


Abstract
Background Spine surgery has evolved at an accelerated pace, allowing the development of more efficient surgical techniques while providing a decreasing rate of morbimortality. One example of these approaches is the anterior lumbar interbody fusion (ALIF). The aim of this study was to evaluate the surgical complication rate when performing ALIF without the help of a vascular “access” surgeon.
Methods A retrospective descriptive study was conducted at the Hospital Universitario San Ignacio between 2014 and 2018 and included all patients who underwent ALIF during this time. A nonsystematic review was performed assessing approach-related complications in ALIF and the impact of “access” surgeons in surgical outcomes.
Results A total of 337 patients were included and 508 levels were fused. ALIF was performed as ALIF-360° (27%), ALIF-lateral lumbar interbody fusion (LLIF) (8.9%), and stand-alone ALIF (62%). Most procedures were single-level fusions (51.9%), 45.4% involved 2 levels, and 2.6% were 3-level fusions. The mortality rate was 0%, and only 9 cases of vascular injury were observed and described. Left and common iliac veins were the predominant affected structures. Only a single case required blood transfusion without any other treatment or intensive care unit surveillance.
Conclusions Our study is consistent with literature reports about ALIF complications, finding an incidence of 1.7%. Therefore, ALIF is an excellent alternative for spine procedures, especially for the levels L5-S1 that require sagittal balance restoration. The approaches were performed without a vascular “access” surgeon and presented complication rates similar to those described in the literature.
INTRODUCTION
Spine surgery has experienced a rapid technological evolution, allowing anterior instrumentation to be performed as an ideal tool for the spine surgeon facing pathologies that require indirect decompression, reduction of spondylolisthesis, and sagittal balance restoration, mainly in the L4-L5-S1 levels.1 Historical development of minimally invasive anterior instrumentation dates to 1932 when Capener2 described, in his review of spondylolisthesis, that an anterior corridor with interbody fusion was possible as an alternative to conventional posterior approaches. In 1933, Burns3 reported the case of a 14-year-old patient with a traumatic L5-S1 listhesis who underwent a transperitoneal anterior lumbar approach (left paramedian vertical abdominal incision). During the procedure, the patient required intestinal loop packing and retraction of the left iliac vein for the surgeon to expose the L5 anterior surface, drill an oblique path piercing the S1, introduce a fibular graft, and achieve L5-S1 fusion with an adequate outcome. To address the risk of bone graft fragmentation or migration, interbody cages were introduced by Cloward and Bagby. The use of interbody cages in the lumbar segment began by 1992, but its incompatibility with tomography and magnetic resonance led to the development of systems with polyetheretherketone by Brantiggan in 1994.4 Given the persistence of high rates of pseudarthrosis, substitute materials were designed to improve fusion rates. These materials include the osteogenic protein 1 and the bone morphogenetic protein 2, both approved by the Food and Drug Administration for use in anterior lumbar interbody fusion (ALIF) in 2015.
The anterior approach is increasingly used, and current indications for the procedure include degenerative disc disease, lumbar spinal stenosis, isthmic spondylolisthesis, degenerative spondylolisthesis, degenerative scoliosis, adjacent segment disease, and lumbar nonunion.5,6 The ALIF is very useful for intervention at L4-L5-S1 levels, but it is limited for L2-L3-L4 due to a lower maneuverability. The ALIF is contraindicated in patients with a history of abdominopelvic radiotherapy, significant intestinal adherences, adverse vascular anatomy, and high-grade degenerative spondylolisthesis due to a higher risk of injury to intestinal, vesical, vascular, and nerve structures.7 The anterior approach, however, offers great advantages due to direct midline visualization of the level for intervention, easing lateral exposure of vertebral bodies, discectomy, and foraminal height restoration. The main purpose of the present article is to describe the experiences and intraoperative complications in ALIF of 2 spine surgeons during a 5-year period.
Intraoperative Complications: Is an “Access Surgeon” Required?
Minimally invasive techniques (ALIF, lateral lumbar interbody fusion [LLIF], transforaminal lumbar interbody fusion [TLIF], and oblique lateral interbody fusion [OLIF]) are interbody procedures for the treatment of degenerative disc disease. Approaches in these procedures require less posterior bone removal and use a more limited muscular dissection, promoting a faster recovery. Interbody anterior surgery has widely evolved. In the beginning, anterior approaches needed transperitoneal dissections and careful management of abdominopelvic and retroperitoneal structures, requiring the assistance of an “access surgeon” familiar with that anatomy. Over the years, minimally invasive anterior approaches with retroperitoneal access have been designed with fewer intraoperative complications. Today, however, there is controversy on how to approach the retroperitoneal region. In some countries, joint participation of an access surgeon and a spine surgeon is common for these procedures. For some, a lower rate of vascular injury, intraoperative estimated blood loss, and surgical time justify this joint management; however, more, and larger studies in reference centers are required to determine the need for joint management, especially in developing countries like Colombia that lack experienced surgeons.
MATERIALS AND METHODS
Investigation Design
This descriptive study with retrospective data collection was aimed to determine and measure the incidence of intraoperative complications for anterior lumbar arthrodesis performed in the Hospital Universitario San Ignacio (HUSI) between April 2014 and May 2018. All procedures were performed by neurosurgeons (M.E.B. and R.C.D.), with surgical assistance from residents of neurosurgery at Pontificia Universidad Javeriana. Data were collected from the Sahi tool and clinical histories. A Windows Excel database was created including sociodemographic variables (gender, age, and diagnosis), along with performed procedures, diagnoses in the clinical history, and intraoperative variables that will be described.
Inclusion Criteria
Age 18 years or older
Chronic lumbar pain (clinical manifestations for at least 3 months)
Lumbar spine disease with indication for surgical treatment using anterior lumbar arthrodesis
Lumbar spinal stenosis
Degenerative disc disease
Spondylolisthesis
Spondylolisis
Adult scoliosis
Recurrent radiculopathy
Exclusion Criteria
Patients with a history of radiotherapy or infectious processes
Technique Description
The HUSI in Bogotá, DC, is a reference center for spine pathology. The institution has 2 spine neurosurgeons (R.C.D. and M.E.B.) trained in minimally invasive techniques. For lumbar interbody fusion, the participation of general or vascular surgeons for surgical access or management of intraoperative complications has not been required. The procedure is performed under general anesthesia in supine decubitus position, with urinary catheterization to widen the surgical corridor and reduce the possibility of bladder injury. An intraoperative neurophysiological monitoring system (electromyography and evoked potentials) is used in patients with previous surgical interventions and/or suspected radicular fibrosis, to avoid traction of neural structures with adherences during vertebral distraction. A roll proximal to the popliteal fossa and a soft support for the heels are placed to avoid pressure on sensitive areas and position-related neuropraxia. The neurosurgeon performing surgical access stands contralateral to the incision, and the neurosurgeon performing dissection of retroperitoneal structures stands ipsilateral to the incision.
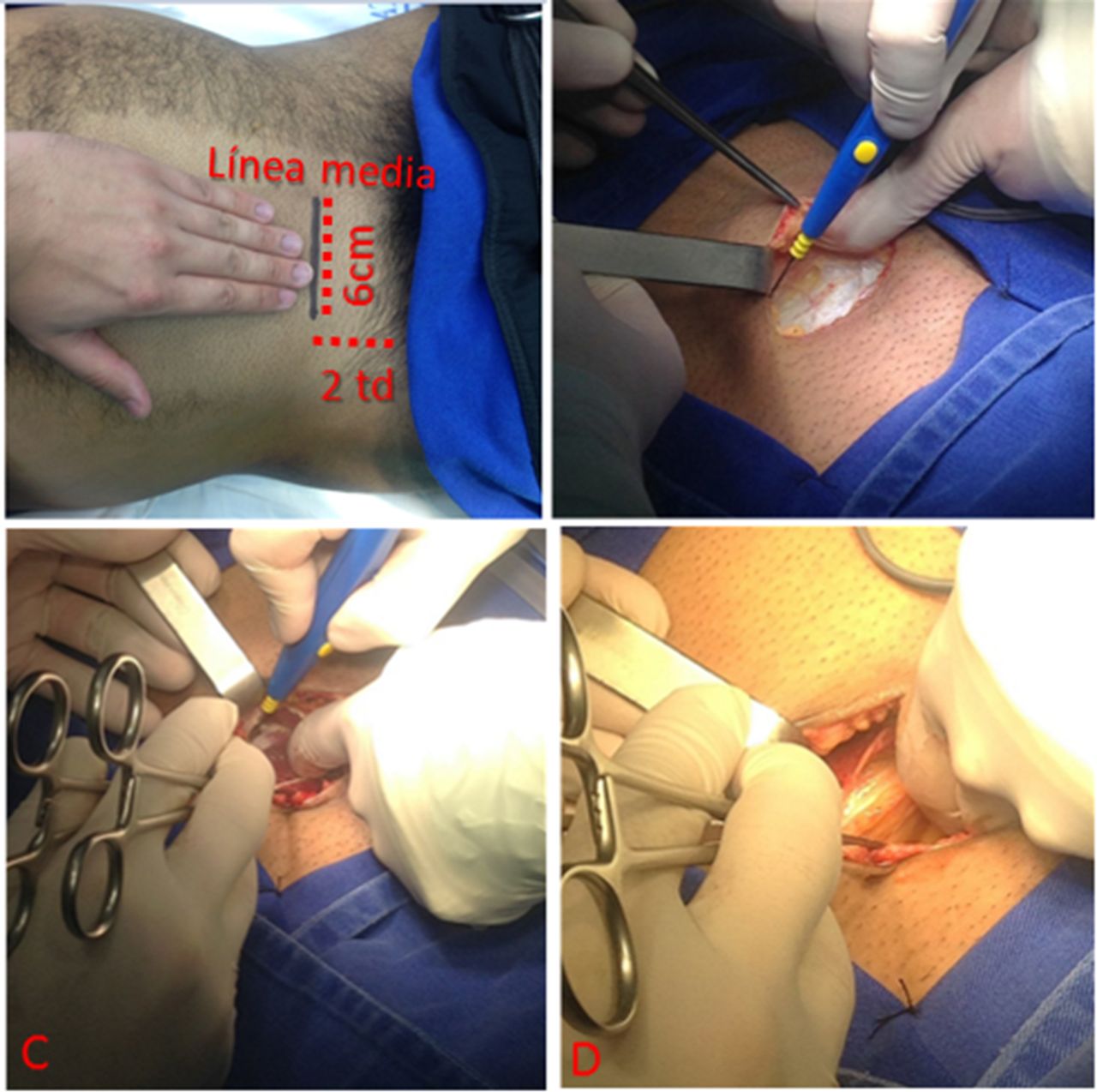
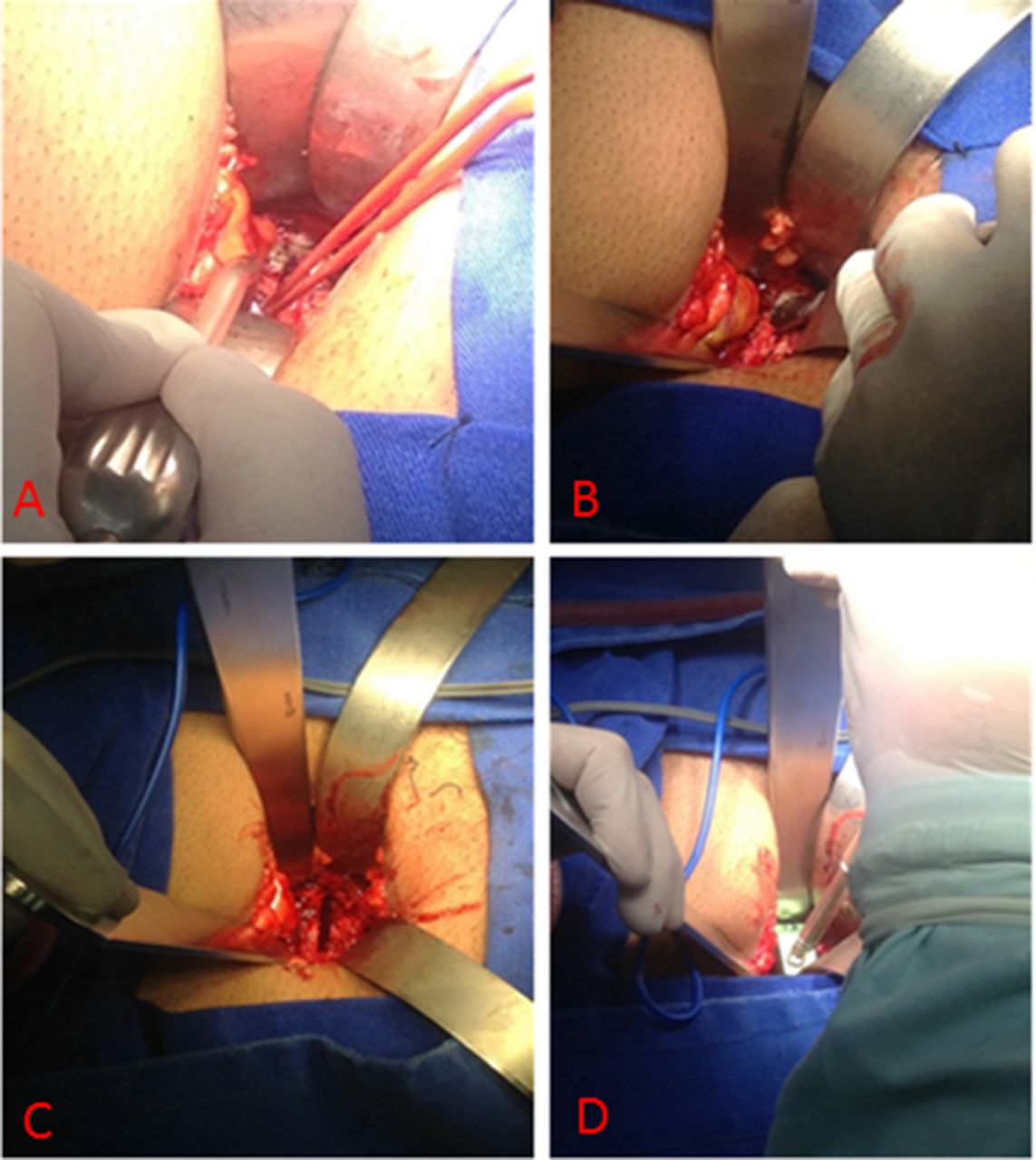
Institutional experience determines the use of mini-open incisions. To approach one disc level, demarcation is made 3.5 cm above the pubis and 3.5-cm fingers from midline. In patients with a history of lipectomy, C-section, or appendicectomy, the incision is located on the previous scar. The horizontal incision is 6 to 7 cm. To approach 2 or more disc levels, a vertical incision is preferred, made in the central one half of a plane between the umbilicus and the pubis (2 fingers above the pubis and 2 fingers below the navel). After the incision, subcutaneous tissue is dissected with electrocautery down to the anterior rectus abdominis fascia, and the fascia is grasped with Allis clamps. The plane of loose areolar connective tissue between the lateral edge of the rectus abdominis muscle and the anterior sheet of the transversalis fascia is exposed, and the surgeon opens the fascia (Figure 1) to access the retroperitoneal space. Cutting the arcuate line of Douglas in the Spiegel semilunar area widens the surgical corridor. Blunt finger or swab dissection of retroperitoneal fat exposes the retroperitoneal structures. For the L5-S1 level, an adequate dissection of the hypogastric plexus with a pillar retractor (Hurd Dissector), avoiding electrocautery, is important. The median sacral vessels are coagulated and dissected to completely expose the disc level (Figure 2).

(A) Demarcation for anterior lumbar interbody fusion approach, right L5-S1 level, incision 6-cm long, 3.5 cm above the pubis, and 3.5 cm away from midline. (B) Exposure of the rectus abdominis anterior sheet. (C) The rectus abdominis anterior sheet and fascia transversalis are opened, then the arcuate line of Douglas is incised. (D) Finger dissection of retroperitoneal space with visible retroperitoneal fat.

(A) The hypogastric plexus is dissected, and the median sacral vessels are coagulated. (B) The exposed L5-S1 disc is released from the vertebral endplates and is removed with a rongeur. (C) The vertebral endplates are prepared, and the zone for arthrodesis is completely exposed. (D) A trial cage is placed in the discectomy zone to define the implant size. Fluoroscopy is performed to confirm depth, position, and lordosis to proceed with the implantation of the cage. Additional grafting materials are added to ensure fusion.
For level L4-L5, it is necessary on many occasions to retract the iliac vessels. To displace the left iliac vein to the right, the surgeon locates, coagulates, and cuts the iliolumbar vein, avoiding tears of the iliac vein wall. Once arthrodesis is completed, the rectus abdominis is reimplanted, and the anterior sheet of the transversalis fascia is closed with multifilament absorbable suture. Subcutaneous fat is also closed with polyglactin, and skin is closed with monofilament absorbable suture.
RESULTS
In clinical records, 337 patients underwent ALIF-type surgery. Approaches were as follows: 27% ALIF 360o (92 patients); 8.9% ALIF-LLIF (30 patients); and 62.9% stand-alone ALIF (212 patients). Of the total patients, 49.5% were men (167 patients) and 50.4% women (170 patients). Age ranged from 18 to 84 years, with an mean age of 53.4 years.
A total of 508 levels of arthrodesis were performed: 51% at 1 level, 45.4% at 2 levels, and 2.6% at 3 levels. Mean surgical time was 121 minutes. (Time was registered for only 147 patients.)
There was no intraoperative mortality, and there were no cases of dural, intestinal, ureteral, or vesical injury in this series of patients. Regarding vascular complications, there were no cases of arterial injury. There were 9 cases of vein injury (1.7% of the total levels of discectomy), with a mean estimated blood loss of 125.7 cc. Transfusion was required in a single case, without the need for intensive care in the postoperative period. In 2 cases, the injured vascular structure was not specified, and bleeding was controlled with electrocoagulation and a hemostatic sponge. There was 1 case of iliolumbar vein injury, 1 case of iliopelvic vein injury, and 5 cases of iliac vein injury that were controlled with suture and hemostatic sponge. One case required human thrombin to complete hemostasis after the previously mentioned strategies (Table 1).
Case characteristics and vascular complications, age, surgical level, injured structure, lesion treatment, and estimated blood loss.
DISCUSSION
Vascular Injury
In a 2006 review about vascular injuries in spine surgery from 1993 to 2005, Guiot et al8 found the rate of vascular injury in ALIF to be between 0% and 18.1%. Injury to venous structures was more frequent during retraction maneuvers to expose interbody spaces. In 2004, Brau et al found a vascular injury rate of 1.9% in a series of 1310 patients, 16 with injury to the common iliac vein.9 The case series in the present article had 5 iliac vein injuries, most frequently on the left side, all adequately controlled; only a single patient required hemoderivate transfusion, with no need for intensive care. Left iliolumbar vein avulsion in the level L4-L5 is also common during the left iliac vein retraction.
Possible anatomical variations, such as multiple iliolumbar veins, must be considered. In 2002, Jasani et al10 described 3 types of variation: (1) a common trunk that drains into the common iliac vein, 68.5% of cases; (2) proximal and distal iliolumbar trunk that drain into the common iliac vein, 31.2%; (3) ascending lumbar vein reaching the common iliac vein independently and more proximal than the iliolumbar vein, 12.5%. In most series, the vein injury was managed with hand compression, followed by primary suture of the vascular tear. Although it is not frequently described, location and ligation of the ascending lumbar vein in the space L4-L5 are important to prevent bleeding of the iliac vein, just as with the iliolumbar vein.10,11 (This technique is performed in the Department of Neurosurgery at HUSI, where only a single case of iliolumbar vein injury has occurred during the study period.)
Currently, a novel classification of the common iliac vein bifurcation complex related to the ALIF procedure, is being developed at our institution (HUSI) to predict the risk of vascular injury during this type of procedure.
Arterial structures are affected with lower frequency. Their walls are more resistant, and arteries can be moved more easily. The most common arterial injury occurs in the left iliac artery (0.9%).12
Dural Lesion
The literature reports a low risk of dural lesions as intraoperative complications for anterior arthrodesis.13,14 A meta-analysis by Phan et al in 2015 found a low occurrence of dural lesion in patients undergoing ALIF, with a 0.29 risk ratio and 95% CI (0.08–1).15 Consistent with this, a systematic review of the literature by Mobbs et al in the same year mentioned a lower incidence of dural lesions with ALIF compared with other lumbar arthrodesis techniques. The series of patients in this article did not have dural lesions with the anterior approach. The technique might explain the low risk for dural lesion in ALIF, as the anterior approach allows better visualization and avoids unnecessary manipulation of neural elements.16
Intestinal Injury
Intraoperative complications of ALIF related to gastrointestinal injuries are less frequent than other types of complications.13,14 In a systematic review, Mobbs et al reported visceral injuries of 0% to 1.7%.17 A study performed between 2009 and 2013 in a 227-patient cohort, found 3 cases of incisional hernia (1.3%) requiring revision surgery.17 In a cohort of 87 patients, Amaral et al reported minor peritoneal lesions in 4 cases (4.6%) requiring intraoperative suture.18 In this series, no gastrointestinal complications occurred in patients who underwent anterior arthrodesis. Patient selection and surgical technique explain this difference in reports from multiple studies. At the HUSI, patients with a history of radiotherapy or of infectious processes are not selected for anterior arthrodesis. Also, the meticulous dissection with gauze swabs separates the spine and psoas muscle from the posterior sheet of the peritoneum.
Ureteral Lesion
In 2015, Parks et al evaluated 37 patients for hydronephrosis with pre- and postoperative ultrasound, considering hydronephrosis an indirect sign of ureteral lesion during ALIF. No hydronephrosis was found in any patient. The authors describe injury to the ureter vascular pedicle located distal to L4-S1.19 The present series did not have any case of intraoperative ureteral or bladder injuries.
Vascular Surgeon Assistance
Medicolegal issues and the surgeon’s experience in a special anatomical corridor drive the use of an “access surgeon.” Some studies report fewer complications20,21,21 with the assistance of a vascular surgeon, but others describe lengthier surgical times and higher numbers of complications (Table 2).
Case series reports from 1961 to 2019 with vascular injury rate during anterior lumbar interbody fusion procedures.
In a systematic review, Phan et al compared ALIF approach outcomes by neurosurgeons alone with outcomes when a vascular surgeon assisted neurosurgeons. That study found higher rates of arterial complications (OR 2.67, P < 0.001), retrograde ejaculation (OR 2.34, P < 0.001), and ileus (OR 2.45, P < 0.001) in surgeries performed with the help of vascular surgeons. Jarett et al found a higher rate of complications in interventions performed by a team. The percentage of patients with at least 1 complication was 8% for cases with neurosurgeons alone and 12% for cases with access surgeons.21 A study in a retrospective cohort found a significantly higher incidence of ileus in procedures supported by vascular surgeons (58% vs 2.6%, P < 0.0000001).22 This suggests that neurosurgeons with adequate training can perform the ALIF initial approach without the participation of a vascular surgeon, achieving better outcomes and experiencing fewer complications.
CONCLUSIONS
Anterior interbody surgery is an excellent option for disc disease management, especially for levels L4-L5-S1 that require sagittal balance restoration. This study offers a case series without intraoperative mortality or nonvascular injuries. The vascular injury rate was 1.7% without arterial complications, a result comparable to rates found in international literature (Table 2). Studies with larger samples are necessary to evaluate the real impact of the use of an access surgeon on vascular injury, transfusion requirements, and surgical procedure duration.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosure The authors report no financial disclosures related to this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.