


Abstract
Background Bone autograft options may be limited in revision spinal fusion cases. Reconstruction of the iliac bone graft (IBG) donor site with cancellous bone allograft allows for reharvest for patients who subsequently have another fusion. This study examined viability of the reconstructed IBG (RIBG) donor sites. Secondarily, we assessed the feasibility of whether the RIBG sites could be reharvested for obtaining a successful arthrodesis for a secondary fusion.
Methods Prospectively collected data of 154 consecutive lumbar revision fusions were reviewed, of which 17 cases had their IBG donor site backfilled with allograft bone at the time of their primary fusion and subsequently had secondary surgery for a pseudarthrosis repair or fusion extension. Biopsies of the RIBG and computed tomography (CT) images were obtained at the time of secondary fusion. Histology analyzed the ratio of filled to unfilled lacunae and marrow cellularity. Histology controls were from normal iliac crest. Clinically, postoperative CT and >2-year outcomes (visual analog scale [VAS] and Oswestry Disability Index [ODI]) evaluated the feasibility of the secondary fusion surgery using RIBG. The RIBG fusion rate and outcomes were compared with clinical control revision groups that had IBG and/or bone morphogenetic protein (BMP) used for their revision fusion.
Results CT images prior to RIBG harvest found bony healing of the original graft donor site in all except 1 case. RIBG bone marrow histology found lower cellularity vs controls, but this characteristic did not appear to compromise bone viability with filled lacunae in 83% ± 14% in the RIBG group, vs 88% ± 8% for iliac controls. After revision fusion, often combined with bone growth stimulator or BMP, repeat CT demonstrated solid spinal fusions in 16 of 17 patients, whereas control revision group fusion rates were approximately 80%. Clinical improvement was significant (VAS decrease = 3.8, ODI decrease = 16.5) and comparable with the IBG revision controls.
Conclusion RIBG using allograft remodels into viable predominately cancellous bone and is clinically feasible for revision fusion if IBG or BMP is unavailable.
Clinical Relevance Reconstructed iliac bone graft is viable and may be used as a bone graft option.
Level of Evidence 3.
- bone allograft
- bone histology
- bone morphogenetic protein
- iliac bone graft
- iliac reconstruction
- nonunion
- pseudarthrosis
- revision spinal fusion
Introduction
Iliac bone graft (IBG) is the preferred biological material for posterior spinal fusion of the thoracolumbar spine since it is osteoinductive, osteoconductive, and osteogenic and is the standard reference to which other bone biologics are compared.1,2 For secondary fusion surgery, such as a posterior pseudarthrosis repair or fusion extension of adjacent spinal levels, the contralateral IBG is typically harvested. In some circumstances, such as for multilevel cases, when multiple prior fusions were performed with IBG or if iliac fixation was used, both iliac crests may not be available for harvest, and the bone autograft supply may be insufficient, then a bone graft substitute is necessary.
Alternatives to IBG include nonviable bone allograft, demineralized bone matrix, ceramics, and synthetics. Most alternatives result in low fusion rates, and even with the addition of autograft bone or osteoprogenitor cells (ie, bone marrow aspirate) the fusion rates are variable for primary fusion.2–8 In revisions, particularly in multilevel cases, in which the fusion bed environment is compromised, these alternatives are not reliable. Relative to other bone graft substitutes, bone morphogenetic protein (BMP) has a high success rate for both primary and revision posterior spinal fusion.5,6,9–14 Although BMP is the preferred biologic for revisions, this off-label use is increasingly being denied by payers and hospitals.15 Many facilities prohibit BMP due to its expense and safety concerns.16
Reconstructed iliac bone graft (RIBG) donor site has previously been described for decreasing postoperative pain at the donor site.17 Potentially, RIBG may also be a source of additional bone for secondary fusion surgeries. A viable bone graft option has potential advantages of more consistent healing; however, the viability of RIBG is unknown.
The lead author (G.R.B.), with >20 years of experience, has consistently reconstructed the iliac crest donor site after IBG harvesting using bone allograft cancellous chips to reduce donor site pain. For a small number of patients who had secondary surgery after prior IBG reconstruction, this site was considered a source of bone graft. We hypothesized that RIBG site would remodel to viable bone. The primary purpose of this study was to assess the viability of the RIBG site through histological evaluation. A secondary purpose was to assess the clinical feasibility of RIBG site reharvest for secondary fusion and obtain a successful arthrodesis with related clinical outcomes in a small pilot sample of revision fusion patients. Due to differing graft bed environments, the secondary fusions were subanalyzed for treatment for pseudarthrosis versus adjacent segment conditions requiring fusion at levels either above or below a prior fusion.
Methods
During an 8-year period, 945 patients had thoracolumbar fusion, 154 of whom had secondary (revision) fusions. Prior to and during this period, the author routinely used IBG and reconstructed the donor site with allograft bone at the time of their original primary fusion to effectively reduce donor site pain. At the time of their original fusion surgery, the posterior superior iliac spine was harvested for ~25 cc of cancellous bone autograft using an intracortical window technique.18–20 The donor site was reconstructed using at least 30 cc of freeze-dried cancellous allograft cubic chips (~5 mm size, MTF Biologics, Edison, NJ). The chips were gently impacted into the iliac defect, resulting in light crushing of the chips similar to prior reports.21,22
The revision fusion patients, who having failed nonoperative treatment for pseudarthrosis or adjacent segment conditions, underwent lumbar computed tomography (CT) imaging and then secondary revision spinal fusion using various bone graft sources: contralateral IBG (preferred), BMP (preferred), local autograft (single level), or RIBG (if IBG not available and/or BMP use restricted). The RIBG was the study cohort, and the other groups were the “clinical control” (CC) groups of secondary fusion. RIBG cases (n = 18, 12%) did not have IBG/BMP options as they had had IBG harvested for prior remote cervical or thoracic posterior fusions without reconstruction of the donor site so that only 1 remaining IBG site was available for the patient’s primary lumbar fusion; 2 had bilateral iliac fixation. Study inclusion criteria were patients who had both their original and secondary fusion by the lead author. This subset of revision fusion cases had 18 consecutive study patients who fit the inclusion criteria had iliac crest reharvested from RIBG for either a pseudarthrosis repair (n = 7) or extension above a prior multilevel lumbar fusion (n = 11) and were followed prospectively.
At the time of revision surgery in the fusion extension cases, typically, those whose fusion extended 1 or 2 levels had bone graft obtained from the RIBG only. Given the unproven osteogenic potential of RIBG, those who were smokers and those having >2-level fusion extension had additional supplemental treatments to the fusion site, as did all the pseudarthrosis repair cases to optimize successful revision fusion, specifically, an internal bone growth stimulator (BGS; EBI SpF, Parsippany, NJ), or BMP (small InFuse, Medtronic, MN) (Table 1). No other autograft or allograft/synthetic products were used. Clinically, the consecutive RIBG revision posterior fusion study cases were evaluated prospectively with visual analog scale (VAS) and Oswestry Disability Index (ODI) outcomes at 1 and 2+ years. One year after revision, all had high-resolution CT images and radiographs for final fusion assessment. The clinical feasibility portion of this study also tracked complications directly related to RIBG and it’s reharvest. Additionally, outcomes were compared with the control groups to assess whether revision fusion with RIBG had an adverse clinical effect.
Bone graft types used for revision posterior fusion.
The pseudarthrosis CC consisted of 53 patients (17 of whom had the primary fusion performed by the senior author); many had an internal BGS used at the revision fusion. All these consecutive pseudarthrosis CCs had 1 year postoperative high-resolution CT images to assess healing of their revision fusions. During this same study period, another 83 patients had extension of their prior thoracolumbar fusion at the adjacent levels above or below the index fusion (extension CC), 53 of whom had their primary surgery performed by the senior author). Postoperative CT images were available in 80 of extension CC patients to assess revision fusion healing. All 154 revision patients also had prospectively obtained clinical outcomes (VAS and ODI) and preoperative CT of the lumbar spine that included the superior pelvis (and RIBG site) prior to the revision surgery. The distribution of types of bone grafts and use of BGS are shown in Table 1.
Histological analysis of the 18 RIBG cases was performed on the reharvest samples. At the revision fusion, 20 to 25 cc of grossly cancellous RIBG were used for bone graft, of which 0.5 cc of the curettings were reserved for histological analysis. Biopsies were bathed in formalin bath at harvest, then simultaneous fixation and decalcification for 1 to 2 hours. The samples were then embedded in paraffin for preparation of routine 5-μm histologic sections that were stained with hematoxylin and eosin. These standard stains reliably identify live osteocytes with dark staining of oval or round nuclei.23,24 Histology analyzed marrow cellularity and the ratio of filled to unfilled lacunae. Counted osteocytes were those within lacunae. Peripheral osteoblasts were noted but not counted.
Each patient had 2 to 4 slides analyzed, of which the median osteocyte count was used to represent that patient. Excluding 1 patient diagnosed with connective tissue disease (Ehlers-Danlos), histology was analyzed for 17 patients. Bone marrow was assessed and graded as hypercellular, normocellular, or hypocellular based on the age of the patient.25–27 To account for variability of osteocyte counting under high power, low-power analysis was performed to determine the percent of trabeculae with >1 osteocyte (indicative of viability).
Normal, histology control (HC) specimens were screened from 220 iliac bone marrow samples submitted for possible diagnosis of new hematologic disorder or malignancy to be age- and sex-matched to the RIBG specimens. They were prepped and had standard hematoxylin and eosin staining in the same laboratory as the RIBG specimens. Additional specialized stains were also used to rule out hematopoietic neoplasia, and none were identified. Of this control sample, 17 were of the same sex and comparable age distribution and were free of malignancy, infection, ischemic injury, or metabolic disorder. These HC specimens were analyzed identical to the RIBG histology. Institutional review board approval was obtained in 2005 for biopsy of the RIBG sites during the secondary fusion, as well as for control histology screening and analysis.
Statistical analysis included between group and within-group paired t tests over time for the change in the pain and disability parameters from preoperative values. The marrow cellularity and filled lacunae count were compared between groups including using the Wilcoxon rank sum as the data were not normally distributed. χ 2 testing analyzed difference in fusion rates.
Results
The average ± SD age of the RIBG case series was 55.3 ± 8.6 years (Table 1). The RIBG pseudarthrosis repair cases (n = 7) had an average time span between index surgery (which included reconstruction of the IBG donor site) and pseudarthrosis repair of 2.3 years. These patients had risk factors for pseudarthrosis including 6 patients who were smokers and one who had undergone 3 prior decompressions at the fusion level with advanced fibrosis and hypovascularity at the fusion bed. Six in this pseudarthrosis repair group had multilevel fusion, 3 had a remote history of pseudarthrosis of another spinal region, and 4 had prior contralateral IBG harvested for other spinal fusion procedures (thus they had bilateral prior IBG harvest prior to pseudarthrosis repair). The RIBG spinal fusion extension patients (n = 10) had an average time span between index and secondary surgery of 9.5 years. This group had 6 smokers. There were no complications related to the surgical procedure (infection, iliac fracture, and prolonged pain at the harvest site) at the time of initial reconstruction or at the time of reharvest of the RIBG.
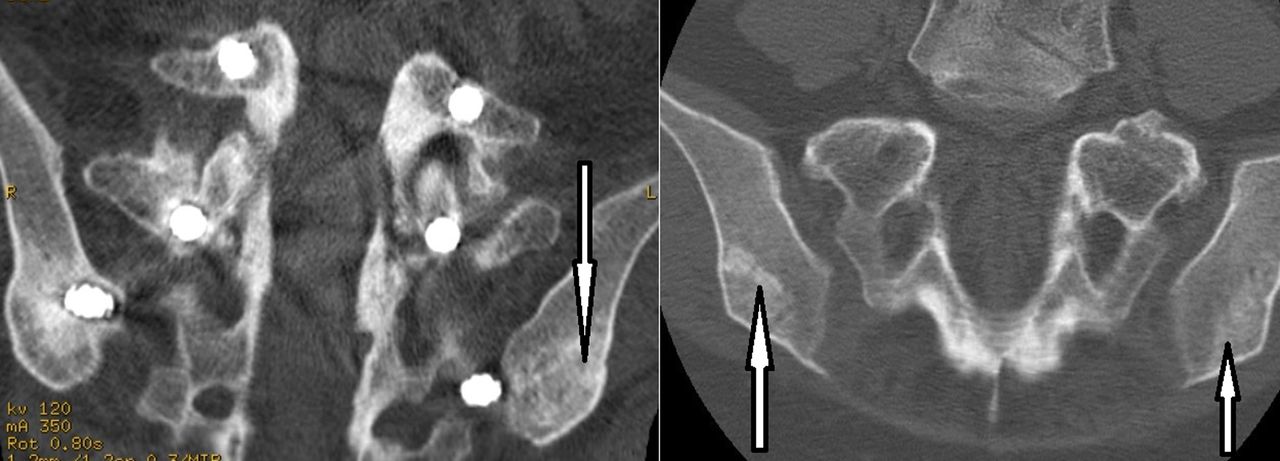
CT imaging prior to the secondary fusion surgery found 16/17 cases that the RIBG had been completely filled, and 1 partially filled, the original iliac defect. The 1 RIBG site that was not completely filled was in the fusion extension group; this patient who was a smoker developed a nonunion of the revision fusion. The RIBG site appeared completely cancellous in 8/17 and cancellous with small cortical islands in 9/17 patients (Figure 1).
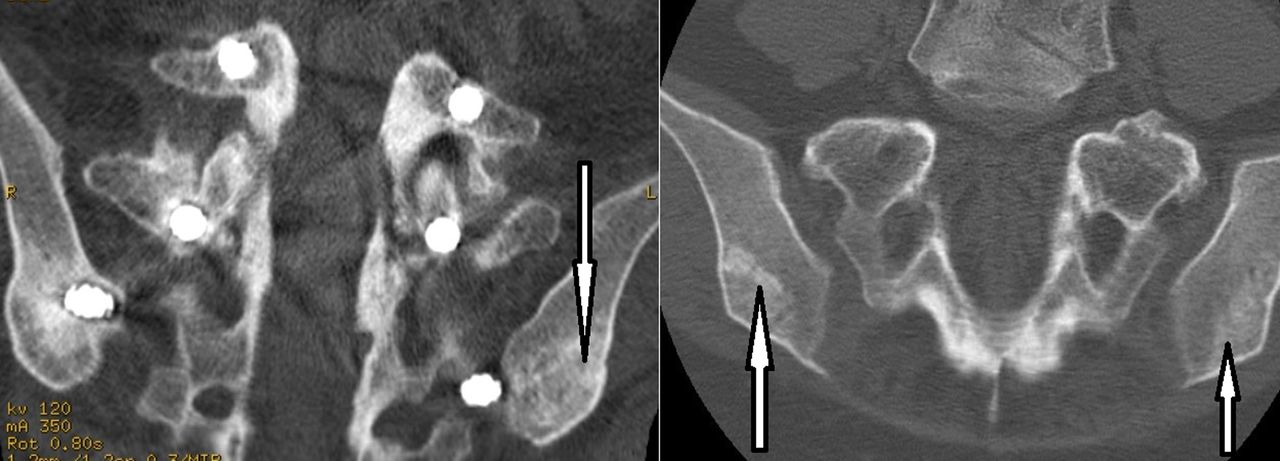
Representative computed tomography image of reconstructed iliac bone graft (RIBG) prior to secondary surgery and reharvest. The left image demonstrates cancellous with interspersed regions of cortical bone appearance of RIBG. This patient had 3 prior surgeries for scoliosis, adjacent segment deformity, and later for adjacent segment stenosis over a 15-year period. Iliac fixation is identifiable. The right image demonstrates both cancellous bone (far right) and cancellous with interspersed regions of cortical bone (left arrow). Arrows indicate RIBG.
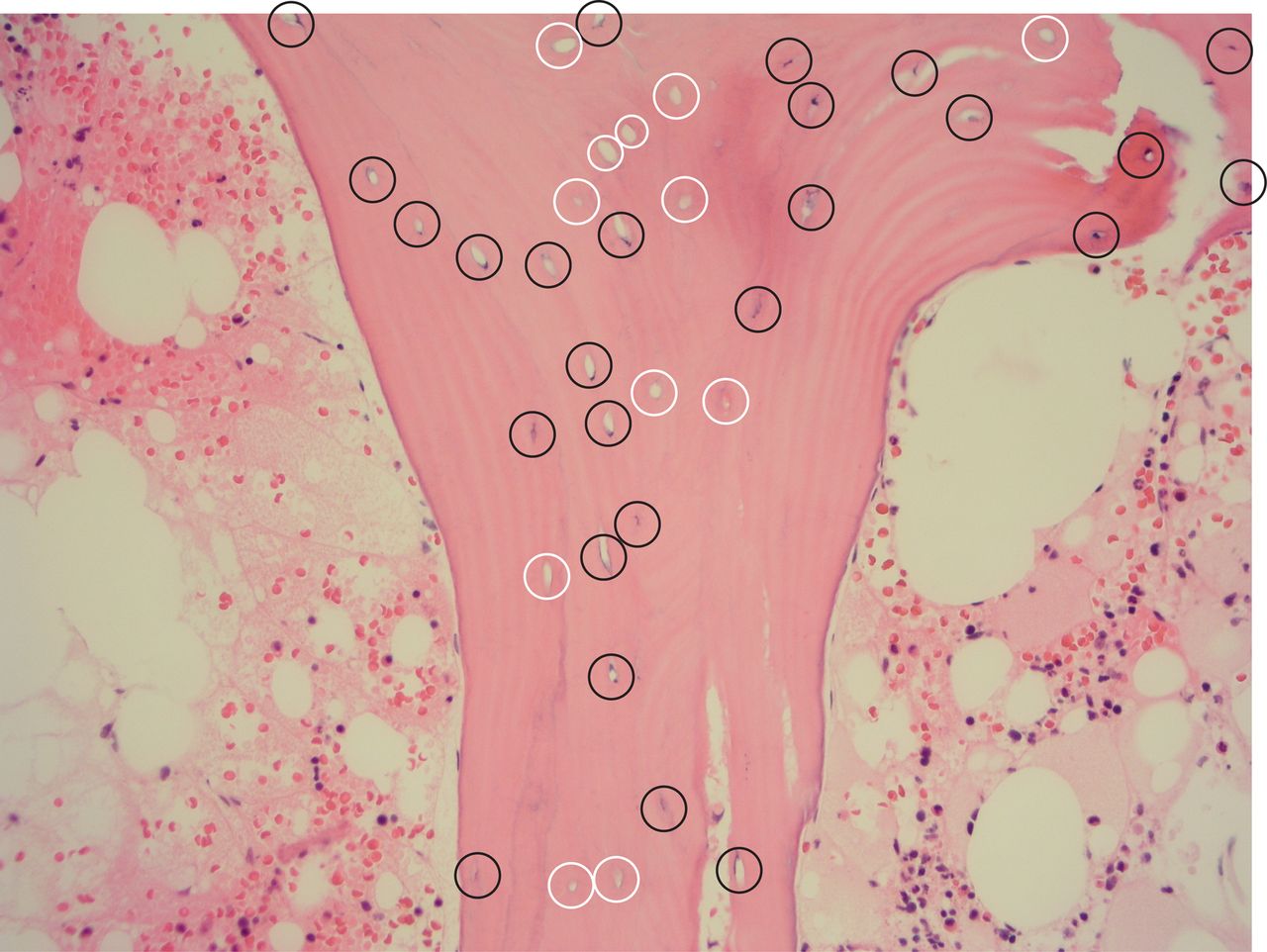
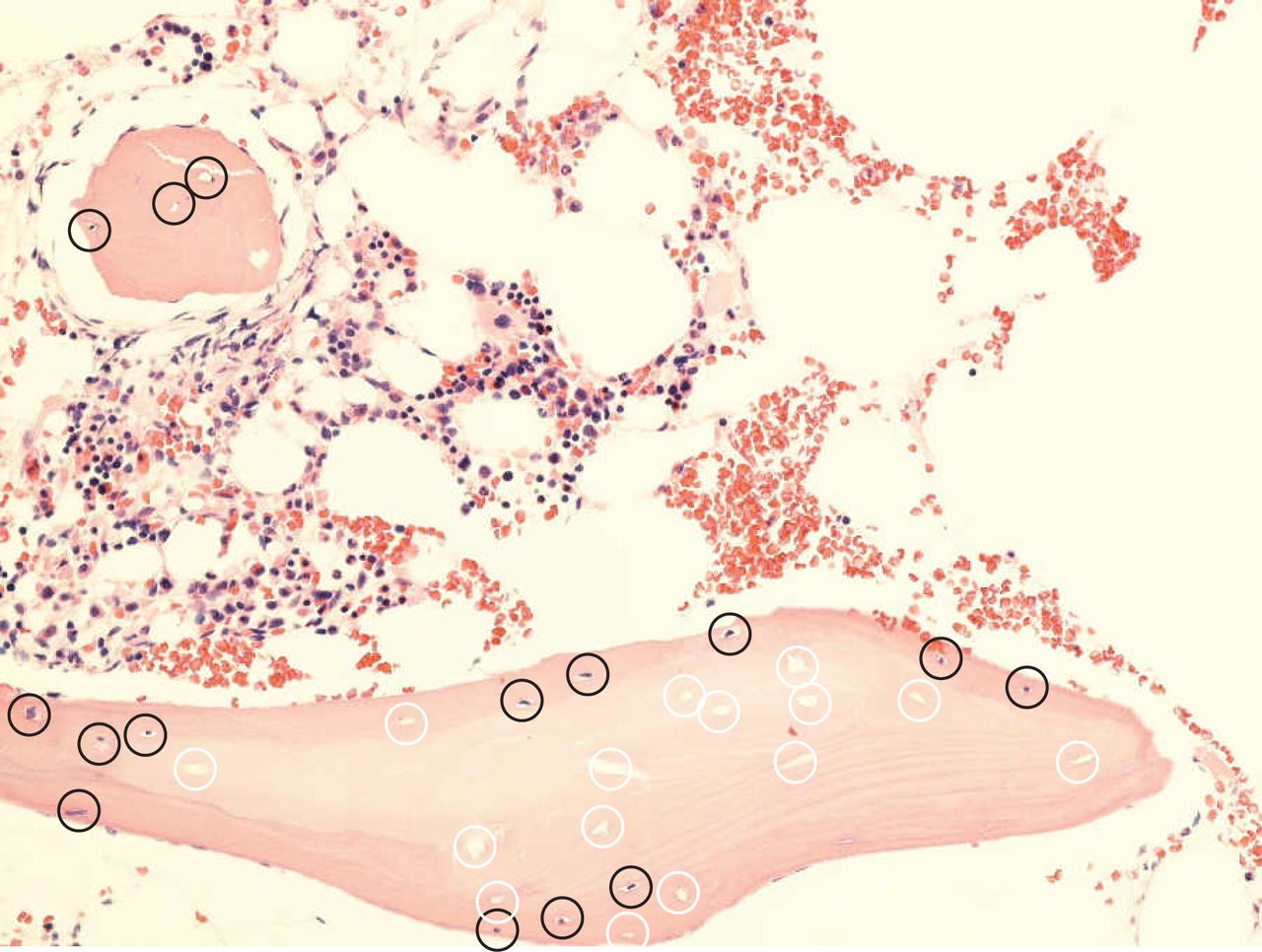
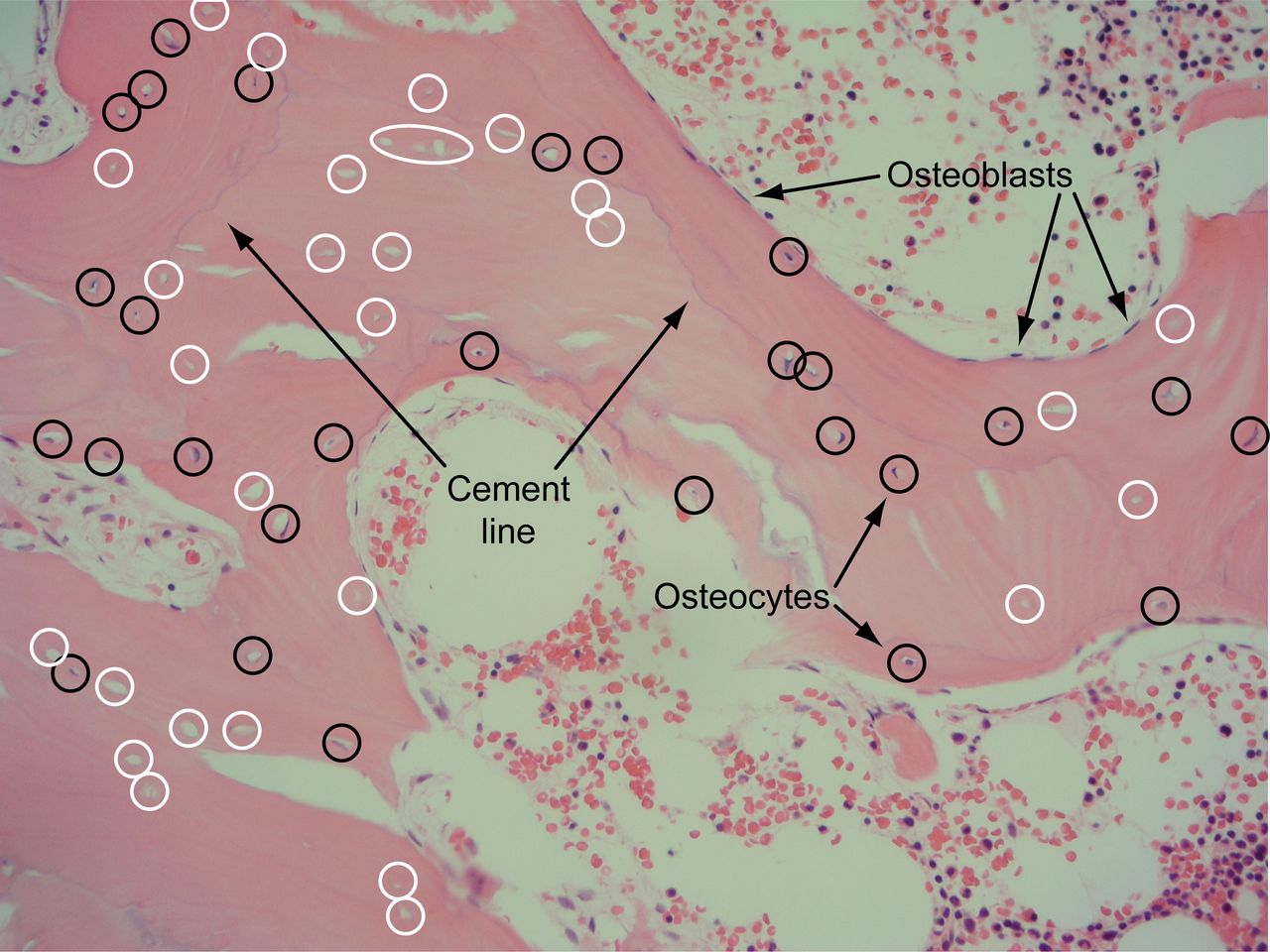
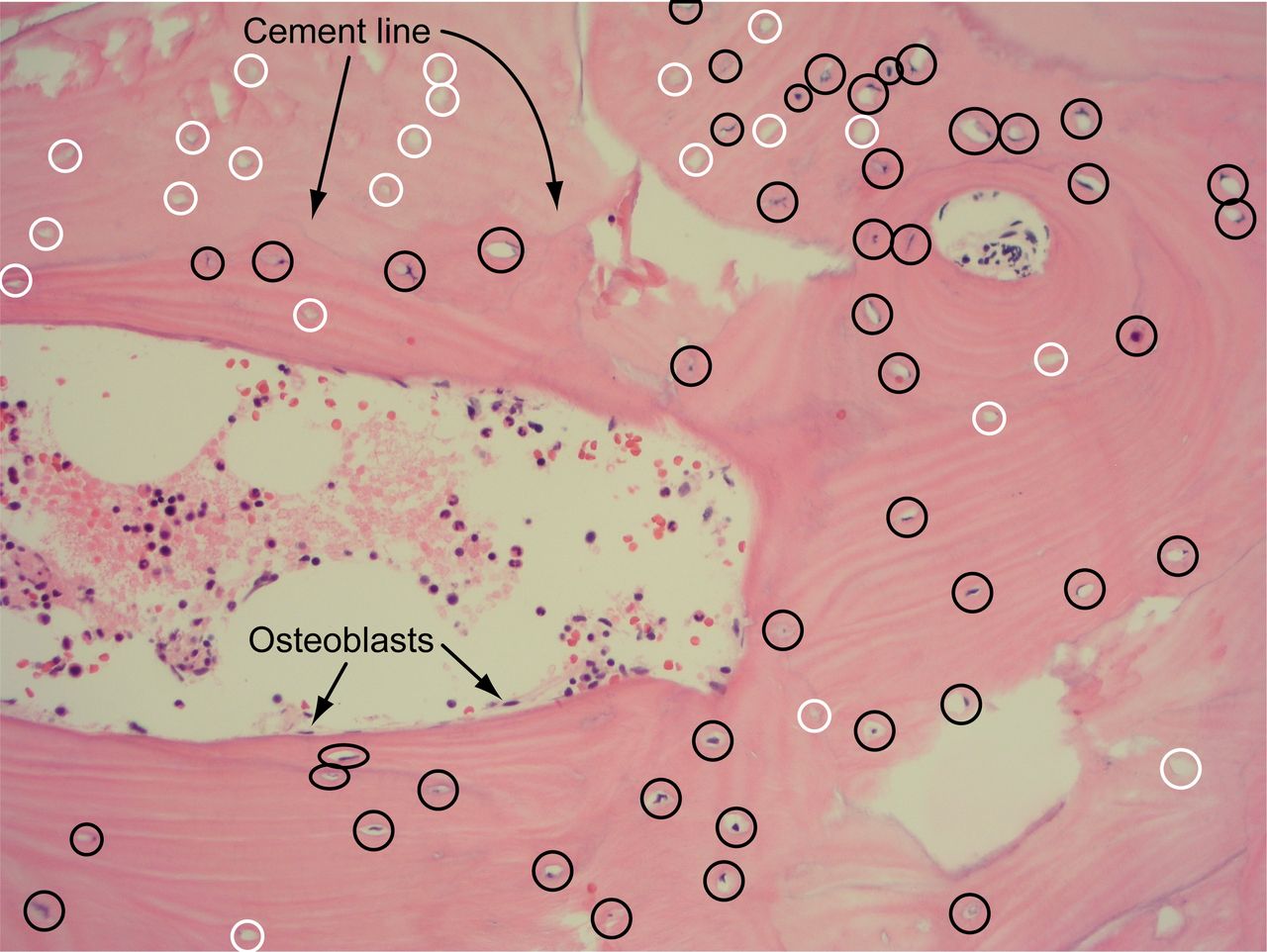
All histology samples of the RIBG case series identified cancellous bone with focal variability in filled vs unfilled lacunae (Figures 2–5). Figure 2 exhibits filled lacunae (viable osteocytes) vs unfilled lacunae (nonviable osteocytes). The distribution of filled lacunae was not uniform within the remodeling bone (Figures 3 and 4). Cement lines were also identified as a boundary between viable bone (osteocytes with filled lacunae) and unfilled regions (Figures 4 and 5). Osteoblasts could also be identified on the periphery of viable bone.
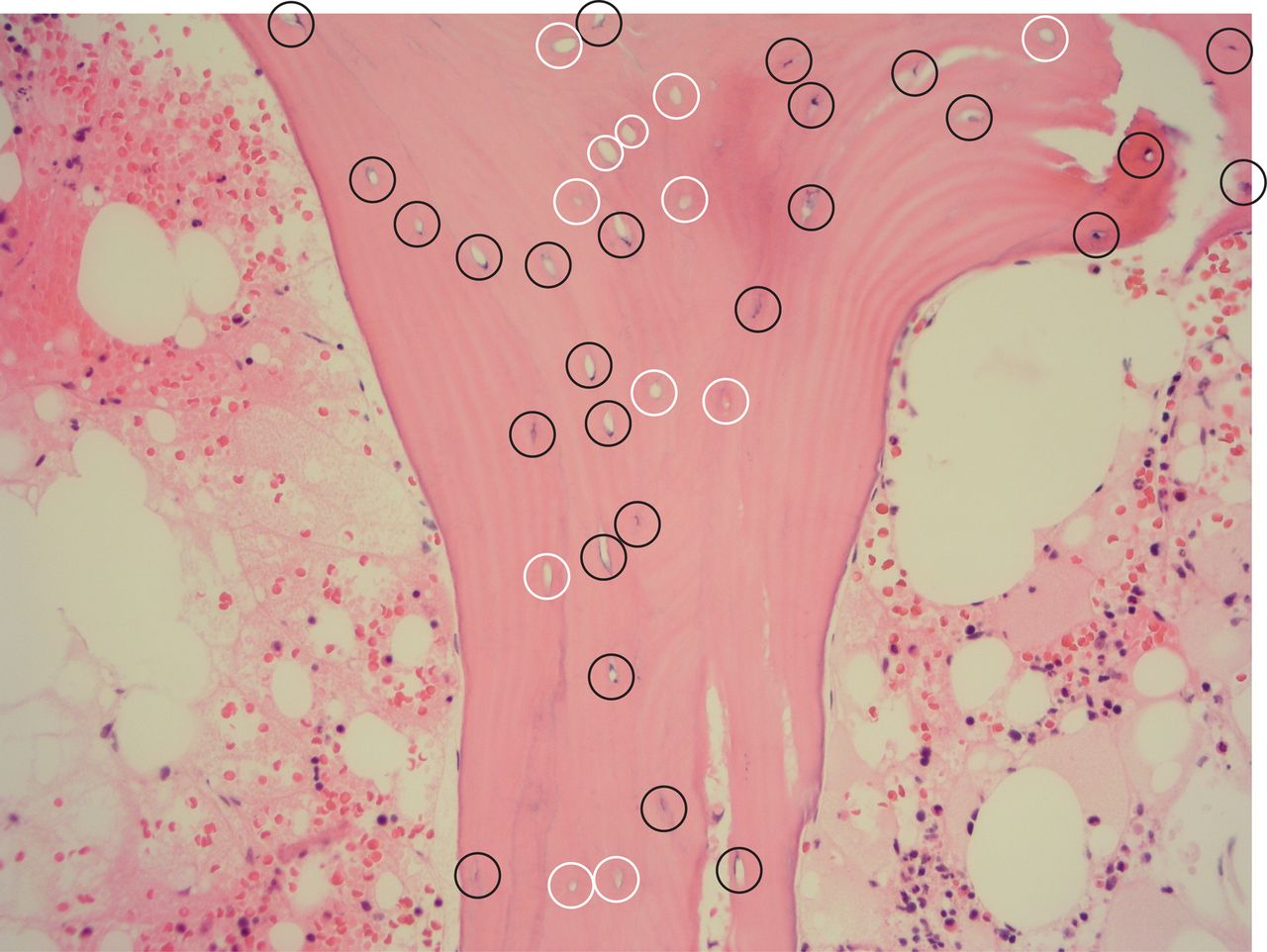
Representative reconstructed iliac bone graft histology (hematoxylin and eosin stain) of filled (dark circles) and unfilled (white circles) lacunae representing viable and necrotic bone, respectively. Lamellae are seen in the viable bone region. Original magnification ×200.

Histological section (hematoxylin and eosin stain) demonstrating region of viable reconstructed iliac bone graft bone with filled lacunae (dark circles) surrounding a region of necrotic bone with unfilled lacunae (white circles). Original magnification ×200.

Histological reconstructed iliac bone graft section (hematoxylin and eosin stain) demonstrating “cement line” (arrows) between region of filled lacunae (dark circles) surrounding a region of predominately unfilled lacunae (white circles). Marrow is also represented. Original magnification ×200.

Histological reconstructed iliac bone graft section (hematoxylin and eosin stain) demonstrating “cement line” (arrows) and region of filled lacunae (dark circles) predominately on lower side of cement line compared with a region of predominately unfilled lacunae (white circles) above the tidemark. This image also demonstrates a concentric arrangement of the lamellae in addition to longitudinally arranged lamellae. Original magnification ×200.
For the entire RIBG group, the percentage of osteocytes, identified by filled lacunae, was 82.7 ± 14.1% (mean ± SD), which was not significantly different than HC values of 87.8 ± 7.5% (P = 0.242, Table 2). Although the patients who had a fusion extension had a longer time period for the allograft to transform into viable autograft, there was no significant difference in the percentage of filled lacunae between groups, that is, there was no correlation between the period (range of 1.2–12.9 years) from iliac reconstruction to reharvest for the revision fusion and the percentage of filled lacunae (r² = 0.0083). RIBG specimens had an average marrow cellularity of 31%, which was less than the control cellularity of 45% (P = 0.052) and had more hypocellular cases (Table 2).
Histology findings by group.
Clinical and radiographic results of revision fusion with either RIBG or IBG were comparable. However, to encourage success of these salvage procedures, additional use of supplemental bone healing material/devices was common (Table 1). All RIBG patients in the pseudarthrosis repair group and 5/10 (all smokers) in the fusion extension group had supplemental BMP/BGS. Five patients, all in the fusion extension group, did not have any additional supplemental bone healing enhancement used; all went on to a solid posterior arthrodesis. Clinical outcomes found significant improvement in VAS back and leg pain, and ODI for both RIBG (and over the threshold for minimal clinically important differences) and control IBG groups at both follow-up periods relative to preoperative values (Table 3). There was no significant difference between RIBG and control IBG outcomes for back VAS (P > 0.07), leg VAS (P > 0.19), and ODI (P > 0.4). For the RIBG patients, analysis found no significant back pain improvement difference between extension and pseudarthrosis cases; however, the control IBG group had significantly greater VAS back pain improvement for the extension compared with the pseudarthrosis repair group (P = 0.01). There was greater leg pain improvement for extension compared with the pseudarthrosis repair RIBG patients (P ≤ 0.04 at 2 years postoperative). Control IBG subgroup analysis found no difference in leg VAS improvement for the extension vs pseudarthrosis repair groups (P ≥ 0.05). ODI analysis for RIBG and control IBG group found no significant differences in improvement at both follow-up periods (P > 0.15).
AClinical outcome measures.
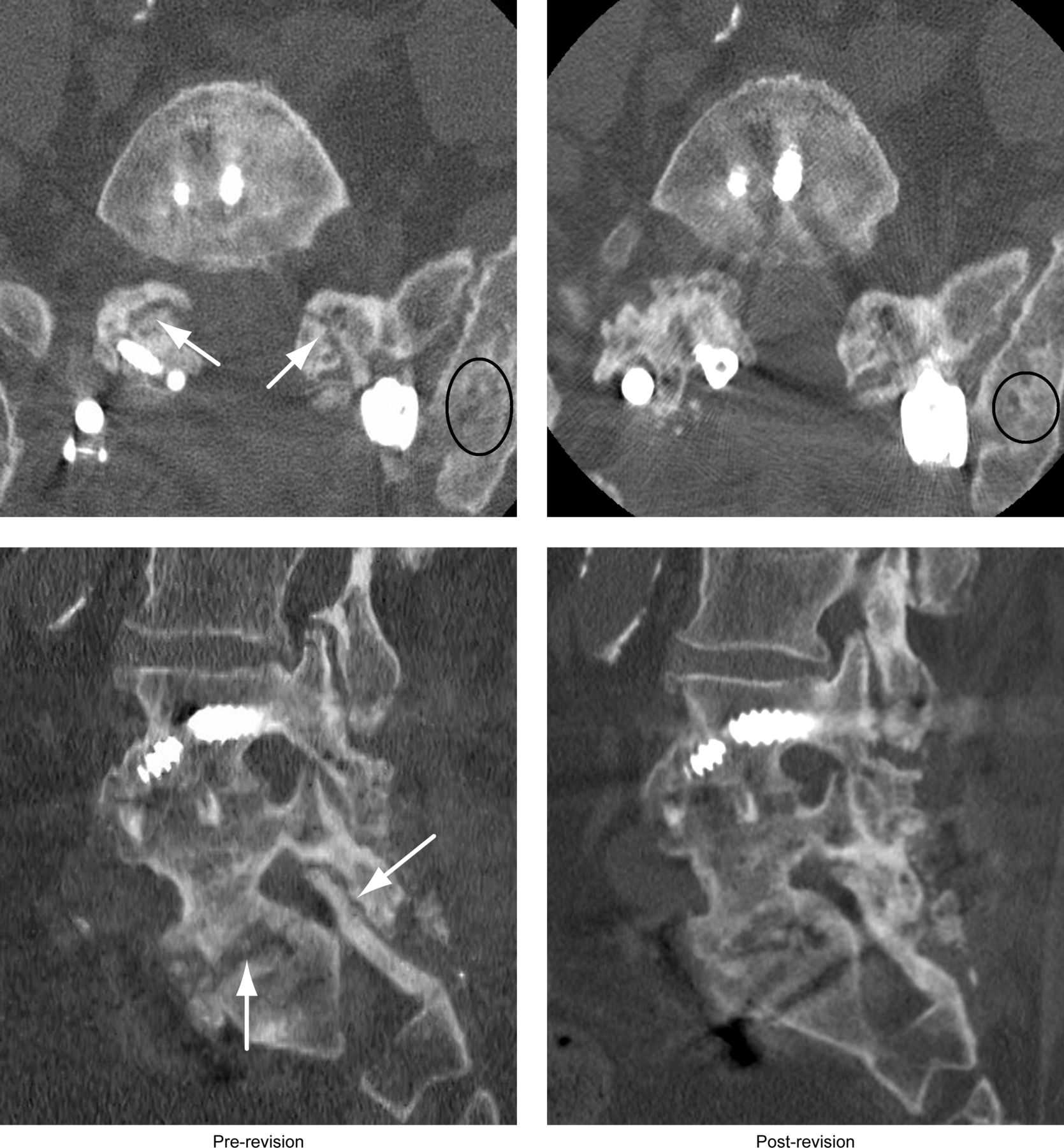
Postoperative (after the revision surgery) CT images found revision surgery with RIBG resulted in a solid posterior fusion (Figure 6), except for 1 patient who had fusion extension with BMP supplement, had hypocellular RIBG marrow, and was the only patient who had incomplete healing of the RIBG in CT prior to revision fusion. Controls who had revision fusion during the same period, using IBG/BMP had ~80% solid posterior fusion rate (not significantly different to RIBG fusion rate, P = 0.26, Table 1). The exception was a very small group of pseudarthrosis patients utilizing only local autograft resulting in a low fusion rate. It is also notable that many of these revision patients also had an interbody fusion performed at their secondary surgery, most of which healed despite posterior nonunion so that ultimately only 4 of 53 control pseudarthrosis repair patients and only 8 of 80 control fusion extension patients had continued nonunion of either anterior or posterior columns.
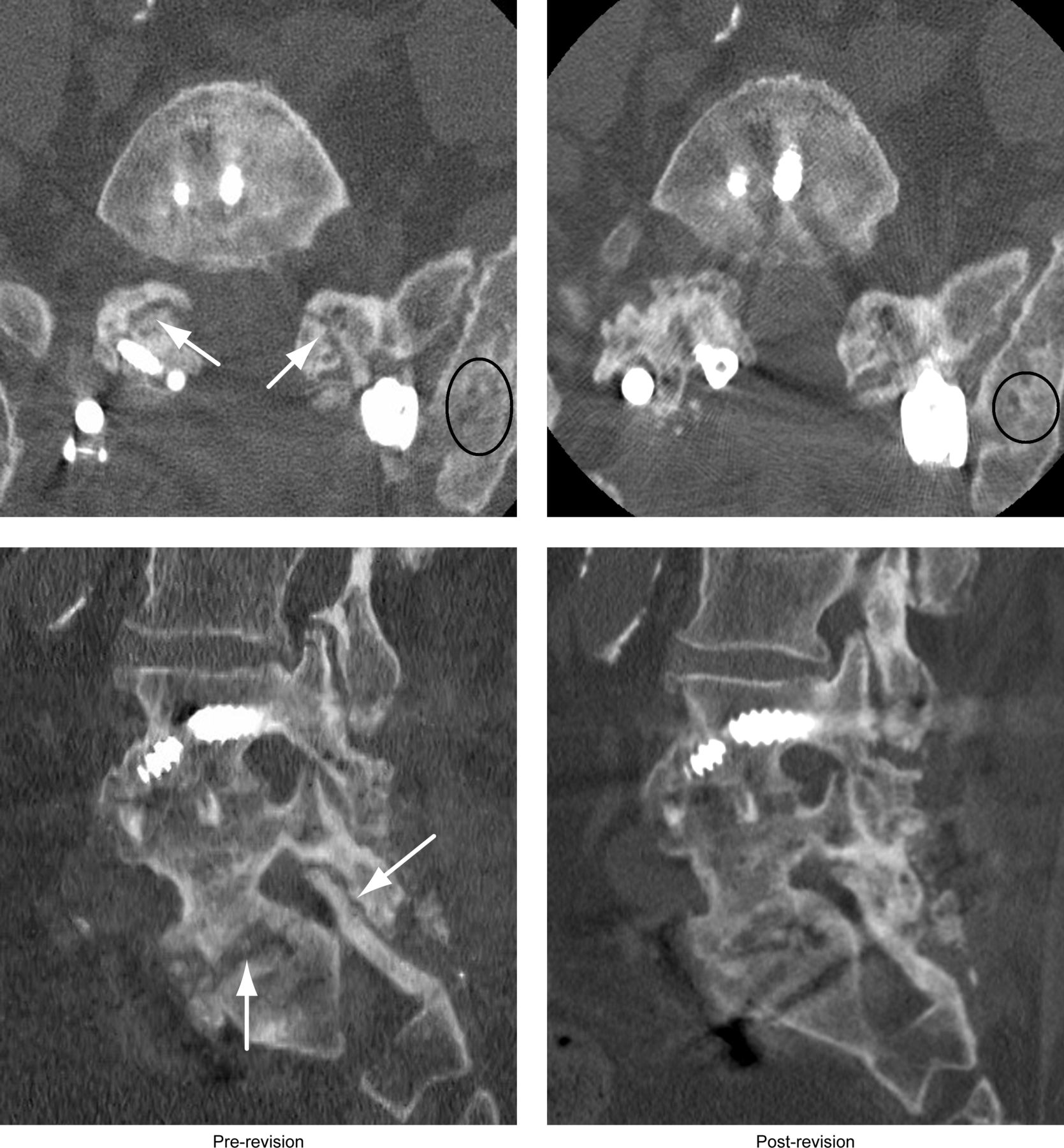
Example of a patient who underwent a second attempt at posterior pseudarthrosis repair of failed L4-S1 anterior-posterior fusion using posterior hybrid facet screws on right and pedicle screws on left. Computed tomography image axial and sagittal reconstruction prior to second revision of pseudarthrosis (left), arrows indicate bilateral facet joint and interbody nonunion. Axial and sagittal reconstruction (right) 1 year after successful pseudarthrosis repair using reconstructed iliac bone graft (RIBG) demonstrating solid arthrodesis of facet joint and interbody region. Ovals indicate revised RIBG.
Discussion
Bone graft options for revision spinal fusion are preferably osteogenic or osteoinductive in addition to osteoconductive.14 IBG and BMP are preferred bone graft materials for revision fusion in that they have these attributes.28 The present study demonstrated that reconstruction of the IBG graft donor site with cancellous allograft bone typically remodels into viable bone represented by normal osteocyte density but of lesser marrow cellularity compared with HC. RIBG histology was indicative of remodeling, and this appeared to occur primarily in the first year, after which the viability appeared stable for 1 to 13 years after reconstruction. Clinically, reharvest from the RIBG site is feasible with a low risk of complications or adverse outcomes. With BGS, RIBG may be an option in obtaining solid fusion for cases requiring secondary fusion.
Few studies have investigated IBG donor site reconstruction as a source of bone graft for revision fusion. One small prior study used hydroxyapatite for reconstruction of the donor site with subsequent CT and bone images.21 This study found integration and biological activity of the bone graft substitute. Additionally, 1 patient had a biopsy, and osseous ingrowth was identified. A larger study of hydroxyapatite RIBG demonstrated bony replacement of the bone substitute.22 These studies, however, did not report on the feasibility or effectiveness of hydroxyapatite RIBG for obtaining a subsequent fusion. In the present study, histology of the allograft bone RIBG demonstrated many features consistent with viable new bone. Overall, this included a mean of 83% filled lacunae indicative of viable osteocytes and cement lines between new and existing bone. Additionally, the concentric arrangement of the lamellae was consistent with remodeling of bone. Although there were regions of unfilled lacunae, nonviable bone, the overall percentage of filled lacunae was in the range of normal bone.29–31 Despite less cellular bone marrow findings for the RIBG, the overall viability of RIBG was not adversely affected and is supported by the high fusion rate as demonstrated on postoperative CT images.
Findings in the clinical arm of the study for control pseudarthrosis repair patients found BMP to have an similarly high fusion rate as IBG, which was greater than for local bone graft consistent with prior reports.32,33 Both RIBG and IBG groups found modest outcomes improvements and are consistent with prior reports of this type of revision surgery.14,34 The clinical outcomes of both types of revision fusion in the present study found using RIBG was feasible and did not have an adverse effect on outcomes in these revision surgeries.
Limitations include possible undercounting of the filled lacunae due to tissue shrinkage during formalin fixation. However, this applies similarly to HC that had identical sample preparation in the same pathology laboratory. The greatest limitation is that clinically it is underpowered, and the confounding factors of additional BMP/BGS are used for many patients who were smokers. Outcomes of revision fusion also reflect multiple patient factors beyond the scope of this study.
Conclusion
Reconstruction of the IBG donor site, which has historically been performed to decrease donor site pain, is a potential source of subsequent bone graft. In general, RIBG from allograft bone reliably remodels into viable cancellous bone with similar osteocyte density as normal iliac bone despite lower and variable marrow cellularity. The authors contend that the optimal bone graft options for revision fusion surgeries are products that are osteoinductive, osteoconductive, and osteogenic, which seem to be present in RIBG. This report is the first to investigate the clinical feasibility of RIBG for revision fusion. RIBG is not a substitute for IBG or BMP for revision fusion based on this case series. However, when used with adjunctive measures, RIBG may be an option when IBG or BMP is not readily available for revision fusion. We contend that reconstruction of the IBG site at the time of primary harvest has potential long-term benefit as fusion revisions, best treated with viable bone graft, is always possible in a small proportion of patients. Given this study’s findings, including the lack of adverse effect on clinical outcomes of the small clinical feasibility study arm, larger comparative investigations of RIBG vs bone substitutes independent of BMP/BGS supplements are warranted to determine efficacy. The clinical part of this feasibility study suggests the fusion extension group rather than pseudarthrosis repair group would be a better treatment group to determine efficacy because, from a practical aspect, a surgeon would more likely use combinations of BMP/IBG and/or BGS in a pseudarthrosis patient, which would make the results confounding.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Glenn R. Buttermann discloses a license agreement with Solco FG and consulting with Dio Medical. The remaining authors have nothing to disclose.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.