


Abstract
Background Anterior lumbar interbody fusion (ALIF) is used to improve spinopelvic alignment, most commonly by increasing segmental lordosis (SL) at L5 to S1. Achieving certain radiographic parameters is critical for good patient outcomes. However, the relationships between pre- and postoperative SL and interbody dimensions are inexact and have not been well studied. This study investigated the relationships between postoperative SL at L5 to S1, ALIF cage angle, and preoperative radiographic measurements to improve the predictability of surgical radiographic outcomes after L5 to S1 ALIF.
Methods A single-center database was retrospectively reviewed for patients who underwent L5 to S1 ALIF from January 2017 to December 2022. Patients with posterior percutaneous instrumentation were included in the study, but patients with posterior decompression or facetectomies at L5 to S1 were excluded. Pre- and postoperative scoliosis films and patient surgical data were analyzed. A multilinear regression analysis was performed to create a predictive model of postoperative L5 to S1 SL.
Results This study evaluated 46 single-level L5 to S1 ALIFs. Using mixed-effects linear regression analysis, postoperative L5 to S1 SL can be predicted with statistical significance (P < 0.001) and power of 0.98 if the cage angle and preoperative L5 to S1 SL are known using the following formula: SLpost = 8.741 + (0.454 × C) + (0.595 × SLpre), where SLpost is postoperative L5 to S1 SL in degrees, C is cage angle in degrees, and SLpre is preoperative L5 to S1 SL in degrees.
Conclusions Cage angle and preoperative L5 to S1 SL were predictive of postoperative SL after L5 to S1 ALIF. The ability to predict postoperative radiographic values is critically important for good patient outcomes, and efforts should be made to develop more sophisticated mathematical models.
Introduction
Adequate restoration of lumbar sagittal balance after lumbar fusion has been shown to improve clinical outcomes.1–3 To accomplish this task, surgeons must rely on knowledge of the patient’s preoperative balance as well as the potential amount of achievable surgical correction. In minimally invasive spine surgery, surgeons rely on interbody cage dimensions, choosing cage lordosis and graft size, in part, to achieve the amount of segmental lordosis (SL) offered by the cage. This is critically important in the distal lumbar spine, where small changes in lordosis can have a great effect on overall sagittal balance.4 However, the amount of SL achieved rarely aligns with the value expected on the basis of the cage dimensions alone.5,6
Theoretically, small changes in lordosis at L5 to S1 should have a greater effect on overall sagittal balance than changes at more proximal levels because L5 to S1 is located at the base of the spine. The anterior lumbar interbody fusion (ALIF) procedure has become a workhorse of minimally invasive spine surgery and is most commonly used at this level.7 ALIF cages are offered in a number of dimensions, including hyperlordotic cages that purport to provide up to 30° of lordosis. However, without posterior column osteotomies, this degree of lordosis is unlikely to be achieved.5
In this study, we sought to understand the relationships between postoperative SL at L5 to S1, ALIF cage angle, and preoperative radiographic measurements in a select group of patients who have undergone L5 to S1 ALIF surgery.
Methods
We retrospectively identified all patients who underwent single-level L5 to S1 ALIF at our institution (St. Joseph’s Hospital and Medical Center, Phoenix, AZ) between January 2017 and December 2022. Patients with concurrent posterior percutaneous instrumentation were included. However, patients with posterior decompression or facetectomies at L5 to S1 were excluded from the study. Pre- and postoperative radiographs were collected and analyzed to compare spinopelvic alignment outcomes. For inclusion in the study, patients were required to have preoperative radiographs completed within 1 year before surgery and postoperative radiographs completed within 8 weeks after surgery. This study was approved by the institutional review board of St. Joseph’s Hospital and Medical Center in Phoenix, Arizona, and complied with the Health Insurance Portability and Accountability Act. This study was exempt from the requirement to obtain informed consent due to its retrospective nature.
Patient Clinical and Surgical Data
Patient clinical data, including age, sex, body mass index (defined as weight in kilograms divided by height in meters squared), patient comorbidities, history of prior thoracolumbar surgery, and surgical indication were collected. Each ALIF cage was categorized based on the lordotic angle as reported by the manufacturer (12°, 15°, 20°, 25°, and 30°). Categorization of the cage dimensions and cage material was also performed. Cage angles were selected based on the surgeon’s expertise and a thorough preoperative evaluation of patient-specific variables, with the primary goals of reestablishing lumbar lordosis, achieving optimal sagittal alignment, and facilitating indirect decompression. Different angles were used to specifically target the individual needs of each patient, with the aim of restoring disc height, maximizing endplate contact for enhanced fusion potential, and correcting spinal deformities such as spondylolisthesis. These tailored decisions are integral to optimizing postoperative outcomes, reducing complications, and promoting long-term spinal stability and patient functionality because these factors have been closely correlated with significant postoperative improvements.
Radiographic Data
Radiographic parameters were measured on upright standing scoliosis radiographs using the institutional picture archiving and communication system software. Two blinded readers collected each patient’s pre- and postoperative spinopelvic parameters, including pelvic tilt, pelvic incidence, sacral slope, and lumbar lordosis (here defined as the angle formed by the superior endplate of S1 and the superior endplate of L1). The difference between pelvic incidence and lumbar lordosis was measured to assess for mismatch between the patient’s pelvic morphology and lumbar curve. Other variables collected included T2 to T5 thoracic kyphosis, T5 to T12 thoracic kyphosis, and T1 pelvic angle (the angle between the line connecting the center of the T1 vertebral body and the femoral head axis and the line connecting the femoral head axis to the midpoint of the S1 superior endplate). Data on SL at each level of the lumbar spine were collected. The sagittal vertical axis is the distance between a vertical plumb line drawn from the center of the C7 vertebral body and a line drawn from that same point to the posterior superior sacral endplate. Global tilt is defined as the sum of the pelvic tilt and C7 vertical tilt minus 180°. Anterior disc height was defined as the distance between the inferior and superior endplates at the anterior vertebral body line. Posterior disc height was defined as the distance between the inferior and superior endplates at the posterior vertebral body line. Neuroforaminal height was defined as the distance between the pedicles of L5 and S1.
Statistical Analysis
Relationships between postoperative L5 to S1 SL, preoperative measurements, and cage angle were studied using Pearson correlation analysis followed by multiple regression analysis to identify independent correlates with the primary outcome of interest (prediction of postoperative L5–S1 SL; SigmaPlot v. 14 [Systat Software]). A type I error rate of P < 0.05 was considered significant. Postoperative L5 to S1 SL was treated as a dependent variable, and preoperative radiographic measurements and cage angles were treated as independent variables. Independent variables showing significant correlations (P < 0.05) with postoperative L5 to S1 SL during the initial univariate analysis (Pearson) were included in the subsequent multivariate analysis (multiple regression). Paired sample t tests were performed to compare pre- and postoperative radiographic data.
Mathematical Model Design for Postoperative L5 to S1 SL Prediction
The compiled retrospective data helped identify significant variables after correlation analysis. The exposed relationships with preoperative variables and postoperative L5 to S1 SL were used to create a mixed-effects linear regression analysis to evaluate the predictive powers of the independent variables. The resulting fixed effects delivered the mathematical model as a simple equation for L5 to S1 SL postoperative achievement with its respective statistical significance and power.
Mathematical Model Validation
To validate our mathematical model, we compared the patients in the formula derivation group with patients in an external validation group. The validation group consisted of patients who underwent single-level L5 to S1 ALIF within the same period and under the same clinical inclusion and exclusion criteria but without standing scoliosis radiographs. All patients in the validation group had completed pre- and postoperative lateral lumbar radiographs. Nonpaired t tests were used to compare the mean difference between predicted and actual measured postoperative L5 to S1 SL in the derivation and validation groups.8
Results
Patient Demographic and Surgical Data
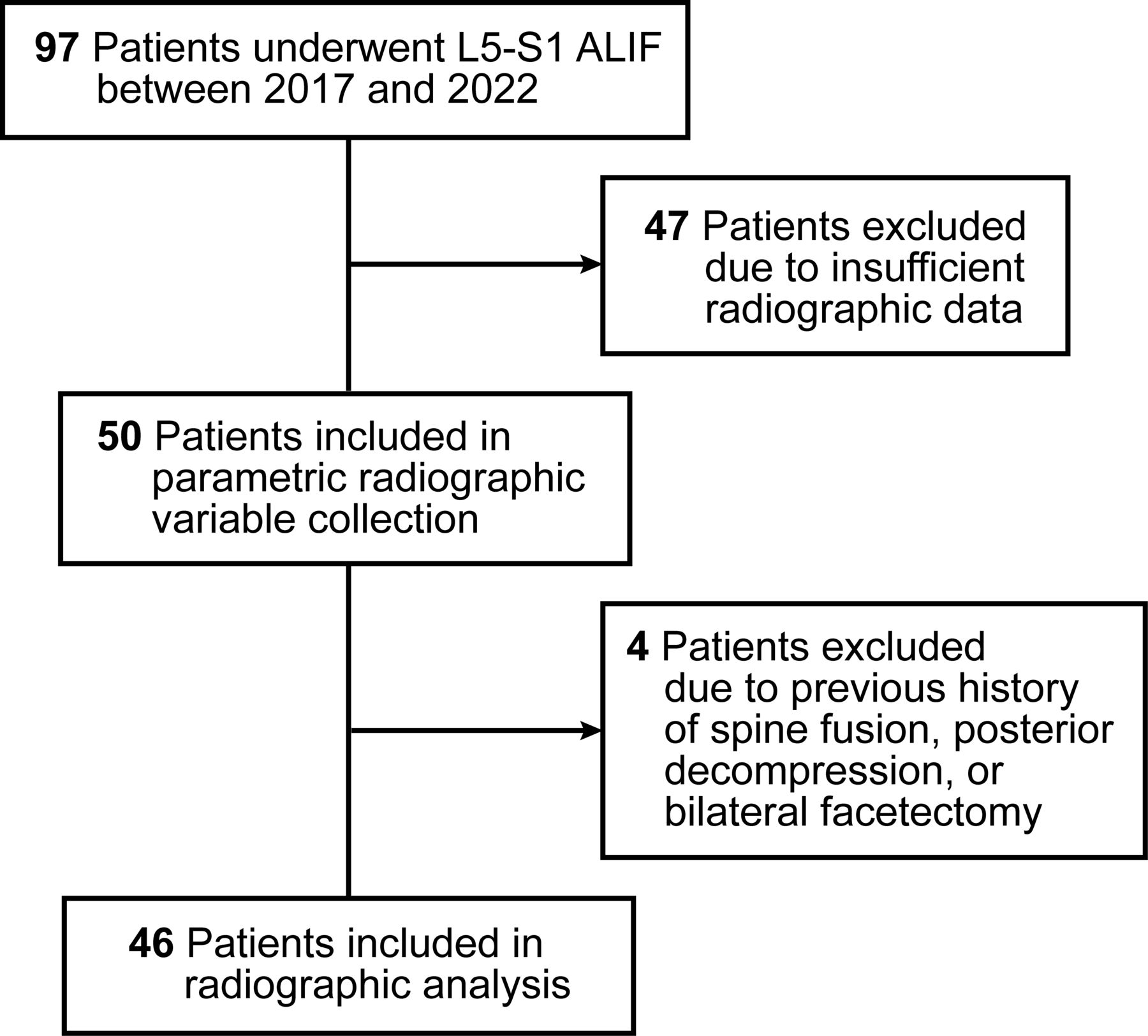
All single-level L5 to S1 ALIFs performed by a total of 3 experienced spine surgeons at our institution between 2017 and 2022 were retrospectively evaluated (n = 97; Figure 1). Forty-seven patients were excluded because of insufficient radiographic data. Four patients were excluded because of prior fusion and decompression at L5 to S1. Forty-six patients were included in the analysis, 22 (48%) of whom also underwent posterior pedicle screw instrumentation during the same surgery. Patient demographic data can be found in Table 1. The mean (SD) age of the patient population was 56.6 (13.5) years at the time of surgery. Of the 46 patients analyzed, 23 (50%) were women, and the mean (SD) body mass index was 28.3 (4.9). Thirteen patients had previous surgery at L5 to S1. These procedures included hemilaminotomy at L5 to S1 with (n = 9, 20%) or without (n = 4, 9%) microdiscectomy. None of the patients had a prior thoracolumbar fusion. Indications for ALIF surgery included spondylolisthesis (59%), spondylosis (98%), stenosis (96%), and spinal deformity (17%). Five patients (11%) had diabetes, and 3 patients (7%) were current smokers.

Patient flowchart showing inclusion and exclusion criteria. ALIF, anterior lumbar interbody fusion. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
Patient demographic and operative characteristics (N = 46).
The variables collected for the 46 ALIF cages included cage dimensions, materials, and angle (Table 2). Twenty-three (50%) of the cages were polyetheretherketone, and 23 (50%) of the cages were titanium. Cage angle was distributed as follows: 2 (4%) were 12° cages, 7 (15%) were 15° cages, 29 (63%) were 20° cages, 5 (11%) were 25° cages, and 3 (6.5%) were 30° cages. The mean (SD) width was 38 (5.25) mm, depth was 28 (4.6) mm, and height was 7 (4.1) mm.
ALIF cage dimensions and materials (N = 46).
Patient Radiographic Data
Patient pre- and postoperative radiographic data can be found in Table 3. All values are reported as a mean and SD. All preoperative standing scoliosis radiographs were obtained within 1 year before surgery. A comparison of pre- and postoperative radiographic data found that patients had an increase in mean L5 to S1 SL (19.6° vs 29.6°, P < 0.001). Patients also had compensatory decreases in L2 to L3 SL (6.7° vs 4.9°, P = 0.002), L3 to L4 SL (9.4° vs 7.1°, P < 0.001), and L4 to L5 SL (16.4° vs 14.4°, P = 0.002). A comparison of spinopelvic parameters found that pelvic tilt improved postoperatively (19.0° vs 17.7°, P = 0.04), as did lumbar lordosis (52.4° vs 54.8°, P = 0.03). There were also significant changes in anterior disc height (9.5 vs 19.7 mm, P < 0.001), posterior disc height (4.7 vs 7.7 mm, P < 0.001), and neuroforaminal height (12.2 vs 14.6 mm, P < 0.001).
Pre- and postoperative patient radiographic data.
Univariate and Multivariate Analyses
In our univariate analysis, we found statistically significant correlations between postoperative L5 to S1 SL and cage angle (r = 0.40, P = 0.009), sacral slope (r = 0.36, P = 0.02), lumbar lordosis (r = 0.38, P = 0.01), L4 to L5 SL (r = 0.42, P = 0.007), and preoperative L5 to S1 SL (r = 0.54, P < 0.001) (Table 4). These variables were subsequently included in our multivariate analysis (Table 5). The multivariate analysis showed that cage angle (P = 0.048), together with preoperative L5 to S1 SL (P = 0.01), was statistically significant in predicting postoperative L5 to S1 SL. A final multiple regression analysis showed that postoperative L5 to S1 SL can be predicted using the following equation with a statistical power of 0.98: SLpost = 8.741 + (0.454 × C) + (0.595 × SLpre), where SLpost is the postoperative L5 to S1 SL in degrees, C is the cage angle in degrees, and SLpre is the preoperative L5 to S1 SL in degrees.
Summary of r and P values from Pearson correlation analysis including postoperative L5 to S1 SL vs cage angle and preoperative radiographic variables.
Summary of coefficients and P values from multiple linear regression analysis including postoperative L5 to S1 SL and preoperative variables with significance during univariate analysis.
Mathematical Validation
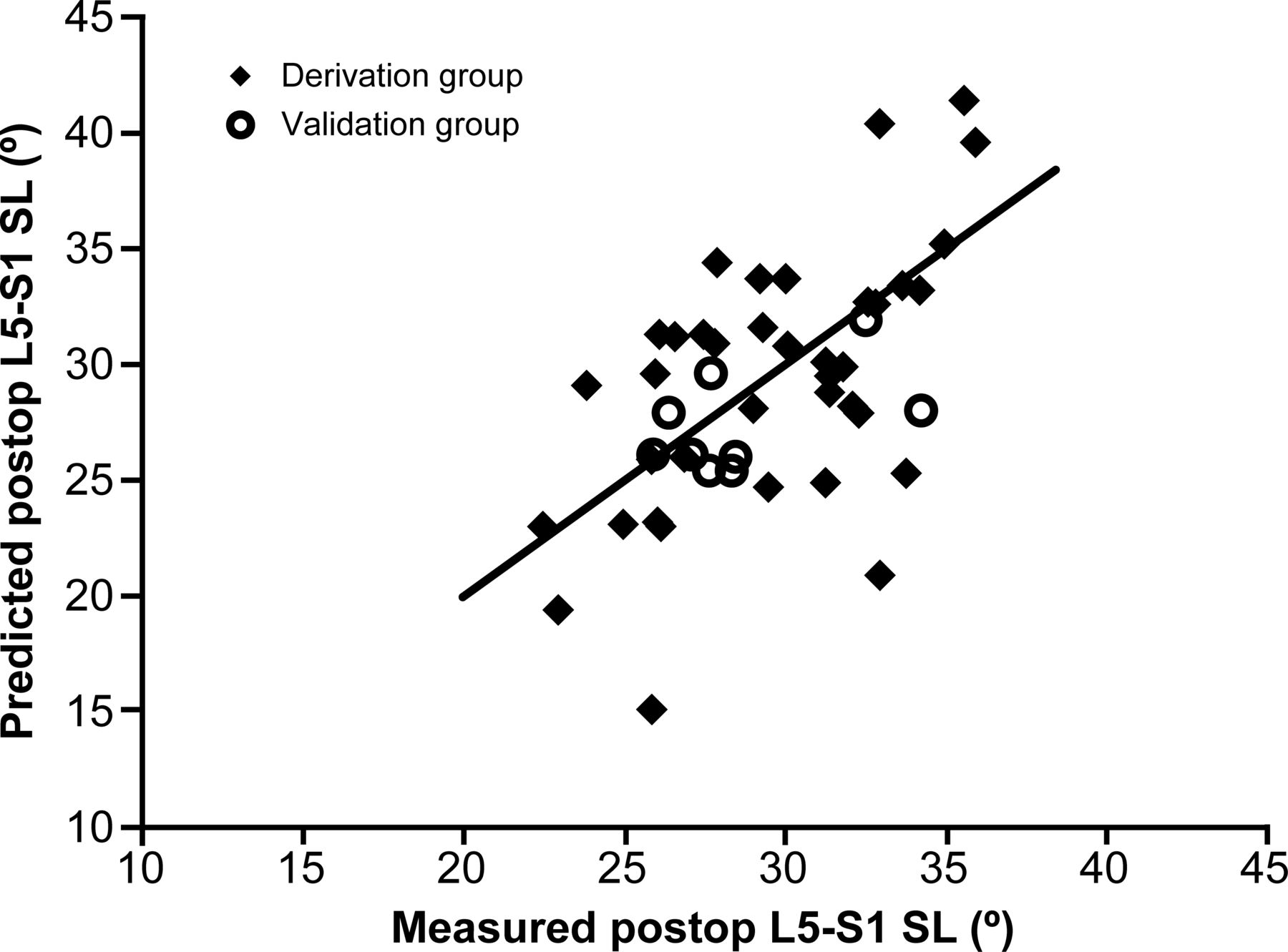
To validate the predictive formula, patients who originally did not meet inclusion criteria due to the lack of standing scoliosis radiographs but who had completed lumbar spine radiographs were identified. There were 9 patients who met these criteria and formed the validation group. Our predictive formula was applied to each patient in the derivation (n = 46) and validation (n = 9) groups. The mean (SD) differences between predicted vs measured postoperative L5 to S1 SL in the derivation group (0.01° [4.89°]) and the validation group (−1.33° [2.51°]) were compared using a nonpaired t test and found to not be significantly different (P = 0.44). These results are shown as a scatterplot in Figure 2.

Scatterplot of predicted vs measured postoperative (postoperative) L5 to S1 segmental lordosis (SL) in derivation (n = 46) and validation (n = 9) groups. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
Discussion
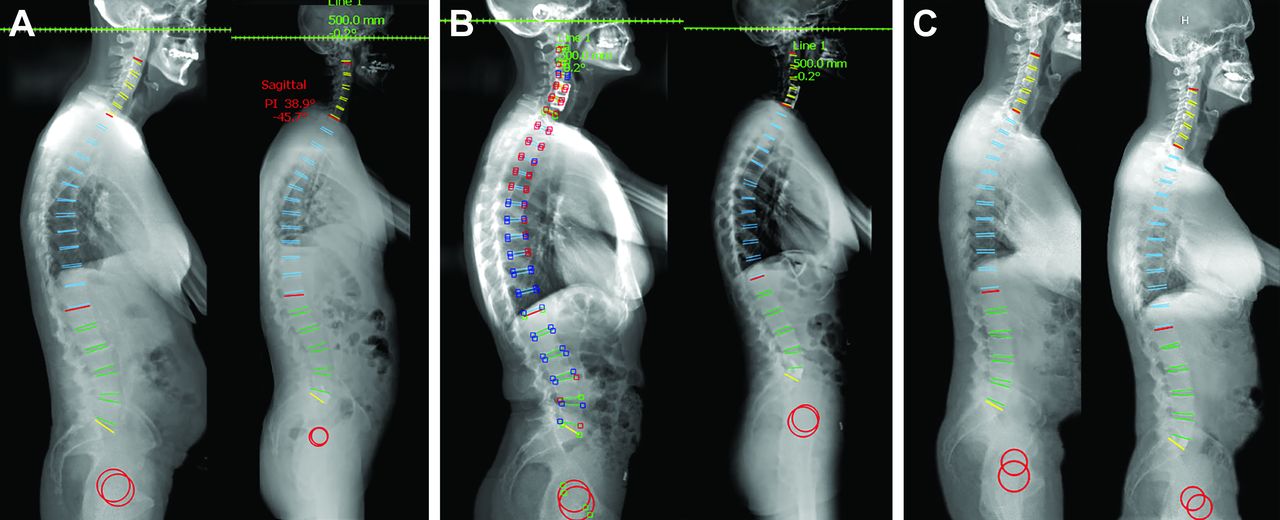
The achievement of spinopelvic and radiographic alignment goals is a critical step for patient improvement after spine surgery.9,10 The current literature suggests that achieving patient-individualized radiographic parameters improves spinal pathology and long-term outcomes.11,12 However, the ability to predict radiographic outcomes after spine surgery on the basis of preoperative radiographic data and surgeon-selected cage angle has not been previously described. Using data from this retrospective series of 46 patients who underwent L5 to S1 ALIF, we were able to find which variables are needed to accurately predict postoperative L5 to S1 SL using a simple linear equation.13,14 The mathematical model is simple to use, and given the same inclusion criteria, it can be used to predict postoperative SL within just a few degrees of actual postoperative measurements. Figure 3 illustrates case examples in which this formula is applied to patients in the derivation and validation groups.

Case examples demonstrating the use of the following formula for prediction of postoperative L5 to S1 SL: SLpost = 8.741 + (0.454 × C) + (0.595 × SLpre), where SLpost is the postoperative L5 to S1 SL in degrees, C is the cage angle in degrees, and SLpre is the preoperative L5 to S1 SL in degrees. Images were generated using Surgimap software (Nemaris, Inc., New York, NY), in which green indicates a value within the normative range, yellow indicates a measurement value just outside the normative range, and red indicates a measurement value far outside the normative range. (A) Case example from the derivation cohort. Preoperative (left) and postoperative (right) standing radiographs show a preoperative L5 to S1 SL of 23.9° and a postoperative L5 to S1 SL of 28.0°. Using the formula, postoperative L5 to S1 SL = 8.741 + (0.454 × 15°) + (0.595 × 23.9°), resulting in a predicted postoperative L5 to S1 SL of 29.7°. (B) Case example from the derivation cohort. Preoperative (left) and postoperative (right) standing radiographs show a preoperative L5 to S1 SL of 27.3° and a postoperative L5 to S1 SL of 37.2°. Using the formula, postoperative L5 to S1 SL = 8.741 + (0.454 × 20°) + (0.595 × 27.3°), resulting in a predicted postoperative L5 to S1 SL of 34.1°. (C) Case example from the validation cohort. Preoperative (left) and postoperative (right) standing radiographs show a preoperative L5 to S1 SL of 14.4° and a postoperative L5 to S1 SL of 27.9°. Using the formula, postoperative L5 to S1 SL = 8.741 + (0.454 × 20°) + (0.595 × 14.4°), resulting in a predicted postoperative L5 to S1 SL of 26.4°. SL, segmental lordosis. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
Many preoperative radiographic variables were analyzed with the goal of understanding which of these variables led to predictive relationships. We found that the combination of cage angle and preoperative L5 to S1 SL led to the most accurate prediction of postoperative SL, with a predictive power of 0.98. Although it is logical that cage angle and preoperative SL would be important factors in a resulting postoperative SL, this is, to our knowledge, the first study to quantify such a relationship. It is hoped that this model can be used as a mathematical tool to assist spine surgeons in choosing the best ALIF cage angle for L5 to S1, given a preoperative L5 to S1 SL and a desired postoperative SL. Our predictive model is based on multilinear regression analysis because of its ability to take into consideration multiple independent variables in the prediction of postoperative L5 to S1 SL.13,14 These study findings indicate that the lordosis achieved through ALIF is highly dependent on preoperative lumbar radiographic variables.
In this study, we also noted that there were significant compensatory changes at more proximal levels of the lumbar spine. As the SL at L5 to S1 increased, there were statistically significant decreases in the SL at adjacent levels. This is consistent with previous literature showing a correlation between greater ALIF cage angle and changes in adjacent segment SL.6,15 Although our current model does not predict changes at other levels, this is an avenue of study that should be explored to create better predictive tools for long-segment spinal deformity surgery, in which postoperative radiographic parameters are of utmost importance to patient outcomes.
As our understanding of how to predict postoperative radiographic outcomes improves, newer models should be integrated with automated and semiautomated radiographic tools. Current platforms are designed to facilitate preoperative planning, intraoperative guidance, and postoperative assessment in the context of spinal surgery. A commonly used example of this type of software system is Surgimap (Nemaris, Inc., New York, NY). Key features of these platforms include aiding in surgical simulation, image overlay, surgical navigation, and outcome assessment.16,17 However, the utility of similar software to predict outcomes would be greatly improved if trained on actual patient data.
Limitations
This study has several limitations. Its retrospective design may subject our findings to selection bias because not all patients who underwent single-level ALIF were included due to a lack of radiographic follow-up. Also, our model is only predictive of immediate postoperative results for patients within the demographic ranges listed in Table 1. Outcomes for patients outside these ranges and for cage selections made by other surgeons are unknown. In the future, more complex models may need to consider factors such as bone quality and the risk of subsidence to predict long-term radiographic outcomes. Our study also does not account for patients with facetectomies or posterior decompression, which would be an important next step for a more sophisticated modeling system. It should also be noted that each cage included in this study was selected by an experienced spine surgeon. It is unknown whether the relationships would remain significant if inappropriate cage angles were selected. Further research could investigate whether different cage angles lead to varying degrees of lumbar lordosis after surgery.
Conclusions
ALIF is an invaluable procedure for the restoration of L5 to S1 lordosis and achieving sagittal balance. In our analysis of 46 patients who underwent L5 to S1 ALIF, cage angle and preoperative L5 to S1 SL were used to approximate early postoperative L5 to S1 SL with high reliability using a simple mathematical equation. The ability to predict postoperative radiographic values is critically important to improving patient outcomes, and future efforts should be made to develop more sophisticated mathematical models to understand the relationship between cage dimensions and radiographic outcomes.
Acknowledgments
We thank the staff of Neuroscience Publications at Barrow Neurological Institute for assistance with manuscript preparation.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures J.S.U. receives royalties from NuVasive Medical, receives consulting fees and royalties from SI-BONE, and is a consultant for Aclarion, Misonix, Viseon, ATEC Spine, and Mainstay Medical. J.D.T. receives royalties, consulting fees, and research support from NuVasive Medical, Alphatec Spine, and SeaSpine and receives consulting fees and research support from SI-BONE. L.A.S. receives consulting fees from Globus, Depuy, Medtronic, and Aesculap. The other authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices described in this manuscript.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.