


The December 2023 issue of The International Journal of Spine Surgery (IJSS) is dedicated to examining complications and outcomes in spine surgery. Complications, and their honest assessment, are intimately associated with improving outcomes. The journal’s parent organization, the International Society for the Advancement of Spine Surgery (ISASS), is indelibly linked to spinal arthroplasty, a specialty that was advanced by ISASS from its inception as the Spine Arthroplasty Society in 2000. Cervical artificial disc replacement (c-ADR) is the most successful spinal arthroplasty procedure and one of the most studied devices in the history of spinal surgery. This success can be attributed, in large part, to the unprecedented volume of scientific evidence supporting the safety and efficacy of cervical arthroplasty. The continued adoption and evolution of this technology are dependent on expanding that firm evidence basis, including an unbiased examination of complications. The key to improving outcomes is complication avoidance.
The ideal indications of cervical arthroplasty include radiculopathy due to soft central/paracentral disc herniation, 1- and 2-level, in the setting of early, focal spondylosis. Following the US Food and Drug Administration approval of the first c-ADR device in 2007, cervical arthroplasty became more widely adopted, and with increasing popularity, indications expanded in real-world practice. As with any other procedure, as usage expanded, complications became more evident. The well-characterized complications of c-ADR include (a) dislocation/expulsion, (b) subsidence, (c) osteolysis, (d) recurrent radiculopathy, (e) focal device kyphosis (FDK), and (f) heterotopic ossification (HO). One of the central themes of complication avoidance is understanding the mechanism of failure, whether the complication is related to surgical indication/patient selection, surgical technique, or the device itself.1
As with any surgical procedure, patient selection is paramount to a successful outcome. Special attention must be paid to the presence of significant facet disease, extent of bony foraminal stenosis, osteopenia/osteoporosis, and degree of cervical spondylosis. Cervical computed tomography is advised in the majority of cases to evaluate the bony anatomy. Advanced facet disease limits motion and predisposes one toward recurrent radicular symptoms due to foraminal stenosis. Osteoporosis predisposes one to subsidence, displacement, and expulsion.
Proper surgical techniques, with attention to detail and symmetry, can minimize several potential complications. Adequate posterior release requires resection of the posterior longitudinal ligament and proximal, symmetrical foraminotomies with proximal uncovertebral joint resection, which facilitates disc space mobilization and allows for proper device sizing and optimal placement. Lack of proper release and mobilization predispose one to displacement and expulsion. Proper sizing is crucial as maximizing width from uncovertebral joint to uncovertebral joint essentially self-centers the device in the midline. Overdistraction of the disc space or undersizing of the device can both lead to displacement/expulsion. Fluoroscopic images should be obtained prior to closure; the best time to reposition a suboptimally placed device is at the index surgery.1
HO does not typically result in negative clinical outcomes or require reoperation, but advanced HO limits motion. Nearly every c-ADR device shows varying degrees of HO, but devices that require exposure of cancellous bone or significant drilling may predispose a patient to HO. The likelihood of bridging HO may be diminished by eliminating or minimizing the use of high-speed drilling. When the high-speed drill is necessary, irrigate copiously and use bone wax liberally on exposed cancellous bone, especially when using devices with keel-based fixation. Proper device sizing with maximal endplate coverage may also decrease HO incidence by limiting exposed bony surfaces. The use of postoperative nonsteroidal anti-inflammatory drugs routinely for 2 to 4 weeks is advised to potentially decrease the occurrence of HO.2
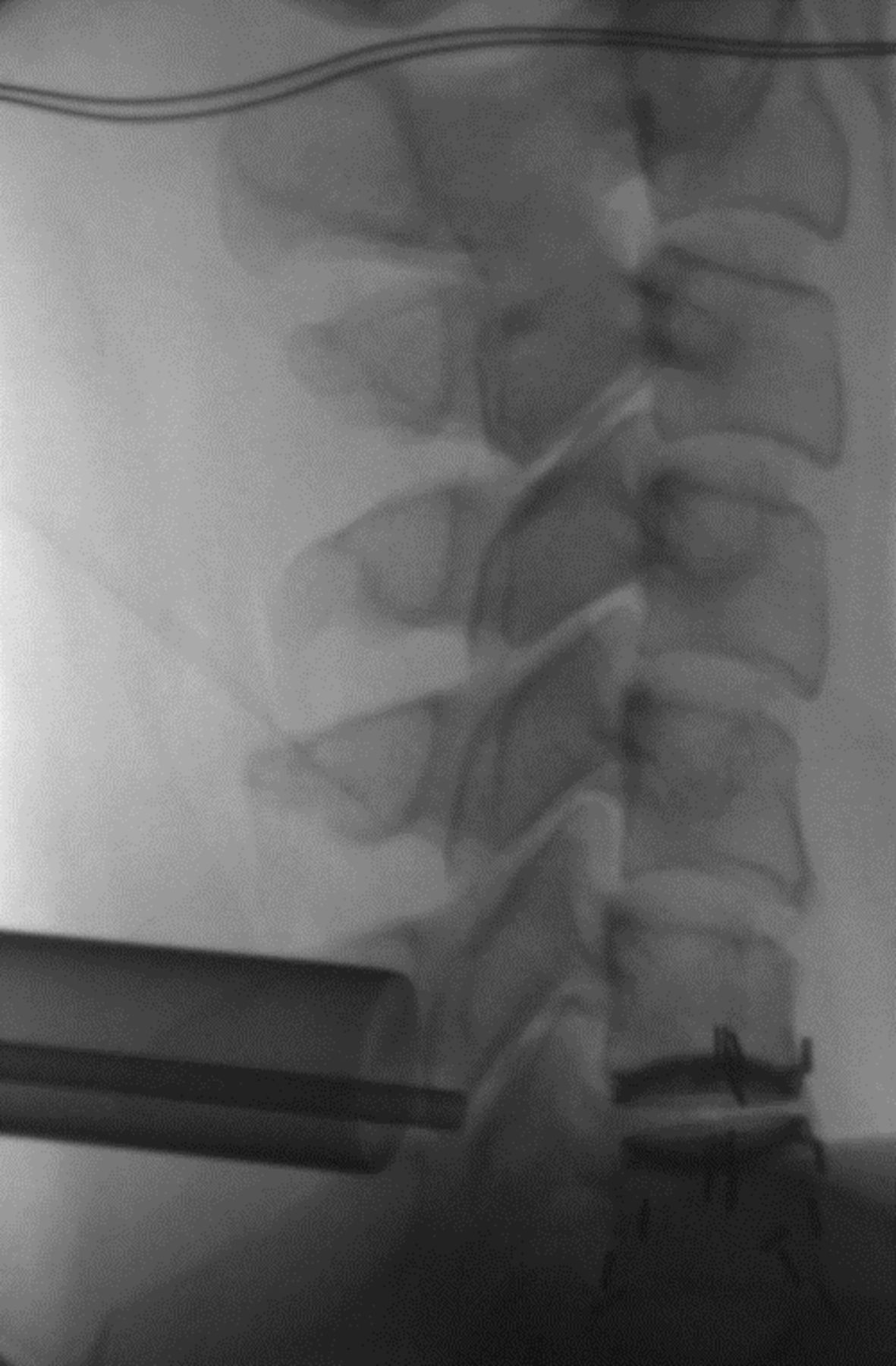
FDK (Figure 1) is another complication that also does not necessarily have a clinical correlate but limits motion. FDK may rarely lead to dislocation and core expulsion. Biomechanically, devices with less constraint may predispose to FDK, especially in “off-label” adjacent to fusion indications. Using more constrained devices with robust, keel-based fixation should be considered in these biomechanically challenging indications.

Focal device kyphosis.
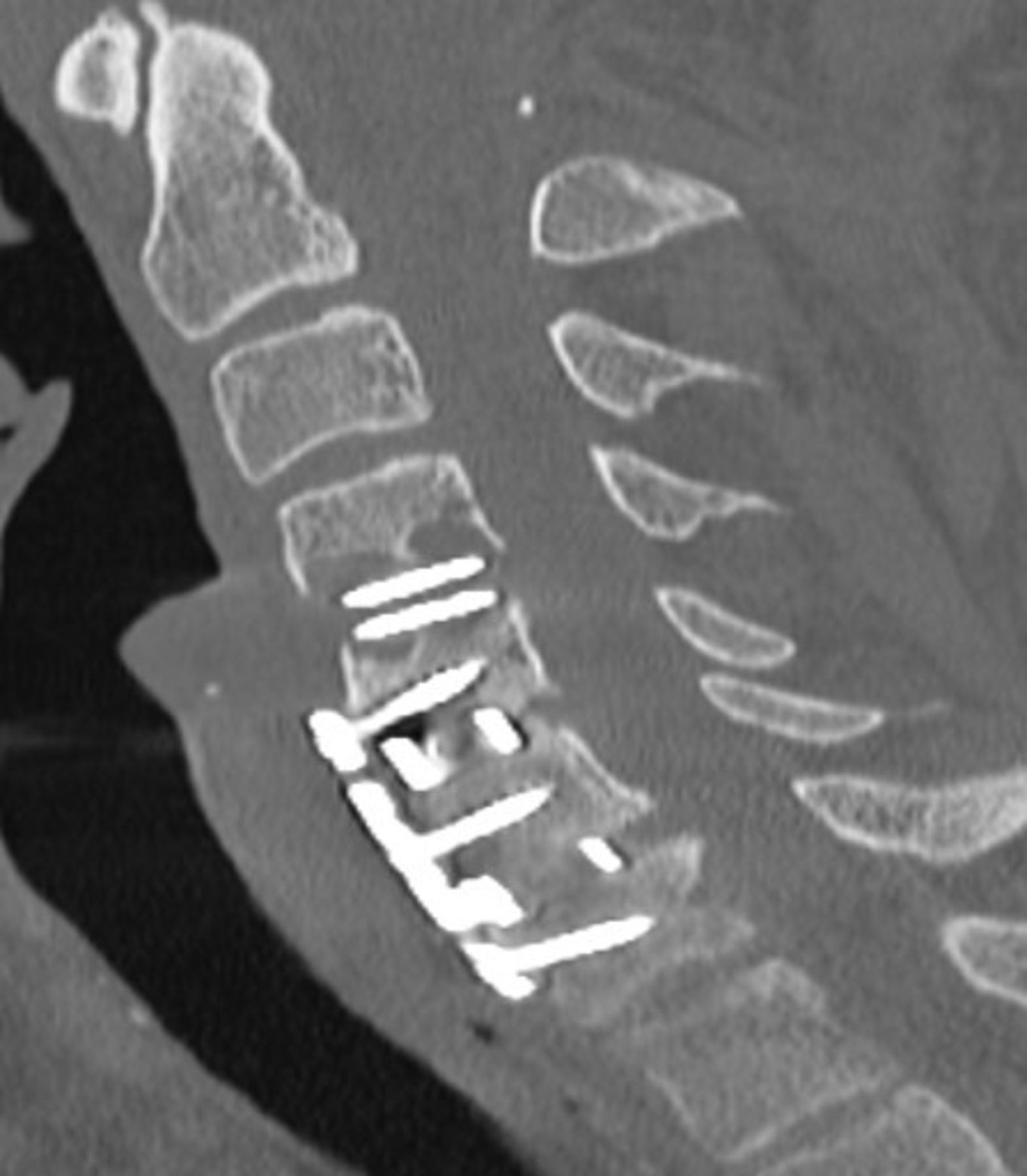
Osteolysis (Figure 2) is a potentially destabilizing complication, which may not become evident until several years following c-ADR. Metal-on-metal devices or circumstances where core wear leads to direct device endplate-to-endplate contact may predispose one to osteolysis. Intermediate to long-term complications, such as osteolysis, require extended surveillance following c-ADR placement with routine flexion and extension radiographs as well as a low threshold to obtain computed tomography imaging.3

Osteolysis.
Revision strategy is strongly correlated with the mode of failure. Residual/recurrent foraminal stenosis is ideally salvaged with tubular posterior cervical laminoforaminotomy. This procedure is complementary to c-ADR as it is both minimally invasive and motion preserving and avoids the previous operative approach (Figure 3). Osteolysis, as well as subsidence, dislocation, and expulsion, are typically treated with anterior revision. In contradistinction to lumbar artificial disc replacement, anterior cervical revision can be accomplished in a straightforward fashion with repeat artificial disc replacement, anterior cervical discectomy and fusion, or corpectomy.4

Tubular posterior laminoforaminotomy following cervical artificial disc replacement.
Cervical arthroplasty complications are relatively rare and typically not catastrophic. Cervical arthroplasty revision, posterior or anterior, is generally straightforward, not necessarily requiring an exposure surgeon. The best way to prevent revision surgery and improve outcomes is complication avoidance.
Footnotes
Funding The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Globus Medical—Consultant/Royalties; Spine Wave—Consultant/Stock/Royalties; Medtronic—Consultant/Royalties; Integrity Implants—Royalties; and Premia Spine—Stock. None are pertinent to the contents of this manuscript.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.