


Abstract
Background Anterior cervical discectomy and fusion (ACDF) for the surgical treatment of cervical degenerative disease often includes an intervertebral cage, which restores disc height and lordosis while promoting fusion . Cage materials include titanium (TTN) or polyetheretherketone (PEEK). Controversy in material selection stems from higher fusion rates with TNN, despite a higher subsidence rate, while PEEK cages demonstrate superior preservation of interspace height. Combining the advantages of both materials, TTN-coated PEEK (TCPEEK) cages were developed, featuring a PEEK core with similar stiffness to the bone, enveloped with a TTN coat, improving osteointegration. However, the potential superiority of TCPEEK over TTN cages has not been investigated. This study aimed to compare clinical and radiographic outcomes following single- or double-level ACDF using either TTN or TCPEEK cages.
Methods This retrospective single-center study included patients undergoing single- or double-level ACDF between 2017 and 2019. Clinical outcomes included the Neck Disability Index and revision surgery incidence. Radiographic parameters included cervical and segmental lordosis, C2 to C7 sagittal vertical axis, fusion, subsidence, and adjacent segment degeneration at a minimum 12-month follow-up.
Results A total of 45 patients (16 TTN; 29 TCPEEK) and 58 cervical levels (21 TTN; 37 TCPEEK) were included. Both cages significantly improved Neck Disability Index scores (TTN −10.0; TCPEEK −14.1) without significant differences. Two single-level TCPEEK patients required revision surgery due to non-union. In the radiological assessments, no significant difference was found for subsidence rates (TTN 52.4%; TCPEEK 56.8%), adjacent segment degeneration, cervical and segmental lordosis, and changes in C2 to C7 sagittal vertical axis. Though not statistically significant, fusion rates trended slightly higher with TTN (90.5%) vs TCPEEK cages (86.5%).
Conclusion TTN and TCPEEK cages achieve satisfactory clinical and radiological outcomes in single- or double-level ACDF. This finding suggests that the choice between them can be based on other factors, such as surgeon preference or availability, rather than specific material properties.
Clinical Relevance This study found that the selection of ACDF cage material did not affect clinical outcomes.
Level of Evidence 3.
Introduction
Anterior cervical discectomy and fusion (ACDF) integrates decompression with the insertion of an intervertebral spacer aiming to restore foraminal height and cervical lordosis while promoting fusion in patients suffering from cervical radiculopathy or myelopathy nonresponsive to conservative treatment. During the initial application of ACDF, a bone graft sourced from the iliac crest or bone bank was used to bridge the intervertebral space after extracting the cervical disc.1 However, these bony grafts showed several limitations, such as donor site morbidity, graft collapse, or subsidence, potentially leading to nonunion of the operated segment.2–4 Therefore, intervertebral devices or spacers evolved to replace these bone grafts, consisting of variable synthetic materials such as stainless steel, titanium (TTN), polymethyl-methacrylate, and polyetheretherketone (PEEK).5 These artificial cage designs aim to restore and maintain disc height and lordosis while potentially preventing graft collapse or resorption.
While all these materials strive to preserve the segment’s height and facilitate fusion, variations in their efficacy and the rate of adverse events, including subsidence, are described.5 TTN and PEEK emerged as superior options compared with polymethyl-methacrylate or autograft, showing lower rates of subsidence in ACDF.2,3,5
However, controversy arises when comparing TTN and PEEK. A study by Cabraja et al demonstrated a higher occurrence of solid interbody fusion for TTN when compared with PEEK cages (TTN 93.2% and PEEK 88.1%), albeit with a higher incidence of subsidence (TTN 20.5% and PEEK 14.3%).6 Conversely, Niu et al showed the superiority of PEEK cages to TTN cages in achieving radiographic fusion and preserving cervical interspace height.7
These differences are attributed to the specific biomechanical properties of each material. On the one hand, TTN exhibits favorable biocompatibility and corrosion resistance but possesses a higher stiffness (Young’s modulus: 110 GPa) compared with bone (cortical bone 17 GPa and cancellous bone 2.8 GPa), potentially leading to subsidence.2,3,5,8 On the other hand, its surface properties have demonstrated the ability to promote effective osteointegration.9,10 Whereas PEEK cages possess a stiffness (3–4 GPa) comparable to bone, they demonstrated weak osteointegration characterized by fibrous encapsulation associated with an inadequate bone union rate and a lack of significant improvements in interbody lordotic angle and interbody height.11–14
To combine the advantages of both materials, TTN-coated PEEK (TCPEEK) cages were developed, featuring a PEEK core with similar stiffness to bone, enveloped with a plasma-sprayed outer layer of TTN coat, adding its osteointegrative benefits.15 A prospective multicenter study by Nakanishi et al demonstrated the potential of TCPEEK cages for enhanced osteointegration with severe cage subsidence in only 3.2% of patients after 6 months.16 Despite these promising properties, in 1 comparative study, TCPEEK cages showed a significantly lower rate of fusion compared to PEEK cages (TCPEEK 44.1%; PEEK 88.2%) at 12 months postoperatively.17 However, to our knowledge, no study to date has directly compared the performance of TTN and TCPEEK cages in patients undergoing ACDF.
The aim of this retrospective study is to assess and compare clinical and radiographic outcomes after 1- or 2-level ACDF utilizing either TTN or TCPEEK cages.
Materials and Methods
The present study is a retrospective single-center study. Institutional approval was given by the ethical review board (BASEC-2022-00575).
Patients
Patients who underwent 1- or 2-level ACDF as a primary surgery from January 2017 until December 2019 with a minimal follow-up of 12 months were included. Excluded were patients with revision surgery, a different type of surgery than a stand-alone cage, missing radiological or clinical data, or a follow-up of less than 1 year. Parameters such as age, sex, smoker status, alcohol consumption, and disease requiring surgery were collected.
Two cohorts of patients were formed based on the implant material utilized, categorized as either the TTN group and the TCPEEK group. Since TCPEEK cages were introduced in March 2018 at the performing institution, all patients undergoing surgery prior to this date received TTN cages (Syncage-C, DePuy Synthes J&J, Zuchwil, Switzerland), whereas those operated as of March 2018 received TCPEEK cages (Mecta-C, Medacta International, Castel San Pietro, Switzerland or ACIS, DePuy Synthes, Oberdorf, Switzerland). No patient received a combination of both cages.
Surgery
All surgeries were performed at a single university spine center by board-certified spine surgeons possessing a minimum of 6 years of experience. A standard Smith-Robinson anterior cervical approach was performed with the patient in the supine position.18 Complete removal of the disc and posterior longitudinal ligament was conducted to decompress the nerve roots and the spinal cord. The endplates were prepared by gently removing the remaining cartilage. Afterward, the appropriate size of the cage was determined by the surgeon and guided by fluoroscopic imaging. After deciding on the implant size, the cage was filled with local autologous bone graft and demineralized bone matrix (DBX, DePuy Synthes J&J, Zuchwil, Switzerland) and inserted under light distraction with Caspar pins. The position was verified under fluoroscopy aiming for exact anteroposterior cage alignment within the intervertebral space.
Outcome Measures
All patients underwent preoperative, as well as 2-day, 6-month, and 12-month postoperative anteroposterior and lateral standing x-ray examinations of the cervical spine. Disc height and segmental lordosis measurements were conducted preoperatively and postoperatively for the operated level and both adjacent levels. Subsidence was quantified for each cage in millimeters on the final x-ray image by comparing it to the first postoperative x-ray image. A cage was defined as subsided if there was a difference of 1 mm or more.5 Fusion status was assessed by verification of a solid osseous connection between the involved vertebrae on the final x-ray image. Pre- and postoperative lordosis from C2 to C7 and C2 to C7 sagittal vertical axis (SVA) was determined as described by Martini et al.19 Adjacent segment degeneration (ASD) was recorded based on radiological findings. All radiological measurements were executed by a board-certified radiologist with 9 years of experience in musculoskeletal radiology.
Clinical outcome was assessed with the Neck Disability Index (NDI) both before surgery and at the latest follow-up appointment. Any instances of revision surgery were documented for all patients.
Statistical Analysis
Due to the non-normality of the data, nonparametric tests were used. Parameters are summarized with median, mean, and interquartile ranges or percentages as applicable. Continuous variables were compared between the groups using Wilcoxon signed rank or Mann-Whitney U tests. Frequencies were compared with Fisher’s exact tests. Associations between continuous variables were quantified with Spearman rank correlation tests. In the case of dichotomous predictors, point-biserial correlation tests were applied. P values below 0.05 were considered statistically significant. Statistical analysis was conducted with SPSS (version 27.0; IBM Corporation, Armonk, NY).
Results
A total of 45 patients (16 TTN patients; 29 TCPEEK patients) and 58 cervical levels (21 TTN levels; 37 TCPEEK levels) were included. Demographic data for the TTN and the TCPEEK group in terms of age, sex, alcohol, smoker status, and operated level were not significantly different and are displayed in Table 1. The mean follow-up was 2.4 years (1.0–3.9 years) after primary surgery. Out of the 58 levels, 32 were single-level surgeries (11 TTN; 21 TCPEEK), whereas 26 were part of a double-level surgery (10 TTN, 16 TCPEEK). The majority of patients underwent surgery for radiculopathy (either sensory or motoric) caused by degenerative disc disease (27 out of 45), followed by myelopathy (18 out of 45). In the TTN group, the indication for surgery was in half of the cases of myelopathy and radiculopathy caused by degenerative spinal stenosis (each 8 out of 16). In the TCPEEK group, the majority of indications were degenerative disc disease causing radiculopathy (10 out of 21) followed by myelopathy (11 out of 21).
Patient demographics and operative variables by implant type.
Radiological Outcome
The height of all operated segments increased significantly by 2.0 mm (0.8–3.3 mm; P < 0.001), as did cervical (2.2° [0.20°–5.2°]; P < 0.001) and segmental lordosis (1.0° [0.4°–2.1°]; P < 0.001). Conversely, a significant decrease in disc height occurred at the levels adjacent above (−0.1 mm [−0.3 to 0.0 mm]; P < 0.001) and below (−0.1 mm [−0.3 to 0.0 mm]; P < 0.001). The C2-C7 SVA also shifted significantly anterior with 2.8 mm (−2.1 to 7.7 mm; P = 0.018; Table 2).
Overall changes in radiographic parameters from pre- to postoperative.
The comparison of the radiologic parameters for the 2 cage types (TTN vs TCPEEK) yielded no significant difference in changes of cervical lordosis, segmental lordosis, C2-C7 SVA, and disc height of the operated levels as well as in the adjacent levels above and below. There was a significant difference in the preoperative disc height of the adjacent level above (TTN 4.8 mm, TCPEEK 3.9 mm; P = 0.04), and this remained significantly different postoperatively (TTN 4.5 mm, TCPEEK 3.7 mm; P = 0.03). However, the pre- to postoperative change was not statistically significant between both groups. All radiological measurements and changes are displayed in Table 3.
Radiographic parameters from pre- to postoperative by implant type.
Subsidence
The overall subsidence rate (>1 mm) of all operated levels was 55.2% (32 out of 58 levels). When looking at the cage groups individually, 52.4% (11 out of 21) of TTN and 56.8% (21 out of 37) of TCPEEK showed a subsidence greater than 1 mm not being significantly different, as shown in Table 4. Median subsidence was 1.25 mm (0.6–1.9 mm) with no difference between both cage types (TTN 1.3 mm; IQR 0.3; 2.3 mm; TCPEEK 1.2 mm; IQR 0.6; 1.7 mm).
Subsidence, fusion, and ASD compared between both cage groups.
Subsidence greater than 3 mm was seen in 5.2% of all operated levels (3 out of 58 levels). This refers to 4.8% of TTN cage levels (1 out of 21 levels) and 5.4% of TCPEEK cage levels (2 out of 37 levels). Of the 24 cages without subsidence, 87.5% (21 out of 24) showed radiographic fusion.
The amount of postoperative increase in the height of the operated level did not significantly affect the risk for subsidence (P = 0.15).
In smokers, subsidence was not significantly greater with a median of 1.5 mm (1.2–2.5 mm) compared with 1.2 mm (0.6–1.9 mm) in nonsmoking patients (P = 0.11). Still, the subsidence was similar for both cage types (TTN: 2.8 mm [1.5–2.9 mm]; TCPEEK: 1.25 mm [1.2–1.8 mm]; P = 0.07) in this group of patients.
Fusion
Fusion was radiologically confirmed in 87.9% (51 out of 58 levels) of all operated levels at mean follow-up. More specifically, the fusion rate for TTN was 90.5% (19 out of 21 levels) and 86.5% (32 out of 37 levels) for TCPEEK, but this difference was not statistically significant (P = 0.89).
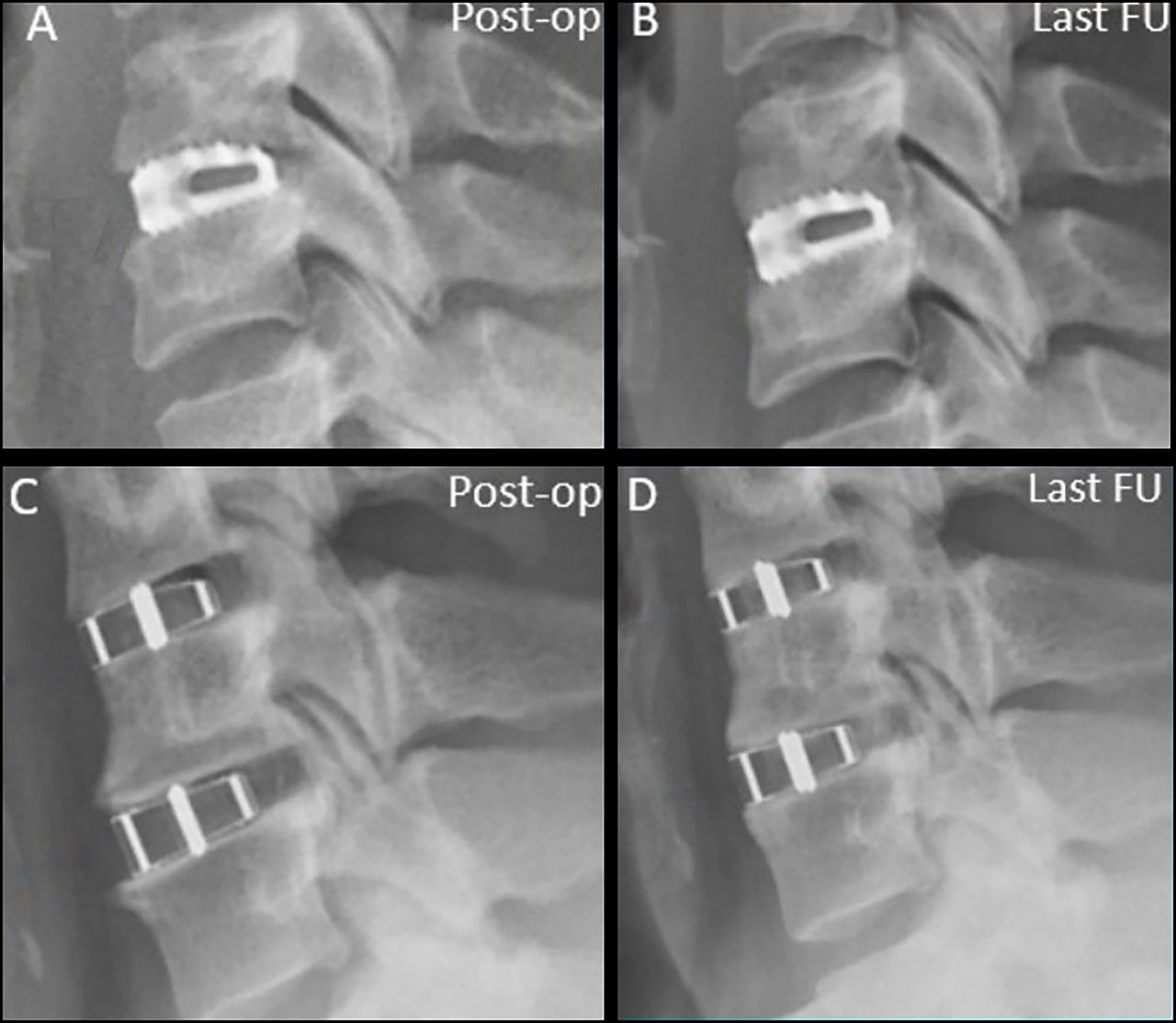
In patients who had undergone single-level ACDF, the overall fusion rate was 87.5% (28 out of 32 levels) with 81.1% (9 out of 11 levels) for TTN and 90.5% (19 out of 21 levels) for TCPEEK cages. The difference in fusion rate in single-level ACDF was not significant between cage types (P = 0.59). Representative images of postoperative fusion are shown in the Figure.

Immediate postoperative lateral x-ray image (A) depicts single-level surgery with a titanium cage. The same image at the last follow-up (B) shows slight subsidence; however, successful osseous fusion posterior to the cage is evident. The lateral x-ray image of a 2-level surgery with titanium-coated polyether-ether-ketone cages (C) also demonstrates successful osseous fusion at the last follow-up, both within and posterior to the cage (D). Abbreviation: FU, follow-up.
In patients who had undergone double-level ACDF, the overall fusion rate was 88.5% (23 out of 26 levels) with 100% (10 out of 10 levels) and 81.3% (13 out of 16 levels) for TTN and TCPEEK cages, respectively. The difference in fusion rate in double-level ACDF was not significant between cage types (P = 0.26).
Adjacent Segment Degeneration
There was no significant difference between the 2 cage types for the rate of radiological ASD (0% for TTN, 5.4% TCPEEK; P = 0.53).
Clinical Outcome
The improvement of the NDI was −14.8 points for all patients, with a change in NDI of −10.0 points for TTN and −14.1 points for TCPEEK (P = 0.37). No significant difference in the preoperative and postoperative median NDI was seen for the 2 different cage groups (Table 5). Two patients received revision surgery after single-level ACDF with a TCPEEK cage due to nonunion of the operated segment with persistent pain, therefore receiving a fusion with plate and a new TCPEEK cage. No patient with a TTN cage required revision surgery.
Pre- and postoperative NDI scores by cage type.
Correlation of Radiological Outcome to Clinical Outcome
Patients without fusion exhibited no less improvement in the NDI than those with confirmed fusion. The improvement for patients lacking fusion was a decrease of 14.0 points, while for those with fusion, it was a decrease of 12.0 points (P = 0.82).
There was no significant correlation between the level of subsidence and the variation in NDI (r = −0.015; P = 0.91). Similarly, alterations in cervical lordosis showed no significant association with NDI improvement (r = −0.145; P = 0.27). However, a moderate positive correlation was observed in the change of the C2 to C7 SVA (r = 0.259; P = 0.049).
Discussion
This retrospective comparative study analyzed the clinical and radiological outcomes for 2 different cage materials, TTN and TCPEEK, in single- or double-level ACDF. All patients experienced satisfactory clinical outcomes with each type of cage with an average improvement in the NDI of 14.8 points, surpassing the minimal clinically important difference threshold of 7.5 points.20 No differences in radiological outcomes such as subsidence, fusion, and ASD have been shown between the 2 cage types.
The radiological outcomes show a a significant improvement in the height of operated segments and segmental lordosis across all patients, without a substantial change in overall cervical lordosis postsurgery, which suggests that both TTN and TCPEEK cages are effective in restoring the alignment of the cervical spine. This is relevant because the loss of cervical lordosis has been considered a risk factor for the degeneration of the adjacent segments.21,22 However, the lack of significant differences between the 2 cage types in terms of changes in cervical lordosis, segmental lordosis, and C2-C7 SVA suggests that the choice of material is not critical for the radiological alignment outcomes of single- or double-level ACDF.
The fusion rates observed in this study highlight a nonsignificant trend toward better outcomes with TCPEEK cages compared with TTN for single- and double-level surgery. Although the difference was not statistically significant, the higher fusion rate shown with TTN (90.5%) cages suggests a potential material-related benefit that warrants further investigation, particularly in more complex surgeries involving multiple levels. Interestingly, in another study, complete fusion was noted significantly more often with PEEK implants than with TCPEEK implants in ACDF at 12 months postsurgery, which does not align with the biomechanical and histological concept of using TTN coating to enhance osseointegrative properties.15,17,23,24
Subsidence rates did not significantly differ between cage types, indicating that both materials are similarly susceptible to this complication. Subsidence of any extent was found in a slight majority of the levels operated, yet there was no significant difference observed between the TTN group, at 52.4%, and the TCPEEK group, at 56.8%. Therefore, the expected reduction in subsidence when using a TCPEEK cage, due to its lower elastic modulus, could not be demonstrated in our study. Regarding the clinical relevance of subsidence, we found no correlation to the postoperative clinical outcome, which is congruent with other findings for different cage materials.25,26
When looking at the current literature, some authors apply a threshold of 3 mm for defining subsidence. When adapting the subsidence to 3 mm or more to our study, the overall incidence of subsidence decreased to 5.2%. This rate is lower than the described rates in a systematic review where PEEK cages showed a 24.9% subsidence rate and TTN cages showed a 30.2% subsidence rate of at least 3 mm at the last follow-up.5 However, a broad variety of subsidence rates from 0% up to 83% can be found in the literature.27 This variability leads one to question the reliability of subsidence as a comparative parameter, potentially being influenced by several confounding factors such as variations in surgical methodologies, heterogeneity among patient cohorts across studies, and the potential misidentification of cages that have not fully fused—these may exhibit radiographic characteristics imitating subsidence, including anterior constriction of the intervertebral gap and perceived endplate proximity during the fusion process. Additionally, the accuracy of measurements needs to be challenged considering the manual assessment of millimetric changes on radiographic images. This rate may depend primarily on other factors than the cage material itself, such as the selection of cage height.28
The clinical outcomes, assessed with NDI, improved across the cohort without significant differences between the 2 cage groups. This improvement in NDI, regardless of fusion status or the degree of subsidence, suggests that the primary goal of ACDF—relieving symptoms and improving function—can be achieved with both TTN and TCPEEK cages. Notably, a moderate positive correlation between the change in C2 to C7 SVA and improvement in NDI points to the importance of sagittal balance in achieving favorable clinical outcomes matching previous findings in the literature.29
In alignment with our findings is a study comparing the efficacy of TTN and TCPEEK cages within the context of posterior lumbar interbody fusion, which identified no statistically significant differences in patient-reported quality of life as well as in cage subsidence and fusion rates at the 6-month and 1-year postoperative milestones.30
Limitations of our study include its retrospective design, lack of randomization, and small sample size, which may obscure minor differences in fusion rates that could emerge in a larger cohort. Despite the absence of systematic randomization, both groups underwent surgery using the same technique and by the same surgical team. Regarding radiological evaluation, the lack of postoperative computed tomography scans to corroborate our results is a notable limitation, potentially under- or overestimating the fusion rates of each material. Consequently, future research addressing these limitations will be needed.
Conclusion
This study demonstrates that both TTN and TCPEEK cages are effective in achieving the desired radiological and clinical outcomes in ACDF surgery. While certain radiological differences were noted, these did not translate into significant clinical distinctions between the 2 materials. The findings suggest that the choice between TTN and TCPEEK cages can be made based on other factors such as surgeon preference rather than specific material properties.
Footnotes
Funding No funding was received for the present study.
Disclosures Mazda Farshad has received research support from Medacta; consulting fees from Incremed, Zimmer Biomet, Medacta, and 25Segments; fellowship support from DePuy Synthes; and stock from Incremed (Balgrist Startup); and has private investments in Incremed (Balgrist Startup) and 25Segments (Balgrist Startup). The remaining authors have nothing to disclose.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.