


Abstract
Background A challenge of C2 pedicle screw placement is to avoid penetration into the C1-C2 facet joint, as this may alter normal biomechanics and accelerate joint degeneration. Our objective was to clarify how local anatomy and surgical technique may relate to C2 pedicle screw penetration into the C1-C2 facet joint.
Methods C2 pedicle screws were inserted using a fluoroscopically assisted freehand technique. Independent fellowship-trained spine surgeons blindly reviewed intraoperative fluoroscopic and postoperative computed tomography (CT) images for evidence of facet joint penetration (FJP). C2 pedicle morphometry, the sagittal angle of the facet joint, axial and sagittal pedicle screw angles, and screw length were measured on the relevant CT images.
Results A total of 34 patients fulfilled the study criteria, and a total of 68 C2 pedicle screws were placed. Eight screws (16%) penetrated the C1-C2 facet joint. The mean sagittal angle of the C1-C2 facet joint was significantly lower in the FJP group compared with the non-FJP group. The mean sagittal angle of the screws was significantly higher in the FJP group compared with the non-FJP group. The mean screw length was significantly greater for screws causing FJP compared with the non-FJP group. The mean axial screw angle was significantly lower in the FJP group compared with the non-FJP group. Pedicle width, length, height, and transverse angle were not significantly associated with FJP. Independent reviewers were able to identify FJP on intraoperative fluoroscopic imaging in 2 out of 8 cases.
Conclusion Lower sagittal angle of the facet joint, higher sagittal angle of the pedicle screw, and screw length >24 mm are associated with higher risk of C1-C2 FJP. When placing C2 pedicle screws under these conditions, caution should be taken to avoid FJP.
Clinical Relevance Several anatomical and technical factors may increase the risk of C1-C2 FJP during placement of C2 pedicle screws using a fluoroscopically assisted freehand technique, underscoring the importance of preoperative planning and limiting screw length.
Level of Evidence 3.
Introduction
The need to obtain fixation at the C2 vertebral level can result from traumatic, inflammatory, neoplastic, congenital, iatrogenic, or degenerative disorders. Options for C2 fixation include pedicle, pars, transarticular (Magerl), and translaminar screws as well as spinous process wiring. While the precise indications for each type of fixation are complex and dependent on a given patient’s vascular and osseous anatomy, length of construct, amount of correction, and surgeon’s experience, pedicle screws are often preferred and may provide a superior biomechanical fixation.1 C2 transarticular screw placement is not anatomically feasible in up to 10% to 23% of patients due to variations in vertebral artery anatomy or a large vertebral artery groove (high-riding or aberrant vertebral artery). Translaminar screws require intact posterior elements, adequate laminar thickness, and a stable anterior spinal column.2–4 Furthermore, clinical studies have reported lower rates of pseudarthrosis and hardware failure in patients treated with C1 lateral mass and C2 pedicle screws (Harms technique) compared with those treated with pars and translaminar screw constructs.5–8
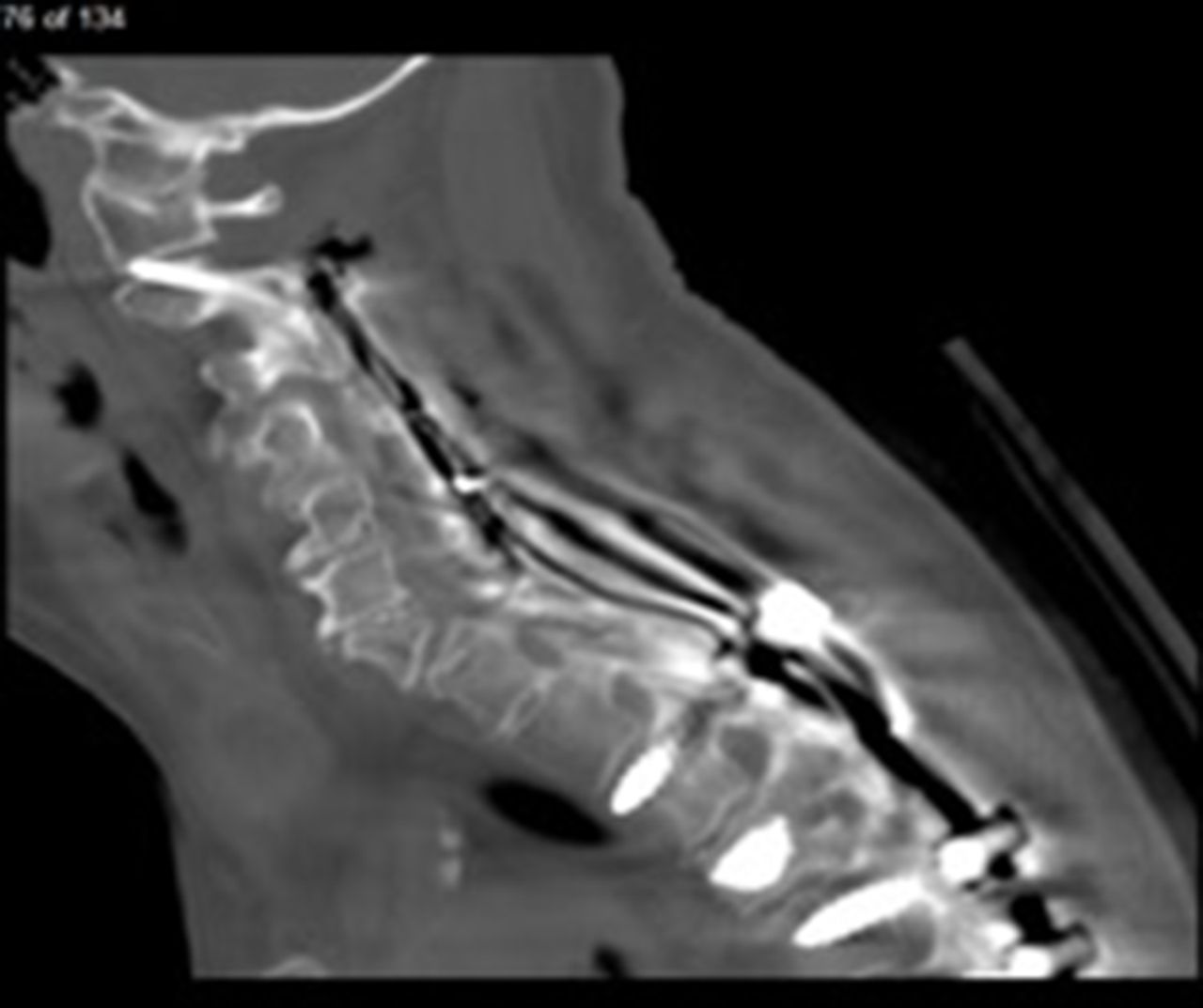
The instrumentation of the C2 pedicle is particularly challenging due to the vascular, neurological, and osseous anatomy of the segment. The vertebral artery typically lies immediately lateral and inferior to the pedicle as it makes a right angle turn within the lateral mass of C2.5 The anatomical variants of the vertebral artery are relatively common, especially in patients with congenital skeletal anomalies such as os odontoideum.9,10 Narrow pedicle width and a high-riding vertebral artery may complicate screw placement in up to 23% and 31% of patients, respectively.11–14 Another challenge of C2 pedicle screw placement is to avoid penetration into the C1-C2 facet joint, unless C1-2 fusion is desired, as this may alter normal biomechanics and accelerate joint degeneration at the C1-C2 motion segment (Figure 1).15–17 Direct facet joint violation, instability, and C1-C2 kyphosis may also result in painful motion postoperatively.18–20 For example, facet joint penetration (FJP) of lateral mass screws during cervical laminoplasty, a motion preserving technique of cervical decompression, has been associated with significantly increased rates of axial neck pain and stiffness.17,21,22 The reported incidence of C1-C2 FJP during freehand placement of C2 pedicle screws ranges from 4% to 20%.23–25 To the authors’ knowledge, however, no previous study has investigated the anatomical and technical risk factors associated with C2 pedicle screw FJP.

Sagittal computed tomography image of C1-C2 facet joint penetration.
The purpose of the present study was to clarify how penetration of C2 pedicle screw into the C1-C2 facet joint is related to the C2 pedicle morphometry, the sagittal angle of the C1-C2 facet joint, sagittal and axial pedicle screw insertion angles, bone mineral density of C2, and screw length. We postulated that more vertically oriented C1-C2 facet joints, softer bone, and longer pedicle screws may predispose to inadvertent C1-C2 FJP. In addition, we report on the incidence of FJP undetected on intraoperative fluoroscopic imaging and subsequently confirmed on postoperative computed tomography (CT).
Methods
An institutional review board approval was obtained prior to the initiation of the study. The institutional review board had granted a waiver of informed consent for this study. A retrospective radiographic review was conducted on all patients who underwent a posterior cervical fixation with C2 pedicle screws at a single tertiary care urban teaching hospital from 1 January 2010 to 1 April 2022 and had intraoperative fluoroscopy and postoperative CT imaging available for evaluation. Exclusion criteria included a lack of postoperative CT images of the cervical spine. Pediatric patients were not included in the study.
Surgical Technique
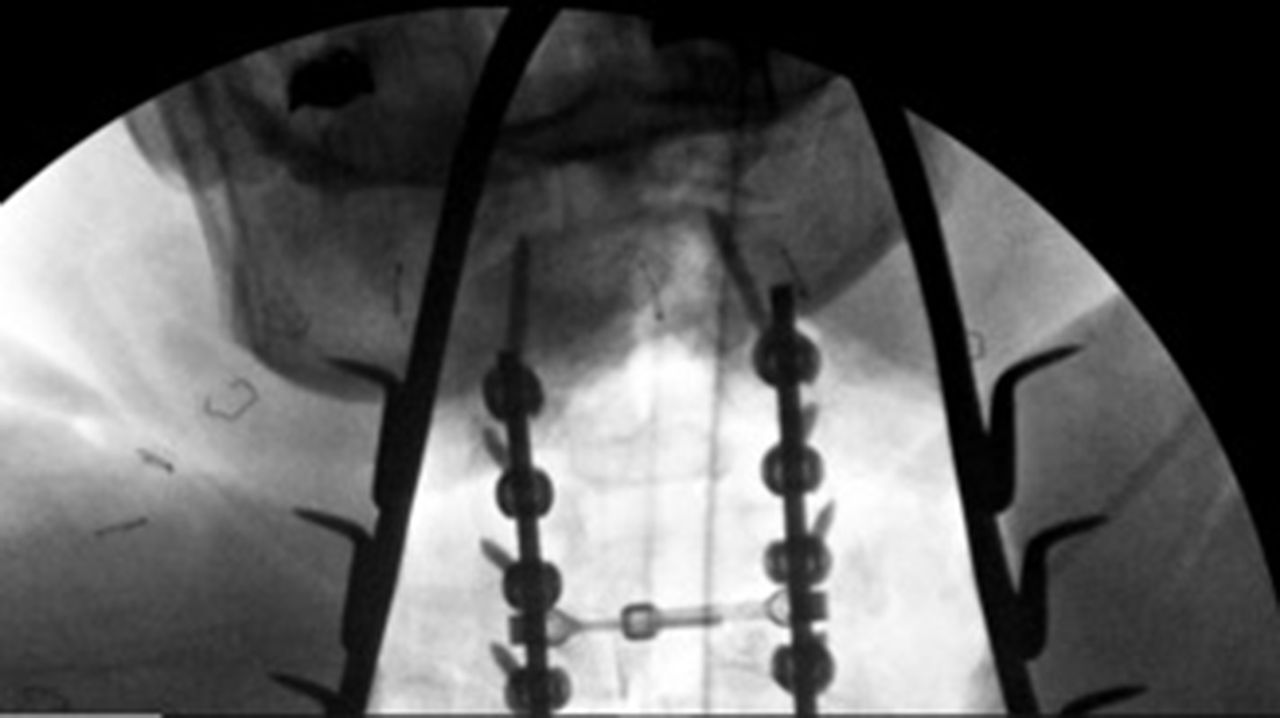
C2 pedicle screws were inserted using the freehand technique with fluoroscopic confirmation. First, general endotracheal anesthesia was achieved, and intraoperative somatosensory–evoked potential monitoring was initiated to detect any changes during the procedure. A wine cork or radiolucent bite block was placed to help visualize the C2 pedicles on the intraoperative fluoroscopic open mouth view (Figure 2). A Mayfield head clamp was applied with 60 lbs/inch of torque. The patient was placed in reverse Trendelenburg position on a Jackson or ProAxis table with the patient’s arms at their sides. A posterior midline approach to the cervical spine was then performed. The C1-C2 interlaminar window was exposed and the vascular plexus of epidural sinusoids packed with Floseal hemostatic matrix (Baxter) and Cottonoid patties. A straight freer or Penfield 2 elevator was used to palpate the cephalad and medial aspect of the C2 pedicle and guide the placement of the starting hole. A small burr (typically 1.7 mm) was then used to make a unicortical pilot hole. A cervical pedicle awl was used to cannulate the C2 pedicle to a depth of approximately 10 mm. The tip was angled facing medially away from the vertebral artery. At the same time, an assistant held a freer or Penfield 2 elevator against the medial aspect of the C2 pedicle to help guide the angulation of the awl in the axial and sagittal planes. At this point, a lateral view and an open mouth fluoroscopic views were obtained. On the open mouth view, we ensured that the tip of the awl started to enter the outline of the C2 pedicle. The lateral view was used to check the cephalad angulation of the awl within the pedicle. The awl was advanced to approximately 20 to 24 mm in depth. If unable to advance, the trajectory was changed, and the awl was rotated outside of the pedicle tract 180°. If the awl continued to be unable to advance, but on lateral view the trajectory appeared correct, a shorter screw was used. The open mouth view was then rechecked to ensure that there was no violation of the C1-C2 facet, and the lateral view was rechecked to ensure that the awl was parallel to the axis of the pedicle. The inside of the pedicle was then palpated with a balltip probe to ensure no breaches in the pedicle wall and a solid bottom. The pedicle was undertapped in softer bone or tapped line to line in stronger bone. The balltip probe was again used to feel the inside of the pedicle. The pedicle screw was then advanced. If unable to advance past 14 to 16 mm despite adjustments in trajectory, a shorter pedicle or a pars screw was placed. If possible, bilateral instrumentation was performed simultaneously to save time on the above steps.

A wine cork placed in the mouth to help visualize the C2 pedicles on the intraoperative open mouth view.
Independent reviewers blindly reviewed the intraoperative fluoroscopic images for evidence of FJP. Presence or absence of FJP on CT imaging was evaluated according to a modified classification described by Gertzbein and Robbins. Grade 0 screws are positioned entirely within bone. Grade 1 screws had a breach of the pedicle with less than 50% of the diameter of the screw entering the cortex. Grade 2 screws had greater than 50% of the screw diameter entering the cortex.26,27 The Gertzbein and Robbins grades were independently reviewed by a fellowship-trained spine surgeon as well as senior residents to determine inter- and intrarater reliability.
Morphometric Measurements
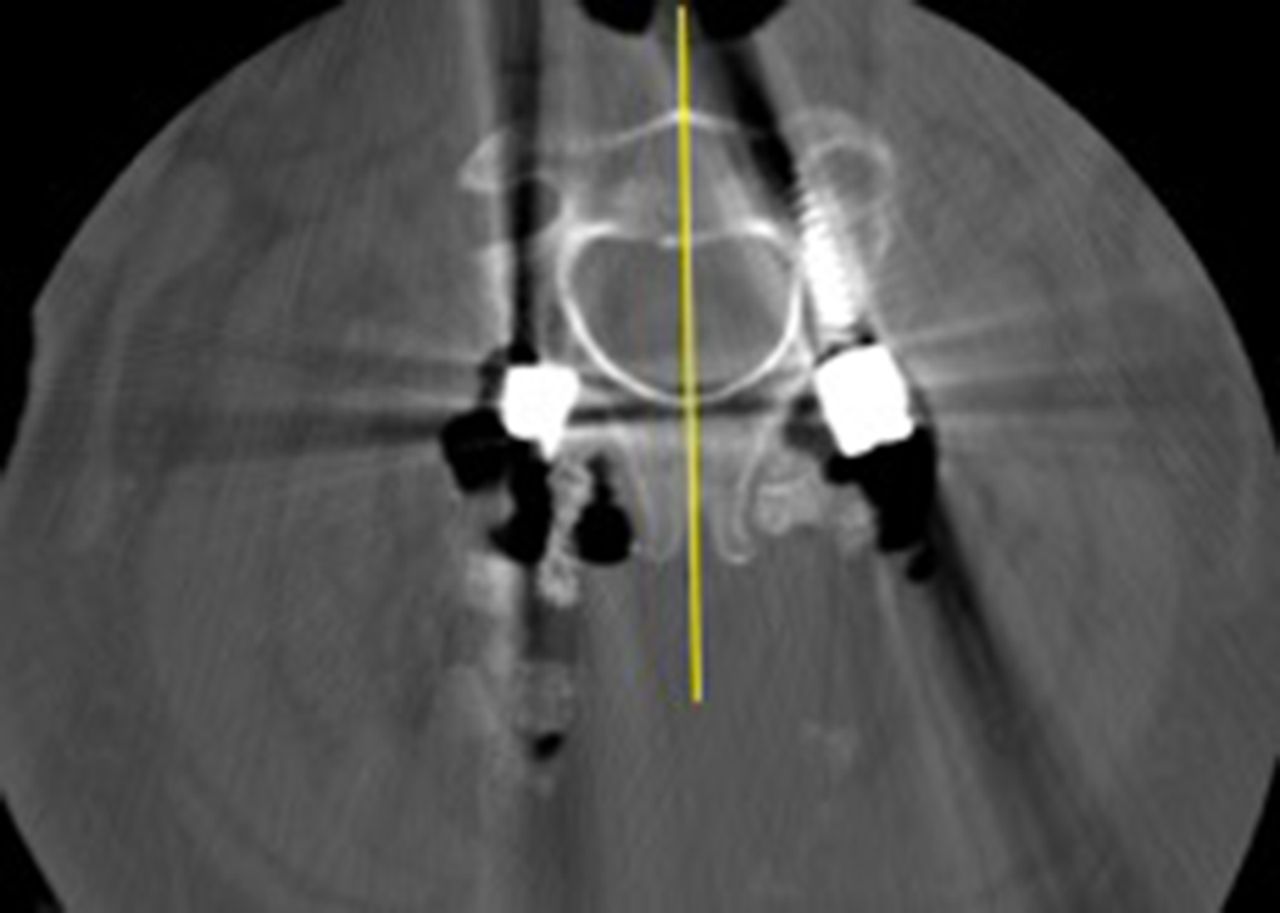
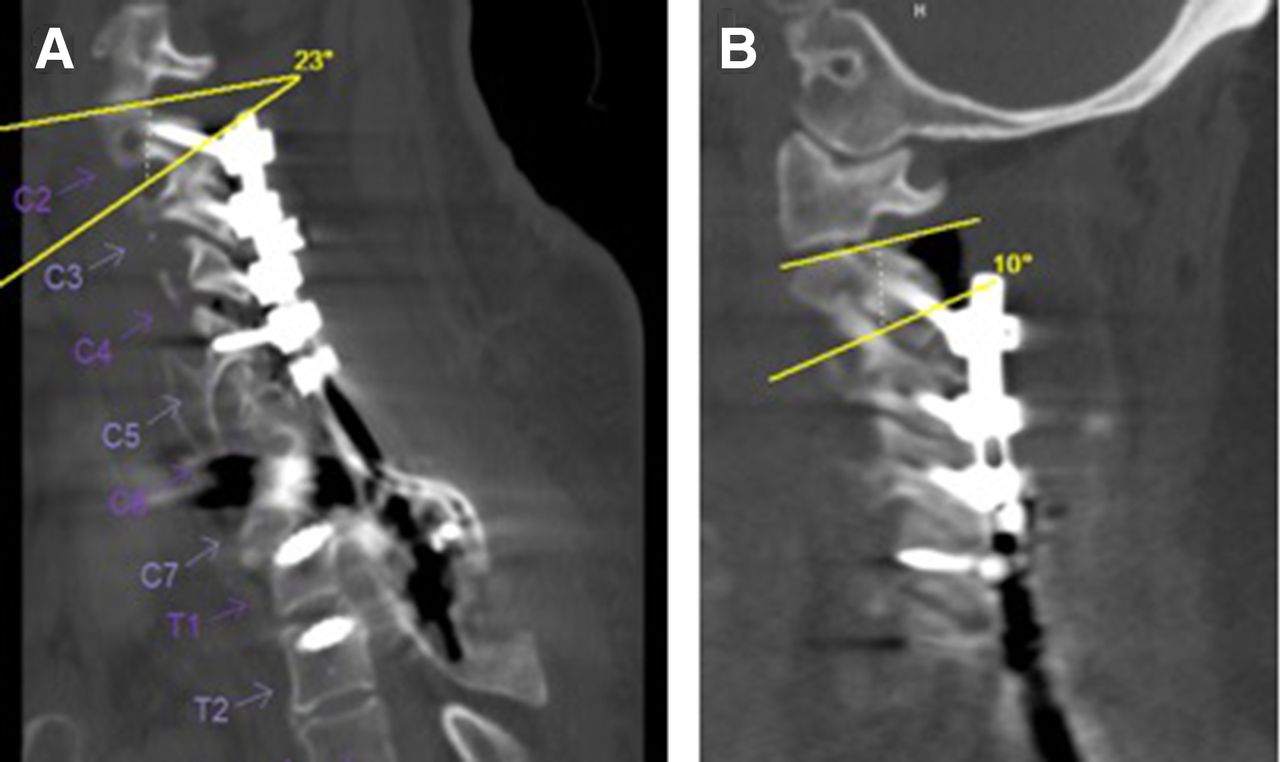
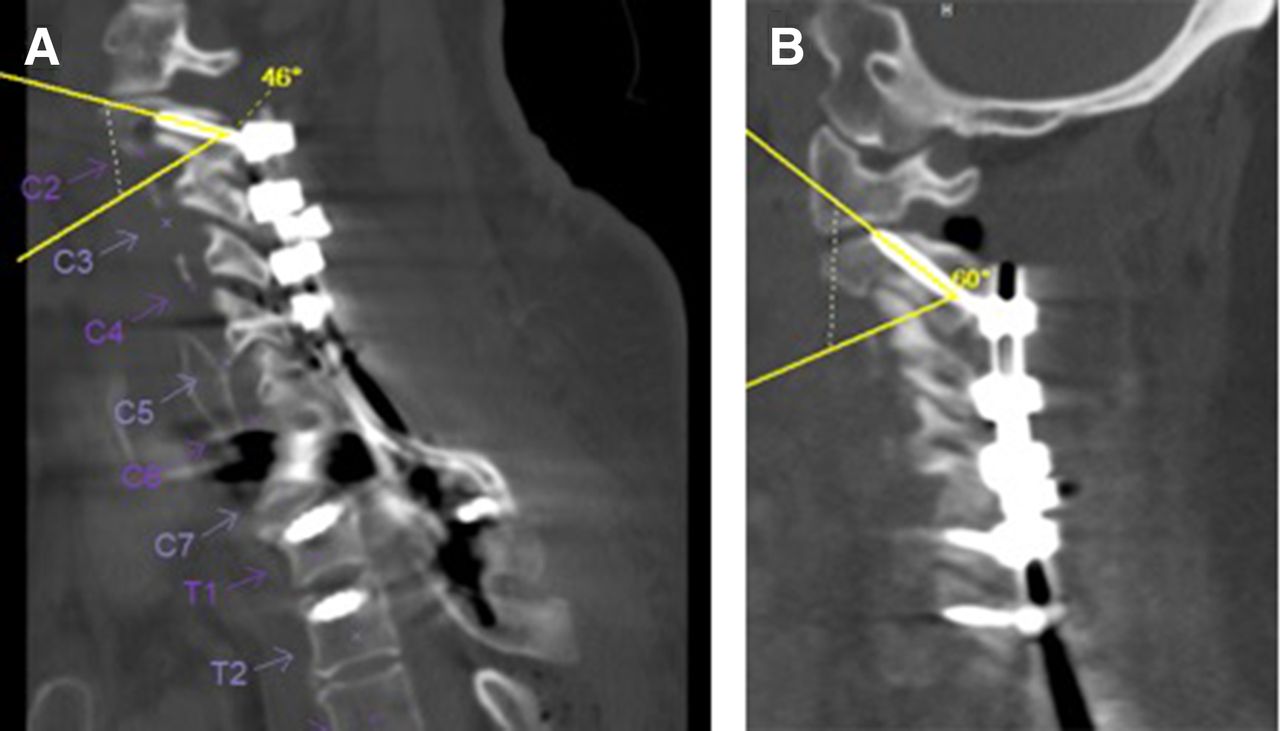
C2 pedicle morphometry including pedicle width, length, height, and transverse angle was measured using preoperative CT images. The sagittal angle of the facet joint, axial and sagittal pedicle screw angles, and screw length were measured using postoperative CT images. The sagittal angle of the C1-C2 facet joint and sagittal screw angle were measured relative to the inferior endplate of C2 on CT images to reduce the effects of head position and/or variations in cervical lordosis (Figure 3).28,29 The axial angle of each pedicle screw was measured relative to the vertebral midline on axial CT images to account for the presence of any vertebral rotation (Figure 4). The bone mineral density of the C2 vertebral body was assessed using preoperative CT images. Hounsfield units obtained from CT images of the lumbar spine have been previously shown to correlate with dual-energy x-ray absorptiometry T scores.30 CT measurements less than 100 Hounsfield units correlate with osteopenia or T scores less than −1.0.

Measurement of the sagittal angle of the C1-C2 facet joint. The inferior endplate of C2 represents the reference line (A). A second line approximates the slope of the C1-C2 facet joint (B). The sagittal screw angles were measured using a similar method.

The axial angle of each pedicle screw was measured relative to a line bisecting the C2 vertebra and aligned with the spinous processes to account for any vertebral rotation.
Statistical Methods
A 2-tailed unpaired t test was used to evaluate any differences between the non-FJP and FJP groups. The cutoff point for significance was defined as P < 0.05. Inter- and intrarater reliability were obtained by using Kappa statistical analysis. All analyses were performed using JMP version 15.0 (SAS Institute, Cary, NC).
Results
Out of the 53 patients who had bilateral C2 screws placed during the study period, 34 patients met the inclusion criteria, with a total of 68 C2 pedicle screws placed. The remainder of the patients had incomplete imaging and were excluded from the study. Seventeen patients were diagnosed with cervical spondylotic myelopathy, 7 with cervical fractures, 6 with metastatic tumors, 3 with cervical kyphosis requiring a pedicle subtraction osteotomy, and 1 with ossification of the posterior longitudinal ligament.
The average age was 66 years in the non-FJP group and 68 years in the FJP group (P = 0.60). There were no neurophysiologic alerts or vertebral artery injuries during the C2 screw placement. Eight screws (14%) penetrated the C1-C2 facet joint. There were 5 Grade 1 and 3 Grade 2 facet joint violations. The Kappa coefficients for inter-and intrarater reliability of the Gertzbein and Robbins grades were 0.87 and 0.93, respectively. The mean sagittal angle of the C1-C2 facet joint was significantly lower in the penetrated (FJP) group compared with the non-penetrated (non-FJP) group (Table 1, Figure 5). The mean sagittal angle of the screws was significantly higher in the FJP group compared with the non-FJP group (Table 1, Figure 6). The mean axial screw angle was significantly lower in the FJP group compared with the non-FJP group (Table 1). The mean screw length was significantly higher for FJP screws compared with the non-FJP screws (Table 1, Figure 7). The mean bone mineral density of the C2 vertebral body was lower in the FJP group compared with the non-FJP group, but this finding did not reach statistical significance (P = 0.06). Pedicle width, length, height, and transverse angle were not significantly associated with FJP (Table 2). Independent reviewers were able to identify FJP on intraoperative fluoroscopic imaging in 2 out of 8 cases (Figure 8). None of the C2 pedicle screws required revision at the latest follow-up (mean 12 months). None of the patients required a cephalad extension of the fusion.
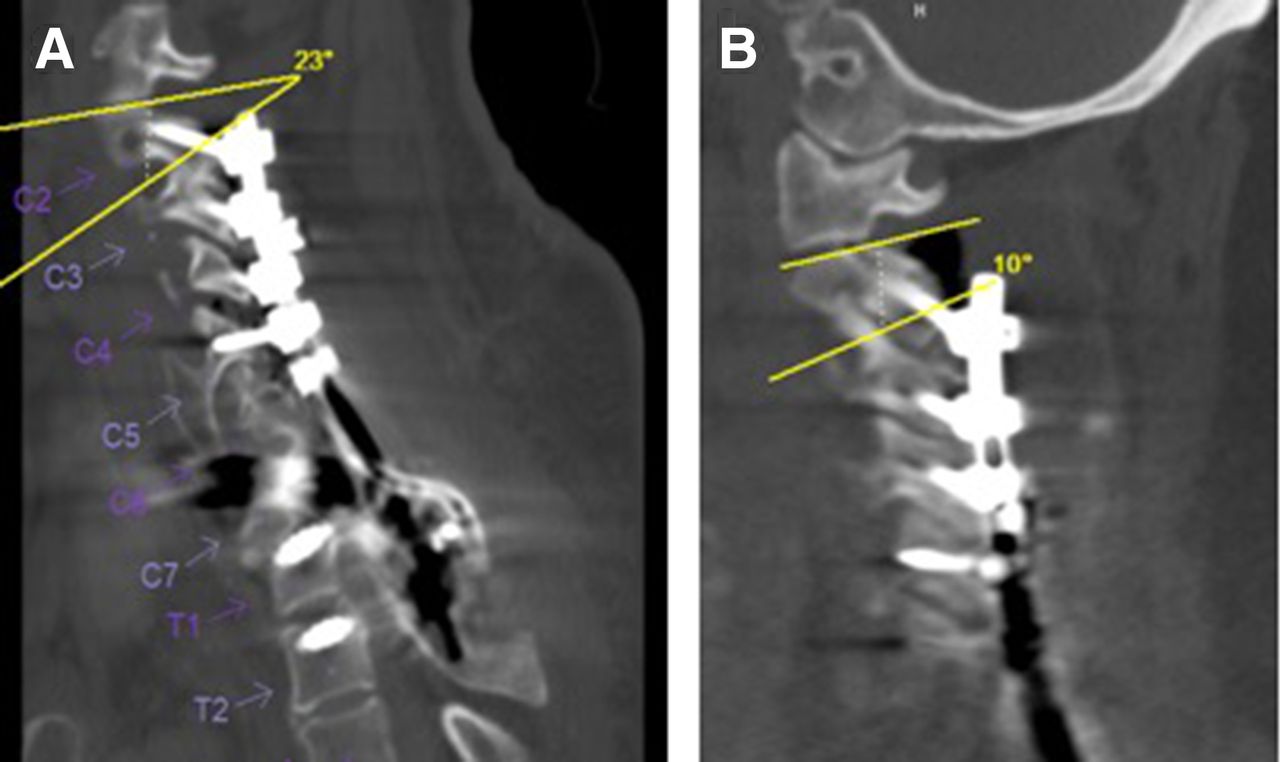
Computed tomography images demonstrating a lower sagittal facet joint angle in the facet joint penetration (FJP) group (B) compared with the non-FJP group (A).

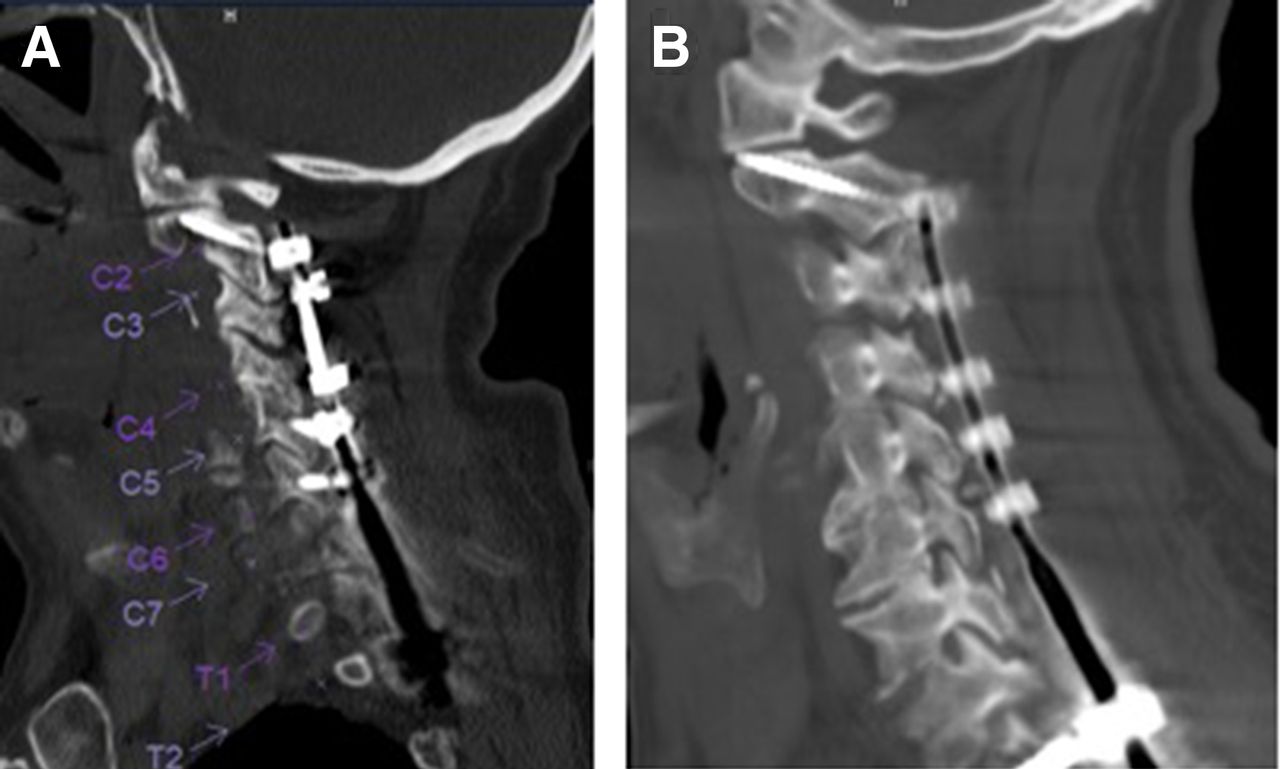
Computed tomography images demonstrating a higher sagittal screw angle in the facet joint penetration (FJP) group (B) compared with the non-FJP group (A).

Computed tomography images demonstrating increased screw length in the facet joint penetration (FJP) group (B, 38 mm) compared with the non-FJP group (A, 26 mm). Both patients had similar sagittal facet joint angles, sagittal screw angles, and axial screw angles (19° vs 21°, 51° vs 53°, and 20° vs 21°, respectively).

Intraoperative fluoroscopic open mouth view demonstrating C1-C2 facet joint penetration.
Comparison of postoperative CT measurements between patients with and without FJP.
Comparison of C2 pedicle morphometry between patients with and without FJP.
Discussion
Our findings demonstrate that lower sagittal angle of the facet joint, higher sagittal angle of the pedicle screw, lower axial angle of the pedicle screw, and longer screw length are associated with a higher risk of C1-C2 FJP. The mean bone mineral density of the C2 vertebral body was lower in the FJP group compared with the non-FJP group, but this finding did not reach statistical significance. Pedicle width, length, height, and transverse angle were not significantly associated with FJP. Careful surgical technique is necessary to avoid FJP when placing C2 pedicle screws under these conditions. Meticulous exposure of the C2 lamina, pars, and C1-C2 interlaminar window as well as palpation and/or direct visualization of the medial wall of the C2 pedicles is crucial to determine the starting point for the C2 pedicle screw and its trajectory. These findings are concordant with our initial hypothesis that more vertically oriented C1-C2 facet joints and longer pedicle screws may predispose to inadvertent C1-C2 FJP, although we also predicted softer bone would predispose to FJP as well.
The results of our study suggest that FJPs may not be apparent on intraoperative fluoroscopic imaging. Similarly, Yoem et al reported in a study of 39 C2 pedicle screws that none of their 8 vertebral artery groove violations was detectable on intraoperative fluoroscopy or postoperative plain radiographs.31 Some authors have suggested that 3-dimensional navigation improves pedicle screw accuracy compared with freehand techniques.32 However, few studies have directly compared the 2 techniques in the cervical spine.33,34 In a retrospective review of 426 C2 pars and pedicle screws, Hlubek et al reported that freehand placement was more accurate than CT-based navigation (acceptable placement was 94% vs 82%, respectively; P = 0.02).35 In their study, the incidence of vertebral artery injury and other complications did not differ between the techniques.
The Gertzbein and Robbins classification has been used in several studies of pedicle screw accuracy in the cervical spine.19,33 Prior studies suggested that FJP contributes to facet degeneration and development of axial symptoms. Most breaches (63%) in our study were Gertzbein and Robbins Grade 1 with less than 50% of the screw diameter entering the joint. A minimal radiographic breach may not represent a true cortical breach due to metal-related artifact on CT imaging.25 Even if present, breaches less than 25% to 50% of the screw diameter represent less than 1 mm of screw length beyond the margin of the cortex.23,25
Despite FJP, at the time of this study no patient from this sample with or without FJP had required a revision surgery for symptomatic adjacent segment disease (ASD) or removal of hardware. The mean follow-up for patients with FJP in our study of approximately 1 year is likely sufficient to address the early radiographic sequelae of facet joint violation such as early arthritis or progressive erosion into C1. It is likely inadequate for symptomatic or operative ASD, especially considering our sample size. We assume there will possibly be some rate of symptomatic or operative ASD at C1-C2 that will present in the future. Although ASD is a leading cause of revision surgery following anterior cervical discectomy and fusion as well as posterior cervical fusion, it is still somewhat unclear whether ASD primarily results from age-related progression of the underlying disease or adjacent segment biomechanical changes related to the fusion.36–40 Clinically, patients may present with new pain, new symptomatic spinal stenosis, or new sagittal or coronal imbalance.41
FJP may lead to altered loading of the facet joint and contribute to eventual facet joint and adjacent segment degeneration.16 However, relatively few studies have investigated clinical outcomes related to FJP in the cervical spine.19,21,27 In a retrospective study of 52 freehand C2 pedicle screws, Punyarat et al reported 2 superior breaches, 1 of which occurred close to the C2 nerve and may have caused occipital neuralgia.23 The authors state that the patient’s symptoms resolved completely with removal of the pedicle screw. In a retrospective study of 40 freehand C2 pedicle screws placed in 24 patients, Pham et al reported 4 FJPs but no clinical sequelae at 6 months of follow-up.24 Other clinical studies have reported an association between FJP of lateral mass screws during cervical laminoplasty and axial pain and stiffness.17,42 Pham et al also noted that “the majority of breaches occurred superiorly as a result of screw length choice and not as a result of error in exposure or anatomical trajectory.”24 This is in line with the results of our study, which did not find a significant association between pedicle width, length, height, and transverse angle and FJP. In a study of 170 C2 pedicle screws, Alosh et al found that a pedicle isthmus diameter less than 6 mm was associated with a nearly 2-fold increased risk of cortical breach; however, any cortical breach was included in their analysis, not only FJP.43 Bydon et al analyzed over 300 freehand C2 pedicle screws and found no association between screw length and medial or lateral breach.44 However, the authors did not include superior cortical violations in their analysis.
The freehand fluoroscopic technique if performed correctly is effective in the placement of C2 pedicle screws. Using the fluoroscopically assisted freehand technique, we were able to place pedicle screws in every patient in whom we had planned preoperatively to perform pedicle screw fixation. The preoperative plan for cephalad extent of the fusion was never altered because of inability to place C2 fixation. The operating room equipment necessary for this technique includes Mayfield head clamp, wine cork or radiolucent bite block, and radiolucent table. The wine cork or radiolucent bite block placed in the mouth is critical in obtaining the open mouth to visualize the C2 pedicle outline for the starting screw position. An inability to obtain a perfect open mouth view due to smaller or tighter jaw opening or metallic dental work producing interference with the beam can present a significant challenge. The FJP detailed in this study occurred early in the inclusion period, prior to the authors becoming aware that fluoroscopy is not always sufficient to detect intraoperative FJP. The subsequent steps the authors undertook included rigorous following of the previously detailed protocol. In addition, although typically the screw length is determined intraoperatively, we generally limited screw length to 24 mm or less to limit FJP. These steps significantly limited FJP during subsequent operations.
Limitations of the study include the lack of clinical assessments of C1-C2 degeneration over time. Future studies should compare patient-reported outcomes and rates of C1-C2 degenerative disease in patients with and without FJP. In addition, none of the C2 pedicle screws in our study required revision at the latest follow-up; therefore, future studies are necessary to investigate the clinical significance, if any, of facet joint violations in the cervical spine. Furthermore, a larger sample size may have been sufficiently powered to detect statistically significant differences in bone mineral density between FJP and non-FJP groups. Osteoporotic patients may require increased cortical purchase and longer C2 screws to achieve adequate fixation, thus confounding the association between bone mineral density and FJP. Also, a larger sample size may allow for comparisons between patients with lower Grade 1 and higher Grade 2 facet joint violations. Additionally, this study was limited to the freehand technique, and navigation and robotics were not included. The higher sagittal angle of the pedicle screw was found to be associated with a higher risk of FJP; however, navigation or robotics may be able to decrease the sagittal screw angle by allowing for a higher starting point than the freehand technique.
Adjacent segment degeneration is a common sequelae of cervical spine arthrodesis and results in recurrent symptoms, patient pain and disability, as well as possible revision surgery to extend the surgical construct. Violation of the unfused facet joints above the cervical fusion construct will result in damage to the articular cartilage of the facet, possibly causing facet arthrosis and progressive degeneration. The C2 vertebra has a unique bony anatomy and close proximity to vital structures such as vertebral arteries and the spinal cord that makes C2 instrumentation quite challenging. With the ever-increasing number and invasiveness of complex cervical posterior reconstruction, C2 pedicle screw placement is becoming more common. This would potentially increase the number of patients with inadvertent violation of the unfused C1-C2 facet joint, setting off a cascade of ASD, possible proximal junctional kyphosis, suboccipital pain, and limited cervical rotation. Thus, any potential guidance on how to avoid the violation of the C1-C2 facet joint by instrumentation is of great importance.
Conclusion
Several anatomical and technical factors may increase the risk of C1-C2 FJP during placement of C2 pedicle screws using a fluoroscopically assisted freehand technique, including a lower sagittal facet angle, higher sagittal screw angle, lower axial screw angle, and screw length >24 mm. Intraoperative fluoroscopy is not always adequate to avoid C1-C2 FJP, underscoring the importance of preoperative planning and limiting screw length. None of the C2 pedicle screws in our study required revision at the latest follow-up.
Footnotes
Funding This work was funded entirely by internal, institutional research funds. No external funding was received for this study.
Declaration of Conflicting Interests The authors declare that the study was performed in the absence of any commercial or financial relationships that could be considered a potential conflict of interest.
Disclosures Dimitriy Kondrashov reports grants or contracts, royalties or licenses, consulting fees, and support for attending meetings and/or travel from Spineart and consulting fees from SI-Bone. The remaining authors have no disclosures.
IRB Approval Our institution’s institutional review board approved this study and granted a waiver of informed consent.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.