


Abstract
Background Lateral anterior lumbar interbody fusion (L-ALIF), or oblique lumbar interbody fusion at L5 to S1 (OLIF51), is a minimally invasive approach between the iliac vessels that provide indirect decompression, alignment restoration, and lordosis. While supine ALIF exposure has historically been performed by vascular surgeons, minimally invasive L-ALIF can be performed by spine surgeons familiar with lateral approaches. The L-ALIF is a relatively newer approach, and the objective of the present study was to assess the learning curve of the L-ALIF approach by comparing the pre- and postoperative radiographic measurements, patient-reported outcome measures (PROMs), and complications in a surgeon’s first 25 L-ALIF patients compared with the subsequent 25 L-ALIF patients.
Methods This retrospective case series includes the first 50 OLIF patients at/or including L5 to S1 by 1 surgeon. Demographics, complications, PROMs, and clinical and radiographic results were collected, and patients were analyzed comparing the surgeon’s first 1 to 25 patients (group A) and last 26 to 50 patients (B).
Results Demographic analysis demonstrated a mean age of 59.7 years and a body mass index of 28.7, and 52% of participants were women. The diagnosis was degenerative disc disease in 36 patients and deformity in 14 patients. Fourteen patients underwent single interbody level fusions at L5 to S1, 21 with 2 levels, and 15 with 3 to 6 levels. Segmental L5 to S1 lordosis increased 9.6° ± 3.9°, final mean lordosis 25.3° ± 8.3°; L5 to S1 disc angle increased 11.5° ± 4.9°, final disc angle 19.7° ± 3.8°; posterior disc height increased 3.6 mm ± 2.1 mm with final mean disc height 7.6 mm ± 1.8 mm. PROMs postoperatively were significantly improved from preoperatively. There were no significant differences in operative times for degenerative 1- or 2-level single-position surgery operations between groups A and B. Two group A patients had incisional hernias requiring repair, and 2 group B patients had postoperative ileus. There were no approach-related injuries.
Conclusion With proper patient selection and meticulous technique, the minimally invasive L-ALIF at L5 to S1 can be performed by surgeons experienced with lateral approaches to other spine levels. This study provides level 4 evidence and low-quality evidence in the Grading of Recommendations Assessment, Development, and Evaluation framework.
Clinical Relevance The lateral ALIF is a safe and effective approach at L5 to S1 for spine surgeons and provides good clinical, biomechanical, and radiographic outcomes, especially for those who do not have access surgeons available. Close attention to left common iliac vein anatomy is paramount for this type of approach and similar to other approaches. With increased repetition and numbers of cases, surgeons are able to improve in their technique.
Level of Evidence 4.
Introduction
For patients with degenerative lumbar disease, surgical management is the mainstay of treatment when conservative measures fail. For patients who require interbody fusion at the L5 to S1 level, anterior or oblique approaches may be advantageous over posterior or posterolateral approaches owing to increased size of interbody graft, increased potential lumbar lordosis, and reduced risk of adjacent segment disease.1
Although anterior lumbar interbody fusion (ALIF) has many advantages over posterior approaches, a major consideration in this surgical approach is the need for an access surgeon. Anterior approaches to the lumbar spine are conventionally performed with the assistance of a vascular or general surgeon2 to mitigate the risk of injury to the bowel, ureter, or vasculature. However, access surgeons often perform these in the supine position,2 which limits the possibilities of single-position surgery or requires patient repositioning if lateral interbody fusion is planned for other levels. Previous studies have shown that anterior approaches to the lumbar spine including lateral ALIF can safely be performed by spine surgeons with no increased risk of complications compared with when performed by access surgeons.3 Of note, the lateral ALIF approach has also been referred to as oblique lumbar interbody fusion at L5 to S1 (OLIF51; a trademark of Medtronic, Minneapolis, MN), although it remains a distinct procedure between the great vessels compared with the oblique lumbar interbody fusion approach for levels above L5.
In the current study, we report a series of patients who underwent lateral ALIF at L5 to S1 with access by a spine surgeon and describe the technical nuances and changes made over time to better understand the role of this approach without an access surgeon.
Methods
Clinical Data
This is a retrospective single-center series of 50 consecutive patients who underwent a minimally invasive L5 to S1 lateral ALIF (OLIF51) surgery performed by a single attending spine surgeon (M.H.P.) without an access vascular or general co-surgeon at an academic medical center. All patients presented either with diagnoses of degenerative disc disease or spinal deformity and had been treated without success with conservative measures before being considered for surgical intervention. Patients were also analyzed based on the surgeon’s first 1 to 25 patients (group A) and last 26 to 50 patients (group B). This research was approved by the medical center’s institutional review board, the patients consented to the procedure, and the participants and any identifiable individuals consented to the publication of his or her image.
Surgical Technique
This surgical approach has been described previously and was performed in a similar fashion.4,5 Patients are placed on a flat top Jackson table in right lateral decubitus with left side up in all cases. The left leg is kept straight with the left hip extended to ensure appropriate working space near the groin crease. The L5 to S1 disc space is marked out with fluoroscopy or navigated assistance, and a 5 to 7 cm oblique incision is marked out halfway between the anterior superior iliac spine and lateral rectus sheath. A muscle relaxant is given, and a muscle-splitting approach is performed down to the retroperitoneal space. The retroperitoneal fat, along with the peritoneal contents, is then gently mobilized anteriorly using serial retractor blades, with the understanding that the ipsilateral ureter is present along this plane. The psoas muscle is identified as the first landmark, and the left common iliac artery and left common iliac vein (LCIV) are identified just medial to the muscle. These are protected with an up-side LCIV retractor blade, while the down-side sacral blade is docked on the undersurface of the contralateral anterior surface of the sacral promontory (Figure 1).

(A) View of pertinent anatomy during the initial stages of the lateral anterior lumbar interbody fusion approach with noted psoas muscle, left common iliac artery, and left common iliac vein. (B) Further medial dissection will reveal the anterior annulus of the L5 to S1 disc space.
The disc space is confirmed on imaging at this point and bluntly dissected down until the annular fibers are seen to confirm that there are no peritoneal or retroperitoneal structures draped across the disc space. The middle sacral vessels are ligated through bipolar electrocautery or the use of large endoclip appliers. Disc space preparation is then carried out in the usual fashion similar to an L5 to S1 ALIF approach with specialized instruments capable of maneuvering down a minimally invasive lateral corridor. An appropriately sized ALIF-style cage is chosen based on preoperative measurements and the disc corridor, filled with bone graft, and inserted in as close to an anterior-to-posterior direction as the incision will allow with either a straight or oblique-angled inserter. Great care is always taken to ensure the LCIV is still protected during these maneuvers. After imaging confirmation of appropriate cage placement, closure of the abdominal fascia, dermis, and skin proceeds in the usual fashion.
Clinical and Radiological Evaluation
Data collected for analysis included age, sex, preoperative diagnosis, body mass index, number of total interbody levels, operating time (operative incision to closure time and in-room time), estimated blood loss, and clinical and radiographic results after surgery. The latest preoperative upright standing radiographs and 6-month postoperative radiographs (3-month films were used for cases without 6-month films) were analyzed for radiographic values. Patient-reported outcome measures (PROMs) were also collected on patients who filled out pre- and postoperative questionnaires utilizing the Oswestry Disability Index and Numerical Rating Scale (NRS) Back and Leg surveys, with a minimum postoperative survey of at least 3 months. Perioperative complications specific to the L5 to S1 lateral approach as well as reoperations for any reason were also recorded.
Statistical Analysis
The L5 to S1 lordosis delta, final lordosis, L5 to S1 disc angle delta, final disc angle, disc height delta, and final disc height were recorded for all 50 cases. The first 25 cases were compared with the second 25 cases using R version 4.2.1 statistical analysis software. Two-tailed t tests were used for all comparisons, with P values < 0.05 considered significant. All hypotheses were considered independent, and no corrections for multiple comparisons were performed.
Results
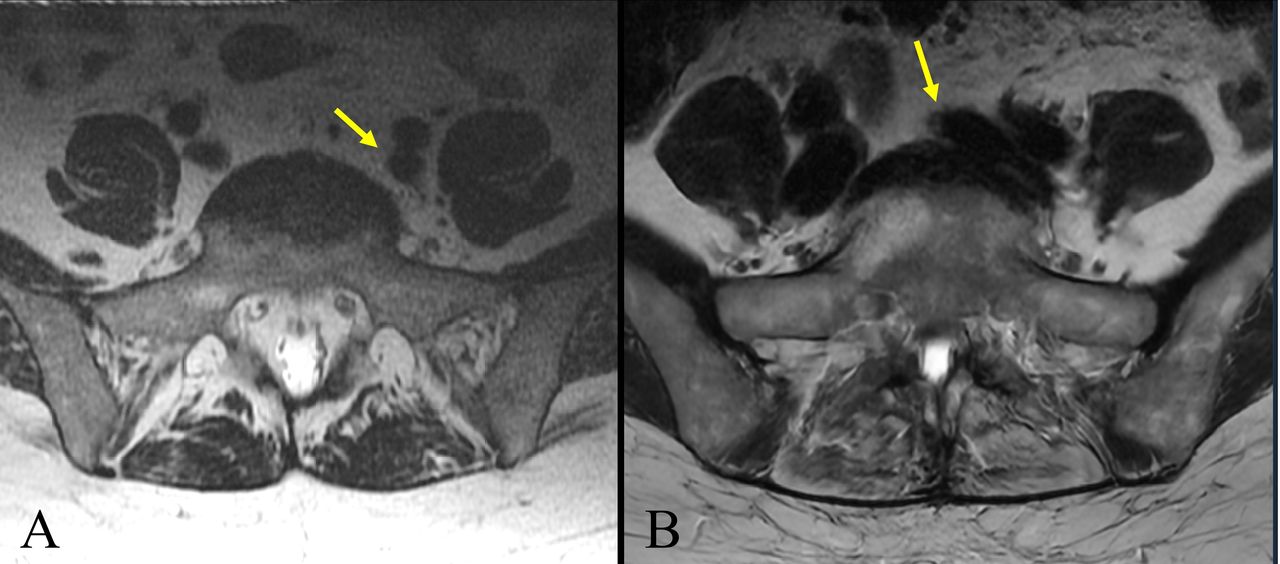
A total of 50 patients (26 women) underwent surgical intervention, which included a minimally invasive lateral ALIF approach to L5 to S1 (Table 1). Mean age was 59.7 (range, 28–80) years with a mean body mass index of 28.7 (range, 18.2–42.6) years over an average follow-up of 17.6 (range, 3.3–46.0) months. Patient selection excluded any prior history of diverticulitis, hernia repair with mesh, abdominal or pelvic cancers, radiation to the abdomen or pelvis, or a low great vessel bifurcation classified as an LCIV type 3.6 Preoperative vessel anatomy was reviewed on magnetic resonance imaging in all cases; all patients in group A had LCIV type 1 anatomy, whereas 20 of 25 patients in group B were LCIV type 1, and the remaining 5 were LCIV type 2 (Figure 2).

(A) Left common iliac vein (LCIV) type 1 of a patient in group A showing wide bifurcation of the iliac veins with the yellow arrow noting lateralization of the LCIV with a generous fat plane. (B) LCIV type 2 of a patient in group B with the yellow arrow showing medialization of the LCIV and a thin fat plane with anticipation of further dissection required for an appropriate anterior corridor in anterior lumbar interbody fusion.
Summary of baseline characteristics.
Surgeries were performed to treat degenerative disease (36 patients) or adult spinal deformity (14 patients), with no surgeries for any primary diagnoses of tumor, trauma, or infection. Fourteen patients underwent single interbody level fusions at L5 to S1, 21 patients at 2 interbody levels, and 15 patients at 3 to 6 interbody levels (Figure 3).

Anteroposterior and lateral lumbar x-ray images of patients who underwent single-position surgeries at (A) 1 level with L5 to S1 and (B) 2 levels with L4 to S1.
All but 2 patients with degenerative disease were performed as simultaneous single-position surgeries (SPS) with pedicle screws placed using robot assistance in lateral decubitus7,8; 1 patient underwent a standalone lateral L5 to S1 ALIF, while another patient underwent removal of a prior L5 to S1 TLIF cage and placement of a lateral L5 to S1 ALIF cage only. Surgeries for adult spinal deformity were part of a same-day or 2-day staged process with the patient subsequently repositioned to prone for the posterior instrumentation. Mean pre- and postoperative radiographic parameters are provided in Table 2.
Mean pre- and postoperative radiographic values.
Segmental L5 to S1 lordosis increased by 9.6° ± 3.9° with a final mean lordosis of 25.3° ± 8.3°; L5 to S1 disc angle increased by 11.5° ± 4.9° with a final mean disc angle of 19.7° ± 3.8°; posterior disc height increased by 3.6 mm ± 2.1 mm with a final mean disc height of 7.6 mm ± 1.8 mm (Figure 4).

Box and whisker plots showing overall improvements in L5 to S1 segmental lordosis and disc angle after lateral anterior lumbar interbody fusion (minimum, maximum, first quartile, third quartile, median, and mean).
When stratified by groups A and B, there were no significant differences found in the improvement of segmental L5 to S1 lordosis (9.6° vs 9.6°) or disc angle (11.2° vs 11.9°), but there was a significant difference between disc height improvement (2.9 mm vs 4.3 mm, P < 0.03).
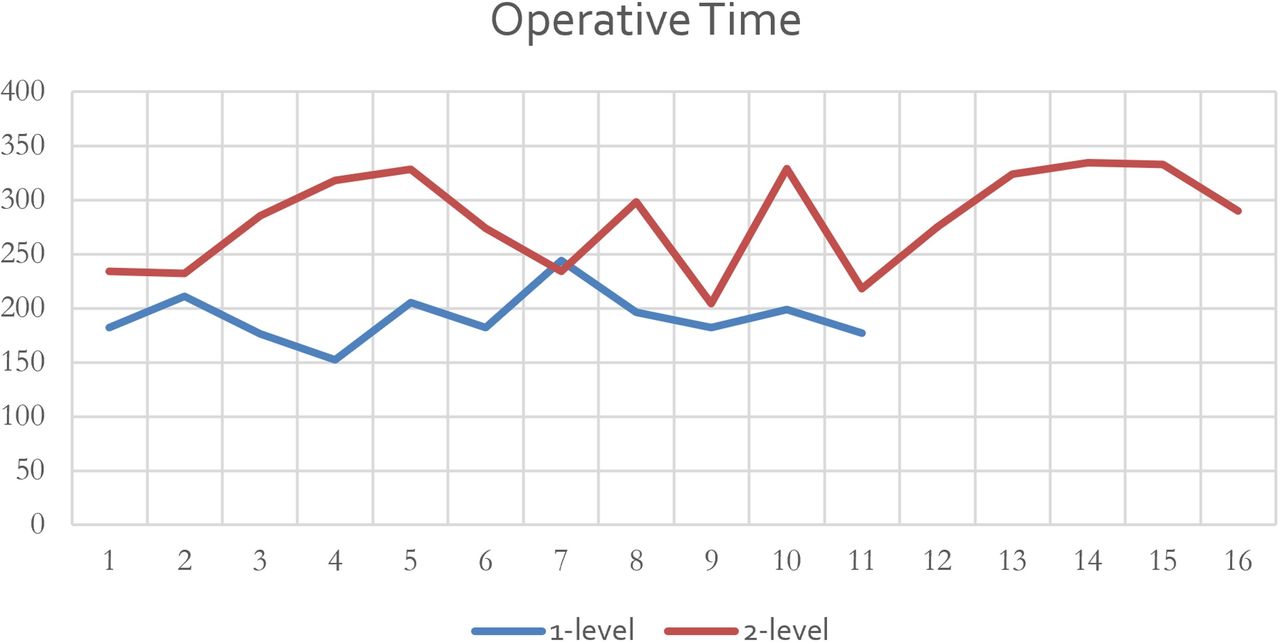
There were no significant differences in operative times for degenerative 1- or 2-level SPS operations between groups A and B (3 h 14 m vs 3 h 6 m and 4 h 39 m vs 4 h 43 m, respectively), in-room times (4 h 39 m vs 4 h 43 min and 6 h 3 m vs 5 h 57 m), or estimated blood loss (54 cc vs 63 cc and 81 cc vs 88 cc; Figure 5).

Operative incision-to-closure minutes of 1- and 2-level single-position surgeries that involved concurrent placement of posterior pedicle screws in lateral decubitus position with robotic assistance.
When comparing results from the first 25 cases to the last 25 cases, in addition to improvement in the median disc height delta, there was also correspondingly a statistically significant increase in the final disc height, which grew from a median of 6.7 mm to 8.1 mm (P < 0.03). All other parameters were not statistically changed (all other P > 0.10).
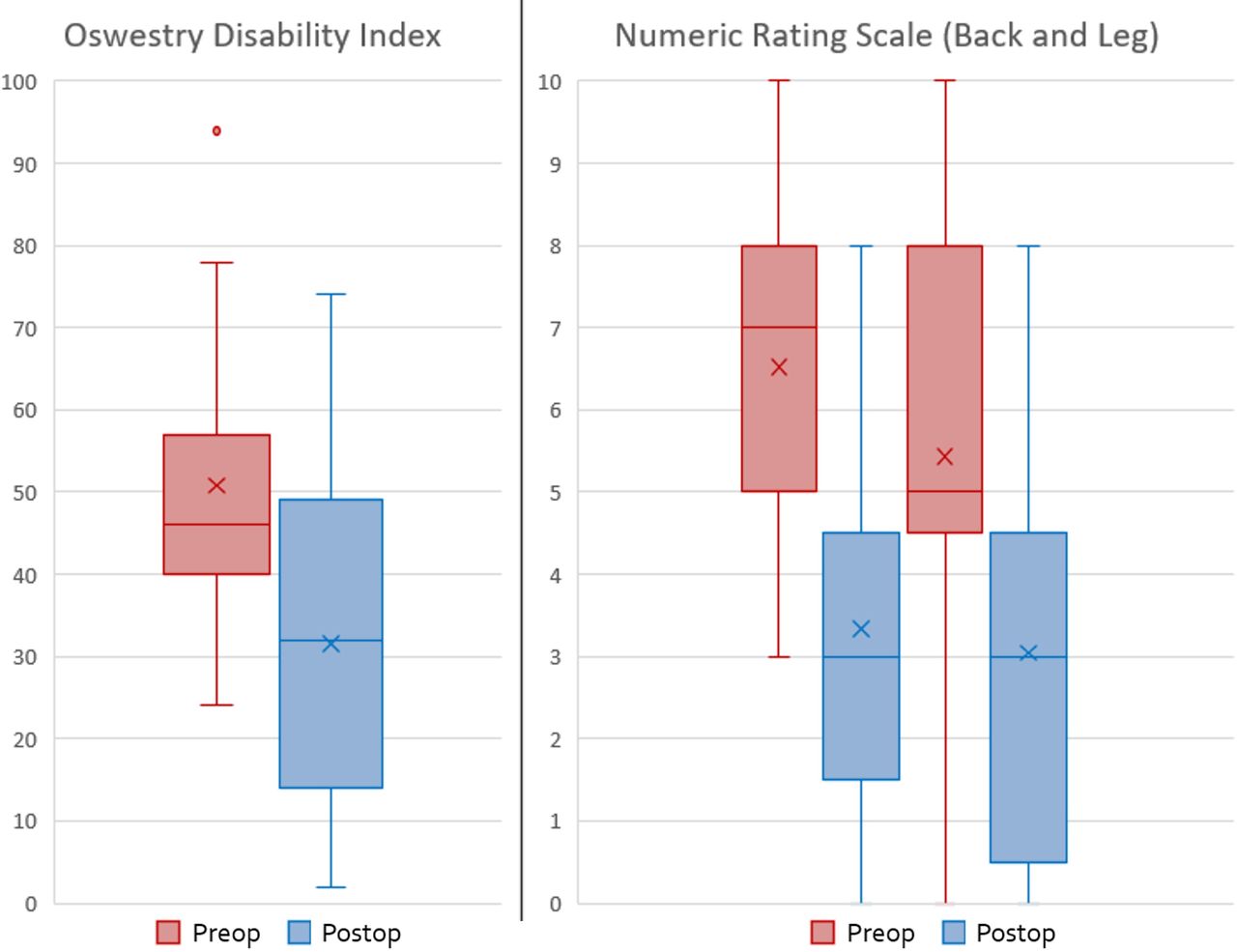
PROM data were available for 21 patients with a minimum postoperative 3-month survey (Table 3). The average postoperative survey follow-up was 6.6 months (range 3–12). Mean Oswestry Disability Index improved from 50.8 ± 16.4 (range 24–94) to 31.5 ± 19.9 (range 2–74), mean NRS back scores improved from 6.5 ± 2 (range 3–10) to 3.3 ± 2.2 (range 0–8), and mean NRS leg scores improved from 5.4 ± 2.8 (range 0–10) to 3.0 ± 2.5 (range 0–8; Figure 6). There was a statistically significant improvement in all PROMs pre- to postoperatively across the whole patient cohort. However, when comparing the improvement in PROM scores between groups A and B, there was no statistically significant difference seen in any of the 3 PROMs.

Box and whisker plots showing overall improvements in Oswestry Disability Index, numerical rating scale (NRS) back, and NRS leg scores after lateral anterior lumbar interbody fusion (minimum, maximum first quartile, third quartile, median, and mean).
Mean pre- and postoperative patient-reported outcome measures.
Two incisional hernias requiring repair occurred in group A and none in group B. None developed postoperative ileus in group B, and 2 developed the complication in group A. There were a total of 4 reoperations in the follow-up period: 2 patients experienced proximal junctional kyphosis above their adult spinal deformity correction requiring extension, 1 patient sustained a fall down the stairs that resulted in a sacral insufficiency fracture requiring distal extension, and 1 patient experienced persistent S1 radiculopathy that resolved after a posterior L5 to S1 facetectomy. Two instances of asymptomatic pseudarthrosis were observed in degenerative patients. There were no approach-related neurologic, vascular, gastrointestinal, or urologic injuries, and no intraoperative blood transfusions were needed. There were no instances where an on-call vascular or general surgeon was needed for an intra- or postoperative consultation.
Discussion
Lateral ALIF, also known as OLIF51, is a minimally invasive approach between the iliac vessels that provides a powerful option for indirect decompression, restoration of alignment, and lordosis.4,5,9 While supine ALIF exposure has historically been performed by vascular surgeons, minimally invasive lateral ALIF exposure has increasingly become a technique performed by spine surgeons familiar with lateral interbody approaches at other levels. An approach to the lumbosacral junction at the L5 to S1 level necessitates an anterior or anterolateral oblique approach between the great vessels. While this may be less familiar to spine surgeons in general, this space is contiguous in the retroperitoneum proximally, and surgeons with significant experience in thoracic, thoracolumbar, and lumbar lateral access surgery will still find similarities to the technical considerations around the unique anatomy of this space.
This study looks to build upon prior work on the successful supine anterior exposure of the lumbar spine by spine surgeons. Smith et al demonstrated that a spine surgeon could successfully and safely perform an anterior exposure to the spine without the aid of an access surgeon as they demonstrated that the group with a spine surgeon alone had statistically significantly less estimated blood loss, operative time, hospital stay, and complications.10 Quraishi et al also published a 304 consecutive patient anterior lumbar spinal surgery cohort over 10 years demonstrating similar complication rates, most common of which was vascular in nature (7.8.%), to other studies’ reported complication rates for anterior lumbar spinal surgery when using a general or vascular access surgeon.11 Lindado’s group in Colombia also showed similar complication rates in supine ALIF procedures without access to surgeon assistance.12 Furthermore, the systematic review and meta-analysis by Phan et al that looked at more than 50 studies published on anterior spine surgery with and without an access surgeon demonstrated mixed data.13 The use of an access surgeon is associated with overall similar intraoperative complication rates but higher rates of arterial injuries, retrograde ejaculation, and ileus and reduced rates of peritoneal injuries, neurological injuries, and reoperation.13 The explanation given for the higher rates of arterial injuries, retrograde ejaculation, and ileus in the access surgeon group was that those surgeries often were biased toward multilevel, more complex surgical exposures that would necessitate or favor the use of an access surgeon.
As a learning curve study, we first sought to determine whether there were improvements in operative times with increasing case numbers. For degenerative single-position lateral 1- and 2-level cases, we did not find any improvements in operative time or in-room time—including equipment setup—when trending cases. This may reflect that the lateral ALIF exposure is expected to take a fairly standard amount of time at the start of an SPS case, without hindering other portions of the single-position workflow. These include concurrent robot-assisted placement of screws, confirmation fluoroscopy or CT, tubular decompressions with minimally invasive laminectomies or facetectomies while in lateral position in some patients, and subsequent placement of rods and closure. However, over time, we did see an increasing number of cases attempted with more challenging LCIV anatomy (LCIV type 2) that would potentially require more dissection to create an anterior ALIF corridor. Other studies have shown that over the course of more than 200 combined oblique and lateral lumbar interbody fusion cases performed without an access surgeon, operative times did decrease without changes in complications,14,15 and our series with only 50 patients may not yet be large enough to capture similar improvements in the future.
As expected in the placement of an ALIF cage at L5 to S1, there was a significant improvement overall in segmental lordosis, disc angle, and disc height. Although there was no significant difference in segmental lordosis or disc angle with increasing case number, there was a significant difference seen in posterior disc height between groups A and B. Regression analysis further demonstrated that this occurred after 11 cases. This likely demonstrates that increasing familiarity and comfort of the lateral ALIF exposure allows for increased trialing (eg, malleting tools down a minimally invasive corridor closely adjacent to great vessels) for the subsequent placement of larger and taller interbody cages that would result in increased posterior disc heights.
As a learning curve, there were notable changes to technique over time. These included the use of an Alexis wound protector to reduce superficial soft tissue creep, thoughtful taping to allow for working airspace near the inguinal ligament and groin crease, and placement of all retractor arms to the surgeon’s left (Figure 7). Changes to the closure technique with the use of braided nonabsorbable polyester sutures for fascia were implemented after the 2 instances of incisional hernias, and no further instances have occurred. Hemostatic tools that have been useful have included the availability of Tachosil fibrin sealant (Corza Medical, Westwood, MA, USA), Aquamantys bipolar sealers (Medtronic, Minneapolis, MN, USA), and endoclip appliers. Notably, in this case series, there were no major vascular injuries or vessel injuries that required blood transfusion, reoperation, or a request to an on-call vascular surgeon. We believe that these potentially life-threatening intraoperative complications present one of the greatest concerns and barriers for the adoption of this surgical exposure by spine surgeons, and we found that meticulous patient selection through preoperative review for favorable vessel anatomy greatly ensures that a safe, straightforward corridor is present. Beyond the previously mentioned incisional hernias, there were otherwise no approach-related complications known to be risks of this surgical exposure.4,16

Operative setup with the patient in lateral decubitus with the left side up as seen anteriorly. Note the retractor arms to the anterior surgeon’s left. K-wires have been placed with navigated assistance in the L3 to L4 and L4 to L5 levels at a separate incision, and the exposure has been performed at L5 to S1 with the retractor blades in place through the Alexis wound protector. The posterior surgeon (background) is completing the placement of L3 to S1 pedicle screws with robotic assistance.
Single-surgeon access to other spine regions is not uncommon. In the case of LLIF, an approach initially assisted by thoracic general surgeons, this is a procedure now commonly performed by spine surgeons.17,18 Similarities can also be drawn for access to anterior cervical approaches. Despite unfamiliar anatomical structures such as the trachea and esophagus, spine surgeons have familiarized themselves with retropharyngeal access to the anterior cervical spine without routine assistance from otolaryngologists.19 Beyond the current study, there has been a growing sentiment that lateral ALIF approaches no longer require a vascular access surgeon, which is supported by a recent Delphi consensus study concluding that routine lateral ALIF cases can be safely performed without a vascular surgeon.20
While there were no vascular or general approach cosurgeons scheduled for these cases, all surgeries were performed at an academic quaternary care center with on-call vascular surgeons who were very familiar with the L5 to S1 ALIF surgical technique in the event of any concerns. We also stress that this approach requires spine surgeons to have a very thorough understanding of lumbosacral anatomy and radiographic imaging interpretation, as well as good judgment in patient selection, which is key to avoiding complications. Prior experience in minimally invasive lateral approaches, whether through LLIF or ATP/OLIF is essential for familiarity with the retroperitoneal space and handling of instruments, as well as the possible complications associated with small surgical exposures with the patient in lateral decubitus position.
We report here our single spine surgeon learning curve experience with the minimally invasive lateral L5 to S1 ALIF (OLIF51) surgical approach. We found favorable clinical and radiographic results consistent with the known benefits of ALIF at this important biomechanical level while leveraging the benefits of minimally invasive lateral access surgery. We do however acknowledge the limitations of the current study. Since this is a case series, albeit a sizeable one, this study provides level 4 evidence. As a single-center, single-surgeon study with a limited patient sample, the generalizability of the results may be limited. As the only spine surgeon performing lateral ALIF exposures at this facility, we were unable to obtain multisurgeon data to determine intersurgeon heterogeneity. Based on the GRADE framework, this study provides low-quality evidence largely owing to the relatively small sample size and because it is a case series. Multicenter studies would help to determine and capture the reproducibility of these learning curves and results. If surgeons have not had ample training with retroperitoneal access to the anterior lumbar spine, we recommend appropriate training prior to performing these approaches independently.
There are several key takeaways from this article. First, the lateral ALIF is a safe and effective approach at L5 to S1 for spine surgeons and provide good clinical, biomechanical, and radiographic outcomes. Second, meticulous patient selection is extremely important for this type of procedure, especially regarding LCIV anatomy. Lastly, as expected, with an increasing number of cases, the surgeon became more comfortable with the approach, refined his technique, and was able to place interbodies that were able to provide greater posterior disc height and indirect decompression.
Conclusion
With good patient selection and meticulous technique, the minimally invasive lateral ALIF approach at L5 to S1 can be performed by spine surgeons already experienced with lateral access approaches to other levels of the lumbar spine.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
IRB Statement This research was approved by the medical center’s institutional review board, the patients consented to the procedure, and the participants and any identifiable individuals consented to publication of his/her image.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.