


Abstract
Background There has been heightened interest in performing percutaneous lumbar interbody fusions (percLIFs) through Kambin’s triangle, an anatomic corridor allowing entrance into the disc space. However, due to its novelty, there are limited data regarding the long-term benefits of this procedure. Our objective was to determine the long-term efficacy and durability of the percutaneous insertion of an expandable titanium cage through Kambin’s triangle without facetectomy.
Methods A retrospective review of patients undergoing percLIF via Kambin’s triangle using an expandable titanium cage was performed. Demographics, visual analog scale (VAS) scores, Oswestry Disability Index (ODI), radiographic measurements, perioperative variables, and complications were recorded. VAS, ODI, and radiographic measurements were compared with baseline using the generalized estimating equations assuming normally distributed data. Fusion was assessed with computed tomography (CT) at 1 and 2 years after the procedure.
Results A total of 49 patients were included. Spondylolisthesis, lumbar lordosis (LL), sacral slope, pelvic tilt, and anterior/posterior disc space height were all significantly improved postoperatively at each time point of 3, 6, 12, and 24 months (P < 0.001). Pelvic incidence—LL mismatch decreased significantly at each follow-up (P < 0.001) with a mean reduction of 4° by 24 months. VAS back scores reduced by >2 points at the 6, 12, and 24 month follow-ups. ODI scores reduced by >15 points at the 12- and 24-month follow-ups. Of the patients who had 1- and 2-year CT images, fusion rates at those time points were 94.4% (17/18) and 87.5% (7/8), respectively. The mean annual rate of surgically significant adjacent segment disease was 2.74% through an average follow-up of 2.74 years.
Conclusion These results highlight that percLIF, a procedure done without an endoscope or facetectomy, can be performed using an expandable titanium cage through Kambin’s triangle with excellent radiographic and clinical results.
Clinical Relevance percLIF via Kambin’s triangle is a safe and succesful procedure with long-term improvements in both clinical and radiographic outcomes.
Level of Evidence 3.
- expandable cage
- Kambin’s triangle
- lumbar interbody fusion
- minimally invasive surgery
- percutaneous spinal fusion
- patient-reported outcomes
- spinopelvic parameters
INTRODUCTION
Minimally invasive lumbar interbody fusion has seen a recent surge in its use, mainly stemming from the current literature that reveale the advantages over historical open surgical approaches.1–3 By placing either a biomechanical device or bone graft in the intervertebral disc space, fusion can be obtained while also aiding in the correction of disc space height, lordosis, and spondylolisthesis, making it a valuable treatment in the subset of refractory symptomatic patients who suffer from degenerative lumbar spine disease.4–6
While there are various anatomic approaches for lumbar interbody fusions, there have been developments in novel corridors to the disc space that offer the familiarity of the prone position, the advantage of minimal muscle disruption, and minimization of exiting nerve root (ENR) injury. Morgenstern et al described one such approach as the percutaneous lumbar interbody fusion (percLIF) through Kambin’s triangle.7–10 Their work, however, utilized an endoscope to visualize entry into the disc space. Additionally, studies have found that the percLIF is still limited by the choice of implant design as the anatomic corridor has an average area ranging from 59.96 mm2 at L1–L2 to 99.60 mm2 at L5–S1.11–13 Other options such as implanting static, nonexpandable cages or porous allograft-containing mesh have been explored, but the benefits of expandable cages have made this option the more common alternative.14,15
While there are several studies demonstrating feasibility of percLIF, there are limited long-term data on the postoperative patient-reported scores and radiographic outcomes, especially for patients with expandable interbody implants. We previously published an initial case series of 16 patients with 1-year follow-up regarding this technique.16 This is the first reported study demonstrating the long-term outcomes of patients with Grade 1 spondylolisthesis undergoing lumbar fusion through the percLIF approach utilizing an expandable titanium cage.
METHODS
Study Design
The authors performed a single-center, single-surgeon retrospective review of patients with the following inclusion criteria: (1) age ≥18 years, (2) undergoing percLIF via Kambin’s triangle, (3) utilizing an expandable titanium cage interbody device, and (4) treatment of Grade 1 spondylolisthesis from July 1, 2018, to October 24, 2022 (Figure 1). Patients who had prior surgical correction of their lumbar spine, including decompressions or fusions, were not included in this study. Demographics, visual analog scale (VAS) scores, Oswestry Disability Index (ODI) scores, and complications, including surgically significant adjacent segment disease (ASD), postoperative radiculopathies, and readmissions, were recorded at the 3-, 6-, 12-, and 24-month timepoints.

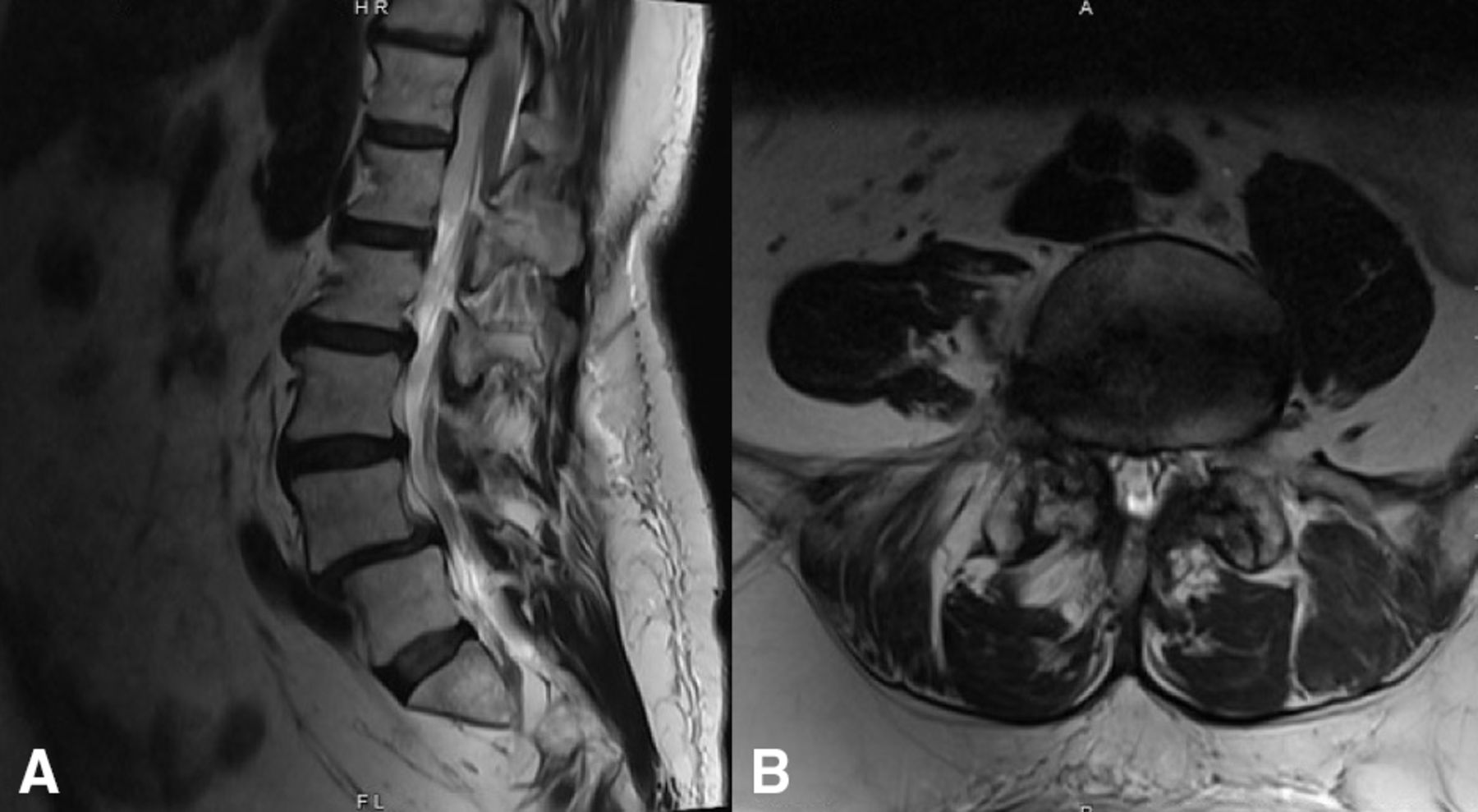
Preoperative T2 magnetic resonance imaging showing Grade 1 spondylolisthesis of the L4–L5 level on the (a) sagittal view and right-sided foraminal compression of the exiting nerve root on the (b) axial slice.
Radiographically, postoperative standing lumbar x-rays at 3, 6, 12, and 24 months were used to measure the anterior disc space height, posterior disc space height, and severity of spondylolisthesis. Additionally, lumbar lordosis (LL), sagittal vertical axis, pelvic incidence (PI), pelvic tilt (PT), and sacral slope (SS) were measured from full-length standing x-rays (Figure 2). Fusion, defined as either bridging disc space or posterolateral fusion without evidence of implant fracture, was assessed on 1- and/or 2-year postoperative computed tomography (CT) scans. In the instance where a patient did not have a 2-year CT, their lumbar radiographs were examined for implant fracture, screw migration, or peri-implant lucency. If any of these findings were present, the patient’s spine was considered “non-fused.” A board-certified, independent neuroradiologist graded the fusions.

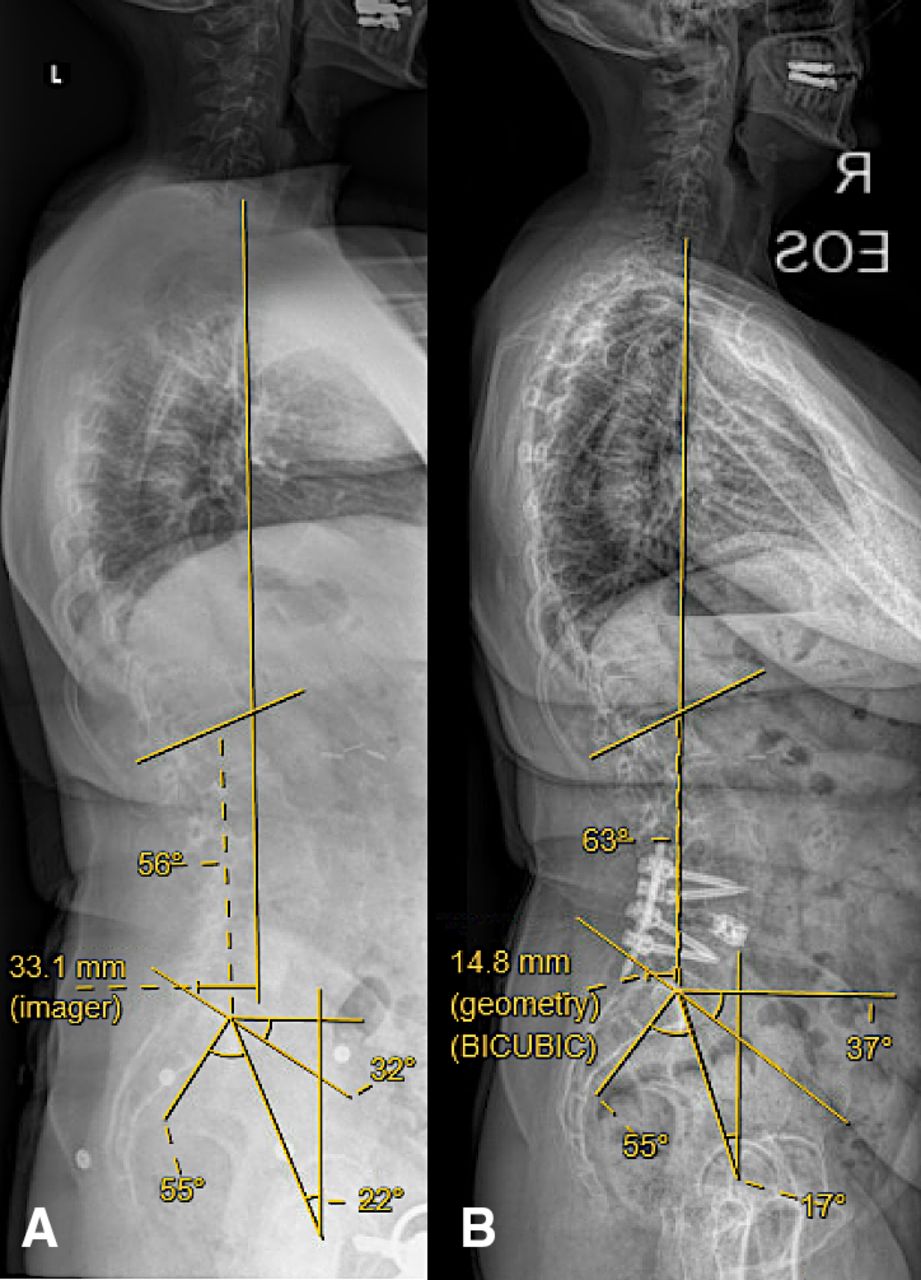
Full-length standing x-ray images showing the improvement in spinopelvic parameters (lumbar lordosis, sagittal vertical axis, pelvic tilt, pelvic incidence, and sacral slope) comparing the (A) preoperative to (B) 1-year follow-up images.
Key Surgical Steps
The surgical protocol was as described in Wang et al.16 If patients receive general anesthesia, electromyography (EMG) monitoring needles are placed into the bilateral lower extremities following intubation. For patients undergoing awake surgery, spinal anesthesia is obtained before lead placement. The patient is then flipped prone on a Jackson table with their arms aimed 90° toward the head. Percutaneous placement of pedicle screws occurred first, with the insertion done via stab or Wiltse incisions per surgeon preference. Next, a paramedian stab incision is made 6 cm from the midline. A blunt EMG probe is used to pierce the fascia and aimed at Kambin’s triangle, and continuous EMG signals were monitored to ensure no damage to the surrounding nervous tissue. If there was no firing at 5 mA when the disc was entered, this was considered a safe entry to the disc space. This threshold was selected based on prior research showing that a threshold above 4 mA led to reduced instances of dorsal root ganglion and nerve root irritation with a specificity of above 80% and a sensitivity of 60%.17,18 Dilators (Spineology, Minneapolis, MN) were subsequently introduced over the blunt EMG probe, and a working channel was docked just inside the annulus to protect surrounding structures. The delivering cannula diameter was expanded up to 8 mm. Disc material was removed with the combination of a pituitary rongeur, fan-blade shaver, curette, and rotating metal-bristle brushes. The discectomy was confirmed by placing a balloon into the disc space and filling it with radio-opaque dye. Therefore, there was no use of an endoscope. In terms of key equipment, a special inserter (Envoy, Spineology, Minneapolis, MN) was used to help place the ELITE Expandable Cage (Spineology, Minneapolis, MN). The cage was inserted at a starting height of 7 to 10 mm and expanded to a final height of a maximum of 10 to 15 mm. The cages can be filled with allograft cortical fibers (Musculoskeletal Transplant Foundation, Edison, NJ) and/or bone morphogenetic protein (BMP; Medtronic, Minneapolis, MN). All cages are 10 mm wide and can come in 0°, 6°, and 12° of lordosis. Cage sizes were determined from preoperative imaging, spinopelvic parameters, desired postoperative lordosis goal, and intraoperative fit. Fluoroscopy was used to confirm appropriate placement of all instrumentation (Figure 3).
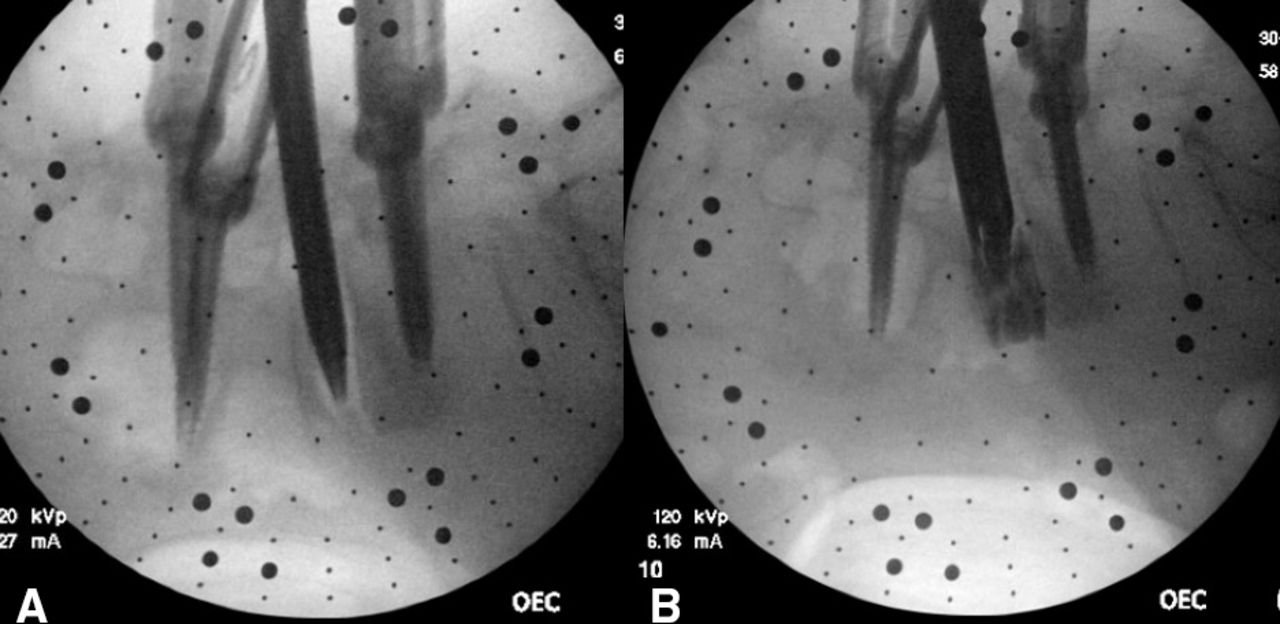
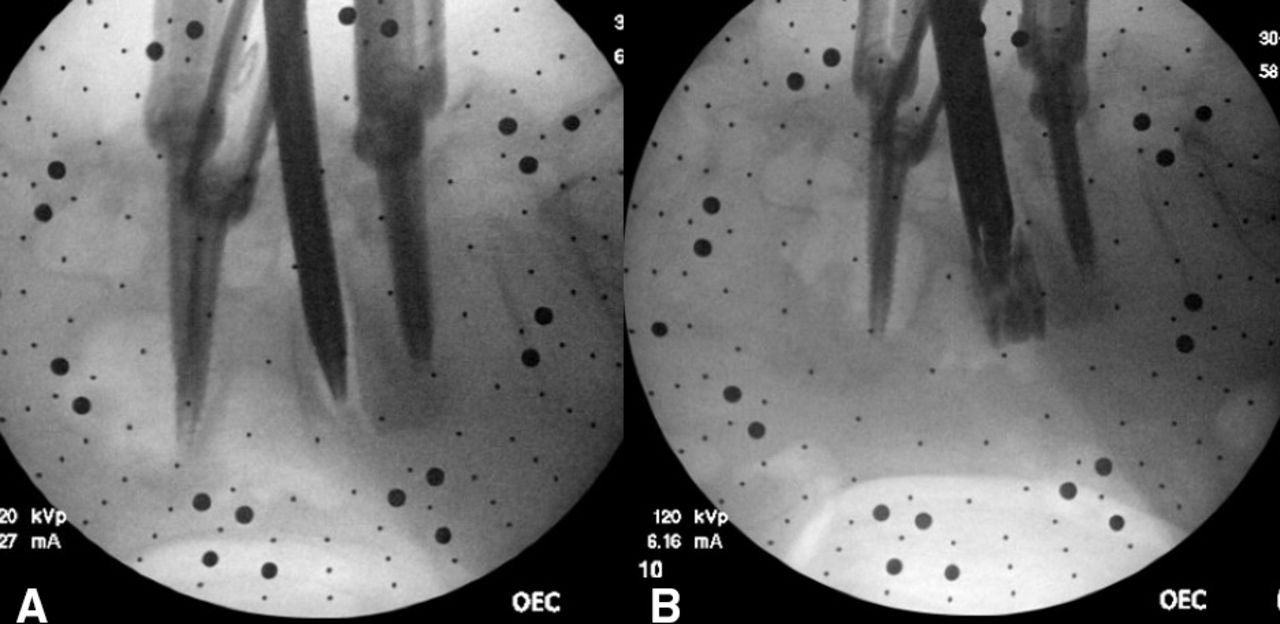
Sequential fluoroscopic imaging showing (A) a blunt electromyography-guided probe traversing Kambin’s triangle into the disc space. (B) After satisfactory end plate preparation, an introducer is placed at the center of the disc space and loaded with an expandable cage.
Statistical Methods
Data were initially compiled in Microsoft Excel (Microsoft Inc, Redmond, WA). Continuous variables were summarized with means, SDs, quartiles, and ranges. Categorical variables were summarized with frequencies and percentages. Postoperative radiographic outcomes at 3, 6, 12, and 24 months were compared with baseline using the generalized estimating equations with an identity link assuming normally distributed data. Within-subject correlation was accounted for by specifying an AR(1) correlation structure. Surgically significant ASD was analyzed using the life table method. Annual incidence of surgery for ASD was calculated by dividing the number of new ASD surgery in each year by the effective sample size in that year. ASD surgery-free probability was plotted using the Kaplan-Meier method. Analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC). Statistical significance was determined if P < 0.05. No adjustment for multiple testing was conducted because of the exploratory nature of this single-center, single-surgeon retrospective study. To determine clinical significance for patient-reported outcomes, a 2-point reduction on a 10-point VAS was considered clinically successful.19–21 An improvement evidenced by a 15-point decrease on the 100-point ODI scale was considered clinically successful.19–21
RESULTS
Demographic Data
Forty-nine (49) patients were identified as having a Grade 1 lumbar spondylolisthesis who underwent percLIF, and all patients were followed postoperatively through at least 2 years. Thirty of the 49 patients were women (61.2%) and 19 were men (38.8%). The mean age was 61.4 ± 11.4 years. The mean body mass index was 31.3 ± 5.1 kg/m2 with a range of 18.9 to 42.1 kg/m2. The most common operative level was L4–5 with 27 patients (55.1%), followed by L3–4 with 10 patients (20.4%), L5–S1 with 9 patients (18.4%), and L2–3 with 3 patients (6.1%; Table 1).
Demographic data.
Hospitalization Data
The mean operative time was 190.4 ± 73.9 minutes, with a mean estimated blood loss of 70.3 ± 82.7 mL. Six (12.2%) surgeries were done with the patient awake under spinal anesthesia instead of general anesthesia. None of the surgeries required conversion to the more traditional open or minimally invasive approaches. Average hospital stay was 3.4 ± 2.9 days, where 13 (26.5%) patients were discharged on postoperative day 1 (Table 2). In terms of cage dimensions, the most common cage used was the 8 to 11 mm cage (51.0%) followed by the 9 to 13 mm cage (38.8%). Across the whole cohort, the average final expanded height of the cages was 11.8 mm. Twenty-five (51.0%) of the cages were filled with both cortical fibers and BMP, while 24 (49.0%) contained only cortical fibers.
Hospitalization and operative data.
Complications
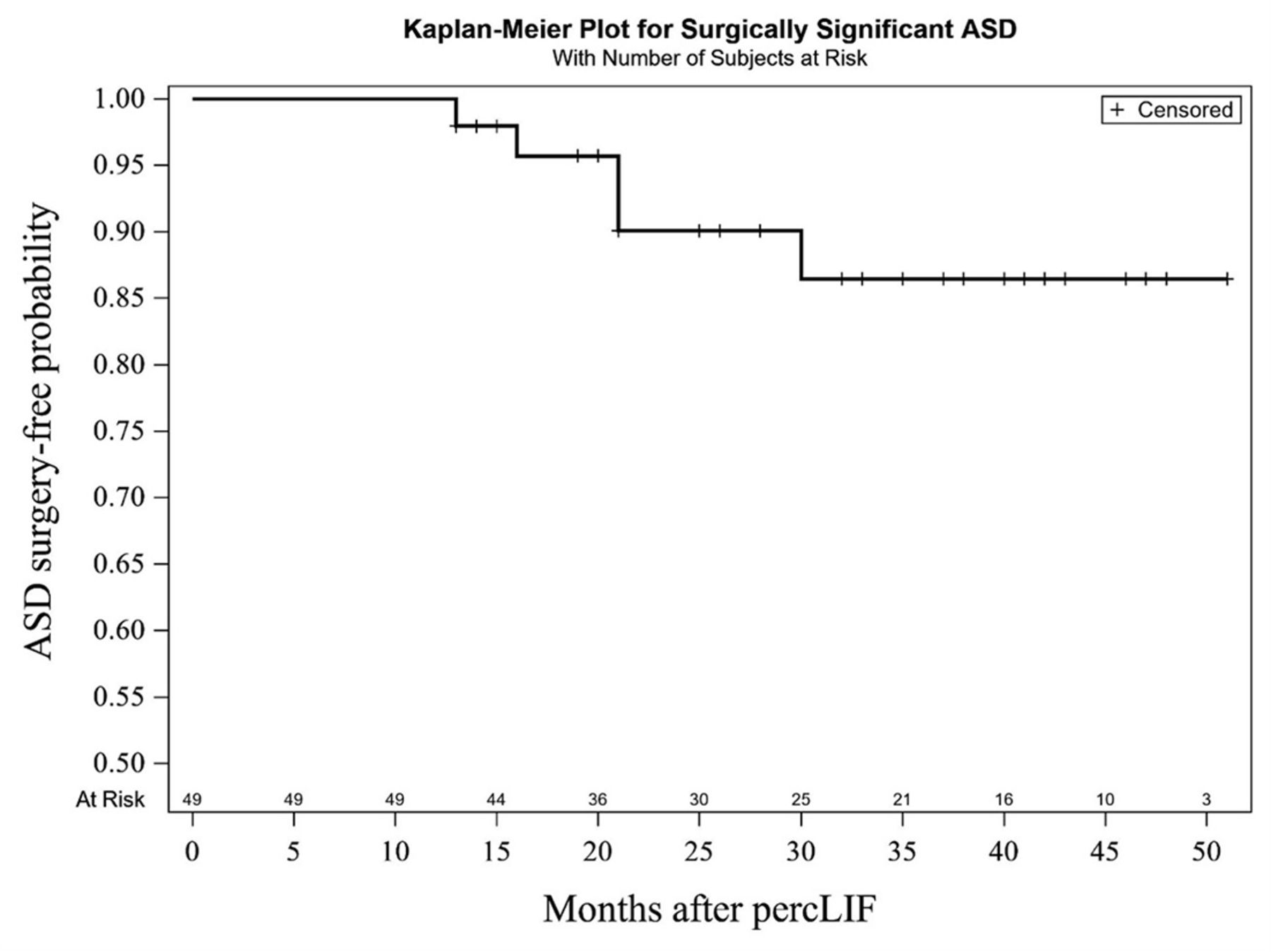
No intraoperative complications were noted. Six patients (12.2%) developed new postoperative radiculopathies; however, 4 of those 6 patients developed these symptoms secondary to a misplaced or breeched pedicle screw. Those 4 (8.16%) patients required removal and redirection of pedicle screws after their procedure due to new onset radicular symptoms, which promptly resolved following revision. The remaining 2 patients were readmitted for (1) complex regional pain syndrome and (2) persistent postoperative left lower extremity pain. For the patient with complex regional pain syndrome, it is to be noted that their preoperative radicular pain and majority of their back pain resolved after surgery, but they had been dealing with a chronic burning sensation on the lateral aspect of their right foot, which was on the same side that the interbody cage was placed. The second patient was admitted to an acute rehabilitation facility after hospital discharge, and their symptoms of left lower extremity pain, which was on the same side that the interbody cage was placed, significantly improved after treatment. One additional patient was readmitted for a syncopal episode secondary to a hypotensive episode 1 month after initial discharge. Only 3 (6.12%) patients were readmitted in total. In terms of ASD, 5 (10.2%) patients required an extension of fusion (Table 2). The mean time to revision was 20.2 ± 6.46 months, with the first revision occurring 13 months after surgery and the last occurring at 30 months after surgery. The mean annual rate of surgically significant ASD at 5 years after surgery was 2.74%, with an average length of follow-up of 2.74 years (Figure 4, Table 3). One (2.04%) patient had failure at the level below their construct, 3 (6.12%) had failure at the level above their construct, and 1 (2.04%) had failure at levels both above and below.
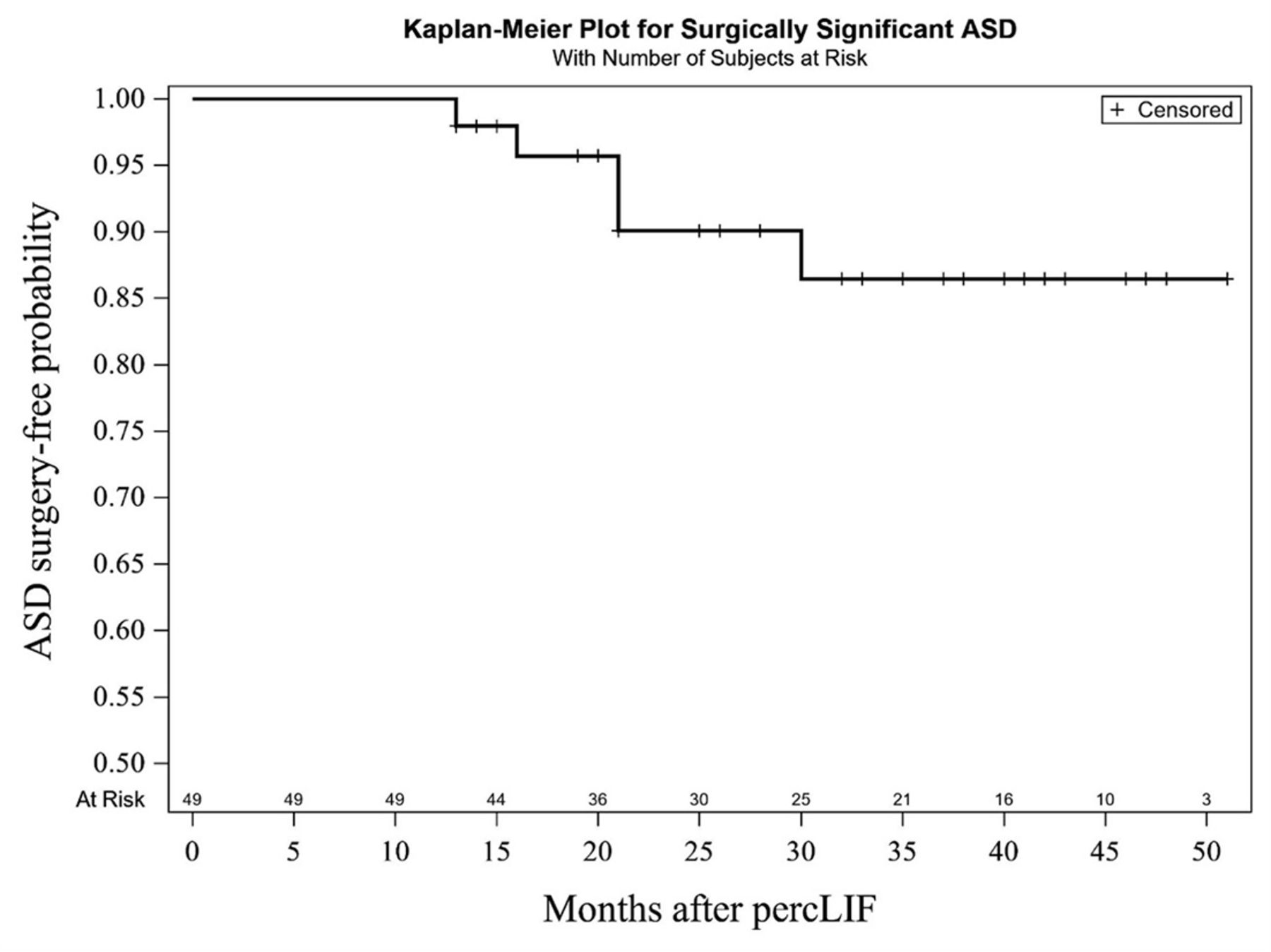
Survivorship model of surgically significant ASD over time. ASD, adjacent segment disease; percLIF, percutaneous lumbar interbody fusion.
Annual incidence of surgery for ASD.
Radiographic Data
Baseline spondylolisthesis was 7.5 ± 3.7 mm and improved postoperatively to 4.1 ± 2.1 mm at 3 months, 4.3 ± 2.9 mm at 6 months, 3.4 ± 2.5 mm at 12 months, and 2.6 ± 2.8 mm at 24 months (P < 0.001 for each time point). Baseline anterior disc space height was 7.5 ± 3.2 mm and improved postoperatively to 12.7 ± 2.8 mm at 3 months, 12.5 ± 2.8 mm at 6 months, 12.7 ± 3.0 mm at 12 months, and 13.6 ± 3.2 mm at 24 months (P < 0.001 for each time point). Baseline posterior disc space height was 4.9 ± 2.2 mm and improved postoperatively to 9.0 ± 2.8 mm at 3 months, 8.1 ± 2.5 mm at 6 months, 8.1 ± 3.0 mm at 12 months, and 8.1 ± 2.1 mm at 24 months (P < 0.001 for each time point; Figure 5). In terms of spinopelvic parameters, LL, PT, and SS were all significantly improved at each follow-up date (P < 0.001; Table 4). PI-LL mismatch decreased from a baseline of 6.4°±10.5° at each time point significantly (P < 0.001; Figure 6, Table 4). Of the patients who had 1- and 2-year CT scans, fusion rates per previous criteria were 94.4% (17/18) and 87.5% (7/8) at those time points, respectively. Of the patients who received a 2-year radiograph instead of a CT scan, 100% (10/10) did not show any signs of peri-implant lucency or instrumentation failure.

Preoperative (A) extension and (B) flexion standing lumbar x-rays showing reduced anterior and posterior disc space heights at the L4–L5 level. Two-year postoperative (C) extension and (D) flexion films highlighting the maintained long-term increase in disc space heights.
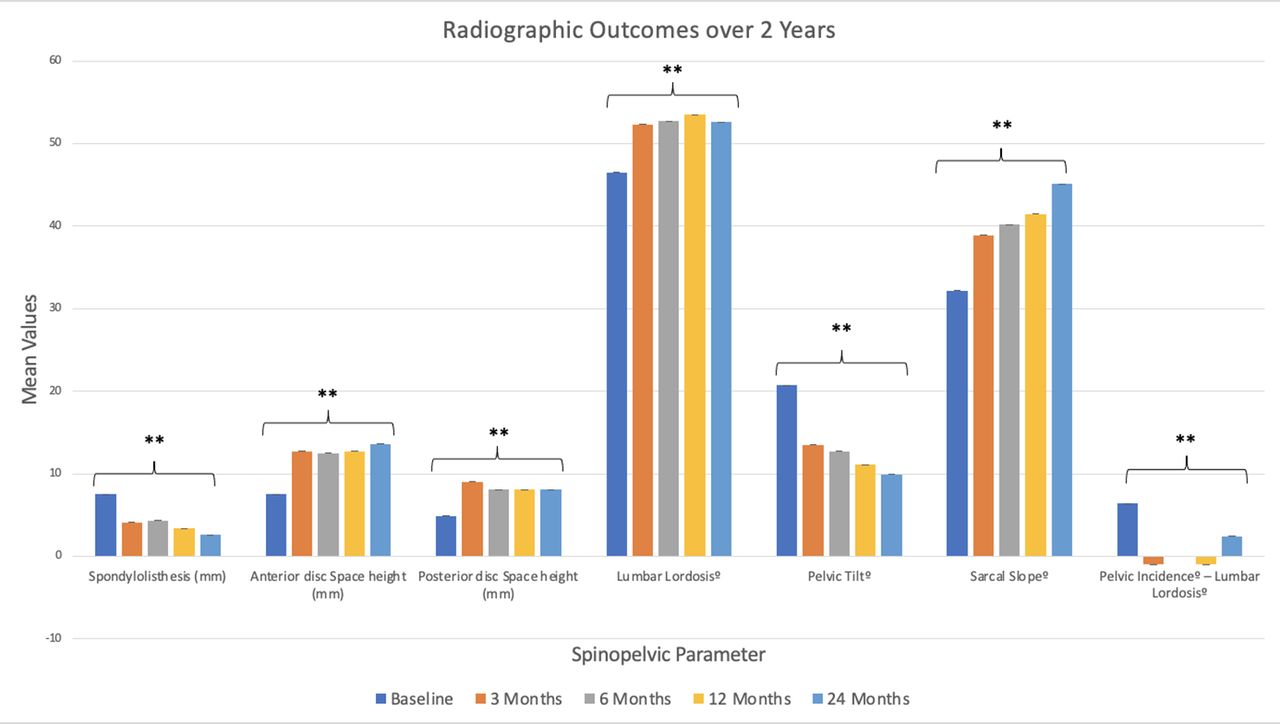
Radiographic outcomes over a 2-year follow-up revealing significant improvement compared with baseline values across each parameter at every recorded postoperative time point. ** P < 0.001.
Radiographic and spinopelvic parameters data.
Patient Self-Reported Outcomes
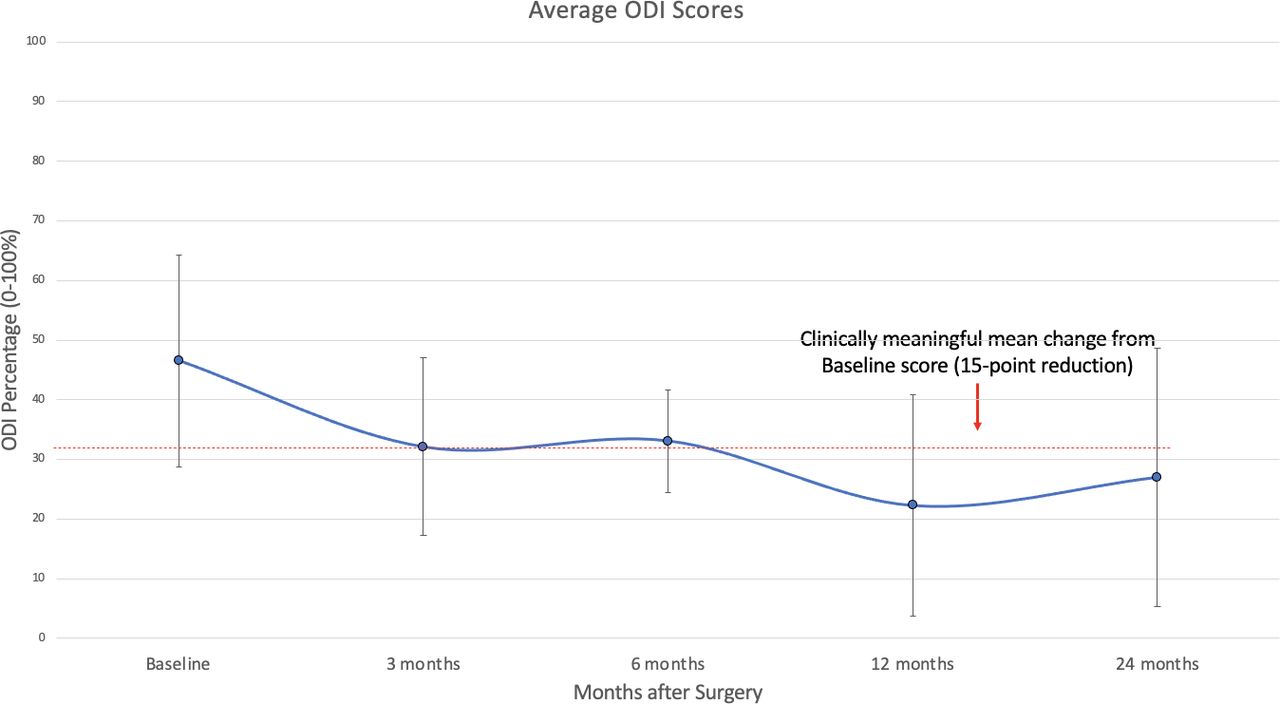
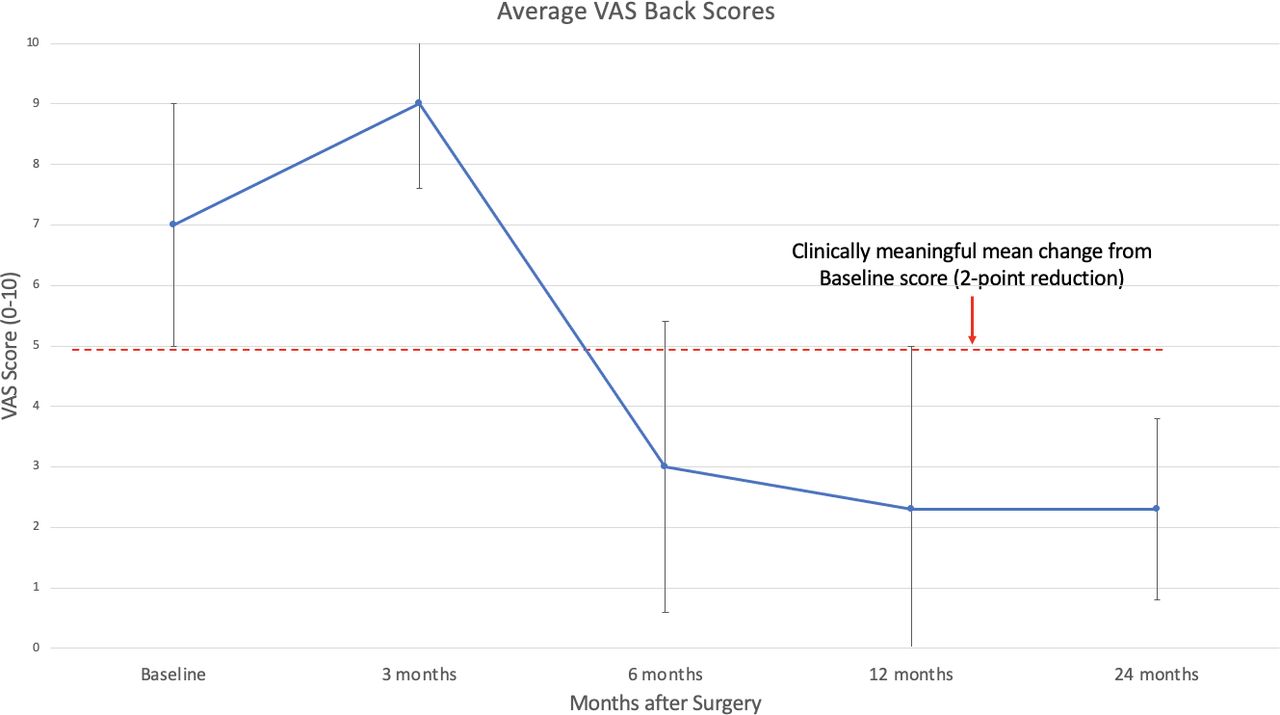
Average baseline ODI was 46.5% ± 17.8% indicating “severe disability” and improved postoperatively to 32.1% ± 14.9% and “moderate disability” at 3 months, 33.1% ± 8.6% and “moderate disability” at 6 months, 22.3% ± 18.5% and “moderate disability” at 12 months, and 27.0% ± 21.7% and “moderate disability” at 24 months. The 12- and 24-month ODI scores reached the clinically significant threshold of a 15-point decrease from baseline (Figure 7).19–21 The average VAS back score was 7.0 ± 2.0 at baseline and improved postoperatively to 3.0 ± 2.4 at 6 months, 2.3 ± 2.8 at 12 months, and 2.3 ± 1.5 at 24 months. The 12- and 24-month VAS back scores reached the clinically significant threshold of a 2-point decrease from baseline (Figure 8).19–21 Among patients who had both a recorded baseline and a 1- or 2-year reported VAS back score, 16.7% did not meet the minimal clinically important difference (MCID). Among the patients who had both a recorded baseline and a 1- or 2-year reported ODI score, 23.1% did not meet the MCID.
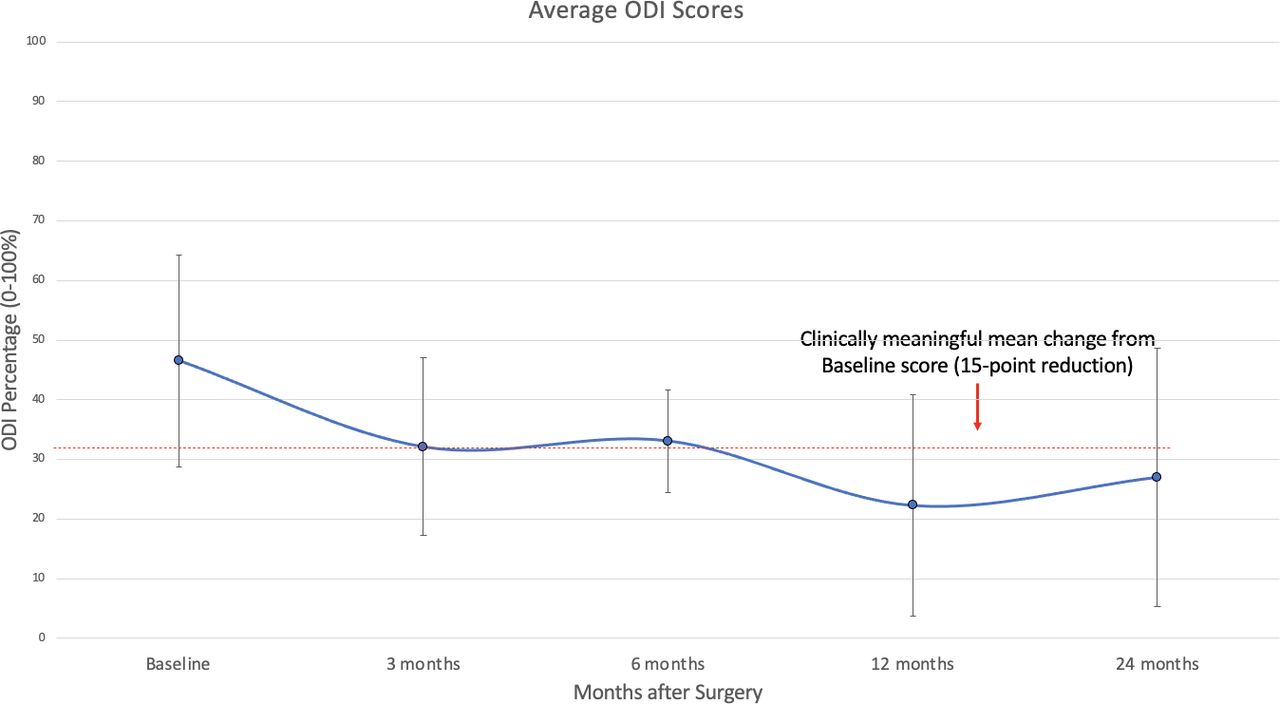
Patient-reported outcomes for the mean Oswestry Disability Index (ODI) through 24 months with the minimal clinically important difference shown (dotted line).

Patient-reported outcomes for the visual analog scale (VAS) back score through 24 months with the minimal clinically important difference shown (dotted line).
DISCUSSION
Here, we report the 24-month outcomes evaluating a novel variation of the percLIF using an expandable titanium cage placed through Kambin’s triangle without the need for facetectomy or endoscopy. Our results illustrate improved patient-reported outcomes (PROs) as well as high fusion rates, correction of radiographic variables, and the absence of device-related or surgical complications.
In prior open or minimally invasive transforaminal lumber interbody fusion (MIS-TLIF) surgery, a certain amount of facet removal for safe exposure and placement of the interbody cage was necessary, which disturbs this neurovascularly rich joint.22,23 To minimize concerns for both neuromuscular retraction and facetectomy, completely percutaneous techniques have now been expanded to include interbody fusion, leading to results comparable to MIS-TLIF. The estimated blood loss for a single-level MIS-TLIF has shown to be in the range of 150 to 350 mL, which is comparatively still much higher than our reported average estimated blood loss of only 70.3 mL for percLIF.24–26 Similarly, for length of stay, multiple studies have shown patients staying for up to an average of anywhere from 3.6 to 4.1 days in the hospital after single-level MIS-TLIF, while our study had a mean of around 3.4 nights with over 25% of patients being discharged on postoperative day 1.27–29 Huang et al described the clinical relevance of early discharges following lumbar fusions.30 They found that an early discharge within 3 days of admission could yield up to a 25% reduced risk of readmission for any cause within 6 months after surgery.
With regard to quality of life, previous reports on the expandable cage demonstrated good outcomes postoperatively at 12 months, but it remained uncertain how durable those functional improvements might be over a longer period.16 In this cohort, both short- and long-term ODI score improvements far exceeded the MCID of 12.8% to 14.3% as accepted in the current literature.19,31 At the 3-month mark, ODI scores decreased by 30.5%; at the 24-month mark, ODI scores had decreased by 41.9%. Of note, the average ODI score did not reach the “minimally disabled” threshold, which is between 0% and 20% ODI. However, given the definition and breakdown of the ODI score cutoffs, an ODI of 21% to 40% indicates that patients experience some pain and difficulty with sitting, lifting, and standing, but personal care, sexual activity, and sleeping are not grossly affected. An ODI of 41% to 60% indicates that pain remains the main problem in this group of patients where activities of daily living are affected.32 These definitions support the notion that although these patients on average did not become minimally disabled, there was a noticeable quality of life improvement compared with their baseline standing. Likewise, when reporting on the percentage of patients who did not reach the MCID, these values may also be skewed by the fact that some patients began at a lower baseline ODI compared with others. For example, a drop in percentage points from 25% to 15% may not meet the MCID of 15 points, but based on the reported cutoff ranges for the ODI scale in the literature, that could shift a patient from the “moderate” to “mildly disabled” category. Given the variability and subjective nature of these grading scales, it is important to note that the generalizability of these results is limited by our overall small cohort size. While still consistent with previous reports on minimally invasive interbody fusion, our results encourage more large-scale research related to PROs and their reliability for percLIF procedures.
The measured radiographic variables provide potential explanations for the improvement in pain scores. Zheng et al recently demonstrated that the degree of back pain after surgery showed a positive correlation with disc space height.33 In our cohort, both anterior and posterior disc space height showed significant increases (P < 0.001) at every follow-up time point. Likewise, multiple studies have linked a decreased PI-LL mismatch value to improved outcomes.34,35 Bourret et al found that the average PI-LL mismatch in an asymptomatic population was −5.4° ± 10.7°. Our cohort’s baseline PI-LL of 6.4° fell outside the confidence interval proposed by their study, but each subsequent PI-LL value fell within the range of the asymptomatic population, further supporting the improvement in functional outcome scores.35
Yet another important clinical aspect of spinopelvic parameters is its link with an increased risk for ASD.36–38 In our cohort, each of these variables was corrected significantly compared with their baseline measurements. The annual incidence rate of reoperation for ASD in our cohort was 2.74%, which is in agreement with some of the other reported rates in the literature looking at long-term follow-up data.39–42 Authors have reported the incidence of ASD in the lumbar spine to range from 3.9% to 14%, meaning our results fall on the lower end of the spectrum.43 Of note, some of these other studies have longer follow-up timeframes compared with ours.44
The literature is still scarce when it comes to determining fusion rates of completely percutaneous minimally invasive spine surgery compared with endoscopy or open approaches. Reported rates have ranged from 71.4% to 100% at the 1-year mark, but the long-term data are lacking.45,46 Our rates of 94.4% and 87.5% for the 1- and 2-year CT scans both fall within this previously reported range. Of note, 100% of patients with a 2-year follow-up radiograph showed no signs of either peri-implant lucency or breakage; thus, our numbers are likely an underestimate of overall fusion rates.
In terms of complications, only 3 patients (6.1%) required readmission. A recent review found complication rates ranged from 0% to 33.3% for MIS-TLIF.47,48 We hypothesize this difference in rates stems from the fact that MIS-TLIF still requires facet removal along with the use of an endoscope to visualize the disc space. Morgenstern et al also addressed this concern of the endoscope usage by publishing a study on full percutaneous interbody fusion using a facet-sparing, trans-Kambin approach, similar to the technique reported here.49 Interestingly, they reported a 32% complication rate consisting mainly of ipsilateral dysesthesias, but they also did not use triggered EMG neuromonitoring.50 Due to the lack of direct visualization in minimally invasive spine surgery, the authors strongly advocate for EMG usage to ensure no damage is done to the ENR during either the discectomy or placement of the interbody cage. Of note, Pairaiturkar et al cited in their radiographic analysis that only 2% of the more than 400 bony Kambin’s triangles in their study were able to accommodate a cannula diameter of greater than 8 mm, which is what our cannula’s dimensions were intraoperatively.51 However, they also reported that the rail-road technique of placing a tapered dilator followed by a snugly fitting cannula does not increase the frequency of ENR injury as previously thought in the literature.52,53 Additionally, the authors mentioned that ENR visualization was often difficult given that the nerve was not always a perfect oval shape. Without accurately visualizing the nerve root, truly measuring the maximum safe area of Kambin’s bony triangle is limited. For this reason, our group has begun experimenting with a more novel approach to the percLIF. By manually segmenting out the nerve roots prior to the measurement of Kambin’s triangle, the surgeon obtains a much clearer picture in 3D of how the ENR traverses over the corridor while also allowing for more patient-specific navigation into the disc space.54 Although this technique was not used for these surgeries due to its recent adoption, the importance of visualizing the ENR prior to operating is crucial for both determining the size of cannulas permissible and the appropriate laterality of approach.
While our study revealed multiple positive outcomes, percutaneous techniques still have limitations. Currently, the indications for percLIF are generally limited to patients with low-grade spondylolisthesis and degenerative disc disease. Due to the inability to perform a direct decompression with this technique, the main contraindications include patients with high-grade spondylolisthesis, facet cysts, large disc herniations, or advanced central stenosis. Additionally, although there have been incredible strides with recent advancements in 3D imaging, preoperative nerve segmentation, and MRI/CT fusion, there has yet to be a gold standard for designing a clear trajectory into the disc space.54–57 Consistent with the limitations of most retrospective studies, surgeons should also be cautious to make broad scale generalizations regarding the outcomes of this study. While the patients in this cohort did not have major surgical complications, it is important to recognize the ever-present risk of nerve root injury when performing these procedures. The small cohort size also poses limitations when interpreting the data. As mentioned previously, it would be beneficial for future studies to not only include more patients but also additional pain grading scales to further corroborate our findings and assess the interscale reliability of multiple PRO systems. Lastly, as this was a single-surgeon, single-institutional study, there may be differences in technique or patient selection within the inclusion and exclusion criteria that may have impacted the measured outcomes.
CONCLUSION
In our retrospective cohort, the percLIF with the insertion of an expandable titanium cage for the treatment of Grade 1 lumbar spondylolisthesis has proven to be an effective long-term treatment and does not require the use of an endoscope or facet joint removal. These patients had significant improvement in their spondylolisthesis, disc space height, spinopelvic parameters, VAS back, and ODI scores over 2 years.
Footnotes
Funding Grant funding was received from Spineology (Minneapolis, MN).
Declaration of Conflicting Interests Dr Abd-El-Barr is a consultant for Spineology, TrackX, and Depuy. Dr Shaffrey has financial relationships with NuVasive, Medtronic, SI Bone, and Proprio. Dr Wiggins is a strategic advisor for Qure.ai. Dr Chi discloses consulting fees from DePuy and K2M. The authors report that there are no other relevant disclosures pertaining to the content of this manuscript.
IRB Approval We received the appropriate IRB approval for this study (Pro00100250).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.