


Abstract
Background There are numerous radiological and anatomical studies on lumbar foramina in the literature, but there are no distinctive studies about the relationship between treatment and the type of foraminal stenosis. This study was conducted to better evaluate foraminal stenosis and to plan treatment accordingly.
Methods Foraminal stenosis was divided into 2 groups: stable and unstable stenosis. Both groups were also divided into 4 subgroups in relation to the cause and type of compression and based on the structure of the intervertebral disc. The visual analog scale for leg pain (VAS-LP) and Oswestry Disability Index (ODI) scores were investigated before and after surgery.
Results A total of 115 patients (59 women and 56 men) underwent surgery for lumbar foraminal stenosis. The mean patient age was 56.1 years (range 17–80 years). The mean follow-up was 29 months (range 24–39 months). There were 36 patients (32%) with stable foraminal stenosis and 79 patients (68%) with unstable foraminal stenosis. The majority of the patients were identified as having unstable type 1 foraminal stenosis (45 of 115). The VAS-LP and ODI scores for each group decreased gradually during the follow-up periods and showed significant decrease during the last follow-up (P < 0.001). Interobserver and intraobserver agreement in the classification of foraminal stenosis was found to be nearly perfect. No patients experienced postoperative radiculopathy complication. Only 2 patients experienced superficial operation site infection and 1 showed deep wound infection. The patient who had a deep wound infection needed to repeat surgery for the infection.
Conclusions We introduced a novel classification system for lumbar foraminal stenosis. We aimed to guide appropriate treatment modality depending on the determined classification. This classification helps to determine the optimal treatment. In the light of our findings, the patients who were operated according to our classification experienced satisfactory clinical outcomes and low complication rates.
Level of Evidence 3.
Introduction
Foraminal stenosis is defined as the narrowing of the bony exit of the nerve root from the dural sac. Pathophysiology of the foraminal stenosis is mainly based on the deterioration of the normal anatomy due to degenerative changes in elderly populations. The basic surgical treatment of spinal stenosis is decompression and enlargement of the spinal canal. Unfortunately, postoperative results are unsatisfactory when the accompanying foraminal stenosis is overlooked and remains untreated. Although there are many anatomical, morphometric, and radiological studies performed on the subject, there are no systematic treatments or classification systems for a treatment strategy.1–4
The purpose of this study was to evaluate the clinical signs of foraminal stenosis to provide a classification and treatment algorithm.
Methods
The data from 156 consecutive patients with symptomatic single-level lumbar foraminal stenosis who were admitted to our institution between August 2016 and October 2019 were carefully reviewed. All 156 patients were enrolled in conservative treatment modalities. However, 127 patients did not get a significant benefit from conservative treatment for their symptoms for at least 6 months. Therefore, surgical treatment was performed for these patients by a senior surgeon. The inclusion criteria were (1) not getting benefit from conservative treatment for at least 6 months prior to surgery; (2) no history of malignancy, infection, previous surgery, and spinal fracture; and (3) having at least 24 months of clinical and radiological follow-up. The visual analog scale (VAS) was used to assess the pain levels preoperatively and at 1, 6, 12, and 24 months after surgery. The Oswestry Disability Index (ODI) was used preoperatively and at 1, 6, 12, and 24 months after the operation to assess disability. Twelve patients were not included due to missing data. Thus, the cases of 115 patients with single-level lumbar foraminal stenosis whose records contained complete information were included in the current study. Ethics committee approval was not obtained as this study was created by evaluating the data retrospectively.
Classification of Foraminal Stenosis
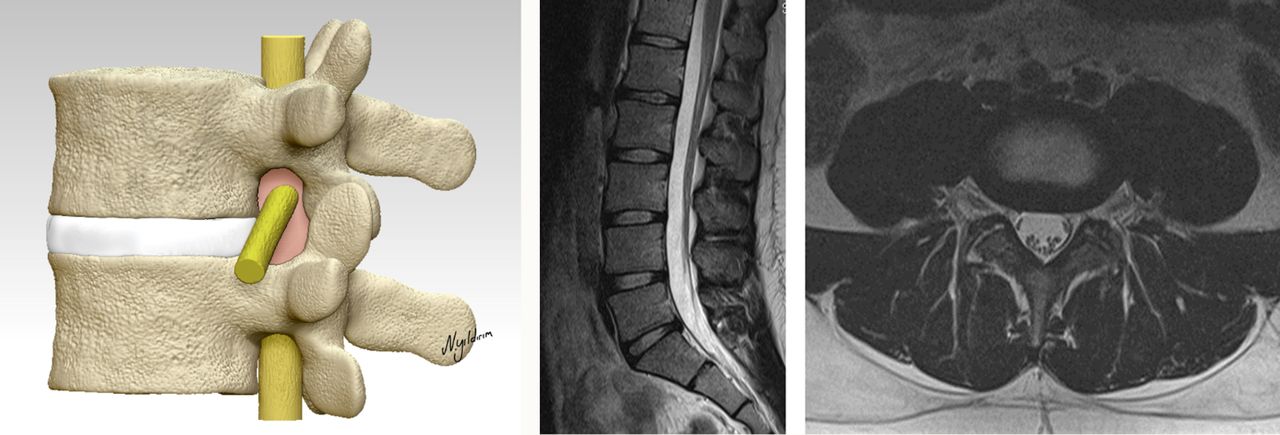
The anatomical and radiological appearance of a normal lumbar foramen is shown in Figure 1. Foraminal stenosis was divided into 2 groups: stable and unstable stenosis. In stable stenosis, the disc and annulus are calcified and fused to the upper and lower corpus vertebrae. Posterior facet joints are hypertrophic and severely degenerated. Fusion of articular facets is not a rare finding. In unstable stenosis, there is a degenerative and mobile intervertebral disc that causes instability in any motion. There are 4 subgroups to each stenosis type.

Normal foramen.
Stable Foraminal Stenosis
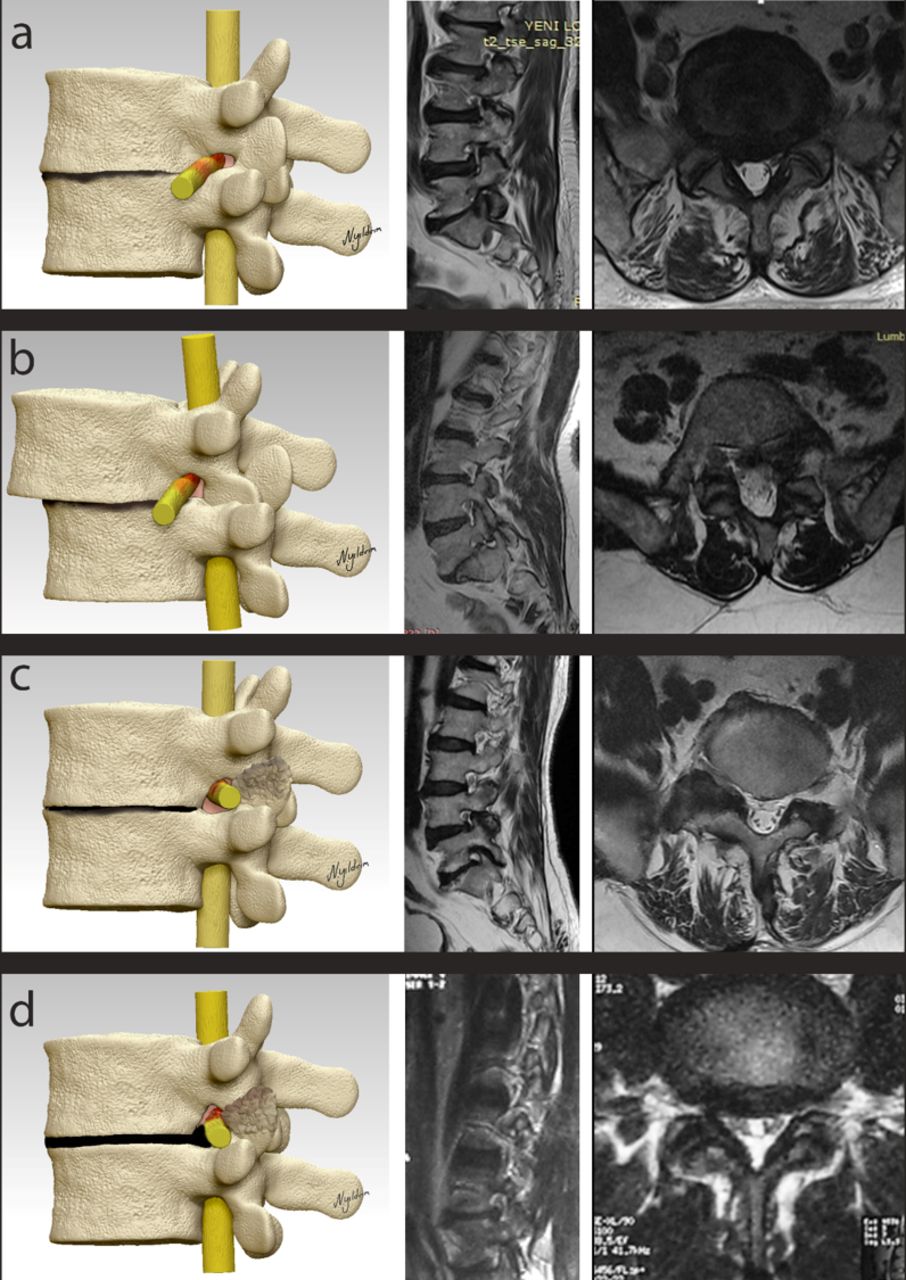
Type I—The disc is completely nonfunctioning and degenerated. The related segment does not show any instability in dynamic radiographs. The root is compressed only between the upper and lower pedicles (Figure 2a).

(a) Type I stable foraminal stenosis. The disc has completely degenerated; the root is squeezed between the upper and lower pedicles. (b) Type II stable foraminal stenosis. The disc has completely degenerated at the base of degenerative spondylolisthesis. The root is squeezed between the upper pedicles and lower vertebral corpus. (c) Type III stable foraminal stenosis. The disc has completely degenerated; the root is squeezed between the calcified facet joint and the corner of the upper pedicles and posterior wall of upper vertebrae. (d) Type IV stable foraminal stenosis. The disc is calcified in some areas and fused in some areas to the upper and lower vertebral corpus, with bulging of the posterior annulus. The root is squeezed between the calcified bulging of the posterior annulus, calcified facet joint, and upper pedicles. For all images, the red areas on the nerve root indicate dense areas where the nerve is squeezed.
Type II—The disc is completely nonfunctioning and degenerated. The related segment does not show any instability in dynamic radiographs. However, there is degenerative spondylolisthesis. The root is compressed between the upper pedicle and the lower vertebral body (Figure 2b).
Type III—The disc is completely nonfunctioning and degenerated. The related segment does not show any instability in dynamic radiographs. However, there is a remarkable calcified hypertrophic facet joint that pushes the root against the corner that makes up the upper pedicle and posterior wall of the upper vertebral body (Figure 2c).
Type IV—The disc is completely nonfunctioning and degenerated. The related segment does not show any instability in dynamic radiographs. However, there is a completely calcified bulged disc that is fused to the upper and lower vertebral bodies. The root is compressed between the calcified bulged disc and the hypertrophic degenerated posterior facets (Figure 2d).
Unstable Foraminal Stenosis
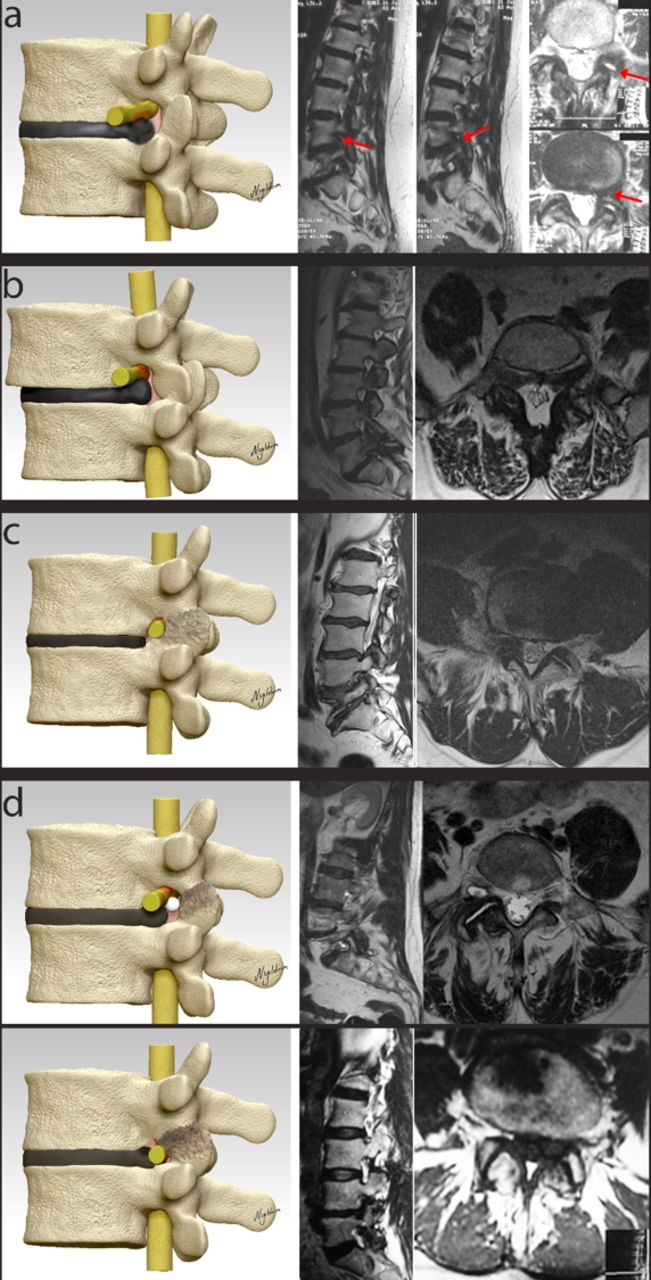
Type I—There is a mobile degenerative and soft bulged intervertebral disc, and dynamic radiographs show instability in the related spinal segment. The root is squeezed between the bulged disc and posterior facet joints. This type of narrowing can be observed in every age group, and extensive degeneration is not usually present or necessary for the development of this type. The majority of the foraminal stenosis patients in the current study were in this group (Figure 3a).

(a) Type I unstable foraminal stenosis. There is a mobile degenerative bulged disc, and the root is squeezed mainly between the bulging of the disc and upper pedicles. (b) Type II unstable foraminal stenosis. The disc is degenerative and mobile, but there are degenerative spondylolisthesis and pseudobulging. The root is squeezed between the pseudobulbed disc and the superior pedicle. (c) Type III unstable foraminal stenosis. The disc is degenerative and mobile, and there is no bulging. The root is squeezed between the posterior degenerative facet joint, the corner between the pedicle and the posterior wall, and the vertebral corpus of upper vertebrae. (d) Type IV unstable foraminal stenosis. The disc is degenerative and mobile; the root is squeezed between the posterior degenerative facet joint and synovial cyst of the facet joint, and the only difference from unstable type III is bulging of the disc, which can be related to compression over the nerve root. For all images, the red areas on the nerve root indicate dense areas where the nerve is squeezed.
Type II—The intervertebral disc is degenerative and mobile, and dynamic radiographs show instability in the related spinal segment. However, there are degenerative spondylolisthesis and pseudodisc herniation due to spondylolisthesis. The root is compressed between the pseudodisc herniation and the upper pedicle (Figure 3b).
Type III—The intervertebral disc is degenerative and mobile without any bulging, and dynamic radiographs show instability in the related spinal segment. The calcified hypertrophic facet joint pushes the root against and toward the corner of the upper pedicle and the posterior wall of the upper vertebral body (Figure 3c).
Type IV—The intervertebral disc is degenerative and mobile with bulging, and dynamic radiographs show instability in the related spinal segment. However, the bulging is not compressing the root and not the main factor of foraminal stenosis. The root is compressed between the hypertrophic degenerated facet joints and synovial cysts that developed in the facet joint (Figure 3d).
Treatment Protocol
In the stable foraminal stenosis group, the disc and annulus were fused to the upper and lower vertebrae. This means that there is no apparent mobilization of the anterior column, and the foraminal stenosis is therefore categorized as stable, and decompression procedures were performed without instrumentation due to spontaneous fusion of the related spinal segment (Table 1).
Treatment options for stable foraminal stenosis.
For stable stenosis subgroup types I and II, complete or partial resection of the pedicle with resection of the lateral recess added to facet joint resection (Gill’s procedure) is essential.5 The microsurgical approach is the gold standard. Similar procedures may be performed utilizing the endoscopic techniques.
In stable type III, compression is caused by the posterior wall. Posterior resection (Gill’s procedure) is sufficient using either microsurgical or endoscopic techniques.
In stable type IV, compression is caused by the bulged calcified rigid disc. Facet excision may provide a solution for the foraminal stenosis; however, removal of the calcified disc using a high-speed drill under a microscope or endoscope provides a satisfactory solution.
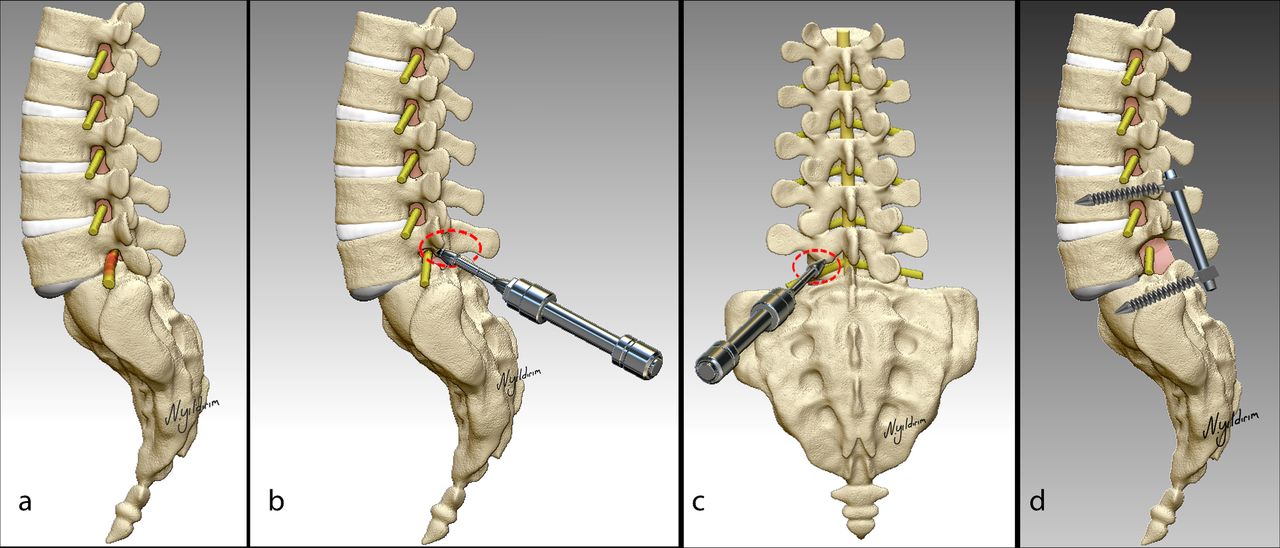
The group of patients with a mobile disc at the segment is classified as unstable foraminal stenosis, and the functional segment is instrumented unilaterally or bilaterally following the root decompression (Figure 4).

Illustration of a patient with unstable stenosis treated with decompression and stabilization. (a) Compressed nerve root under the pedicle. (b, c) Removal of pedicle with a high-speed drill. (d) The decompressed nerve root and screw stabilization.
Unstable type I is the most common subgroup of all foraminal stenosis patients; if there is no solid evidence of instability, it is not necessary to stabilize the patient. Removal of the soft disc by micro- or endoscopic surgery is adequate in this group (Table 2).
Treatment options for unstable foraminal stenosis.
In unstable type II, the segment is highly unstable. The classic approach is partial or total facetectomy, discectomy, transforaminal lumbar interbody fusion or posterior lumbar interbody fusion, and transpedicular rigid stabilization. These procedures can be performed using minimally invasive surgical techniques. If there is no suspicion for imbalance on dynamic radiographs, bilateral transpedicular dynamic stabilization (Dynesys) can be performed.
For patients with unstable types III and IV, the treatment protocol is similar to that for stable types III and IV. Assessment of the mobilization of the disc is important for the selection of the appropriate treatment. In our experience, if the disc is less mobile, partial facetectomy provides enough space for the exiting root, and further instrumentation for added stabilization is not necessary. If disc mobility is high, standard fusion should be performed; however, we have also experienced very good clinical results with dynamic transpedicular stabilization systems (Dynesys).
Statistical Analysis
Interobserver agreement between the 1 neurosurgeon (reader 1) and 1 neuroradiologist (reader 2) and intraobserver agreement were analyzed by using kappa statistics. Kappa values less than 0.00 indicate “poor” agreement, 0.00 to 0.20 represent “slight” agreement, 0.21 to 0.40 represent “fair” agreement, 0.41 to 0.60 represent “moderate” agreement, 0.61 to 0.80 represent “substantial” agreement, and 0.81 to 1.00 represent “almost perfect” agreement.6 Student t test was performed to analyze clinical results, and P < 0.05 was considered statistically significant. Commercially available statistical processing software (SPSS, version 26.0, SPSS Inc.) was used for all calculations.
Results
A total of 115 patients with lumbar foraminal stenosis were included in this study. There was no significant difference between the genders of the patients (59 women and 56 men). The mean patient age was 56 years (range 17–80 years). The mean follow-up was 29 months (range 24–39 months). There were 36 patients (31.3%) with stable foraminal stenosis and 79 patients (68.7%) with unstable foraminal stenosis. Unstable type 1 foraminal stenosis was the most common type (39% of patients) followed by unstable type 2 stenosis (13%). Table 3 shows details of the demographic data and distribution of the foraminal stenosis cases.
Demographic data and distribution of the foraminal stenosis cases.
Two patients developed superficial surgical site infections, which were diagnosed after 1 month and treated with irrigation and antibiotics. One patient treated with dynamic stabilization developed deep surgical site infections in the unstable type II group, and the system was removed. Among the patients in all groups, no revision surgery was needed for radiculopathy complaints such as leg pain, hypesthesia, or weakness.
In our series, a significant clinical improvement was observed after surgery that was performed according to our classification. In all stable and unstable foraminal stenosis types, preoperative VAS-LP showed a statistically significant decrease from preoperative to 24-month postoperative measures (P < 0.001). Table 4 shows details of mean VAS-LP scores at each follow-up.
Patient VAS-LP scores by timepoint.
Likewise, significant ODI score decreases were observed after surgery that was performed according to our classification. In all types of stable and unstable foraminal stenosis, preoperative ODI scores showed a statistically significant decrease during from preoperative to 24-month postoperative measures (P < 0.001). Table 5 shows details of mean ODI scores at each follow-up.
Patient ODI scores by timepoint.
Interobserver agreement in the classification of foraminal stenosis between the 2 readers was found to be nearly perfect (κ values: stable type I, 0.895; stable type II, 0.939; stable type III, 0.917; stable type IV, 0.945; unstable type I, 0.926; unstable type II, 0.919; unstable type III, 0.924; unstable type IV, 0.907).
After more than 12 months, intraobserver agreement in the classification of foraminal stenosis by reader 2 also was found to be nearly perfect (κ values: stable type I, 1.0; stable type II, 1.0; stable type III, 0.948; stable type IV, 1.0; unstable type I, 0.977; unstable type II, 0.982; unstable type III, 0.972; unstable type IV, 1.0).
Discussion
There are many foraminal stenosis classification systems in the literature. However, all of the classification systems have focused on radiological and anatomical aspects of foraminal stenosis. Therefore, there is no foraminal stenosis classification that guides the surgeon for appropriate surgery. To the best of our knowledge, our study presents the first classification system that describes the treatment algorithms for different stenosis types. Besides establishing the treatment algorithm, we defined terms of “stable” and “unstable” for guiding the treatment choice.
Except for foraminal soft discs and synovial cysts, it can be easily concluded that nerve root compression due to foraminal stenosis is an advanced age disease. Unless the movement of the functional segment is lost, painful root irritation is secondary to foraminal mobility. The pain is generally decreased by altering the patient’s body position. However, as the motion in the functional segment diminishes, root irritation becomes more prominent both clinically and radiologically. In these patients, the height of the foramen decreases as the disc height decreases and the nerve root is compressed further in the foramen. This situation is seen mostly in types I and II of stable foraminal stenosis. It should be noted that for patients with both foraminal stenosis and spinal canal stenosis who are undergoing treatment, proper decompression of the foraminal narrowing is overlooked more often than we think.
Although there are many anatomical and radiological studies, written experiences, and different treatment methods available in the literature, there is no certain algorithm for treatment selection. Foraminal stenosis grading based on magnetic resonance imaging findings has been published in the literature; however, none of the existing literature presents an algorithm for treatment selection based on grading.7,8 The structure causing foraminal stenosis must be carefully assessed, and a plan for treatment must be made accordingly. For example, in stable type I foraminal stenosis, the nerve root is compressed between the 2 pedicles, and in type II, the nerve root is compressed between the upper pedicle and posterior aspect of the underlying vertebral body; therefore, the caudal part of the compressing factor is completely different. It has long been established that the nerve root can be decompressed by performing classical unroofing (Gill’s procedure), which is still a valid procedure. Even if the foramina are unroofed, it is doubtful that the patient will benefit from this procedure due to the constant compression between the upper and lower structures caused by the axial load.5,9 It is also important to add that unroofing in certain foraminal stenosis types will not provide pain relief. In these cases, it is necessary to perform a complete or partial pediculectomy to achieve an enlarged foramen. If the pedicle is completely removed, including facet joints, the lower and upper foramen join together to form a large foramen in which 2 nerve roots easily exit. We could not find a detailed study in the literature other than our previous publication.10
In stable foraminal compression, the clinical presentation is continuous and evident and can almost always be treated with minimally invasive methods with no further instrumentation required. However, problems arise in unstable foraminal stenosis. Facet joints play an important role in the stabilization of the lumbar functional segment. Especially in degenerative cases, removal of a facet joint greatly affects the motion segment that is damaged due to the process of aging. In these cases, the neutral zone expands further. In the unstable subgroup types I, III, and IV, if there is no significant evidence of instability, it may be possible to intervene in the pathology without disrupting the anatomy too much. For example, in cases with foraminal soft disc herniation and synovial cysts, microsurgery and endoscopic surgery can be used to remove the pathology without disrupting the anatomy.11–13 Despite the possibility of recurrence, recurrence ratios are not very high; therefore, surgery can be performed without using instrumentation as the first choice. On the other hand, if the hypertrophic facet is the cause of the compression over the nerve root, it is necessary to remove the facet joints. Generally, these cases require stabilization because of the high instability risk following surgical intervention.14,15 Another possible requirement for adding stabilization is the severity of disc degeneration in unstable disc herniation. Severely degenerated and less mobile dysfunctional segments do not require instrumentation to maintain stabilization. It should be noted that a mobile functional segment becomes more unstable after facet resection; therefore, regardless of dynamic or rigid segments, the concept of stabilization should be considered more seriously.
Removal of facet joints, especially in unstable type II patients, leads to increased instability and usually requires instrumentation. These patients constitute a younger age group and mostly have no evident balance problems. The classical approach is to remove the disc, apply fusion with a cage to increase or maintain the disc height, and stabilize the disc with rigid transpedicular instrumentation.16,17 This approach is currently accepted as the gold standard. However, recently, transpedicular dynamic systems (Dynesys) have been proposed by many spinal surgeons in many countries outside the United States.18–20 These systems are reported to be suitable for every age group and provide a softer stabilization. It is a minor surgery compared with fusion with a lower postoperative hospitalization period. It is also a more cost-effective surgery when compared with fusion and rigid instrumentation. Especially for elderly patients with comorbidities, there is no major complication reported at the single level.21,22 In appropriate cases, after removal of the facet joint, a unilateral dynamic system can act as an artificial facet joint.23 Which type of stabilization will be selected for the treatment entirely depends on the choice of the surgeon.
No patients experienced postoperative radiculopathy complications or revision surgery and only 1 patient needed surgery for infection. This was another finding that supports the reliability and proper classification of the foraminal stenosis types before surgery.
The most important limitations of the study are the retrospective nature, the inclusion of only patients with single-level lumbar foraminal stenosis, the short follow-up period, and the relatively small number of patients. Furthermore, this classification may also need to be combined with the evaluation of prognostic factors from other aspects for the development of foraminal stenosis. In addition, the treatment options may be modified owing to the availability of different treatment options, such as type of dynamic stabilization, depending on centers’ availability and experience.
Conclusion
We present a novel classification system for lumbar foraminal stenosis depending on the anatomy and the pathology. We aimed to guide appropriate treatment methods depending on the determined classification. In the light of our findings, the patients who were operated according to our classification experienced satisfactory clinical outcomes and lower complication rates. In the future, we believe that collective knowledge will be accumulated and that better solutions will emerge.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.