


Abstract
Background Lumbar synovial cysts are thought to signal facet joint degeneration and possible instability, leading some surgeons to routinely add a fusion to the decompressive procedure. These recommendations were formulated before the minimally invasive surgery (MIS) era. Here we describe our outcomes in surgical treatment of lumbar synovial cysts using MIS techniques.
Methods The charts of 117 patients who underwent MIS resection of a synovial cyst were retrospectively reviewed. All surgeries were carried out in an ambulatory surgery center (ASC). The preoperative and postoperative visual analog scale (VAS) and Oswestry Disability Index (ODI) were collected prospectively. Surgical variables and complications were also reviewed. The subset of 48 patients followed for over 1 year was analyzed, and the outcome of patients with and without a spondylolisthesis was compared.
Results A total of 117 patients underwent MIS decompression of a synovial cyst. Postoperative follow-up ranged from 3 to 12 months. There were no perioperative complications or 30-day readmissions. Preoperative mean VAS and ODI were 6.2 and 46.7. The postoperative VAS and ODI declined by 3.0 and 22.0 over a mean of 125 days. There were 48 patients with a mean follow-up of 15 months, where the VAS and ODI declined by 2.8 and 22.5, respectively. In this subset, the 23 patients with a spondylolisthesis (all grade 1), were compared to the 25 patients without. The spondylolisthesis group VAS and ODI, preoperatively and postoperatively, declined by 3.3 and 26.1, respectively, while the nonspondylolisthesis group declined by 2.6 and 19.2. These results for each group in this study surpass the standard for a minimal clinically important difference.
Conclusions Patients with lumbar synovial cysts may safely undergo MIS decompression in an ASC setting, with a low risk of perioperative complications. The reduction in pain and disability is meaningful in the short term and sustained over the next 15 months. The presence of a grade 1 spondylolisthesis did not adversely impact patient outcomes over this time period. For patients undergoing MIS resection of a lumbar synovial cyst, with either the presence or absence of a grade 1 spondylolisthesis, the mandatory inclusion of a concomitant spinal fusion is brought into question.
Clinical Relevance This work is among the largest series of synovial cysts published in which the MIS technique is applied. It demonstrates the efficacy of the procedure, along with its safety and appropriateness for performance in an ambulatory care setting. Moreover, it describes the outcomes using the patient-reported outcome measures VAS and ODI. Finally, the long-term outcomes of patients with and without spondylolisthesis are compared, further supporting the position that when performing a decompression of a synovial cyst with an associated grade 1 spondylolisthesis, a concomitant fusion may not always be necessary.
Level of Evidence 4.
INTRODUCTION
Lumbar synovial cysts are well-described lesions capable of causing back or radicular leg pain. In a study of lumbar magnetic resonance imaging performed for the indication of back or radicular pain, synovial cysts were seen in 9.6% of the scans, with 2.3% of the cysts protruding into the spinal canal.1
Synovial cysts are associated with degenerated facet joints and may arise from periarticular tissues.2 Historically, these lesions were classified as either true synovial cysts if a synovial lining was present, or ganglionic pseudocysts if the synovial lining was absent.3 Because of the varying histopathologies, these lesions are sometimes referred to as juxta-articular cysts. Recently, it has been reported that a large proportion are not synovial in derivation, but result from pseudocystic degeneration of the ligament flavum.4 For the present, these distinctions do not have relevance for management of a patient harboring a synovial cyst. Nevertheless, these lesions are thought to signal facet joint degeneration and possible instability. Because of possible instability, some surgeons recommend routinely adding a fusion to the decompressive procedure.5
The initial treatment for patients with symptomatic synovial cysts generally consists of conservative measures. Should these measures fail, then more invasive treatments may be required. Aspiration of the cyst under computed tomography guidance has been described. However, the recurrence rate, with a subsequent need for surgery, can be in excess of 50%.6 When excision of a synovial cyst is indicated, various surgical approaches have been advocated. Early treatments have included hemilaminectomy, total laminectomy, laminotomy, and laminectomy with fusion.
In 2004, the first series using minimally invasive surgery (MIS) techniques for excision of a synovial cyst was published.7 In a comparison of minimally invasive vs open surgery, Vergara concluded that MIS treatment was more effective than open surgical techniques for relieving radicular symptomology.8 Furthermore, they deemed the MIS techniques to be better tolerated by the patients and have potential cost savings due to decreased length of hospital stay. Last, by preserving midline stabilizing structures and muscular attachments, thereby reducing the risk of destabilizing the spine, the use of MIS techniques may obviate the need for fusion and instrumentation. Here, we present our experience with the MIS of lumbar synovial cysts, with and without an associated spondylolisthesis, in the exclusively outpatient setting of an ambulatory surgery center (ASC).
MATERIALS AND METHODS
The patients were referred to a large multispecialty group private practice, specializing exclusively in spinal MIS techniques. As part of an internal review of surgical outcomes, this retrospective analysis was undertaken. Patients were identified, and the data were collected via a search of the institution’s electronic health record database from the period of July 2014 to December 2016. The inclusion criteria required each patient to have (1) evidence of a synovial cyst and associated stenosis on magnetic resonance imaging or computed tomography exam, (2) radicular symptoms concordant with radiological findings, (3) failed at least 6 weeks of conservative care, and (4) completed preoperative and postoperative patient-reported outcome measure (PROM) surveys.
The data for the PROM were collected at the initial clinical intake where the patient manually filled out surveys for visual analog scale (VAS) and Oswestry Disability Index (ODI). Postoperatively patients were contacted at 3 and/or 6 months via email with requests to follow links to Health Insurance Portability and Accountability Act compliant online VAS and ODI surveys. At 1 year postoperatively, patients were again contacted via a phone call and email, with a possible supplemental call at 2 years.
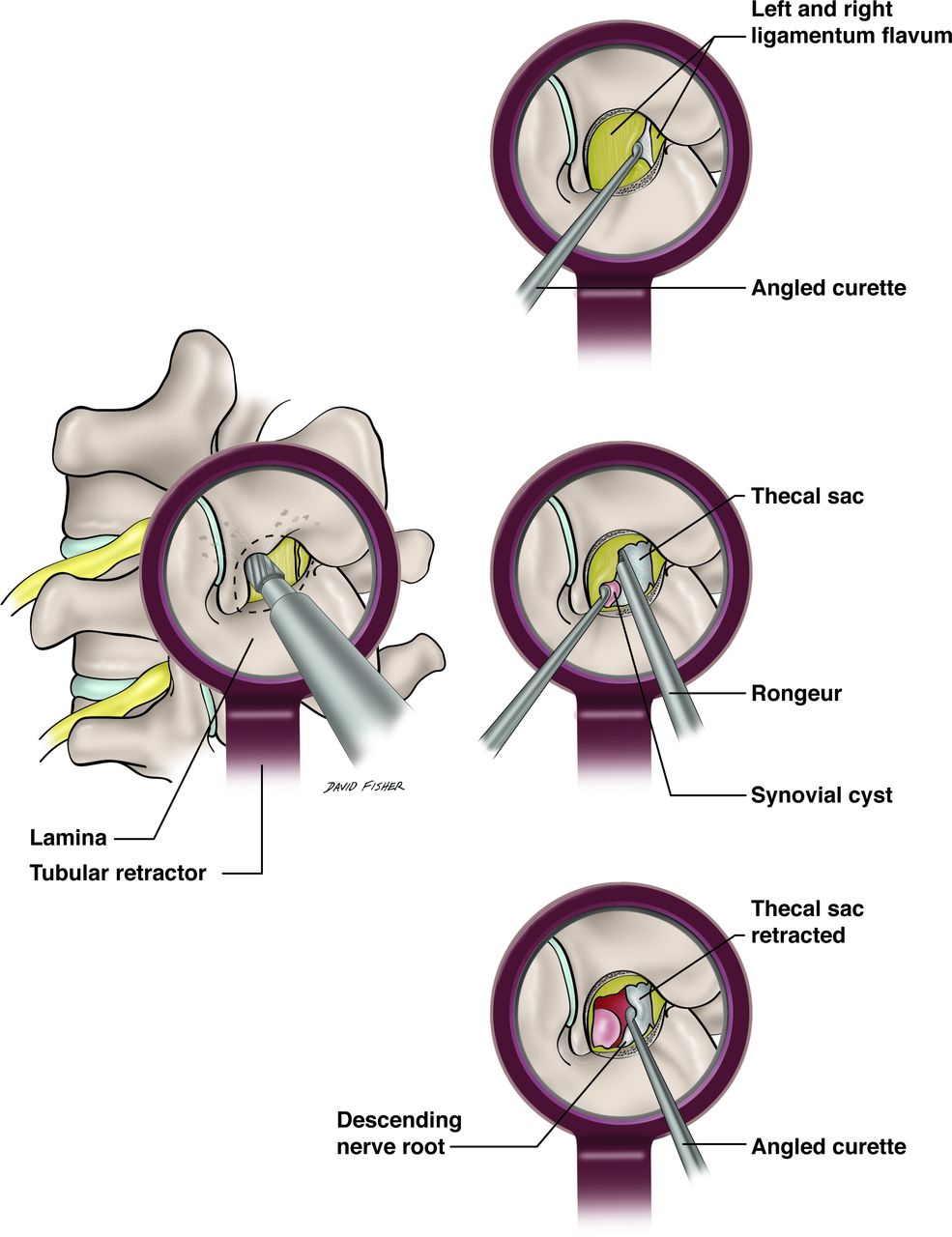
All surgeries took place in multiple associated ASCs, without 23 hours monitoring capabilities. Multiple neurosurgeons or spine fellowship trained orthopedic surgeons performed the procedures, using MIS techniques described elsewhere.9,10 All patients were operated upon in the prone position under general anesthetic. After a sterile skin prep, C-arm fluoroscopy was used for localization of the appropriate spinal level. A small skin incision was then made with a no. 15 blade. Following sequential dilation of the paraspinal muscles, a 14- to 18-mm tubular retractor was docked at the laminar facet complex with fluoroscopic confirmation of the position. The choice of using either the operating microscope or an endoscope, for illumination and magnification, was left to surgeon preference. A laminotomy, foraminotomy, and decompression of the nerve root were performed with high speed drills and rongeurs. Cyst excision and facet debridement were performed in all cases. The decompression included a partial medial facetectomy and, as necessary, undercutting of the superior articular process to assist in complete decompression of the nerve root. The technique for microdissection and cyst removal varied with the individual surgeon. The lead authors’ technique for microdissection involved exposing the ligamentum flavum via laminotomy and medial facetectomy sufficient to expose the entirety of the cyst and some surrounding normal dura (Figure). A plane between the ligamentum flavum and the dura was developed at a location peripheral to the cyst. This plane was generally initiated at the midline where the ipsilateral and contralateral ligamentum flavum abut, or cephalad to the disk space where the ligament initiates. Working toward the presumed cyst position the dura is separated from the ligament with a small angled curette. The ligament is then removed with rongeurs in a piecemeal fashion until the cyst is identified. The plane between the cyst and the normal dura is then developed with microdissection until the dura of the thecal sac and descending nerve root can be mobilized and protected, thus minimizing the risk of incidental durotomy. The cyst is then removed with rongeurs and curettes in a piecemeal fashion, and the facet is debrided. The operative bed is then inspected and explored visually and with dissectors to ensure that the thecal sac and nerve root are fully decompressed. Following antibiotic irrigation some patients had steroid dripped over the nerve root. The incision was then closed.

Left—view through tubular retractor of laminotomy. Right upper—initiation of dissection of the ligamentum flavum from the dura using an angled curette. The safe zone is the area where the left and right ligaments oppose. Right middle—after dissection with a curette to ensure adhesions are lysed, the ligament is removed piecemeal with a rongeur. Right lower—the thecal sac and descending are mobilized and protected prior to cyst removal.
In some patients thermal ablation, akin to radiofrequency ablation, of the periosteal nervous innervation of the contralateral facet joint was simultaneously performed. This technique involved nicking the skin, then percutaneously docking a metal 1-mm tube on the facet under fluoroscopic guidance. A holmium laser fiber was placed through the tube onto the posterior facet surface. The laser was then activated, and the fiber advanced along the entire posterior facet surface by moving the tube slightly, until 400 J of energy were delivered. The laser fiber was withdrawn, and 2 cc of a dilute solution (40 mg of methylprednisolone diluted in 10 cc of 0.25% Marcaine) is placed through the tube onto the ablated joint.
No concomitant spinal fusions were performed on these patients. Patients were then recovered in the postanesthesia care unit until discharge criteria were met.
Primary endpoints included both surgical outcome measures and PROM. Surgical parameters were extracted from electronic health records for each patient. A single PROM consisted of the VAS for pain measurement. Here the patient was asked to rate their pain intensity on a horizontal linear scale of 0 to 10. The ODI was used for disability measurement. A student’s t test was conducted to determine if there were significant differences in pain and disability before and after surgery. Following the initial collection, these data were then pooled, removing any patient identifiers. Shortly thereafter the institution became financially insolvent and closed, thus prohibiting further access to any patients’ medical records or additions to these data. The only data available for analysis are the patient nonidentifiable pooled data. Given that well-established surgical techniques were exclusively used, and that no patient identifiers were present in these pooled data, the institutional review board deemed this study as “Not Human Subjects Research.”
RESULTS
A total of 117 patients were surgically treated (Table 1), with a mean follow-up of 125 days (range 90–387 days, SD 64). There was a male to female predominance of 63 to 54. The group had a mean age of 59 years (range 28–91 years, SD 11) and a mean body mass index of 31 (range 19–51, SD 6). Twelve of the patients (10%) had prior surgery at the index level.
Patient variables and outcomes (N = 117).
The average length of surgery was 72 minutes (range 26–215 minutes, SD 35) with the average estimated blood loss of 52 mL (range 5–950 mL, SD 101). No intraoperative complications occurred. Specifically, there were no dural tears. There was a single event of excessive blood loss of 950 mL, but no transfusion was given, and the patient sustained no significant effects. In the ASC, a cell-saving device was readily available; however, it is uncertain if it was used in this case. The postoperative time to dismissal from the ASC was just over 2 hours (range 69–294 minutes, SD 36). All patients were discharged from the ASC, including the patient with excessive blood loss. There were no perioperative complications, which would include delayed Cerebrospinal fluid (CSF) leaks, infections, or new neurological deficits. Nor were there any 30-day readmissions. No patient subsequently underwent a lumbar fusion during this follow-up period.
Surgical intervention leads to significant improvements in PROM. The preoperative mean VAS declined from 6.2 to 3.1 on follow-up (∆3.1, 50%). While the preoperative ODI declined from 46.7 to 24.7 (∆22.0, 47%).
A subset of 48 patients followed for at least 1 year had a mean follow-up of 15 months (Table 2). The mean age (62 years) and body mass index (30) were similar to the entire cohort of 117 patients. In these 48 patients, the VAS declined from 5.8 to 2.8 (∆3.0, 50%), and the ODI declined from 46.8 to 24.3 (∆22.5, 48%). These declines in PROM were similar to those of the entire cohort, which had a mean follow-up of 10 months.
Patients followed for more than 1 y (N = 48).
Within this subset of 48 patients, 23 patients had a spondylolisthesis at the index level, with all being grade 1 (Table 3). Subset analysis was performed on this group, comparing the 23 patients with a spondylolisthesis to the 25 patients without. In the spondylolisthesis group, the VAS declined from 6.0 to 2.7 (∆3.3, 55%), while the ODI declined from 50.5 to 24.4 (∆26.1, 52%). The group without a spondylolisthesis showed a VAS decline from 5.5 to 2.9 (2.6, 47%), and an ODI decline from 43.4 to 24.2 (∆19.2, 44%).
Spondylolisthesis outcomes followed for more than 1 y (15 mo mean follow-up).
DISCUSSION
Synovial cysts of the lumbar spine are a well-documented phenomenon in patients with symptomatic radiculopathy.1,11 When appropriate, cysts are typically excised surgically in order to decompress the affected nerve root. Extensive decompressions and instrumented fusions are commonly performed, though practice patterns may be shifting away from larger, more invasive surgeries in favor of minimally invasive options, often without fusion or instrumentation.7,8,12
Concurrent with the paradigm shift toward less invasive surgical techniques is a shift away from inpatient stays to more outpatient, ambulatory services.13–15 Smaller incisions often have less associated postoperative pain, requiring fewer pain medications and shorter return-to-mobility periods.9 In order to be considered a candidate for surgery at an ASC, the expected postanesthesia recovery should be minimal; the patient is expected to be at their preoperative level of mobility within a few hours, pain should be controlled by oral medications only, and they should not have any neurologic, hemodynamic, or cardiopulmonary instability. These expectations were achieved for all patients in this study. The length of the surgical procedure averaged 72 minutes, and the average time to recover in the postanesthesia care unit was approximately 2 hours. No patient required overnight observation or transfer from the ASC to an inpatient setting. Additionally, there were no 30-day readmissions, which would have driven up the total cost of the problem management. In November 2019, over 3 years after our patients received surgery at the ASCs, the Centers for Medicare and Medicaid Services changed the requirement for the surgical resection of lumbar synovial cysts (Current Procedural Terminology code 63267) from an inpatient-only procedure to one that is appropriate for an ASC. Our results give further evidence for support of that change, demonstrating the safety and efficiency of MIS resection of lumbar synovial cysts in an ambulatory care setting.
Patient demographics in this study differed slightly from some of the findings established in prior studies. Lumbar synovial cysts were found in this study to be more common in men, which contradicts the female predominance published in some other studies, though the age at presentation was in accordance with those studies.12,16,17
The safety and effectiveness of MIS for synovial cysts have been well demonstrated and was again supported by the findings in this study.7,8,11,12,18 There were no perioperative complications—specifically, there were no CSF leaks or infections. This compares favorably to the CSF leakage rate of 3.3%, and the infection rate of 0.9% reported in a recent literature review involving 1172 surgical cases.11 As our institution involved multiple surgeons performing the MIS procedures, with their varying techniques, the reason for the low CSF leakage rate can only be speculated upon. As there was no control group in this study, the low rate may be a chance occurrence. On the other hand, it may be related to the institution’s surgeons performing exclusively MIS spinal surgery. The surgeons accumulate a large operative experience and are well past the learning curve necessary for safely performing decompressions through a tubular retractor. Additionally, the facility does not participate in the training of residents, further reducing complications associated with limited experience of the operating surgeon.
This study demonstrates the safety and short-term efficacy (10-month mean follow-up) of the procedure, as the VAS improved 3.1 points (50%) and the ODI improved 22.0 points (47%). This short-term improvement was maintained over time, as shown in the subset of 48 patients followed for a minimum of 1 year (mean follow-up of 15 months). This group improved in both measured patient outcomes: the VAS declined by 2.9 (50%) and the ODI declined by 22.6 (48%). The minimum clinically important difference (MCID), representing the smallest clinically relevant change in a PROM, has been used to determine whether interventions benefit patients.19 Recently, it has been shown that a 30% reduction in PROM from baseline to 12 months after surgery is a valid threshold for measuring clinical improvement in a broad spine surgery population.19 Our results, using MIS techniques in an ambulatory surgery setting, surpass the MCID threshold of 30% for evidence of a meaningful clinical improvement in our patients. However, our mean long-term follow-up is 15 months, which falls short of the benchmark of 2 years’ time for evaluating surgical outcomes.
Some authors have argued that the spine is destabilized by resection of a facet adjacent lumbar synovial cyst, thus indicating for the use of fusion, and possible instrumentation, in those cases.20 More recently, it has been shown that MIS techniques preserve much of the surrounding musculature and ligamentous complexes, resulting in maintained postoperative stability, thus diminishing the need for fusion.12,16,18,21 As noted above, the short-term improvement in PROM was maintained over 15 months. Additionally, during the follow-up period, no patient, with or without a spondylolisthesis, required a return to surgery for a spinal fusion. This study demonstrates the lasting efficacy upon pain and disability for MIS decompression of synovial cysts without concomitant fusion for at least 15 months.
An unknown number of patients received contralateral facet joint thermal ablation at the time of surgery. Due to the closure of the institution where the surgery was carried out, retrieving these data is not feasible. The effect of thermal ablation can be comparable to that of radiofrequency ablation, in that the nervous innervation of the facet joint is damaged by heat. In a meta-analysis of radiofrequency ablation trials for lumbar facet joint pain, Leggett et al found the studies reporting only modest improvements in pain scores, with no randomized clinical trials measuring outcomes past 12 months.22 Given these uncertainties it is unknown if the addition of contralateral facet joint thermal ablation impacted the PROM of our patients, independent of the decompressive surgical treatment. However, it should be pointed out that surgical outcome studies generally have not specified whether or not rhizotomies have been performed near the time of surgery. Thus, the potential effect of this treatment modalities impact on outcome is not fully known. Extrapolating this information, we believe that the addition of a contralateral facet ablation at the time of cyst removal probably did not significantly affect the outcome analysis, particularly in the data subset collected after 1 year.
The demonstrated long-term improvements in PROM occurred regardless of the presence of a grade 1 spondylolisthesis. The group of patients with a spondylolisthesis prior to surgical intervention had improvements in their VAS and ODI of 3.3 (55%) and 26 (52%), respectively, while the patients with no listhesis had improvements of 2.6 (47%) and 19.2 (44%). These data do not permit determining if the differences between the groups with, and without, a spondylolisthesis approach statistical significance. However, it is evident that the pain and disability outcomes in the group with a spondylolisthesis were at least as good as those without the presence of a spondylolisthesis. These improvements were maintained throughout the extent of the follow-up period and surpass the established MCID threshold of 30% to show clinical patient benefit. These data give further support to the position that in instances of a patient with a grade 1 spondylolisthesis undergoing MIS resection of a lumbar synovial cyst, concomitant fusion may not always be necessary.
Study Limitations
The limitations of this study include the methodology inherent to a retrospective analysis. Selection bias may, or may not, be present as the inclusion requirement of the patient completing online preoperative and postoperative PROM may have selected out some participants. Facet thermal ablation of the contralateral facet was performed on some of the patients, the impact on the PROM independent of the decompressive procedure is unknown. Additionally, the long-term outcomes follow-up period of a mean of 15 months falls short of the 24-month follow-up standard used in spinal surgery. Because of the above limitations in data collection and analysis definitive recommendations regarding the need for spinal fusions at the index procedure for MIS resection of a lumbar synovial cyst cannot be made from this study.
CONCLUSION
Patients with lumbar synovial cysts may safely undergo MIS decompression in an ASC setting, with a low risk of perioperative complications. The reduction in pain and disability is meaningful in the short term and sustained over the next 15 months. The presence of a grade 1 spondylolisthesis did not adversely impact patient outcomes over this time period. For patients undergoing MIS resection of a lumbar synovial cyst, with either the presence or absence of a grade 1 spondylolisthesis, the mandatory inclusion of a concomitant spinal fusion is brought into question. Further study is required to determine the best approach for management of such patients.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosure The authors report no financial disclosures related to this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.