


Abstract
Background Recombinant human bone morphogenetic protein-2 (rhBMP-2) combined with an activated collagen scaffold (Infuse; Medtronic, MN) has been used to facilitate lumbar intervertebral fusion; however, data regarding its efficacy are inconsistent. We aimed to assess the efficacy of rhBMP-2 when used in posterior lumbar interbody fusion (PLIF) by analyzing the rate of reoperation for nonunion and patient-reported outcome measures in a large retrospective case series. We also aimed to assess the impact of patient and surgical factors on rates of reoperation and determine frequency of complications.
Methods Prospectively collected data from a single-surgeon database of consecutive PLIFs (minimum 18-month follow-up) were retrospectively analyzed. PLIF was performed with pedicle screw instrumentation, intervertebral spacers, and locally harvested bone graft to which rhBMP-2 and bone marrow aspirate (BMA) were added. Multivariate logistic regression was used to determine the influence of patient and surgical factors on the primary outcome: reoperation for confirmed nonunion.
Results A total of 1019 operations at 1485 levels across 908 patients were analyzed. Mean duration of follow-up was 51.7 ± 30.0 months (range 18–172). Twelve patients required reoperation for nonunion (1.2%). Increasing body mass index was found to be significant in predicting reoperation (OR 1.114, P = 0.046). Postoperative radiculitis was common (42%) but transient in most cases. There were significant and sustained improvements in patient-reported outcome measures postoperatively. Four cases of osteolysis and 5 of epidural cyst were recorded, and a reduction of rhBMP-2 dose seemed to ameliorate these sequelae.
Conclusion In this large retrospective observational study, PLIF performed with rhBMP-2 and BMA resulted in a low rate of clinically significant nonunion and significant improvement in patient-reported outcomes. Transient radiculitis was common. Osteolysis and epidural cyst formation were rare and possibly related to dosage.
Clinical Relevance rhBMP-2 is effective when used in PLIF, resulting in a high rate of fusion and improved patient outcomes, and it has an acceptable safety profile.
Level of Evidence 3.
Introduction
Spinal fusion is an important treatment option for chronic low back pain and sciatica. The volume of elective lumbar fusions performed continues to rise.1 To facilitate successful intervertebral fusion, autologous iliac crest bone graft (ICBG) has generally been considered the gold standard—its use, however, carries disadvantages such as potential donor site complications, a limit to the amount of donor graft material available, increased operating time, and the risk of developing nonunion or pseudarthrosis.2
Reported rates of pseudarthrosis vary greatly,3,4 with a higher incidence in fusions at multiple levels.5 Pseudarthrosis results in continued motion and, in combination with postoperative epidural fibrosis, may result in persistent low back pain and radicular symptoms. It is a common cause for revision surgery, carrying surgical risk and economic costs for modest gains in quality of life.6 There is a growing body of literature suggesting a positive correlation between the radiographic presence of fusion and improved clinical outcomes.7,8
Substitutes for ICBG or additives that may further enhance the rate of successful fusion have been investigated. Among the most extensively studied are the bone morphogenetic proteins (BMPs), which are the family of cytokines and growth factors of the TGF-β family, which have osteogenic capabilities.2 Recombinant human BMP-2 (rhBMP-2) appears to be the most promising of this family, and when combined with an activated collagen scaffold is known as Infuse (Medtronic, MN). Infuse initially gained approval in 2002 after being demonstrated as a superior alternative to ICBG for single-level anterior lumbar interbody fusion procedures.9 However, it is increasingly utilized for other types of fusion, and off-label use for cervical procedures and other lumbar interbody approaches is common.
Studies have varied in regard to the superiority of rhBMP-2 over autograft, but there are scant data regarding the effectiveness of rhBMP-2 when used in posterior lumbar interbody fusion (PLIF) procedures, with 3 studies reporting on a total of just 71 patients.10–12 The current study aimed to retrospectively assess rates of clinically significant nonunion in PLIFs performed with rhBMP-2 in a large cohort over a prolonged period. Additionally, it aimed to assess patient-reported clinical outcomes as well as the effect of patient and other surgical factors on rates of reoperation for nonunion and to determine the incidence of complications related to rhBMP-2 use.
Materials and Methods
Study Design
Nonrandomized, observational, and retrospective analysis of prospectively collected data of consecutive patients from a single surgeon.
Patient Sample
Inclusion Criteria
Patients who underwent a PLIF using rhBMP-2 for degenerative pathology or trauma between November 2005 and July 2019 performed by a single surgeon (W.R.S), who had a minimum of 18 months of follow-up data, and who gave consent preoperatively to being part of a prospective surgical outcomes registry were included in this study.
Exclusion Criteria
Patients with tumor involvement in their spine, patients with less than 18 months of follow-up, and patients undergoing fusion procedures other than PLIF were not included. Except for 1 patient early in the series (February 2008 with esophageal cancer), it was the senior author’s practice not to use rhBMP-2 in patients with a recent history of malignancy. Cases that were reoperations at the same level in the same patient were considered the endpoint for analysis and were therefore not reincluded in the analysis. Reoperations at disparate levels in the same patient, however, were included in the analysis.
Surgical Technique
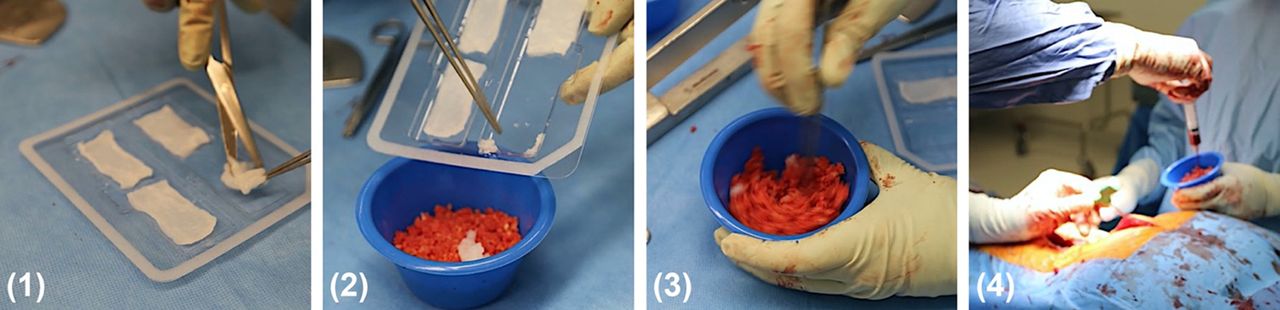
All patients underwent open instrumented PLIF. The surgical technique remained consistent for all patients and used the Steffee PLIF approach, employing bilateral facetectomy, with complete excision of the inferior facets and excision of the cranial half of the superior facets (the portion of the superior facets projecting into the foramen and overhanging the posterior disc annulus).13 The cranial halves of the spinous process and laminae were preserved, except in the case of lytic spondylolistheses, or in those revision cases, where complete laminectomy had been carried out at a previous surgery. Posterior graft was placed between the residual, partially decorticated laminae and the residual, partially decorticated inferior facets (after removing any residual cartilage). No posterolateral graft was used (i.e, no graft was placed between the transverse processes). In all cases, polyetheretherketone intervertebral spacers were used (R90; Medtronic, MN). rhBMP-2 was used in combination with morcellized bone from the laminectomy and 5 to 8 mL of bone marrow aspirate (BMA) from the iliac crest. Initially, the rhBMP-2 dose was 2.1 mg within each intervertebral space (added to 1 small [1″ × 2″] absorbable collagen sponge) and 2.1 mg with the posterior graft material. From August 2007, Spongostan (an absorbable, gelatin sponge used for hemostasis) was no longer left in the epidural space to possibly mitigate the formation of epidural cysts. From April 2008, the dose of rhBMP-2 used at each level was halved to attempt to reduce the occurrence of osteolysis: ~1 mg of rhBMP-2 (in half a small “diced” collagen sponge, mixed with the morcellized local bone and BMA [Figure 1]) in the intervertebral space and ~1 mg of rhBMP-2 over the posterior graft. Dicing was undertaken to provide a more even distribution of BMP-2 throughout the graft material and avoid focal areas of BMP-2 hyperconcentration that may predispose to osteolysis (in those areas).

The author’s current technique for preparing Infuse, per single level. (1) 2.1 mg of recombinant human bone morphogenetic protein-2 is added to a single absorbable collagen sponge, which is then diced. (2, 3) The diced “Infuse” is mixed in with morcellized local bone. (4) ~5 to 8 ccs of bone marrow aspirate from iliac crests is then added to form the final graft material.
Study Endpoints and Outcome Measures
The study’s primary endpoint was binary: reoperation or not for suspected nonunion (for any given level) and with nonunion confirmed at surgery. Suspected nonunion was defined on the basis of clinical symptoms (back pain and/or leg pain) in addition to radiologic features on computed tomography or x-ray imaging (absence of bridging trabecular bone between vertebral bodies and/or bridging bone between residual posterior elements). Assessment of fusion was performed by the senior author (W.R.S.) on the basis of these clinical and radiological features.
The clinical component of the study evaluated patient-reported outcome measures (PROMs), which included the visual analog scale (VAS) for back pain and leg pain, the 36-Item Short Form Health Survey (SF-36) physical component score (PCS) and mental component score, and the Oswestry Disability Index (ODI). PROMs were recorded preoperatively and then at 3, 6, 12, and 24 months postoperatively. Published minimum clinically important difference thresholds were used: 1.2 for VAS back pain, 1.6 for VAS leg pain, 4.9 for SF-36 PCS, and 12.8 for ODI.14
Complications related to use of rhBMP-2 were recorded, including osteolysis, epidural cyst formation, and ectopic bone formation. The complication of early postoperative radiculitis was not documented uniformly; however, treatment (if warranted) was generally with a course of oral dexamethasone. As such, radiculitis was defined as the presence of new leg pain that developed in the early postoperative period (days 2–10), for which oral dexamethasone was prescribed. All patients with pharmacy dispensary data available were analyzed for this purpose.
Data Collection
Demographic, operative, and follow-up information were sourced from a prospective clinical research registry.
Statistical Analysis
Statistical analysis was performed with the Statistical Package for the Social Sciences (IBM, Armonk, NY). Patients who underwent reoperation for nonunion were identified in the registry. Logistic regression analysis was used to determine factors influencing reoperation for nonunion, a binary outcome. Repeated measures analysis of variance was used to analyze PROMs. Statistical significance was nominally set at a P value of less than 0.05.
Ethical Approval
Ethical approval for this study was sought from and granted by the Adventist HealthCare Limited Human Research Ethics Committee (AHCL project ID 2020–020).
Results
Patient Population, Comorbidities, and Follow-Up
A total of 1262 consecutive cases over 14 years from the prospective registry were assessed. Of these, 199 cases (15.8%) were excluded for a lack of adequate (18 months) follow-up or missing follow-up data. Forty-two cases (3.3%) were excluded due to involvement of thoracic levels, and 2 cases were excluded due to tumor involvement, resulting in 1019 operations at 1485 levels across 908 patients being included for analysis (Table 1). There was a female predominance among cases studied (644 cases, or 63.2%). Mean age at surgery was 68.1 ± 12.2 years. Osteoporosis or osteopenia was present more commonly than rheumatoid arthritis, at 12.4% compared with 5.2%, respectively. Mean duration of follow-up was 51.7 ± 30 months (range 18–172 months). Of the patient population for whom smoking data were available, 5.4% were active smokers at the time of surgery (43 out of 789). Mean body mass index (BMI) at surgery was 27.5 ± 5.1.
Patient demographics.
Surgical Demographics
The surgical demographics are shown in Table 2. Foraminal stenosis and instability were the most common indications for fusion. Mean number of levels fused was 1.5 ± 0.8 (range 1–5). Single-level fusions were the most common, with 711 cases (69.8%) performed. L4-L5 was the most commonly fused level followed by L5-S1.
Surgical demographics.
Reoperation for Nonunion
There were 12 cases of reoperation for nonunion (12/1019, 1.2%). In the multivariate logistic regression analysis, surgical factors (number of levels fused, L5-S1 among levels fused) were not found to influence this outcome. However, increasing BMI was found to be significant, with an odds ratio of 1.114 (for every kg/m2 increment, P = 0.046). Other patient factors, including age, gender, previous lumbar surgery, and presence of rheumatoid arthritis or osteoporosis/osteopenia were not found to be significant contributors to the model. There was no statistically significant association between using a higher dose of rhBMP-2 with “undiced” collagen sponges (which was the surgical technique employed for the first ~200 cases in this series) and reoperation for nonunion (P = 0.062, Fisher’s exact test).
Patient-Reported Outcome Measures
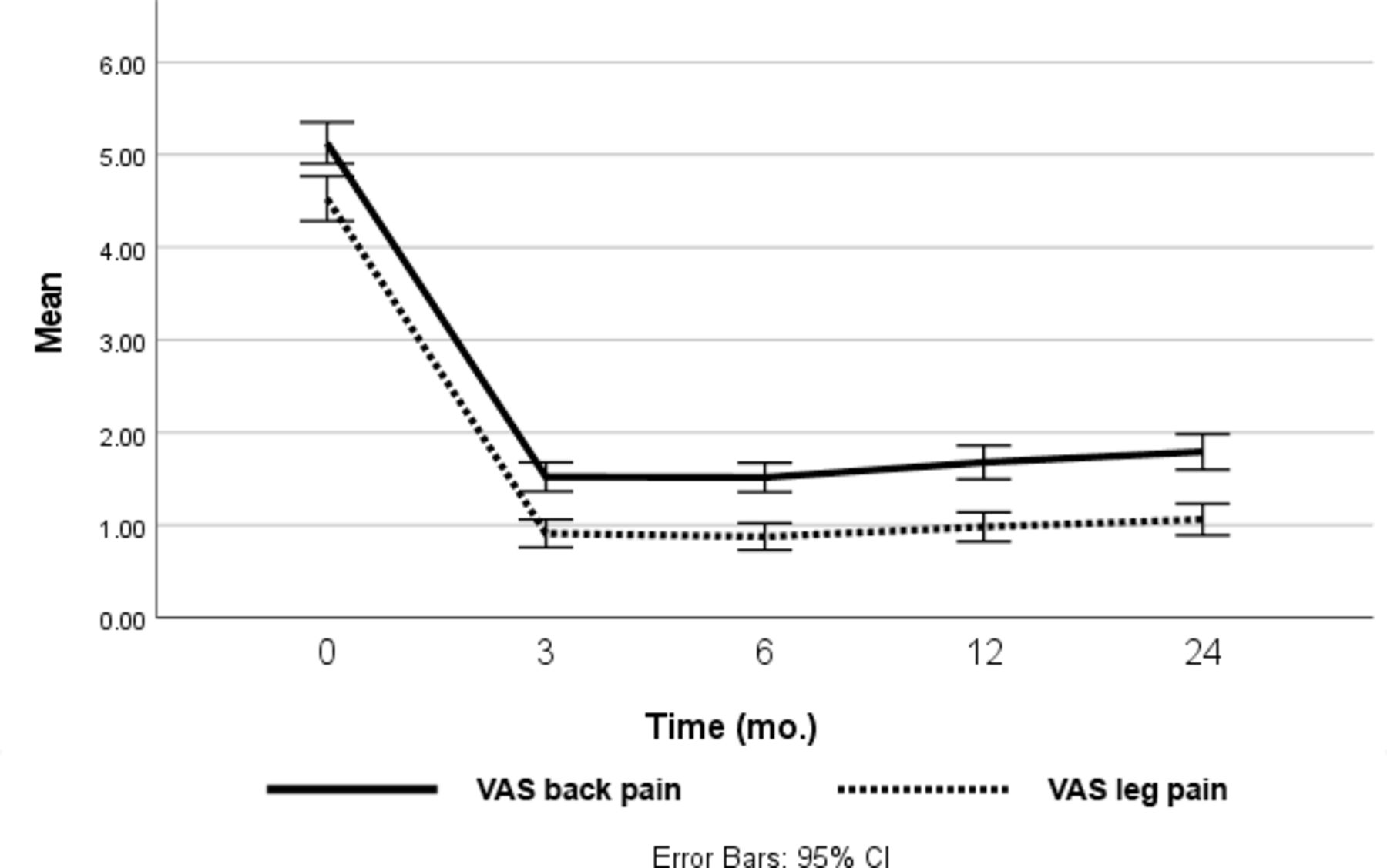
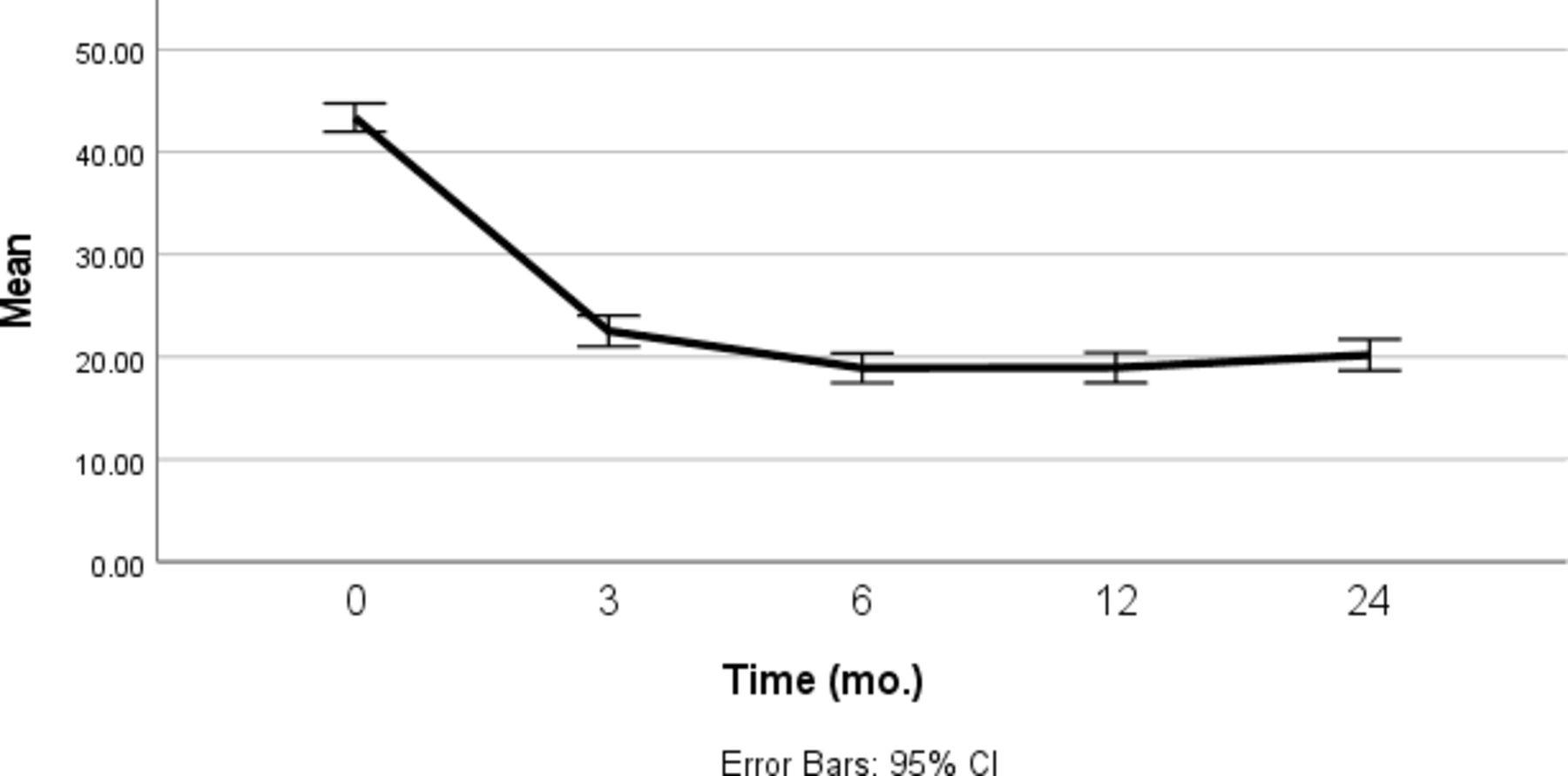
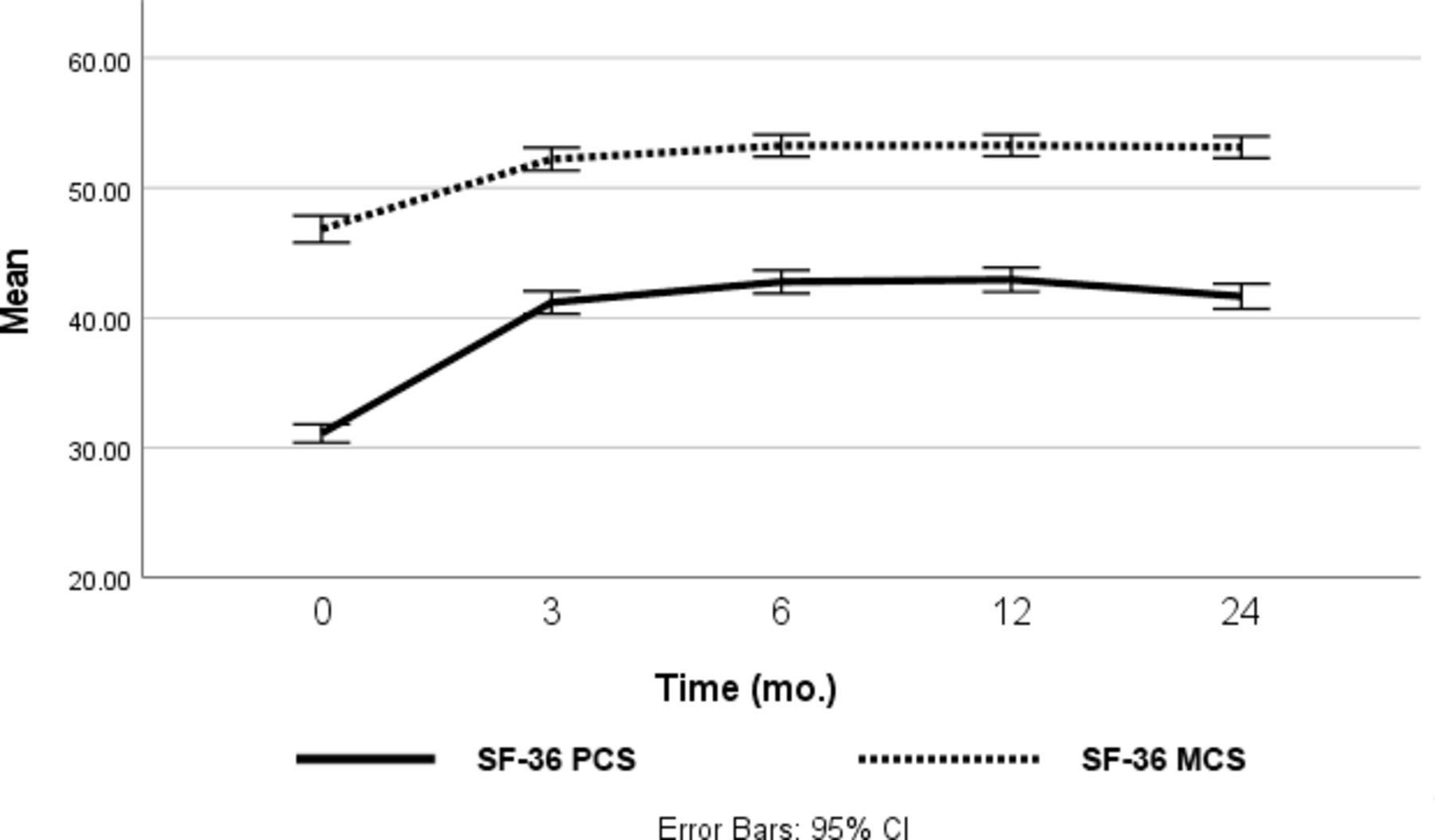
Pre- and postoperative patient-reported outcomes are shown in Table 3. PROM data were available for 931 of the 1019 patients. Mean VAS back and leg pain scores were significantly reduced at 3-month follow-up (P < 0.001). Improvements were maintained and statistically significant through 24-month follow-up (P < 0.001 for all timepoints, Figure 2). ODI and SF-36 PCS were significantly improved at 3-month follow-up, and post hoc tests demonstrated further improvement between 3 and 6 months in both measures (P < 0.001, Figures 3 and 4). Mean changes exceeded published minimum clinically important difference values for all measures.
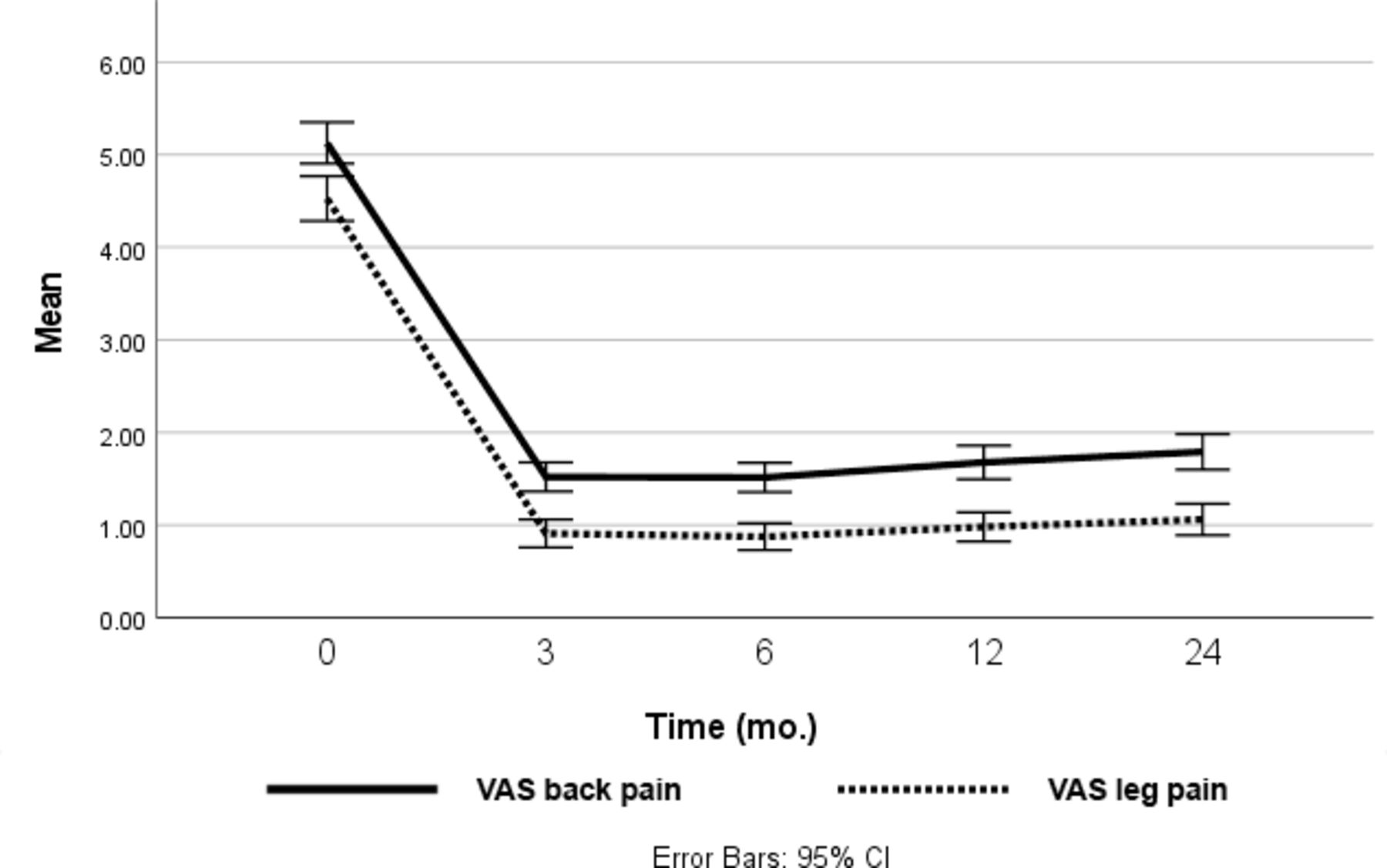
Visual analog scale (VAS) back and leg pain scores over time.
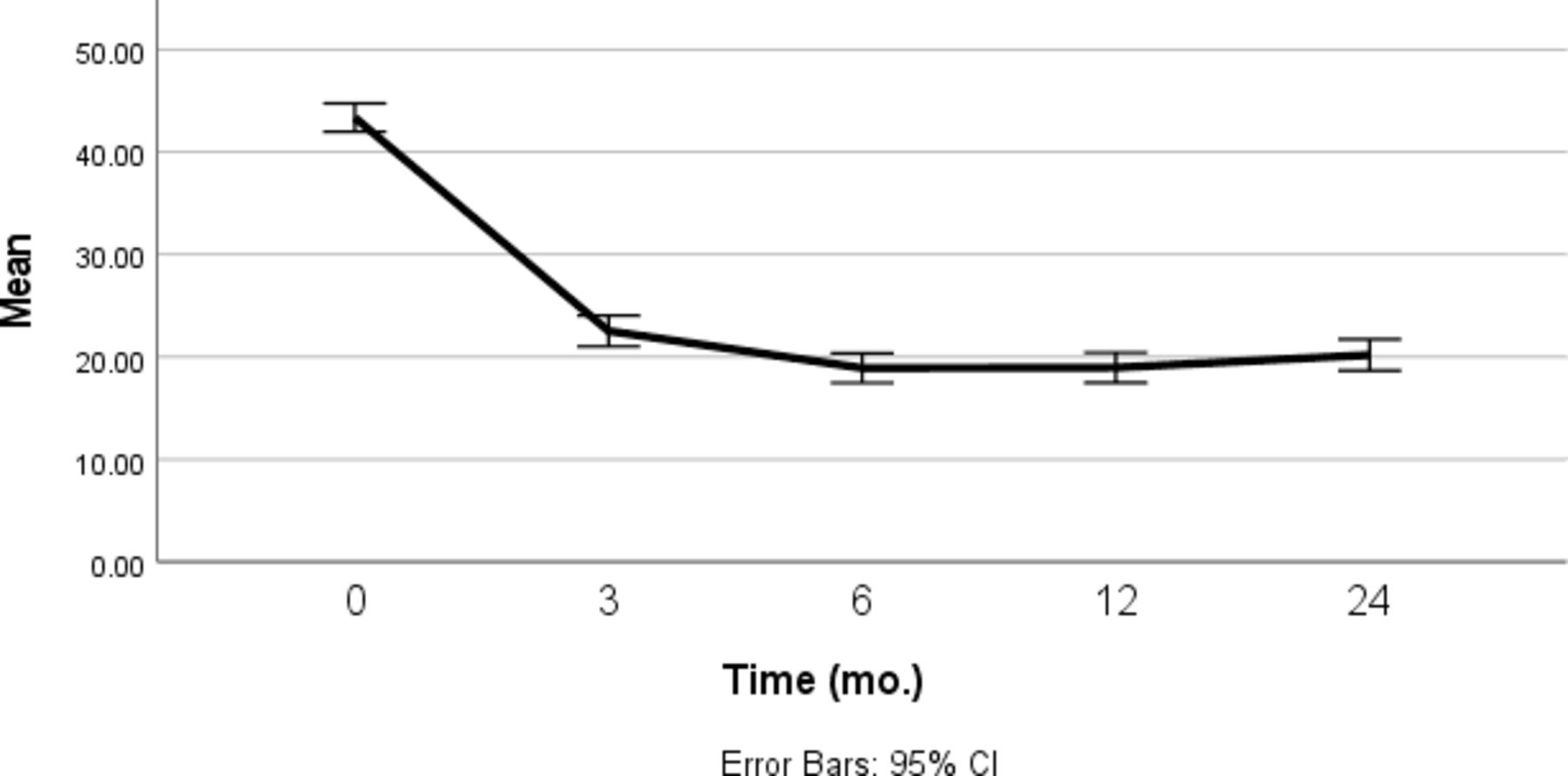
Oswestry Disability Index (ODI) scores over time.
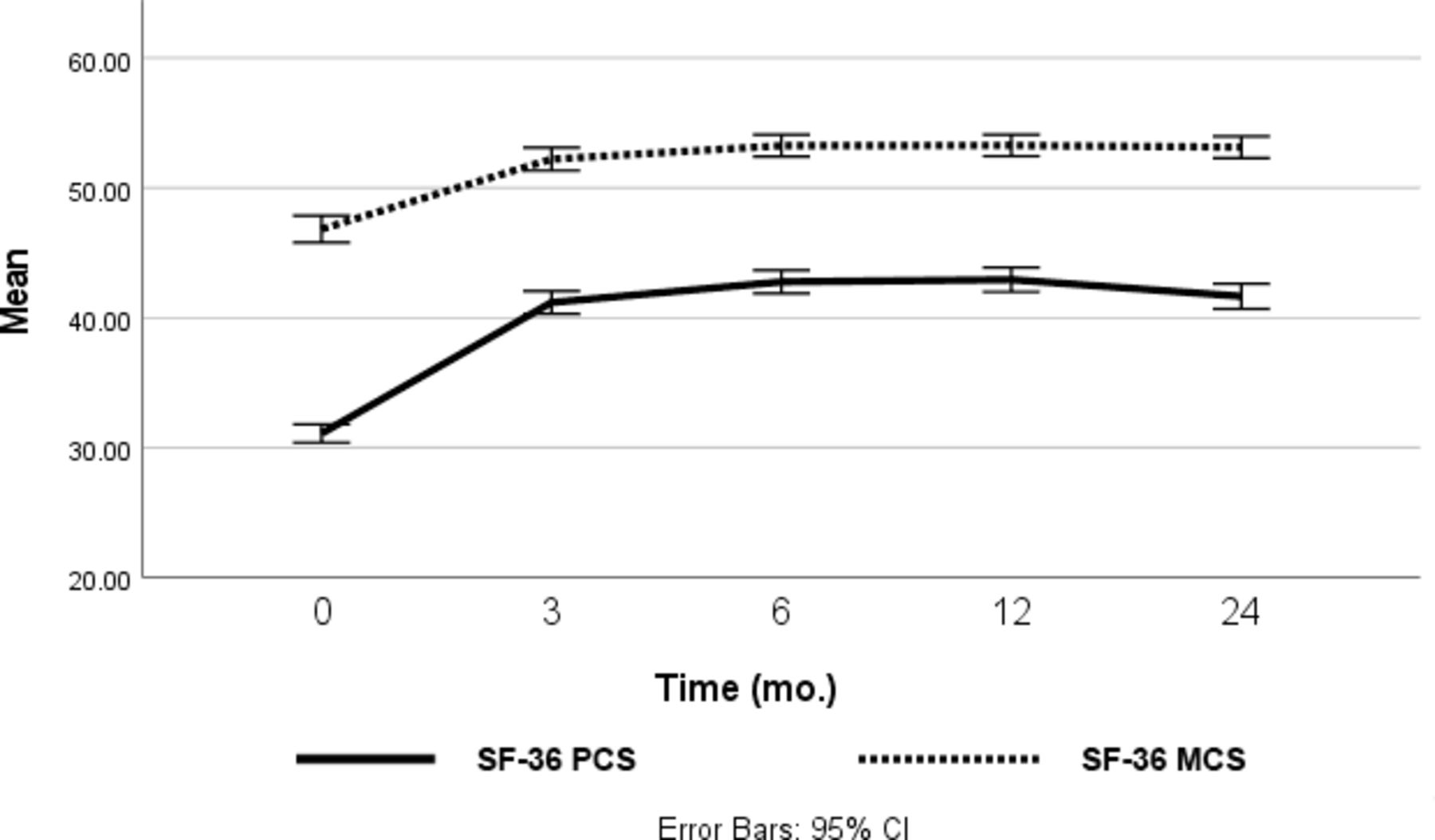
The 36-Item Short Form Health Survey (SF-36) physical component score (PCS) and SF-36 mental component score (MCS) over time.
Mean (SD) PROM scores.
Complications
Radiculitis
Pharmacy dispensary data were available for 221 patients. Dexamethasone was prescribed for radicular symptoms in 93 of these patients in the postoperative period (42.0%). Onset of symptoms (as determined by commencement of steroid treatment) occurred on average at 5.3 ± 1.8 days postoperatively (range 2–10 days). Of these 93 cases, early (3 or 6 months) follow-up VAS leg pain data were available for 78 patients, with 70/78 (89.7%) reporting little or no leg pain (VAS score ≤1/10). Six of 78 (7.7%) patients had persistent leg pain, but improved compared with preoperative levels. Two of the 93 patients (2.2%) given dexamethasone required revision surgery for subsequent nonunion, not significantly different compared with the cohort of patients who did not receive postoperative dexamethasone (P = 0.362, χ 2 test). None went on to develop deep wound or screw infection.
Deep Wound or Screw Infection
There was 1 case of confirmed deep wound or screw infection.
Osteolysis
There were 4 cases of early osteolysis in the cohort, each of whom developed back or leg pain between 1 and 3 months postoperatively with radiographically demonstrated bony resorption. Two of these 4 patients underwent reoperation for suspected nonunion. All 4 patients had gradual resolution of their symptoms and subsequent progress imaging, which demonstrated solid fusion. Figure 5 demonstrates the radiological presentation of 1 such patient.
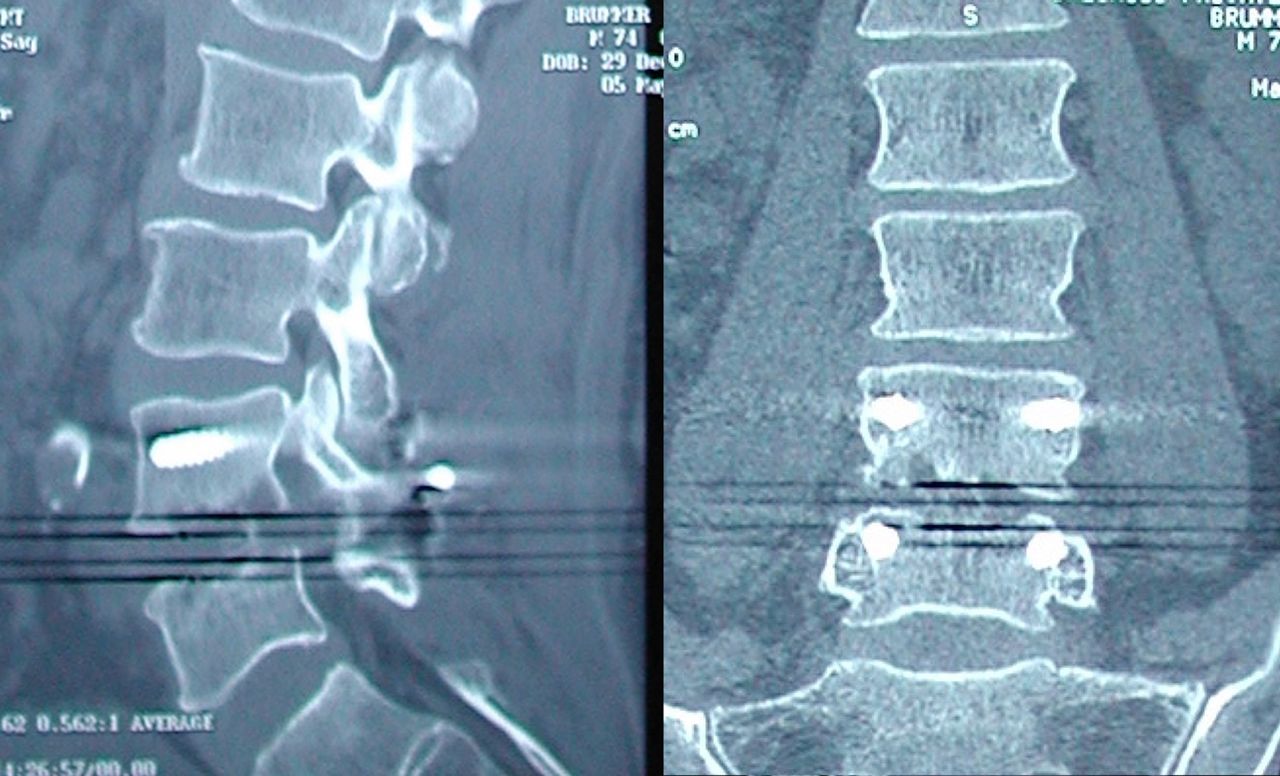
(A) Sagittal and coronal views of computed tomography images of a patient 3 months after an L4-L5 posterior lumbar interbody fusion showing satisfactory position of hardware but demonstrating osteolysis, particularly at the inferior L4 endplate.
Epidural Cysts and Ectopic Bone
There were 5 cases of postoperative epidural cysts in the cohort, each of whom presented with leg pain between 1 and 6 months postoperatively, with 1 requiring reoperation, whereupon only fibrinoid tissue was found lying adjacent to the thecal sac. Figure 6 demonstrates the magnetic resonance imaging findings of a typical case of epidural cyst formation. Oral steroids (dexamethasone) were found to be effective in relieving pain related to these epidural cysts, and subsequent magnetic resonance imaging demonstrated gradual resolution of these cysts in the majority of cases. All 5 patients had subsequent progress imaging, which demonstrated solid fusion. There were no recorded cases of ectopic bone formation.

T2-weighted magnetic resonance imaging, axial views, demonstrating the formation of bilateral epidural cysts 2.5 mo after an L4-S1 posterior lumbar interbody fusion.
Discussion
The senior author’s early experience with PLIF procedures involved high reoperation rates for pseudarthrosis of up to 16.3% for fusions using morcellized, locally harvested bone graft and no anterior interbody implant and no addition of any other graft material, improving to 8.3% when an intervertebral spacer was introduced.15 The current retrospective, observational study examined rates of reoperation for nonunion using a similar PLIF technique but with the addition of rhBMP-2 and BMA to the morcellized, locally sourced autograft and intervertebral spacers. In this large consecutive series, this combination with rhBMP-2 and BMA resulted in low rates of clinically significant nonunion and an acceptable safety profile.
Data in the published literature regarding lumbar fusion rates with rhBMP-2 have been inconsistent.10,11,16,17 This may be due to varying doses being used, different BMP carriers being used, differences in surgical technique, and inconsistencies in the assessment of fusion. Liu et al conducted a meta-analysis of 20 randomized controlled trials comparing rhBMP (both rhBMP-2 and rhBMP-7) with ICBG in lumbar fusion and found a significantly higher fusion rate and significantly lower reoperation rate for rhBMP compared with ICBG.18 The use of rhBMP-2 resulted in a pooled incidence of fusion success of 96.4%, comparable with the 98.8% observed in our cohort.
It should be noted that many surgeons now use transforaminal lumbar interbody fusion (TLIF), lateral lumbar interbody fusion (LLIF), or anterior lumbar interbody fusion (ALIF) rather than PLIF to approach the interbody space, and that the surgical approach may also affect fusion success rates.19 Our finding that increasing BMI predicts reoperation for nonunion concurs with previously published data associating BMI with complications after spinal surgery.20,21
The primary endpoint used in this study was reoperation for symptomatic pseudarthrosis, which was confirmed at surgery rather than at a radiographic endpoint. While other studies have used various radiographic scoring systems for the assessment of fusion, interobserver agreement has been found to be limited.22 Fine-cut computed tomography has been shown to have fair to poor reliability and low specificity in the assessment of lumbar interbody fusion.23 Open surgical reoperation is considered the benchmark for assessing nonunion, being the only method that allows direct visual inspection of fusion integrity, and it has been used in several large studies to compare fusion techniques.24,25 It is acknowledged that this endpoint may be influenced by patient preference or comorbidities and is likely to underestimate the frequency of radiological nonunion, especially in asymptomatic or elderly patients. Nevertheless, it provides a practical, binary endpoint by which to assess clinically significant nonunion. While the decision to reoperate may be subjective, the same surgical decision-making process was applied to all patients in the study cohort and may improve the accuracy of the analysis of the (examined) potential risk factors for nonunion.
Since Carragee et al published a review of reported adverse effects of rhBMP-2, the use of Infuse has been linked to myriad complications, including radiculitis, ectopic bone formation, osteolysis, and development of new malignancy.26 Osteolysis refers to the early resorptive phenomenon that has been well documented and is thought to be due to the aggressive resorptive phase of allograft incorporation during the first few weeks, which is then followed by an osteoinduction phase.27 Epidural cyst formation is thought to result from a proinflammatory process.28 In our series, all 5 cases of epidural cyst formation occurred early in the series and prior to a modification in operative technique, wherein Spongostan was no longer placed in the epidural space. This suggests Spongostan may absorb rhBMP-2 and lead to cyst formation around it when left in the epidural space. Three of the 4 recorded cases of osteolysis occurred within the first 200 cases of rhBMP-2, where high doses were used (2.1 mg in the intervertebral space). Subsequent cases utilized lower dosages (~1 mg) and a modified technique wherein rhBMP-2 sponges were “diced” prior to incorporation with morcellized bone, resulting in only 1 further case of resorption in the subsequent cases in the series. This might suggest a dose-related effect, as has been demonstrated in the literature.29
The incidence of postoperative radiculitis in our series is high, at 42%. The majority of data in the literature regarding postoperative radiculitis in lumbar fusion with rhBMP-2 relate to transforaminal (TLIF) procedures, with limited data pertaining to PLIF procedures. In a recent systematic review by Lytle et al, postoperative radiculitis occurred in between 3% and 57% of patients undergoing PLIF or TLIF procedures.30 The inconsistency in reported incidence of radiculitis may arise from a lack of an accepted definition of postoperative radiculitis or variations in surgical technique predisposing to radiculopathy regardless of BMP use (eg, nerve root retraction or injury during cage insertion). In the current series, the use of bilateral complete rather than partial facetectomy minimized the need for dural sac and nerve root retraction. While the procedure, as first described by Steffee, is referred to as PLIF, it may be more accurately described as a bilateral TLIF.13
Our use of the prescription of dexamethasone as a surrogate indicator for postoperative radiculitis may underestimate the true incidence. Use of dexamethasone in the early postoperative period of spinal fusion is controversial, with some evidence from animal models suggesting that it may inhibit fusion.31 Our prescription of dexamethasone in the early postoperative period did not appear to significantly increase the risk of clinically significant nonunion, with only 2 of 93 patients prescribed dexamethasone going on to require reoperation. However, the small sample size (and lack of control) does not allow us to draw a more robust conclusion. The phenomenon appeared to be transient in the majority of cases, with 97.4% of patients with postoperative radiculitis reporting improved, minimal, or no leg pain at early follow-up.
There are limitations to the current study. It is retrospective and observational in nature. However, the sample size is large (1019 procedures in 908 patients), and there was extensive follow-up (mean of 51.7 months, range 18–172 months). While logistic regression was used to account for previous surgeries, gender, age, and comorbidities, other confounding factors may still exist. Improving surgical “carpentry” and subtle changes in operative technique over this time frame are possible confounding factors that are unable to be quantified or accounted for. However, the single-surgeon nature of the study may reduce the occurrence of unrecognized confounding factors related to different surgical techniques and improve its internal validity but likely reduces aspects of external validity—such as fusion rates.
Future studies may focus on determining the optimal dosage of rhBMP-2 to be used to reduce the risk of transient radiculitis and osteolysis while maintaining a high rate of arthrodesis. The authors are also currently observing fusion outcomes using locally harvested and morcellized autograft mixed with 5 to 8 mL of BMA from the iliac crest, without additional rhBMP-2. The authors will report their observations on the outcomes with this technique in due course.
Conclusion
This large retrospective observational study found that PLIF performed with rhBMP-2 and BMA resulted in a very low rate of clinically significant nonunion. Increasing BMI was found to be a significant risk factor for reoperation. Transient radiculitis was common. Osteolysis and epidural cyst formation were rare following a reduction of rhBMP-2. Long-term patient-reported outcomes were favorable.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests William R. Sears is a consultant to Paradigm Spine (Wurmlingen, Germany) and receives royalties for lumbar spinal fusion implants from Medtronic (MN, USA), makers of Infuse. The remaining authors have nothing to disclose.
Human Ethics Approval Ethical approval for this study was sought from and granted by the Adventist HealthCare Limited Human Research Ethics Committee (AHCL project ID 2020-020).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.