


Abstract
Background Until recently, open decompression was considered the gold standard for the management of spinal stenosis, but the evolution of minimally invasive spine instruments has brought a new dimension to the management of spinal stenosis. Full endoscopic surgery has a lot of advantages in terms of minimal soft tissue damage, less bleeding, shorter hospital length of stay, and earlier return to work. Our aim was to evaluate the efficacy of full endoscopic lumbar decompression for degenerative lumbar canal stenosis compared with classic open decompression surgery.
Methods This is a retrospective cohort study of degenerative lumbar spinal stenosis without instability, consisting of 132 open decompression and 163 full endoscopic decompression patients. We evaluated the clinical result of the pre- and postoperative visual analog scale (VAS) of leg pain, back pain, and Oswestry Disability Index (ODI). We observed the patients until 1 year after the operation.
Results The postoperative ODI scores and VAS scores for back pain and leg pain were better than the preoperative scores. The ODI scores and VAS scores for leg pain were significantly better in both groups (P = 0.033 and 0.04, respectively). The main difference between open and full endoscopic decompression was the VAS back pain and amount of bleeding. In the full endoscopic group, the mean VAS back pain was 1.6 and the amount of bleeding was minimal. In the open decompression surgery, the mean VAS back pain was 3.5 and the amount of bleeding was around 84 mL. The length of hospital stay was shorter in the full endoscopic group, which was 1.5 days compared with 3.4 days in open decompression (P = 0.034).
Conclusion Full endoscopic decompression showed better early results compared with the conventional group, but a long-term study is still needed for further evaluation of the clinical results. The use of the full endoscopic technique is very promising in the management of spinal stenosis.
Clinical Relevance This study provides a comparison of the efficacy of open decompression and full endoscopic decompression in degenerative lumbar canal stenosis.
Level of Evidence 3.
- Degenerative lumbar spine
- spinal stenosis
- minimally invasive spine surgery
- full endoscopic spine surgery
INTRODUCTION
Degenerative lumbar canal stenosis is the most common pathology found in the fifth to sixth decades of life.1 This condition of a narrowing spinal canal is caused by the combination of flavum ligament hypertrophy, bony osteophyte, facet joint hypertrophy, and disc bulging or disc narrowing.2 The symptoms are very debilitating for the patient, which give rise to classic neurogenic claudication with or without radicular pain.3
Conservative treatment, even though it is still considered the first-line therapy, usually shows no significant improvement. Most of the studies on lumbar canal stenosis indicate that decompression surgery offers great improvement in symptoms, and the beneficial effect could last for more than 8 to 10 years.3–5 Over the past decade, surgical techniques and instrumentations have been developed to reduce the invasiveness of the operation from classic open surgical decompression, tubular microscopic, or endoscopic-assisted decompression to full endoscopic decompression. The concern for reducing the invasiveness of the procedure is epidural scarring, which could give rise to clinical symptoms in 10% of cases and makes revision surgery more difficult to perform. The other concern is to reduce the possibility of instability that will happen due to excessive bone and soft tissue resection and muscle injury.6
The procedure of endoscopy has become a standard in other fields of medicine, such as arthroscopy and laparoscopy. Even in some parts of the world, full endoscopic spine decompression has become the first choice of treatment for degenerative lumbar canal stenosis, but the need for sophisticated tools makes this procedure not easily accessible in every place without good preparation.7,8 The improvement in optics, high-speed drills, and surgical instruments enables the surgeon to gain similar results to those obtained during classic open surgery while having the advantages of smaller skin incisions, less muscle injury, less bleeding, less possibility of infection, and fewer wound healing problems.6
The learning curve is one of the biggest challenges in endoscopic spine surgery; converting 3-dimensional images into 2-dimensional images and developing good hand-eye coordination are the major issues.7 During the early phase of the learning curve, problems during surgery may arise, causing the procedure to become more time-consuming and leading to potentially more complications.
The purpose of this study was to evaluate the result of full endoscopic stenosis decompression with a unilateral approach compared with classic open surgery. We tried to evaluate the feasibility of the procedure, the obstacle, and the possible complications that might arise because of the procedure.
MATERIALS AND METHODS
This was a prospective cohort noninferiority study on degenerative lumbar canal stenosis cases that were managed by operative procedure by 3 attending surgeons at Fatmawati General Hospital, Jakarta, Indonesia, between January 2019 and January 2020. There were 612 patients included in the study: 223 male patients and 389 female patients. Full endoscopic decompression was done on 368 patients, and the rest of the patients underwent classic open surgical decompression. The level of operation varied between L3-L4, L4-L5, and L5-S1. The selection of surgical procedures was determined according to the surgeon’s preference. All of the patients had clinical symptoms of neurogenic claudication before the operation that were not relieved by conservative treatment.
The inclusion criteria for the study were leg symptoms in the form of neurogenic claudication with or without radicular pain, minimal back pain with a visual analog scale (VAS) <3, a stable dynamic x-ray image that showed no need for fusion, and central, lateral recess, or foraminal stenosis on magnetic resonance imaging (MRI).9,10 The exclusion criteria were unstable degenerative spondylolisthesis, degenerative scoliosis >20°, and cauda equina syndrome.
The blood loss, surgery duration, and length of stay were noted for each patient. Blood loss in the endoscopic group was defined as the blood loss under the endoscope and evaluated by the total amount of rinse solution minus the total irrigation fluid. Clinical outcomes were evaluated using the Oswestry Disability Index and VAS for back pain and leg pain on the first day after surgery, 3 months, 6 months, and 12 months. All patients underwent MRI on the first day after surgery to evaluate the result of decompression after surgery. The criteria for hospital discharge were the amount of surgical drain and pain symptoms that were manageable with an oral analgesic. The basic characteristics between the 2 groups were similar with no significant comorbidities in the open surgery group that prevented this group from leaving the hospital earlier. All statistical measurements were calculated using SPSS 17 with nonparametric statistics using Mann-Whitney U and proportion data using Fisher exact test.
SURGICAL TECHNIQUES
Conventional Open Decompression
Classic open surgery was performed through a posterior midline incision, muscle retraction on both sides to expose the lamina, facet, and flavum ligament. A bilateral laminotomy was performed until the origin of the flavum ligament and the lateral recess was opened. The flavum ligament was excised until the thecal sac and traversing root were free.
Endoscopic Decompression
Patients were positioned prone with 2 bolsters lying transverse on the chest and the anterior superior iliac spine. This position helps us open the interlaminar window by jacking up the table. In our center, we mostly use general anesthesia for the procedure, even though several patients with several comorbidities received regional anesthesia. In our opinion, general anesthesia provides more comfort for patients, and it is easier to maintain the mean arterial pressure during surgery with general anesthesia.
The skin incision for central and lateral recess stenosis was located as medial as possible near the spinous process, an obturator with a diameter of 8 mm was introduced until the base of the lamina-spinous junction, and a beveled working channel was inserted over the obturator. The endoscopic central and lateral recess decompression procedure (see Video, Supplemental Video 1, which demonstrates endoscopic central and lateral recess decompression) started from drilling the medial facet from the level of midlower pedicle until the tip of superior articular process (Figure 1). The flavum ligament was removed using different types of punches and endo-Kerrison. The contralateral part of the flavum ligament and medial facet was approached posteriorly from the thecal sac (over the top technique) by tilting the whole working channel and endoscope. Decompression was considered finished after seeing the free thecal sac and the traversing nerve root (Figure 2). The patient underwent MRI after the operation to confirm the result of decompression.
Online Supplementary Video 1.
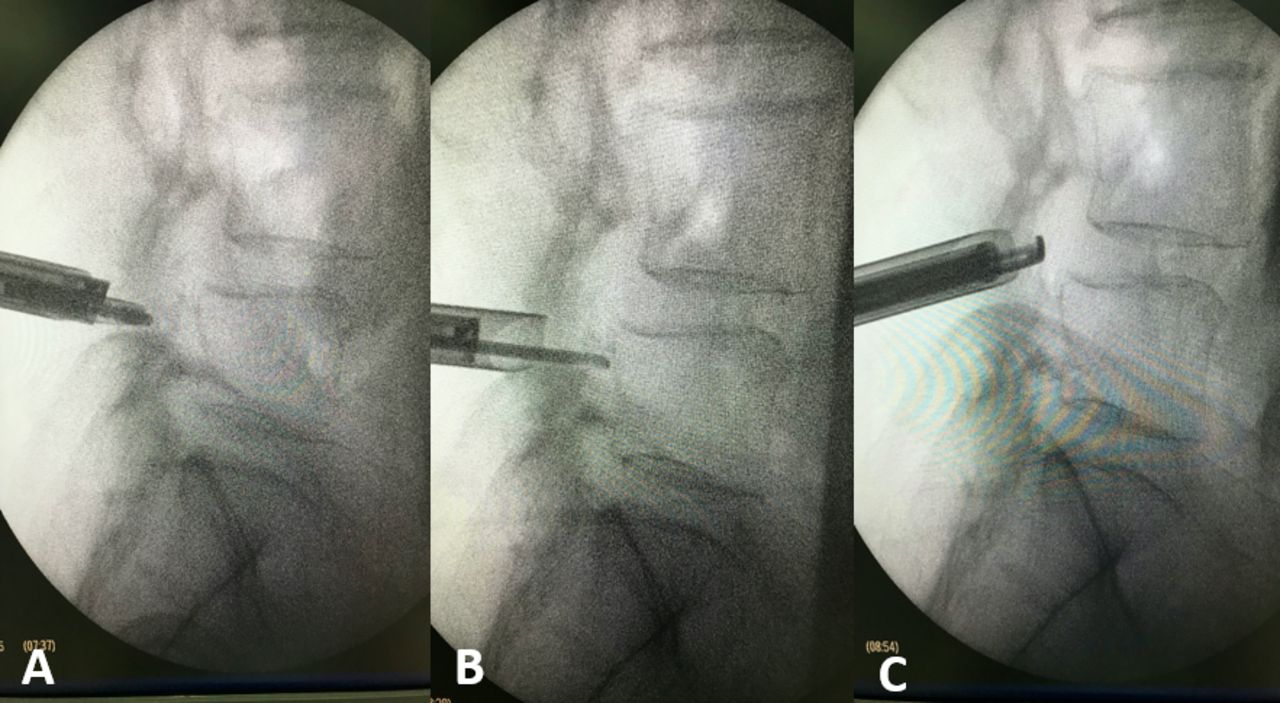
Drilling medial facet started from the midpedicle (A–B) until the tip of the superior articular process (C) to make sure complete decompression.
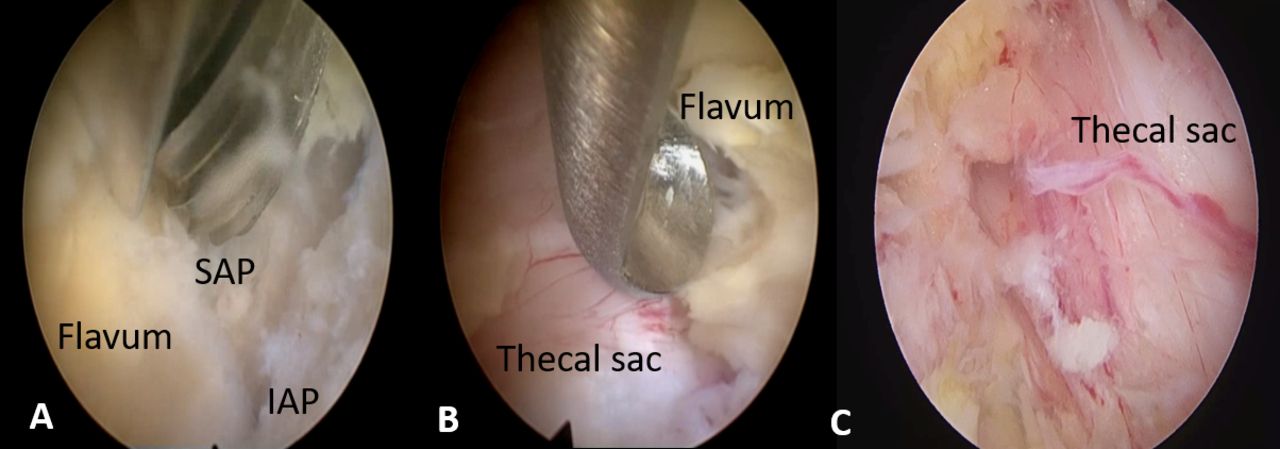
(A) Opening the lamina in the medial side. (B) Removing flavum ligament using Kerrison punch. (C) Free thecal sac after endoscopic decompression. SAP, superior articular process; IAP, inferior articular process
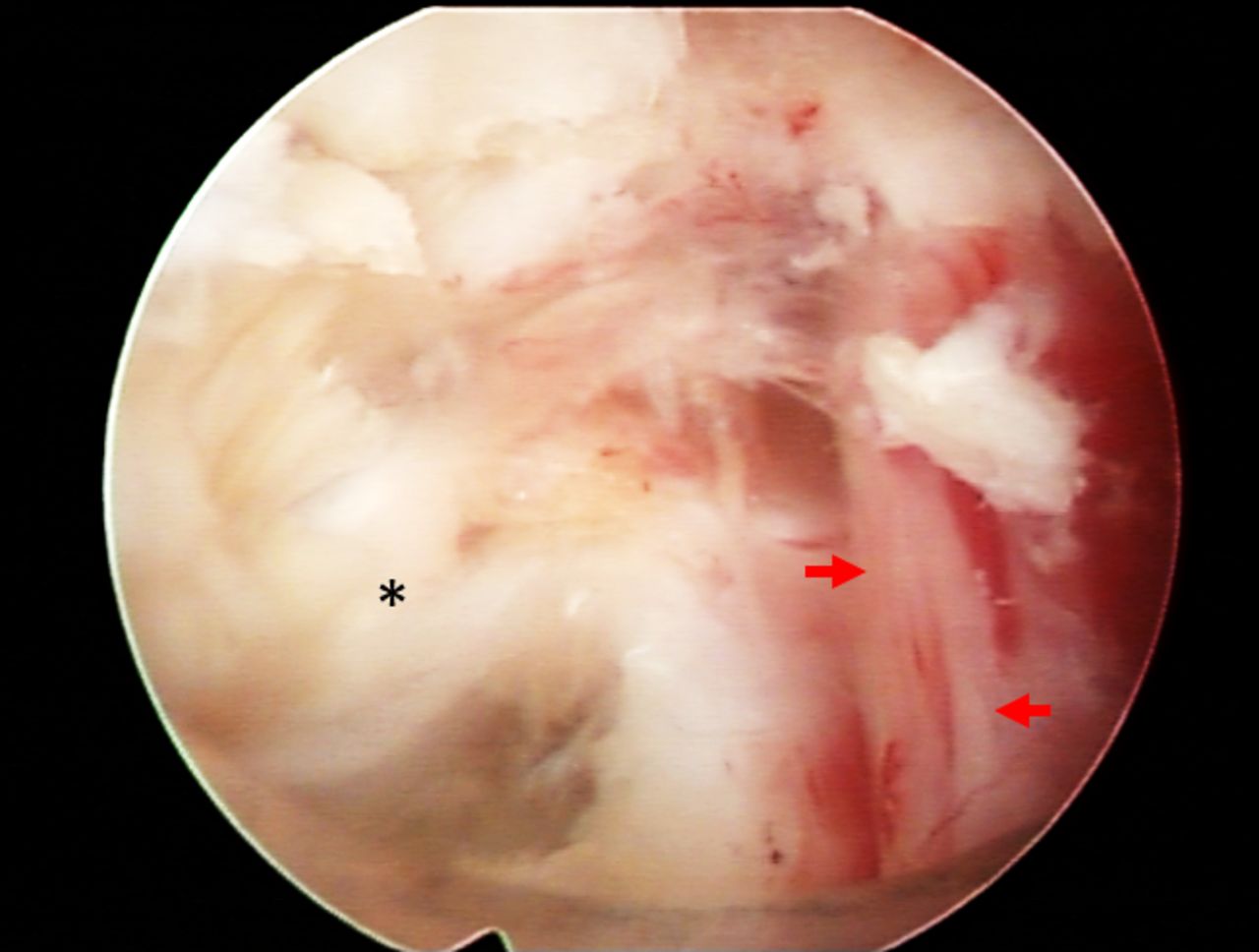
In the case of foraminal stenosis (see Video 2, Supplemental Video 2, which demonstrates endoscopic foraminotomy), the incision is located approximately 5 cm from the spinous process, and this incision is equivalent to the Wiltse approach in conventional open surgery for accessing far lateral disc herniation (Figure 3). The obturator is inserted directly into the pars interarticular, where the drilling for decompression will begin. The decompression of the neural foramen is started from the lateral part of the isthmus, removing the tip of the superior articular process, and flavum ligament until we can see the exiting nerve root (Figure 4). We did not routinely perform discectomy; it was only performed when there were disc protrusion and disc herniation (Figure 5). The parasagittal MRI was used to evaluate the foramen after the operation (Figure 6).
Online Supplementary Video 2.

Location of incision for paracentral endoscopic decompressive foraminotomy.

Free exiting nerve root and disc material that was removed. Asterisk, disc material; blue dot, disc space; red arrows, exiting root.
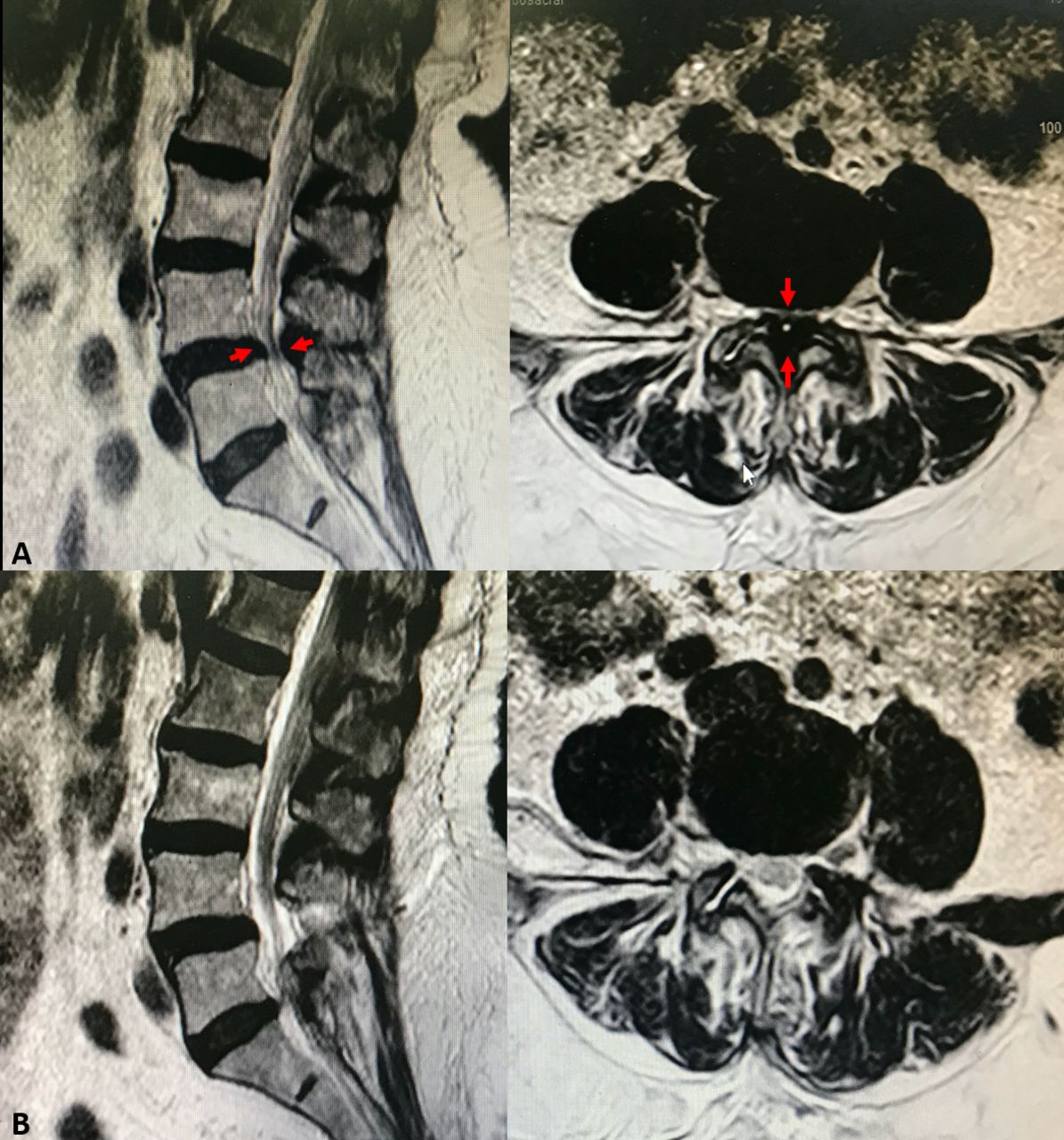
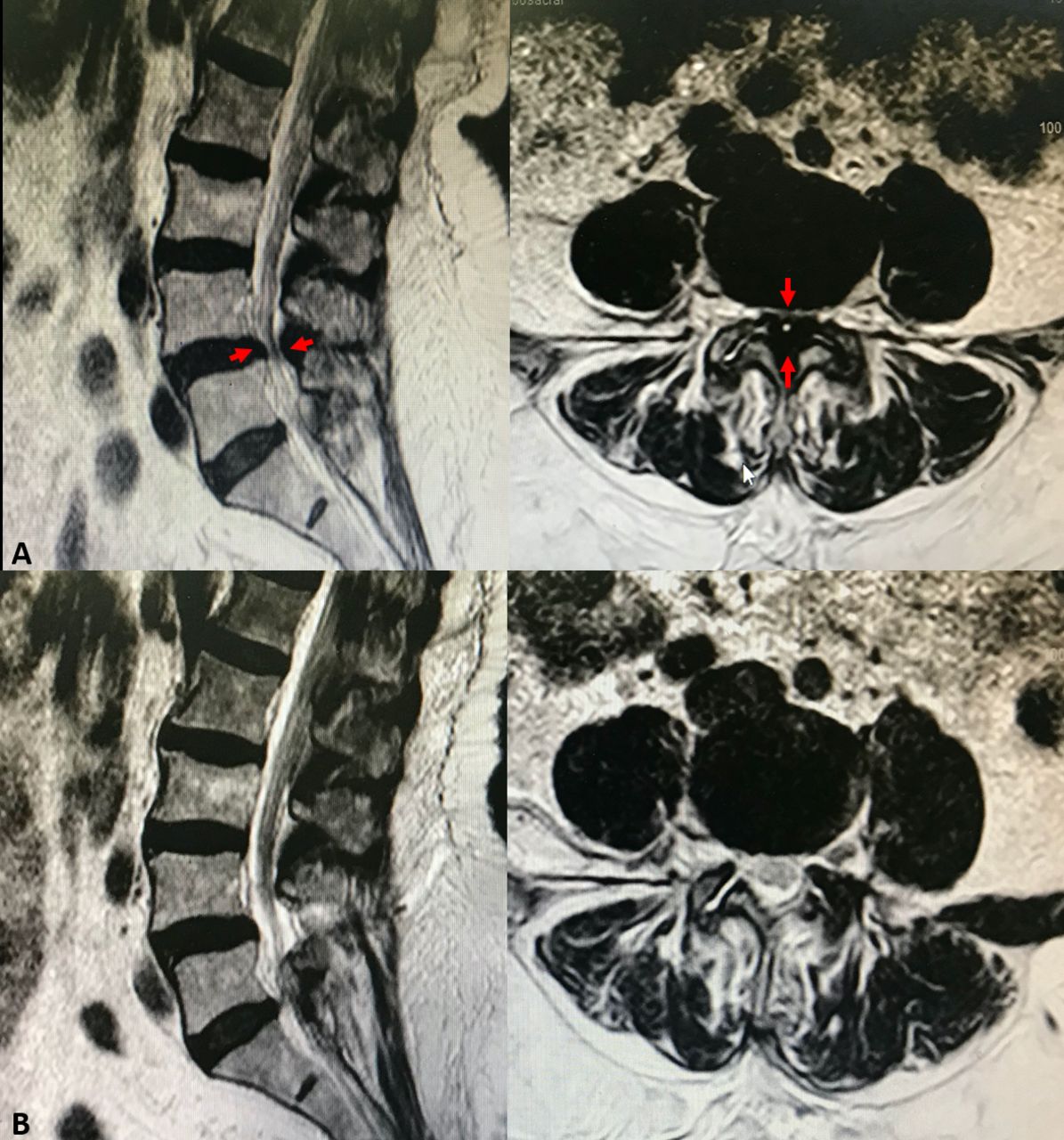
Magnetic resonance imaging (MRI) of a patient with central lumbar canal stenosis. (A) Preoperative MRI: the central canal was compressed anteriorly by the disk and posteriorly by the thick flavum (arrows). (B) Postendoscopic decompression.
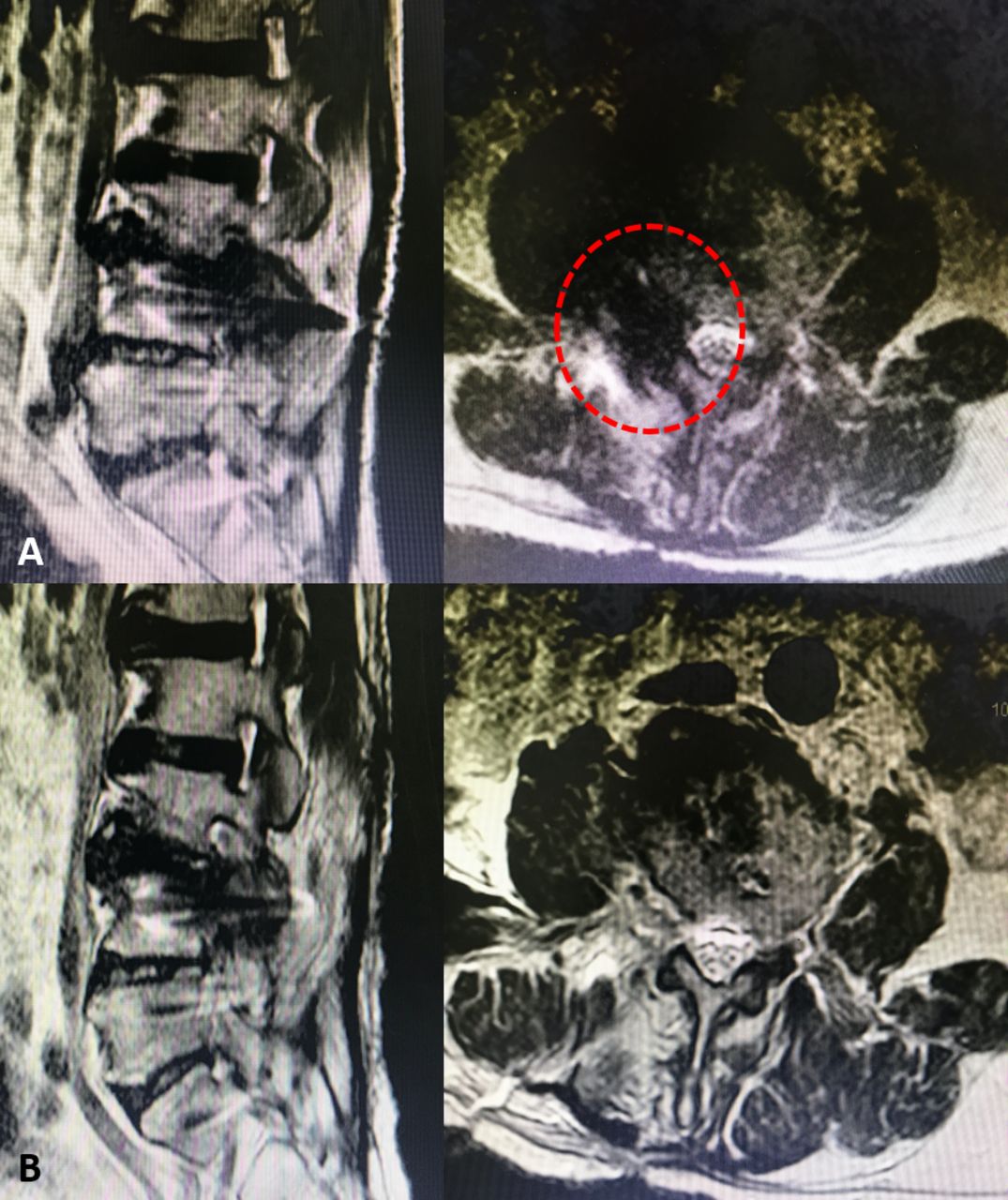
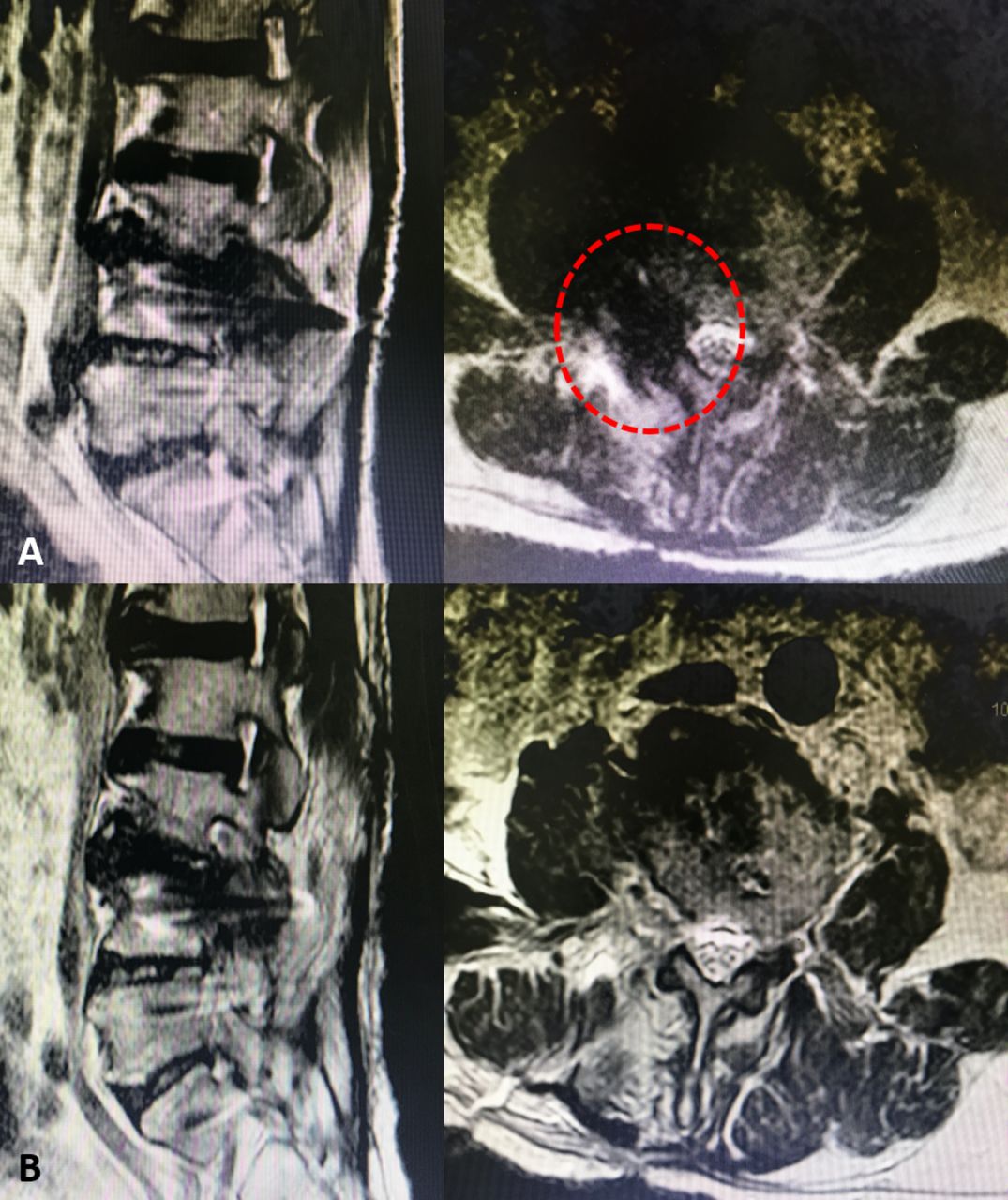
Magnetic resonance imaging of a patient with L3-L4 foraminal stenosis. (A) Preoperative: The right paracentral compression (red dots). (B) After endoscopic foraminotomy.
The endoscope itself is a rigid one with an outer diameter of 9.5 mm, an inner working channel diameter of 5.5 mm, and the lens has a 25° angle. The instrument and speed drill had diameters ranging from 3 to 5.5 mm. All of the endoscopic instruments used in this study were from Riwospine (Richard Wolf, Knitllingen, Germany).
Dynamic lumbar radiographs were measured preoperatively to exclude preoperative instability but not routinely measured in the postoperative period unless the patient suffered instability pain. Segmental angulation and degree of slippage in flexion and extension were measured from the dynamic lumbar radiograph. More than 15° of sagittal rotation angle was defined as segmental angulation, and more than 3 mm of slippage was defined as postoperative spondylolisthesis. Postoperative spinal instability was thought to have occurred if there was any abnormality in both or one of those parameters.11
RESULTS
Overall, there were 295 patients who could be followed up through 1 year. Most of the patients were in the fifth or sixth decade of life (Table 1). The nerve compressions were successfully released that was confirmed in direct vision (open surgery) and endoscopically confirmed by postoperative MRI (Figures 1 and 2). The median preoperation back pain was 2 (1–3) out of 10, which shows that all the patients had no complaint of instability. The main complaint was leg pain in the form of claudication with the median VAS of 5 (4–6) out of 10. The leg pain VAS decreased significantly on day 1 postoperation from 5 (4–6) to 2 (0–3). There were 2 patients in the endoscopic group who had postoperative epidural hematoma, which prolongs leg symptoms (Table 2). There was a significant improvement in the postoperative Oswestry Disability Index compared with the preoperative score. This result showed that both procedures were effective in managing spinal stenosis (Table 3). In the endoscopic group, the postoperative back pain was very minimal, such that almost all patients had no problem doing early mobilization within 4 to 5 hours after surgery. The conventional decompression group had a higher back VAS when compared with that of the endoscopic group (P = 0.033). Thus, more postoperative analgesics were needed to overcome the pain and motivate patients for early mobilization.
Clinical and demographic characteristics of degenerative lumbar canal stenosis patients managed with conventional decompression and full endoscopic decompression.
VAS of patients who underwent conventional decompression and full endoscopic decompression.
Oswestry Disability Index of patients who underwent conventional decompression and full endoscopic decompression.
Complications happened in both of the procedures. Dural tears occurred in 5 cases in the open decompression group and in 7 cases in the endoscopic group (Figure 5). In the open decompression group, the dural tear was repaired primarily using monofilament nonabsorbable sutures. On the other hand, the dural tears in the endoscopic group were managed only using a dural patch. There were no wound problems during the follow-up period for both procedures. There were 12 patients in the open decompression group who experienced postoperative instability back pain. In contrast, only 7 patients in the full endoscopic group had instability back pain. Among those, only 3 patients (all from the open decompression group) required reoperation with spinal fusion with instrumentation associated with the severity of clinical symptoms. Others had clinical improvement with conservative treatments. There was no neurologic deterioration in both groups.
DISCUSSION
As human life expectancy increases over the past few decades, the condition related to the degenerative lumbar spine is also increasing.1,12 The spectrum of the degenerative lumbar spine is very wide, starting from simple degenerative disc disease, simple facet arthropathy until severe deformity of the lumbar spine. The process of degeneration in the form of spondylotic changes most likely results in the narrowing of the central spinal canal or neural foramen, which causes deterioration of quality of life.13 The classic symptoms of lumbar canal stenosis is pseudoclaudication, which is characterized by leg pain, paresthesia, and/or weakness that is aggravated by standing or walking and relieved with forward flexion in the form of sitting or squatting.14
The aim of treatment in lumbar canal stenosis is to increase the walking distance without any claudication.3 A good clinical outcome is more likely to be achieved by having an adequate neural decompression without further destabilizing the joint and with minimal complication.15 The technique of decompression surgery has evolved from conventional open surgery, microscopic surgery, endoscopic-assisted surgery, and full endoscopic surgery.16
Mini-open or tubular microscopic decompression is still considered the mainstay treatment for lumbar canal stenosis.16 Even though the result of microscopic decompression was quite satisfactory, the surgeon still tries to develop the technique of minimally invasive spine surgery (MISS).17 This is due to some problems with instability and epidural fibrosis that might happen. These so-called problems of instability exist mainly due to resection of paravertebral muscle, which serves as the posterior tension band and too much bony resection on the medial facet joint. The probable cause was the approach itself and the inability to look clearly into the surgical field in order to get complete decompression due to sharing the same space for lights and instruments. Endoscopic surgery can overcome this problem by less paraspinal muscle injury and targeted bony resection.18
Endoscopic spine surgery has the advantage of viewing capability into the operative field. The lens which is equivalent to our eyes is located very close to the operative field, and the endoscope has a designated channel for the lights and operative instruments.19 The use of 12°, 20°, or 25° lens configuration enables the surgeon to view clearly into the area that is quite invisible in open surgery without resecting too many bone structures, especially on the undersurface of the medial facet joint. Continuous water irrigation also helps to create a better view and better bleeding control compared with air-based procedures using microscopes.20
The results of our study showed that endoscopic surgery had a better direct postoperative outcome in the form of back pain. VAS in the endoscopic group had a median of 2 compared with 4 in the conventional group with a P value of 0.033. The less muscle dissecting approach—without damaging the posterior tension band—in the endoscopic group was probably the biggest contribution to reducing the postoperative back pain. This is also consistent with a shorter hospital stay in the endoscopic group, which is only 1.5 days. The leg pain VAS consistently had better results compared with preoperation in both groups, which showed both procedures were effective in managing lumbar canal stenosis.
Maintaining spinal stability is essential after any spinal surgery. In the open technique, muscle detachment and bony removal disrupt the surrounding stabilizing structures. However, surgical techniques have evolved over time to allow adequate decompression while minimizing the risk of iatrogenic destabilization. There are options for decompression techniques in open surgery such as total laminectomy, partial laminectomy, and unilateral or bilateral laminotomy. Total laminectomy is preferable for patients with severe degenerative stenosis or marked degenerative instability (spondylolisthesis). However, posterior decompression without fusion with instrumentation leads to patient dissatisfaction in approximately one-third of patients. In Lee et al’s11 study, bilateral laminotomy was found to be superior compared with unilateral laminotomy and laminectomy, with significantly improved outcome parameters.11
In our study, there was neither preoperative instability nor severe degenerative cases. Thus, we found that bilateral laminotomy adequately decompressed the thecal sac. Some patients in the open decompression group still developed postoperative instability. This may be related to muscle detachment during lamina exposure. Although Mosenthal et al’s21 study showed that there were no reoperations for instability in the bilateral laminotomy group compared with the laminectomy group, we performed posterior fusion and stabilization in 3 patients who suffered from severe instability pain.21,22
MISS is an effective procedure with favorable results when used in patients who have stable degenerative spondylolisthesis and concurrent stenosis. It can preserve the attachment of intervertebral muscles, facet joint capsules, and ligaments that stabilize the spine. Thus, it potentially minimizes the risk of instability that comes with a larger exposure, which violates more spinal stabilizers. Moreover, the slippage rate did not progress 2 years after the operation. In a study by Sriphirom et al,23 28 patients with stable degenerative spondylolisthesis who underwent full endoscopic decompression showed that there was a nonsignificant difference in pre- and postoperative disc height ratio and vertebral slippage percentage. In contrast, in our endoscopic group, there was a destabilization process in those patients with pre-existing stable grade 1 or 2 spondylolisthesis, which led to postoperative instability.23 This interesting finding needs to be evaluated further to seek other possibilities that might contribute to postoperative instability in endoscopic spine decompression or other MISS.
In terms of surgical care cost, the concept that the greatest variability in cost lies within operating room expenses and implant costs is a common misunderstanding. In our center, the surgical care cost (acute care) is approximately 50 million rupiahs (3500 USD) vs 60 to 65 million rupiahs (4500 USD) for open decompression and endoscopic decompression, respectively (about 1000 USD for endoscopic system and single-use instrument). However, the growing evidence suggests that by far the greatest variability in surgical cost lies within the postacute care episode (immediate days to weeks postoperatively following hospital discharge). It is during this period that the potential value of MISS is the greatest. The length of stay, surgical complications, hospital readmission, reoperation, and the need for inpatient rehabilitation or skilled nursing care are significant factors that can greatly reduce costs in the postoperative period. MISS can reduce the prevalence of any of these events, which further significantly affect the total health care cost.24
In our study, intraoperative bleeding, operation duration, length of stay, and mobilization time are significantly better in the endoscopic group, which may lead to a significant reduction in total estimated health care cost. This result supports 14 meta-analyses, which showed both cost savings and better outcomes in MISS compared with an open approach.24
The endoscopic procedure is not without disadvantages. The first problem to be encountered is the learning curve, and the surgeon needs at least 10 to 20 cases before they can perform endoscopic surgery.7 Converting 3-dimensional images into 2-dimensional images and coordinating hand-eye movement without seeing directly are not easy tasks to do. The other problem is also handling the instrument, which is quite challenging. Because the working channel only allows 1 instrument at a time, we could not use a double instrument such as the combination of Kerrison punch and dissector to release adhesion between dura mater and flavum ligament.25
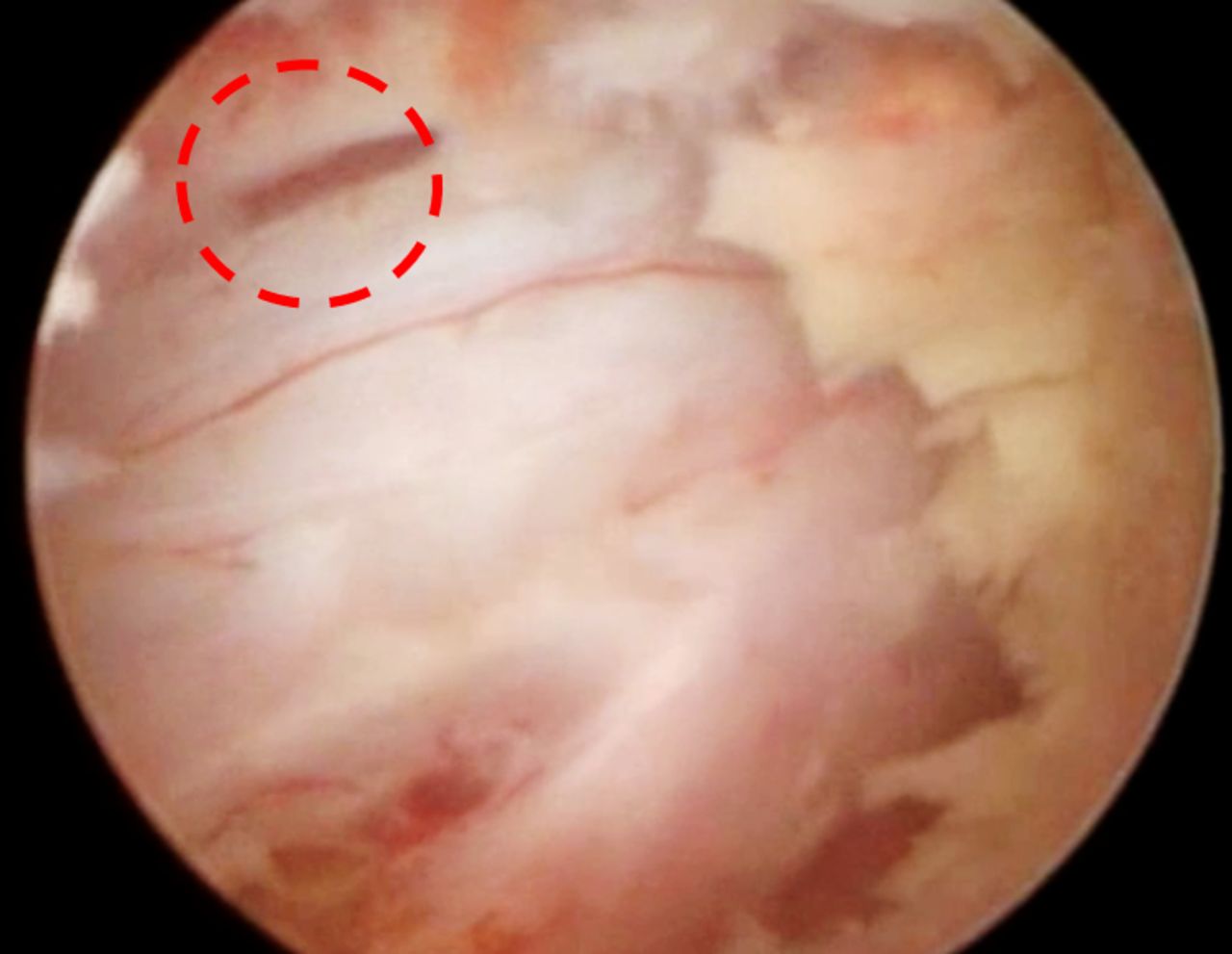
Managing intraoperative complications during the endoscopic procedure is not as easy as an open procedure due to limited field and some technical issues (Figure 7). For example, during endoscopic procedures, the dural tear is not easy to identify because of the continuous water flow. In the case of identified dural tear, primary suture with endoscopy is not a routine procedure. Surgeons sometimes cover the tear using the dural patch or if the tear is quite big then we need to consider converting to open surgery.26 In our study, all of the dural tears that happened in the endoscopic group were managed by the dural patch only. We did not find any postoperative symptoms or complications. Even though wound complications rarely exist after a dural tear and reconstruction usually is not required when using the intermuscular approach, recently a lot of research developing tools for repairing the dura mater endoscopically has been conducted.

Image of dural tear during endoscopic procedure (red circle).
Finally, either tubular microsurgery or endoscopic surgery is a good option to be selected in specific cases, but it is well known that the main limitation of either procedure stays in the number of levels that can undergo decompression. In the case of multiple-level involvement, conventional open surgery is still superior.27
CONCLUSION
The result of our study showed that the fully endoscopic procedure had a potentially excellent result. The development of endoscopic surgical instruments enables us to perform decompression in the same or even more effective way compared with conventional open decompression surgery. Although there are still some limitations regarding the surgical indication, techniques, and instrumentations, advancing knowledge and technology will prompt this endoscopic procedure as the next gold standard in managing degenerative lumbar canal stenosis.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval This research was approved by ethical committee in Fatmawati General Hospital Jakarta.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.