1 sagittal vertical axis (SVA) and global sagittal angle. Regional alignment parameters included T4-T12 thoracic kyphosis, L1-S1 LL, PT, pelvic incidence (PI), and mismatch between PI and LL (PI-LL). Lower extremity alignment parameters included sacrofemoral angle, knee angle, and ankle angle. Additional radiographic analysis assessed T1 spinopelvic inclination, defined as the angle between the vertical plumbline and the line drawn from the center of T1 and the center of the bicoxofemoral axis.
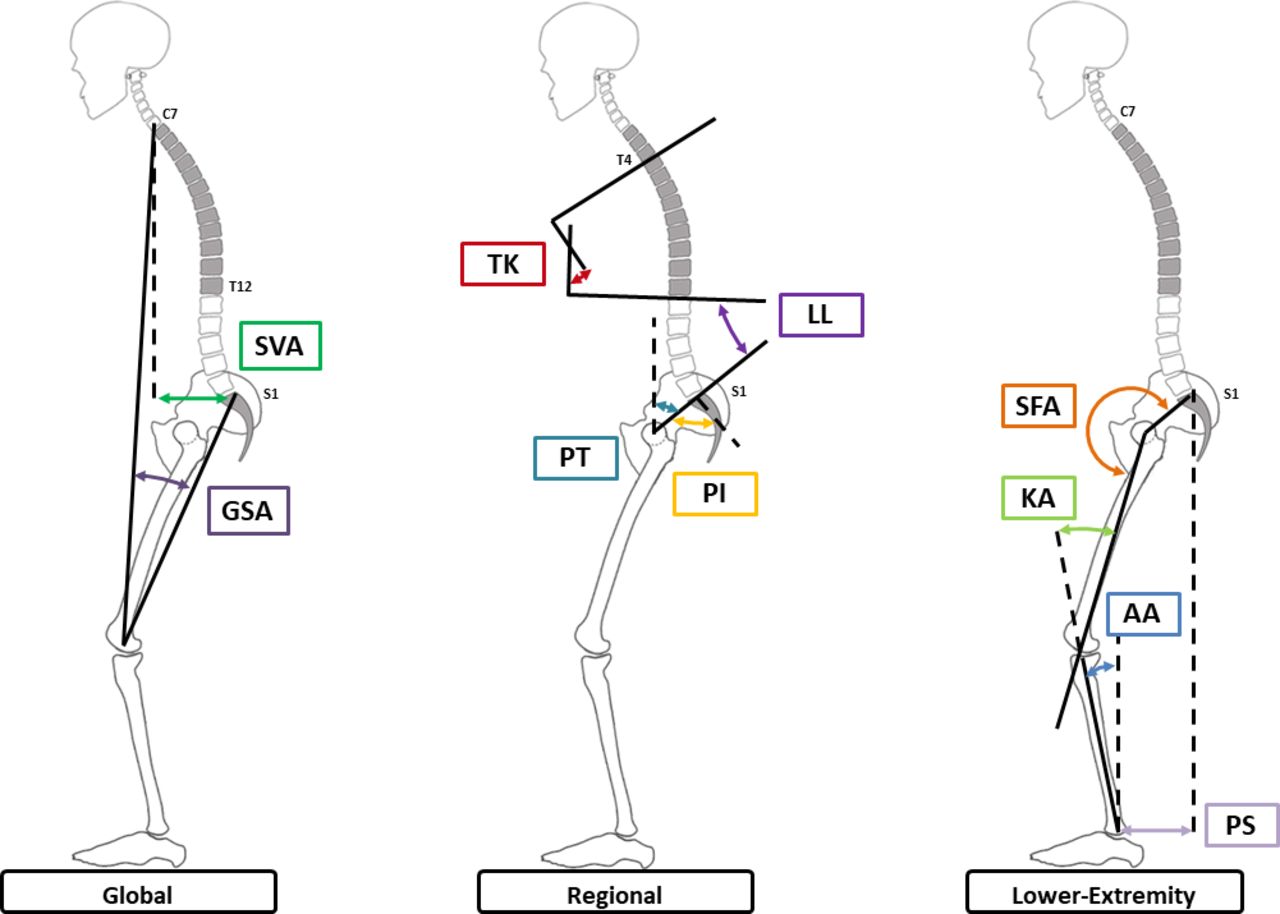
Schematic of global, regional, and lower extremity alignment parameters assessed in this study. SVA, sagittal vertical axis; GSA, global sagittal angle; TK, T4 T12 thoracic kyphosis; LL, L1 S1 lumbar lordosis; PT, pelvic tilt; PI, pelvic incidence; SFA, sacrofemoral angle; KA, knee angle; AA, ankle angle; PS, pelvic shift.
Statistical Analysis
All included patients were assessed for deformity severity at baseline and early postoperative study intervals via the Scoliosis Research Society (SRS)-Schwab ASD classification system.15 Briefly, patients were stratified by increasing deformity severity (0, +, ++) for 3 sagittal alignment modifiers: PI-LL, SVA, and PT. Patients were stratified into 2 groups: those that did not improve in SRS-Schwab PT modifier following surgical intervention (pelvic nonresponders [PNR]), and those did improve (pelvic responders [PR]). To control for differences in baseline deformity between groups, PR and PNR were propensity score matched for baseline PT. Propensity score matching is a logistic regression-based case-control technique commonly used to reduce or eliminate the effects of potential confounding variables in observational data sets.16 Means comparison tests, including Χ 2 and independent samples t tests, assessed differences in demographics, surgical factors, and sagittal alignment between matched groups. Rates of persistent postoperative lower extremity compensation, defined as no pre- to postoperative improvement in lower extremity alignment, were also compared between matched groups via Χ 2 analysis. Changes in alignment within groups were assessed using paired samples t tests.
Subanalysis with Χ 2 tests assessed the relationship between reaching ideal postoperative age-specific alignment targets and rates of pelvic nonresponse.6 Patients were also stratified by deformity severity, per SRS-Schwab ASD classification system modifiers, and rates of pelvic nonresponse were compared across patients overcorrected relative to ideal postoperative alignment, patients undercorrected, and patients matching ideal postoperative alignment via Χ 2 analysis.
Results
Cohort Overview
Prior to propensity score matching, 146 patients met inclusion criteria (70 PNR, 76 PR). Pelvic response groups showed significant variation in baseline PT (PNR: 32.1°± 8.8° vs PR: 20.4° ± 11.7°, P < 0.001), warranting a propensity score matching analysis. Following propensity score matching, 58 patients met inclusion criteria (29 PNR, 29 PR). Matched groups did not differ in baseline PT, demographics, global alignment, regional alignment, or surgical factors (Table 1), although PNR patients did show smaller compensatory knee flexion at baseline (9° vs 14°, P = 0.043). Similarly, at baseline, there were no differences between pelvic response groups in the distribution of SRS-Schwab modifiers for PT (P = 0.286), PI-LL (P = 0.244), or SVA (P = 0.689). Mean postoperative follow-up was 4.6 ± 1.9 months.
Comparison of baseline demographics, surgical factors, sagittal alignment, and lower limb alignment between PNR and PR.
Alignment Outcomes
Although pelvic nonresponse patients did not show pre- to postoperative improvement in SRS-Schwab PT modifier, 58.6% improved in SVA modifier, and 48.5% improved in PI-LL modifier. In contrast, 100% of pelvic response patients improved in SRS-Schwab PT modifier, 85.7% in PI-LL modifier, and 64.3% in SVA modifier. These rates of improvement in SRS-Schwab modifiers significantly lower for pelvic nonresponse patients with respect to PT and PI-LL modifiers, but not SVA (Table 2). Rates of improvement in both PI-LL and SVA modifier did not differ between groups (PNR: 37.9% vs PR: 57.1%, P = 146).
Rates of pre- to postoperative improvement in SRS-Schwab modifiers compared between PNR and PR.
Table 3 compares postoperative sagittal spinal and lower extremity alignment between groups. Notably, PNR showed inferior postoperative lumbopelvic alignment (PT and PI-LL, both P < 0.001). Distributions of postoperative SRS-Schwab modifiers similarly differed between groups for PT (PNR: 0: 0.0%, +: 51.7%, ++: 48.3% vs PR: 0: 65.5%, +: 34.5%, ++: 0.0%, P < 0.001) and PI-LL (PNR: 0: 31.0%, +: 31.0%, ++: 37.9% vs PR: 0: 75.0%, +: 14.3%, ++: 10.7%, P = 0.004), but not SVA (P = 0.493). For pelvic nonresponse patients, these changes in alignment were accompanied by greater compensatory anterior hip extension (pelvic shift: 53 vs 31 mm, P = 0.021).
Comparison of postoperative sagittal alignment and lower limb alignment between PNR and PR.
Changes in Lower Extremity Alignment
Table 4 compares pre- to postoperative changes in lower extremity alignment between pelvic response groups. Pelvic nonresponse patients showed greater persistent compensation for deformity in the lower extremities, as indicated by significantly smaller changes in hip extension (−24 vs −64 mm), pelvic femoral angle (−1.4° vs −3.8°), and global sagittal angle (−3.5° vs −8°), as well as an increase in sacrofemoral angle (2.1° vs −5.3°). Rates of persistent postoperative lower extremity compensation, defined as no improvement in pre- to postoperative alignment, were also significantly higher for pelvic nonresponse patients (Table 4).
Comparison of pre- to postoperative changes in lower limb alignment, as well as rates of residual postoperative lower extremity compensation, between PNR and PR.
Ideal Patient-Specific Alignment and Pelvic Nonresponse
Pelvic nonresponse and pelvic response patients did not differ in rates of reaching ideal age-specific postoperative alignment targets for SVA (PNR: 47.4% vs PR: 52.6%, P = 0.780) or PI-LL (28.6% vs 71.4%, P = 0.066), though patients who matched ideal postoperative PT had significantly lower rates of pelvic nonresponse (25.0% vs 75.0%, P = 0.019).
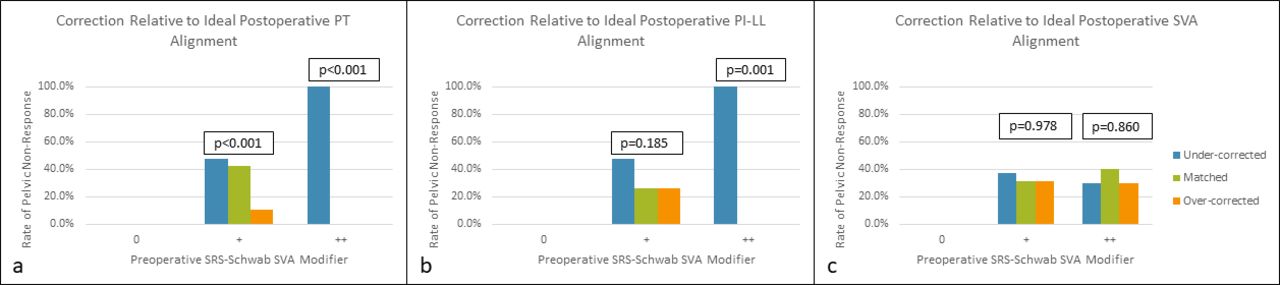
For patients with moderate and severe preoperative SVA deformity (those with SRS-Schwab SVA modifiers + and ++ , respectively), more aggressive correction relative to ideal postoperative PT was associated with the lowest rates of pelvic nonresponse (Figure 2a, P = 0.012 and P < 0.001, respectively). Similar trends were also observed for patients overcorrected relative to ideal age-specific PI-LL alignment (Figure 2b), but not ideal SVA alignment (Figure 2c).
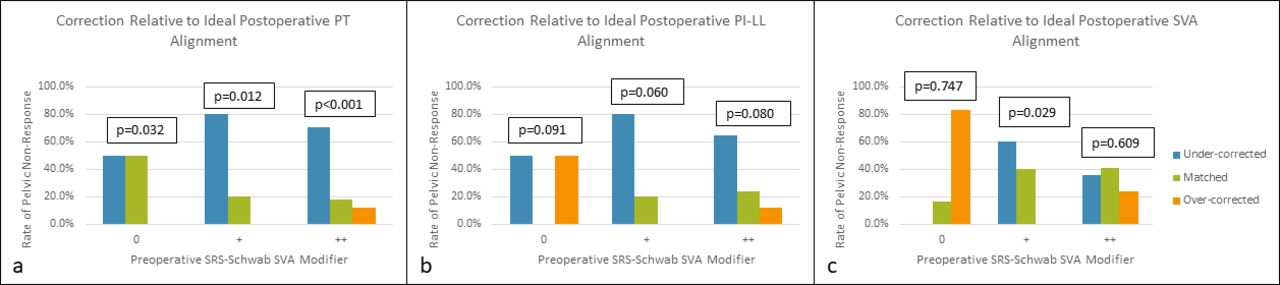
Rates of pelvic nonresponse compared across patients undercorrected relative to ideal age-specific postoperative alignment targets, patients matching ideal targets, and patients overcorrected relative to ideal targets for pelvic tilt (PT) (2a), pelvic incidence and lumbar lordosis (PI-LL) (2b), and sagittal vertical axis (SVA) (2c). These comparisons were conducted within groups of increasing baseline Scoliosis Research Society (SRS)-Schwab SVA modifier severity (0, +, and ++).
For patients with severe preoperative PI-LL deformity (SRS-Schwab modifier ++), lower rates of pelvic nonresponse were also associated with overcorrection relative to ideal postoperative PT (Figure 3a, P < 0.001) and PI-LL (Figure 3b, P = 0.001) targets, but not SVA (Figure 3c).
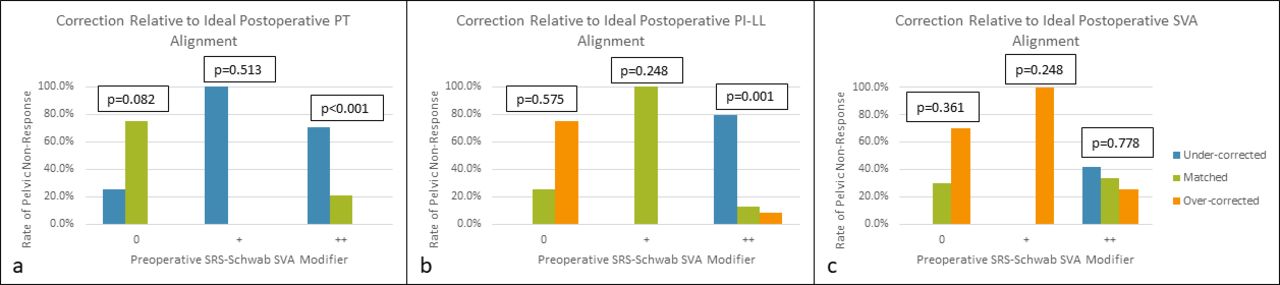
Rates of pelvic nonresponse compared across patients undercorrected relative to ideal age-specific postoperative alignment targets, patients matching ideal targets, and patients overcorrected relative to ideal targets for pelvic tilt (PT) (3a), pelvic incidence and lumbar lordosis (PI-LL) (3b), and sagittal vertical axis (SVA) (3c). These comparisons were conducted within groups of increasing baseline Scoliosis Research Society (SRS)-Schwab PI-LL modifier severity (0, +, and ++).
Similarly, for patients with severe preoperative PT (++), lower rates of pelvic nonresponse were observed in patients overcorrected relative to age-specific ideal postoperative PT (Figure 4a, P < 0.001) and PI-LL (Figure 4b, P = 0.001), but not SVA (Figure 4c, P = 0.860).
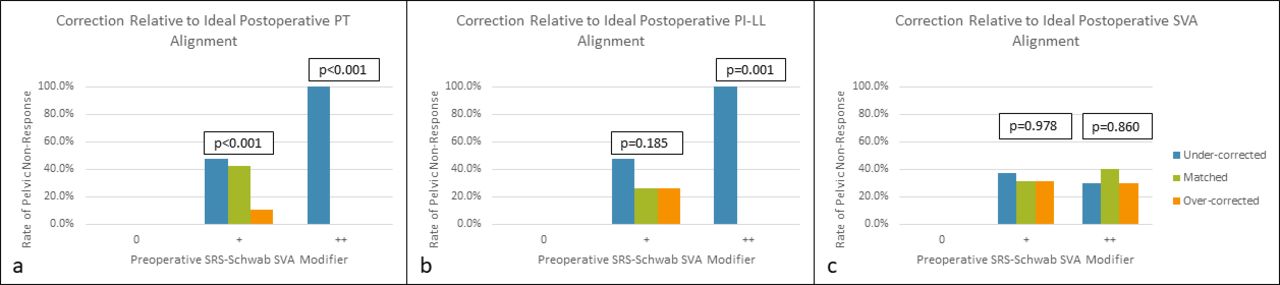
Rates of pelvic nonresponse compared across patients undercorrected relative to ideal age-specific postoperative alignment targets, patients matching ideal targets, and patients overcorrected relative to ideal targets for pelvic tilt (PT) (4a), pelvic incidence and lumbar lordosis (PI-LL) (4b), and sagittal vertical axis (SVA) (4c). These comparisons were conducted within groups of increasing baseline Scoliosis Research Society (SRS)-Schwab PT modifier severity (0, +, and ++).
Case Examples
Figure 5 presents case examples of a pelvic nonresponse and a pelvic response patient. At baseline, the “pelvic nonresponse” patient was 72 years old and presented with severe sagittal malalignment, as assessed by SVA (175 mm, SRS-Schwab Modifier: ++), PI-LL (58°, ++), and PT (43°, ++). This patient underwent posterior fusion from T4 to pelvis, including a pedicle subtraction osteotomy at L3. At 6 months postoperative, the “pelvic nonresponse” patient was undercorrected relative to age-specific alignment targets for SVA (88 mm, +), PI-LL (35°, ++), and PT (35°, ++). The “pelvic response” patient was also 72 years old at baseline and presented with severe malalignment for SVA (124 mm, ++), PI-LL (27°, ++), and PT (24°, +). This patient underwent posterior fusion from T10 to sacrum, including wedge resection osteotomies at L3-L4 and L4-L5. At 6 months postoperative, this patient was overcorrected relative to ideal age-specific PI-LL (−3°, 0) and showed no little residual pelvic compensation (PT: 14°, SRS-Schwab modifier: 0).

Case examples showing preoperative and 6 months postoperative standing lateral radiographs of a pelvic nonresponse (left) and a pelvic response patient (right).
Discussion
Excessive pelvic retroversion, as assessed by PT, is a key indicator of spinopelvic malalignment, and has previously been associated with increased levels of low back pain and disability.1,17 For ASD patients presenting with substantial impairments in health-related quality of life, PT values greater than 20° may constitute an indication for surgical intervention.18 Importantly, operative ASD treatment cannot directly change PT; instead, satisfactory restoration of LL in relation to a patient’s PI reduces the need for pelvic compensation, effectively resulting in PT reduction. Despite recent improvements in the understanding of alignment objectives for patients undergoing deformity corrective surgery, the literature shows examples of patients who continue to have postoperative pelvic compensation, despite achieving physiologically acceptable truncal inclination following surgery.19 This residual postoperative compensation for deformity—or pelvic nonresponse—remains a problem for ASD patients and may be associated with inferior clinical outcomes. The results of our study showed an appreciable number of patients with both residual postoperative pelvic and lower extremity compensation following ASD corrective surgery. Additionally, our study found that for patients with substantial preoperative sagittal deformity, rigorous correction with respect to ideal age-specific alignment is associated with lower rates of postoperative pelvic nonresponse.
In our population of 146 surgical ASD patients, an alarmingly high number of 70 patients qualified as PNR (47.9%), showing no pre- to postoperative improvement in SRS-Schwab PT modifier. This rate of pelvic nonresponse is comparable to previously published studies, which show insufficient or no postoperative PT improvement in 41% to 75% of surgical ASD patients.20,21 Perhaps most importantly, however, the results of this study reveal a novel finding: that for patients with moderate to severe preoperative truncal inclination (SRS-Schwab modifiers + and ++ ), more lumbar correction relative to previously published age-specific ideal postoperative alignment targets is associated with lower rates of pelvic nonresponse following surgery.
Previous studies in the ASD literature demonstrate a clear relationship between PT and health-related quality of life. In a prospective study of 125 adult deformity patients, Lafage et al showed significant correlations between greater baseline PT values and inferior scores on several measures of pain and disability, including the Oswestry Disability Index (ODI), the SRS questionnaire, and the Short Form 12-item survey.1 Regression analysis conducted by Schwab and colleagues similarly showed a relationship between greater baseline PT and inferior ODI scores in a prospective population of 492 ASD patients.22 Additional research shows that pre- to postoperative reductions in PT, as assessed by SRS-Schwab modifier, are associated with significant improvements in overall ODI and SRS scores.21 As a whole, this body of literature effectively highlights the clinical importance of adequate PT correction in ASD corrective surgery. The results of our study suggest that to achieve adequate postoperative PT alignment, patients with substantial baseline sagittal deformity may warrant more aggressive surgical correction relative to their ideal age-specific postoperative alignment targets.
This is not to understate the importance of matching age-specific postoperative alignment targets in surgery for ASD. Particularly for older patients, more aggressive correction relative to ideal age-specific PI-LL alignment is associated with higher rates of complications like proximal junctional kyphosis (PJK).23 Interestingly, however, although undercorrection relative to ideal age-specific postoperative alignment has been associated with inferior 2-year postoperative clinical outcomes, recent research shows no difference in clinical outcomes between patients who match ideal alignment targets, and patients who are overcorrected.1
Differences in clinical outcomes between these surgical correction groups have not been explored in context of pelvic nonresponse—this topic warrants attention in future studies. Still, given the comparable clinical outcomes of patients matching and overcorrected relative to age-specific targets, for ASD patients who have a low risk of developing PJK, greater surgical correction relative to age-specific alignment may be an effective way to mitigate pelvic nonresponse. Our results suggest that for severely deformed patients able to tolerate rigorous correction with respect to medical and PJK risk, ideal age-adjusted alignment targets may need to be adjusted to optimize surgical outcomes. Future studies could identify new target alignment thresholds in low-risk cohorts to improve pelvic response and correlate these thresholds with patient-reported outcomes. This relationship, however, remains speculative, and additional research is also necessary to assess other potential factors associated with residual lumbopelvic compensation following ASD corrective surgery. A better appreciation of the factors that influence the degree of correction appropriately could further individualize surgical planning to decrease PJK development and diminish pelvic nonresponse.
A key limitation of this study is the lack of data tracking both patient health-related quality of life and PJK outcomes. Given the previous body of literature showing an association between PJK and more aggressive surgical correction relative to age-specific alignment targets, it is important that future studies investigate the relationship between PJK, pelvic nonresponse, and age-specific alignment, as well as the relationship between pelvic nonresponse and clinical outcomes. Another important limitation of this study is the lack of data tracking the presence of concurrent hip conditions, which may affect pelvic range of motion, and consequently, compensation for deformity. This study is also limited by the retrospective single-center study design, which allows for the possibility of selection bias and reduces the generalizability of our findings. Our study also does not account for surgeon-specific preoperative goals for ASD correction. Despite these limitations, we maintain that this study is an important step toward understanding the best surgical plan to optimize alignment outcome following surgery for ASD.
Conclusion
In this population of surgical ASD patients, the rate of residual postoperative pelvic retroversion, or pelvic nonresponse, was 49.7%. For patients with moderate to severe baseline truncal inclination, this study showed that more aggressive surgical correction relative to ideal age-specific PI-LL was associated with lower rates of pelvic nonresponse. These results suggest that for patients with substantial preoperative sagittal deformity, existing postoperative alignment targets may need to be adjusted to optimize alignment outcomes.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Peter G. Passias reports other financial or material support from Allosource; research support from the Cervical Scoliosis Research Society; paid presenter or speaker for Globus Medical and Zimmer; paid consultant for Medicrea, Royal Biologics, SpineWave, and Terumo. Daniel Sciubba reports paid consultant for Baxter, DuPuy Synthes, K2M, Medtronic, Nuvasive, and Stryker. Themistocles Protopsaltis reports IP royalties from Altus; paid consultant for Globus Medical, Medicrea, Nuvasive, and Stryker; stock or stock options from Spine Align and Torus Medical. Aaron J. Buckland reports paid consultant for Nuvasive and Stryker. Frank J. Schwab reports research support from DePuy Synthes; paid consultant for Globus Medical, K2M, Medicrea, Medtronic, and Zimmer; paid presenter or speaker for Globus Medical, K2M, Medtronic Sofamor Danek, and Zimmer; IP royalties from K2M, Medtronic Sofamor Danek, and Zimmer; research support form Nuvasive and Stryker; board or committee member for the Scoliosis Research Society and the International Spine Society Group. Renaud Lafage reports stock or stock options from Nemaris. Virginie Lafage reports paid presenter or speaker for DePuy Synthes and The Permanente Medical Group; editorial or governing board for European Spine Journal; paid consultant for Globus Medical; IP royalties for Nuvasive; and board or committee member for the International Spine Study Group and the Scoliosis Research Society. The remaining authors have no disclosures.
Disclosures Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article. For disclosures outside the current work, please see below.
Ethics Statement Institutional Review Board approval was obtained prior to patient enrollment. All patients provided informed consent.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.