


Abstract
Background This is a retrospective review of 25 patients with severe lumbar nerve root compression undergoing multilevel anterior retroperitoneal lumbar interbody fusion and posterior instrumentation for deformity. The objective is to analyze the outcomes and clinical results from anterior interbody fusions performed through a lateral approach and compare these with traditional surgical procedures.
Methods A consecutive series of 25 patients (78 extreme lateral interbody fusion [XLIF] levels) was identified to illustrate the primary advantages of XLIF in correcting the most extreme of the 3-dimensional deformities that fulfilled the following criteria: (1) a minimum of 40° of scoliosis; (2) 2 or more levels of translation, anterior spondylolisthesis, and lateral subluxation (subluxation in 2 planes), causing symptomatic neurogenic claudication and severe spinal stenosis; and (3) lumbar hypokyphosis or flat-back syndrome. In addition, the majority had trunks that were out of balance (central sacral vertical line ≥2 cm from vertical plumb line) or had sagittal imbalance, defined by a distance between the sagittal vertical line and S1 of greater than 3 cm. There were 25 patients who had severe enough deformities fulfilling these criteria that required supplementation of the lateral XLIF with posterior osteotomies and pedicle screw instrumentation.
Results In our database, with a mean follow-up of 24 months, 85% of patients showed evidence of solid arthrodesis and no subsidence on computed tomography and flexion/extension radiographs. The complication rate remained low, with a perioperative rate of 2.4% and postoperative rate of 12.2%. The lateral listhesis and anterior spondylolisthetic subluxation were anatomically reduced with minimally invasive XLIF. The main finding in these 25 cases was our isolation of the major indication for supplemental posterior surgery: truncal decompensation in patients who are out of balance by 2 cm or more, in whom posterior spinal osteotomies and segmental pedicle screw instrumentation were required at follow up. No patients were out of sagittal balance (sagittal vertical line <3 cm from S1) postoperatively. Segmental instrumentation with osteotomies was also more effective for restoration of physiologic lumbar lordosis compared with anterior stand-alone procedures.
Conclusions This retrospective study supports the finding that clinical outcomes (coronal/sagittal alignment) improve postoperatively after minimally invasive surgery with multilevel XLIF procedures and are improved compared with larger extensile thoracoabdominal anterior scoliosis procedures.
New technology and methods continue to push the limits of minimally invasive spine surgery. The benefits of new techniques have proved advantageous for both patients and surgeons. Shorter surgery times, decreased hospital stays, decreased tissue trauma and blood loss, decreased postoperative pain, and a shorter return to daily life are all reported advantages associated with minimally invasive spine surgery.1–4
In 2001 Pimenta5–8 introduced an innovative minimally invasive spine surgery that accessed the anterior lumbar spine, using a lateral, transpsoas approach. Ozgur et al.,9 who later made the procedure popular in 2006, described a minimally disruptive spine procedure called the extreme lateral interbody fusion (XLIF) (NuVasive, Inc., San Diego, California). Through the XLIF procedure, access can be gained to the lumbar spine via a lateral approach that passes through the retroperitoneal fat and psoas major muscle.2
Unlike the traditional interbody fusions and approaches, the XLIF approach offers numerous advantages. A general surgeon is not required for access, the need to retract or violate the peritoneum is eliminated, and the approach avoids mobilization of the great vessels, thereby avoiding the related risk of sexual dysfunction.10–13 In comparison with anterior lumbar interbody fusion, the lateral approach offers safer access to the retroperitoneal space and disk space in patients who have had prior open abdominal surgery. When compared with transforaminal and posterior lumbar interbody fusion, the lateral approach allows a more complete diskectomy, annulectomy, osteotomy, and insertion of a larger interbody device. XLIF also results in limited posterior paraspinal muscle dissection and helps to avoid epidural scar dissection during revision spinal fusion for postlaminectomy surgery. Postoperative standing 3-foot radiographic results have shown an improvement in the sagittal- and coronal-plane alignment of the spine.7, 14–16
The indications for XLIF include symptomatic degenerative disk disease with instability, junctional lumbar degenerative disease (also known as adjacent segment disease or transitional zone disease), degenerative spondylolisthesis, recurrent disk herniation, degenerative scoliosis, and poor healing capacity of patients (eg, nicotine abuse, antiseizure medication use, diabetes, chronic steroid use, and other medical comorbidities). The purpose of this study was to review our series of 25 multilevel XLIF cases (78 XLIF levels) requiring supplemental posterior surgery—pedicle screw instrumentation and posterior osteotomies.
The contraindications for XLIF include previous bilateral retroperitoneal surgery, pregnancy, radiation because of retroperitoneal scarring, or bony pathology that precludes fusion surgery such as osteopenia, osteopetrosis, chronic autoimmune disease, and steroid dependence.11, 17, 18
Methods
Outcomes assessment
Little published literature is available that significantly supports the use of XLIF as an effective treatment for lumbar spine deformity or other degenerative cases as compared with traditionally accepted techniques using more extensile anterior exposure.
This article reports on data compiled from a database that includes a total of over 300 patients who underwent an XLIF procedure from 1993 to 2010. The majority were stand-alone lateral procedures with lateral plates and/or anterior rods inserted for spinal stabilization. The main principle of XLIF is to perform an anterior spinal decompression and indirectly decompress the spinal canal by gradually restoring the disk space height. This serves to decompress symptomatic lumbar nerve roots by increasing the height of the neural foramen. There were particular cases in our series that had spinal stenosis symptoms from complex multiplanar lumbar deformity—a combination of spondylolisthesis, lateral listhesis, and scoliosis. A retrospective database of over 300 cases of XLIF performed at our institution was analyzed over the last 17 years.1, 2, 18 A group of 25 patients fulfilled the following criteria: (1) a minimum of 40° of scoliosis; (2) 2 or more levels of translation, anterior spondylolisthesis, and lateral subluxation (subluxation in 2 planes), causing symptomatic neurogenic claudication and severe spinal stenosis; and (3) lumbar hypokyphosis or flat-back syndrome. In addition, the majority had trunks that were out of balance in the coronal plane (distance between plumb line and central sacral vertical line >2 cm from midline) or sagittal imbalance, defined by a distance between the sagittal vertical line (SVL) and S1 of greater than 3 cm.
There were 25 patients who had severe enough deformities fulfilling these criteria in whom supplementation of the lateral XLIF with posterior osteotomies and pedicle screw instrumentation was required (Fig. 1). The mean age of the 25 patients was 65.9 years (range, 41–78 years). They had a minimum of 3 contiguous lumbar spinal levels with XLIF, ranging up to 5 levels. The posterior instrumentation ranged from 4 to 6 levels, with a mean of 4.52 levels—the vertebral levels of posterior instrumentation and fusion always spanned, at a minimum, the intervertebral disk spaces with XLIF spacers.

Preoperative anteroposterior and postoperative radiographic views show a 53° degenerative scoliosis, disk space collapse, and neural foraminal narrowing from L1 to L5. Grade II subluxation laterally at L3 to the left of L4 with degenerative lateral listhesis is also seen at L3–4 with a rotatory component. The central sacral vertical line indicates that the patient's trunk is 2 cm out of balance toward the left compared with the coronal plumb line (case 5). The postoperative scoliosis correction was from 53° down to 7°.
At follow-up, most patients had computed tomography (CT) scans and all patients had flexion/extension radiographs to review so that we could assess the progress of fusion. The number of levels treated, procedural complications, mean operative time, mean estimated blood loss, mean length of hospital stay, perioperative complications, and postoperative complications were all assessed when reviewing records. The indications included in the multilevel XLIF series were deformity (spondylosis, spondylolisthesis, and scoliosis), adjacent segment disease, and lumbar nerve root compression reflected by severe neurogenic claudication.
XLIF technique
The XLIF approach requires the necessary understanding of anatomy and appropriate positioning of the patient. All cases fulfill the definition of minimally invasive surgery as defined in our prior publication.1 During dissection, a 1-incision technique less than 4 cm in length is recommended and caution should be exercised to ensure that it does not extend anteriorly to put the peritoneal contents and abdominal vascular structures at risk. Our preference is to perform the XLIFs on the concave side of the scoliosis with the hinge in the radiolucent table flexed opposite the curve to help reduce the scoliosis. This also serves to open up the disk spaces and provide easier access. We always start at the L4–5 level and work successively more proximally up to either L2–3 or L1–2. A dissection that strays too far posteriorly can cause risk to the neural foramen and exiting nerve roots. It is recommended that real-time, dynamic, and discrete neurologic monitoring be used during the procedure to ensure that the lumbar plexus is protected (Neurovision; NuVasive, Inc.).7, 19, 20 Running electromyography is performed throughout the decompression to ensure that the nerve roots are decompressed and also ensure that the lumbar plexus is not stretched or compromised during the lateral dissection through the psoas major muscle. Our initial dissection through the psoas is in zone 2.14, 19, 21 Axial images on the magnetic resonance imaging/CT scanner should be reviewed preoperatively to observe neural structures at the operative level(s) and to confirm that abdominal vessels do not obstruct the lateral disk space. Intraoperative fluoroscopy is used throughout the diskectomies—the C-arm needs to be constantly repositioned as the scoliosis is reduced, and the imaging beam needs to stay orthogonal to the vertebral end plates. The rotational deformity is corrected with Cobb elevators, which release the contralateral marginal vertebral body osteophytes. The osteotomies and anterior reduction essentially comprise a lateral adaptation of the spondylolisthesis reduction technique described by Bradford and Steffee using a “spinal persuader.”14, 22
After closure of the lateral multilevel XLIF approach, fluoroscopy images characteristically show good reduction of the scoliosis and spondylolisthesis but not the sagittal imbalance or the lumbar hypokyphosis. The patient is now positioned in the prone position, and standard open lumbar decompression with Smith-Peterson closing wedge osteotomies at each XLIF level is performed. In our experience this is the only way to correct (1) trapezoid-shaped vertebral bodies in the apex of the curve, (2) lumbar hypokyphosis, and (3) global imbalance with an SVA of 2 cm or more. In this series autograft and Osteocel (NuVasive, Inc.) were used as the biologics of choice for arthrodesis. Bone morphogenic protein 2 or INFUSE (Medtronic, Inc., Minneapolis, Minnesota) was not used for any procedures.
Results
Twenty-five cases were found that fulfilled the multiplanar deformity criteria outlined earlier. These 25 cases had undergone 3- or 4-level XLIF, anterior and posterior osteotomies, and posterior pedicle screw instrumentation. The patients presented with severe neurogenic claudication preventing ambulation. Each had 3-dimensional deformities in 2 planes (coronal- and sagittal-plane deformities) with 40° or more of lumbar scoliosis, axial rotation, and a minimum of grade I (25%) lateral or anterior spondylolisthesis (Table 1) with global imbalance.
Data for 25 consecutive cases
The neurogenic claudication resolved in all cases. The mean preoperative scoliosis was 42.9° (range, 40°–55°), and this improved to 5.08° at follow-up (range, 0°–15°). No patients were out of coronal balance at final follow-up, aside from case 23, whose SVA was 2 cm. The mean operative time was 236 minutes (range, 75–393 minutes), and the mean estimated blood loss was 958 cc (range, 50–3600 cc). The mean length of hospital stay was 4.75 days (range, 3–8 days). The preoperative visual analog scale (VAS) score for leg pain was 77.8, and this improved to 30.4 at follow-up. The mean follow-up was 24.6 months.
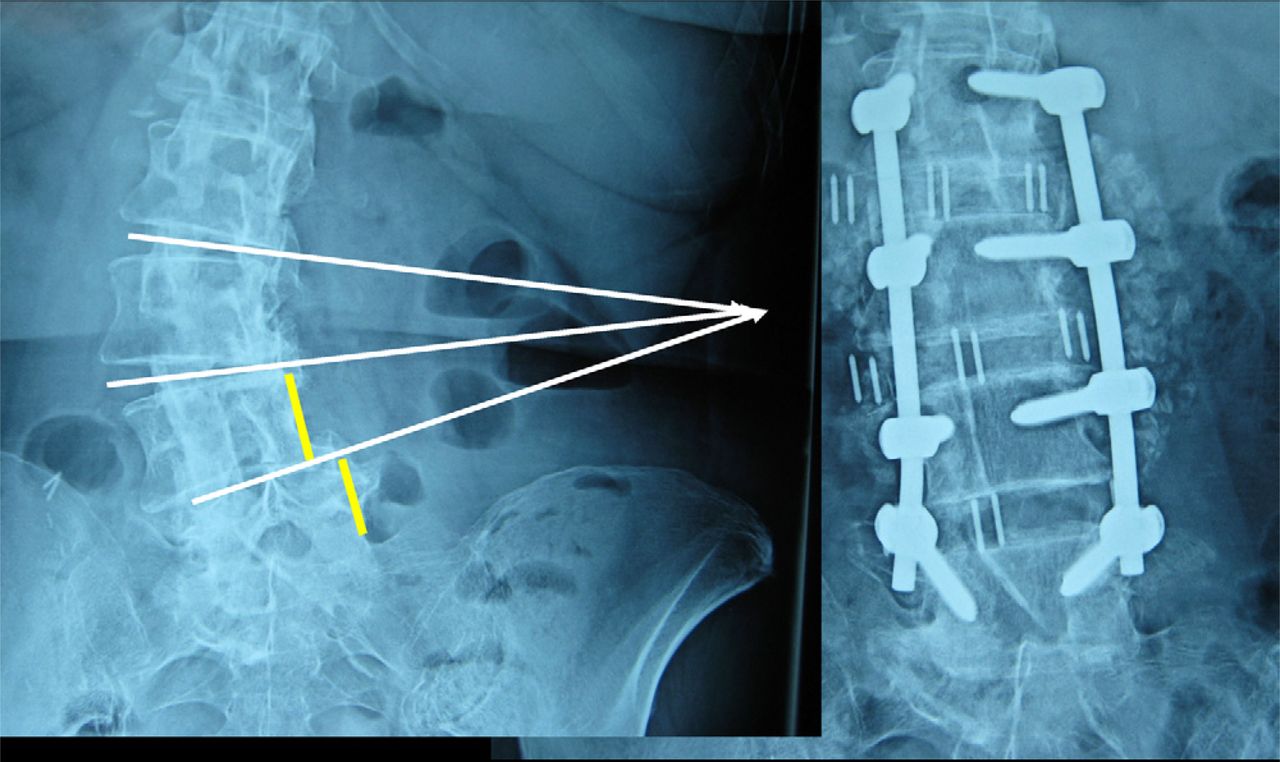
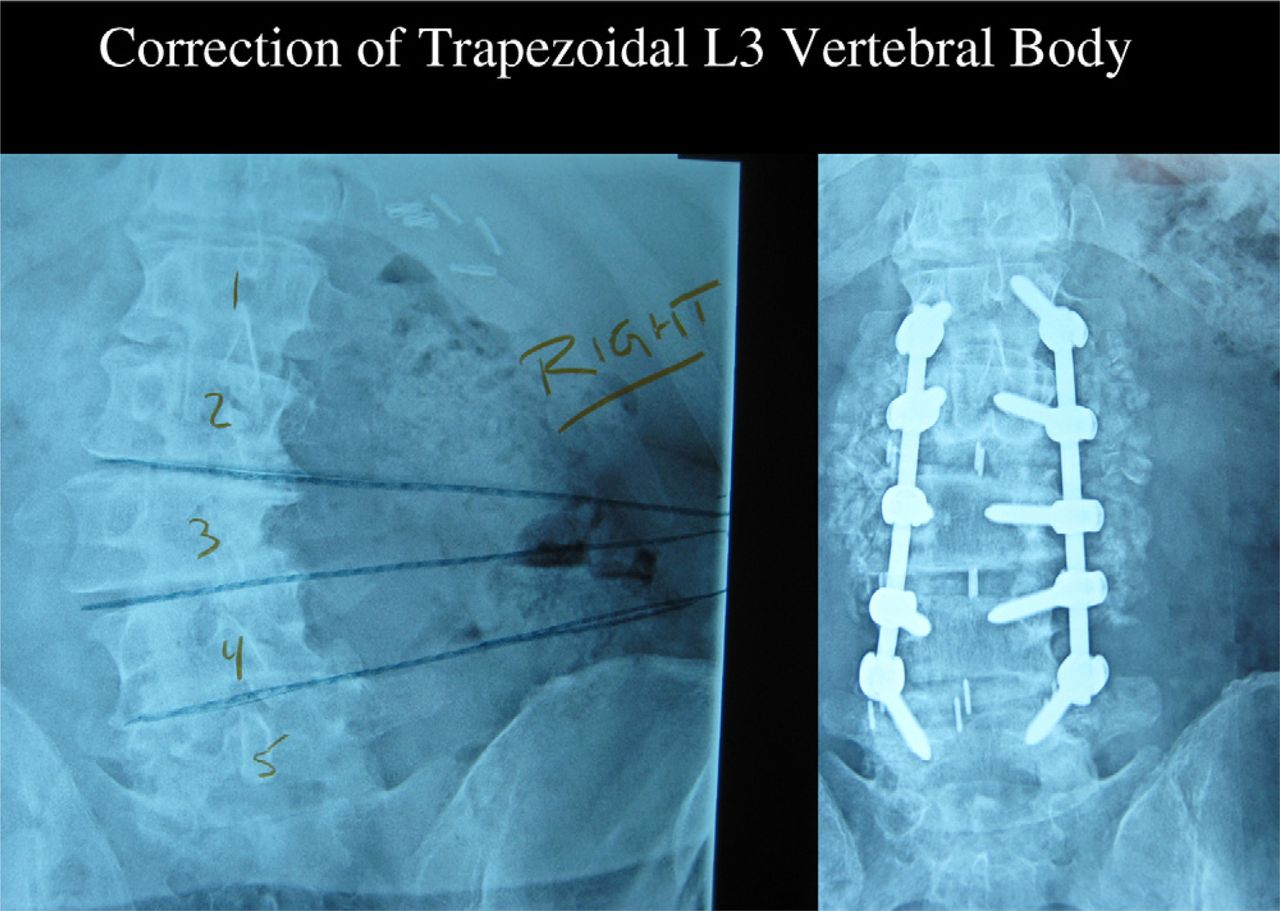
Some previous investigators have measured disk space and neural foraminal height from preoperative and postoperative radiographs, but we do not believe that these measurements are reliable without both preoperative and postoperative high-resolution multiplanar CT imaging, thought to be too expensive and not justified for this study. The best evidence for accurate reduction of rotational plane abnormalities was to confirm derotation of the ipsilateral pedicles on the convex side of the scoliosis just below the apex. In Fig. 1 this is the left L3 and L4 pedicles on the left image. On the post-instrumentation standing radiograph on the right side, it should be noted that the left L3 pedicle and the left L4 pedicle are almost collinear and the “Scotty dog” oblique profile of the left L3 pedicle has a markedly improved orientation postoperatively. In a similar fashion, the malrotation in the transverse plane can be confirmed in Fig. 2 by observing the disappearance of the Scotty dog profile of the right L3 pedicle compared with the right L4 pedicle just below.

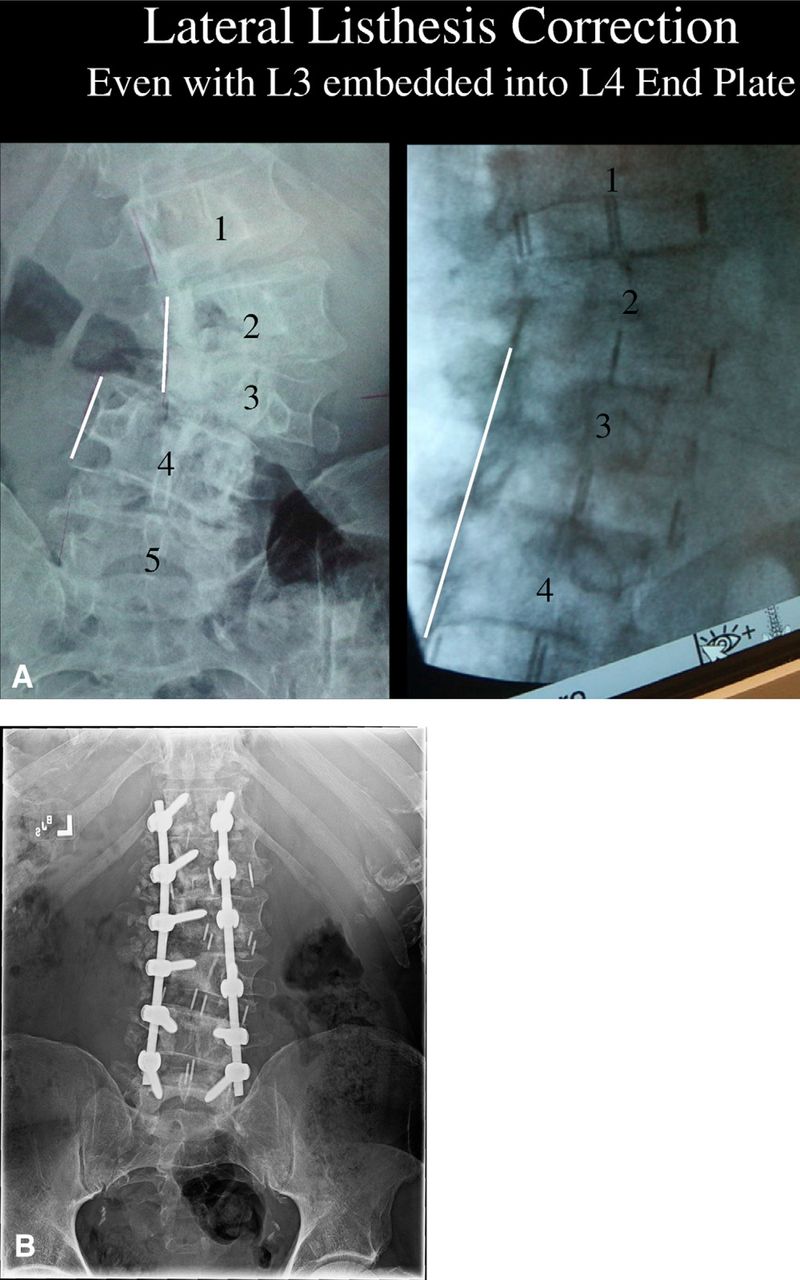
Lateral listhesis correction is possible with minimally invasive multiple-level XLIF. Even with the L3 vertebra embedded within the superior end plate of L4, this grade II lateral listhesis was reduced with the first-stage XLIF. The major reduction techniques include hinging the operating table such that the patient is bent toward the convexity, complete circumferential annulotomy, and XLIF performed from the concave side. In contrast to open traditional anterior scoliosis procedures, which are approached from the convex side, multilevel XLIF is performed from the concave side. Even the most severe cases of lateral listhesis can be corrected via the concave side. The trajectory to each of the L1–2, L2–3, L3–4, and L4–5 disks can be reached through a minimally invasive surgery incision 5 cm or shorter in length. Preoperative axial magnetic resonance imaging views showed severe stenosis at L3–4 with compression of the thecal sac, severe ligamentum flavum hypertrophy, and facet arthropathy, which were corrected through XLIF. However, a synovial cyst and soft-tissue compression of the nerve roots need to be directly decompressed through a posterior approach. (A) Correction of a coronal decompensation of 2 cm or more and sagittal decompensation of 10 cm or more needs to be achieved with posterior instrumentation. (B) Standing anteroposterior radiograph of same patient at follow-up. The pedicle orientation on the right side at L3 and L4 is now collinear, whereas in A, the right L3 pedicle is the oblique typical Scotty dog profile. It would require multiple postoperative CT cuts through the vertebra at different angles to quantitate the derotation more precisely, but the important point clinically is that the symptoms of radiculopathy from pedicular kinking of the convex apical nerve roots were alleviated. This 67-year-old man's neurogenic claudication was dramatically relieved postoperatively, and he could walk upright for extended periods.
Complications
One patient (patient 6) had an incidental durotomy during the procedure, which was repaired with No. 4-0 Nurolon suture (Ethicon, Somerville, NJ) and monitored for cerebrospinal fluid leakage postoperatively. Case 9 was a 64-yearold woman who had progressive weakness on the fifth postoperative day because of an epidural hematoma. This was emergently surgically explored and was decompressed. She successfully regained normal neurologic function with no long-term neurologic sequelae. There were no cases of cage migration or clinically relevant polyetheretherketone spacer subsidence.23
The incidence of neurologic complication that we experienced mirrors that of the prospective randomized trial of Isaacs et al.,15 a prospective nonrandomized trial of 107 patients. Eighty percent of patients had transient proximal ipsilateral thigh weakness due to passage of retractors through the psoas muscle (Fig. 3). Isaacs et al. defined major neurologic weakness as weakness that either did not resolve by the 6-month postoperative visit or was decreased by more than 2 grades at any point (7 of 107 patients [6.5%] in their series). In our series of 25 consecutive patients, we encountered 2 patients, cases 17 and 18, with residual quadriceps weakness persisting for more than 6 months (2 of 25 [8%]). The patients were ambulatory in a modified knee immobilizer. We also encountered 2 additional patients with pseudoparesis of the abdominal wall due to neurapraxia of the twelfth intercostal nerve. This caused the lower abdominal wall to bulge but was more of a cosmetic than a functional limitation.
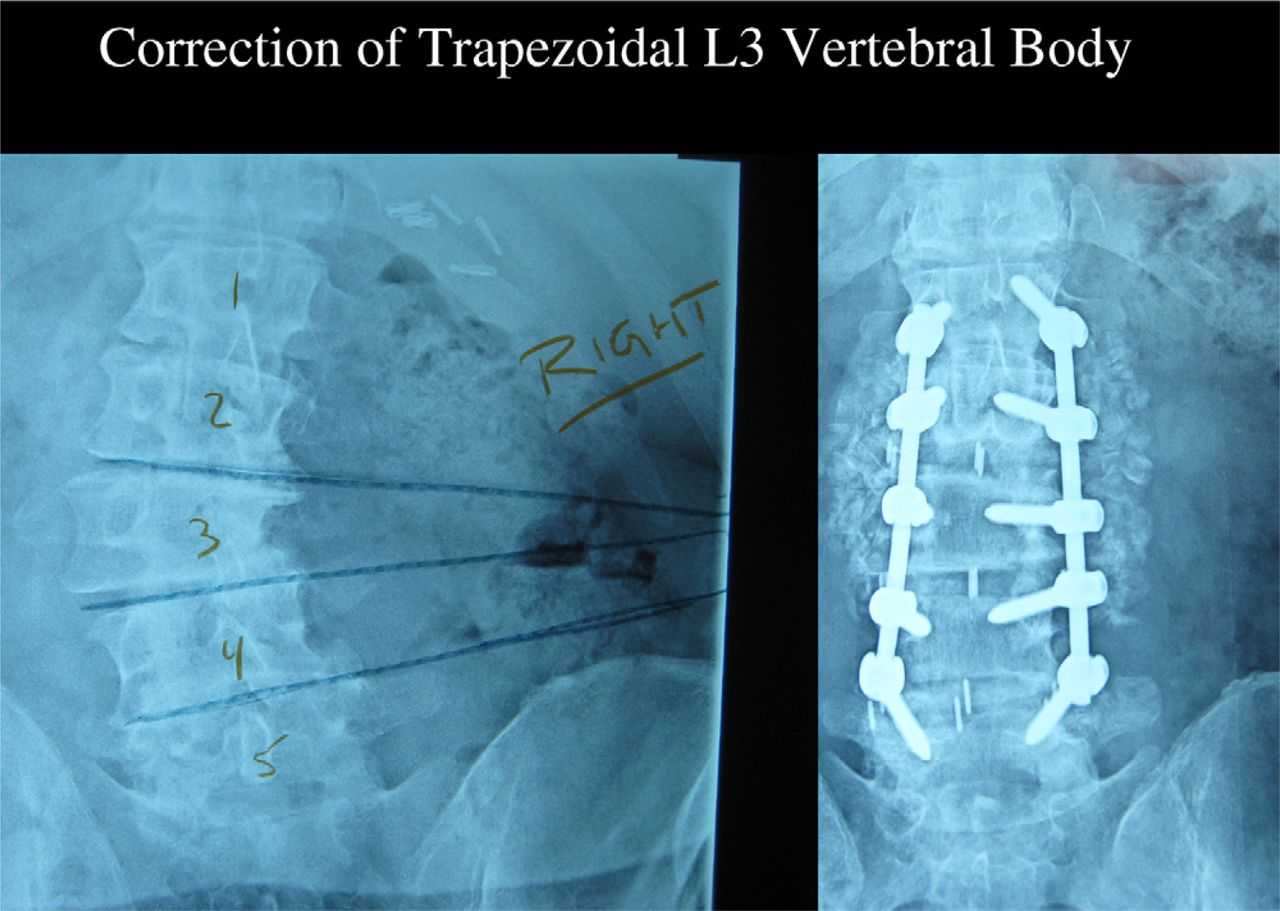
Correction of an L3 trapezoid-shaped vertebral body also needs to be performed by posterior shortening with multilevel osteotomies. Supplemental posterior osteotomies and pedicle screw instrumentation were necessary to restore 40° of physiologic lumbar lordosis.
Discussion
Historically, the 3 major anterior instrumentation procedures for correction of scoliotic deformities have involved an extensile exposure directed toward the convex side of the lumbar curvature—Dwyer, Zielke, and Kaneda. The advantages of an approach to the convex side of a scoliotic curvature are as follows: (1) the apex of the curve is rotated closer to the skin incision, making the spine more superficial; (2) the intervertebral disk spaces are wedged open wider toward the surgeon; and (3) the lumbar plexus and great vessels are situated more deeply toward the contralateral side (Table 2). The major disadvantage of the convex approach is that the major structures requiring release of the deformity are the osteophytes and bridging bone on the concave side of the curvature. In degenerative scoliosis there are usually bridging osteophytes and heterotopic bone along the narrowed disk spaces on the concave side. To resect these osteophytes and perform anterior osteotomies, the concave approach provides a closer exposure and more direct vision (Fig. 4). For the most part, the restoration of disk space and neural foraminal height is dependent on sequential spreading of the concave side of the disk spaces. To gain the advantages of the concave approach, the surgical technique requires neural monitoring and surveillance of the lumbar plexus to avoid postoperative neurapraxia. The concave approach allows more thorough resection of the disk and osteophyte syndesmophytes on the concave side of the curve. It also allows more direct insertion of loadbearing spacers within the disk space to maintain correction. The convex procedures are directed at the tension side of the curve; therefore the instrumentation compresses the vertebral bodies together in tension, which can result in unwanted lumbar kyphosis. The insertion of load-bearing spacers spanning from ring apophysis to contralateral ring apophysis from the concave side of the scoliosis allows for more effective lordotic correction (Fig. 5). The spacers also serve to increase neural foraminal height to alleviate spinal stenotic leg pain.

Multiple-level XLIF with supplemental posterior instrumentation reduced the scoliotic deformity from 47° down to 5°, and the grade II L3–4 lateral listhesis was also well corrected. The combined 3-dimensional deformity correction added over 3 cm of lumbar height.

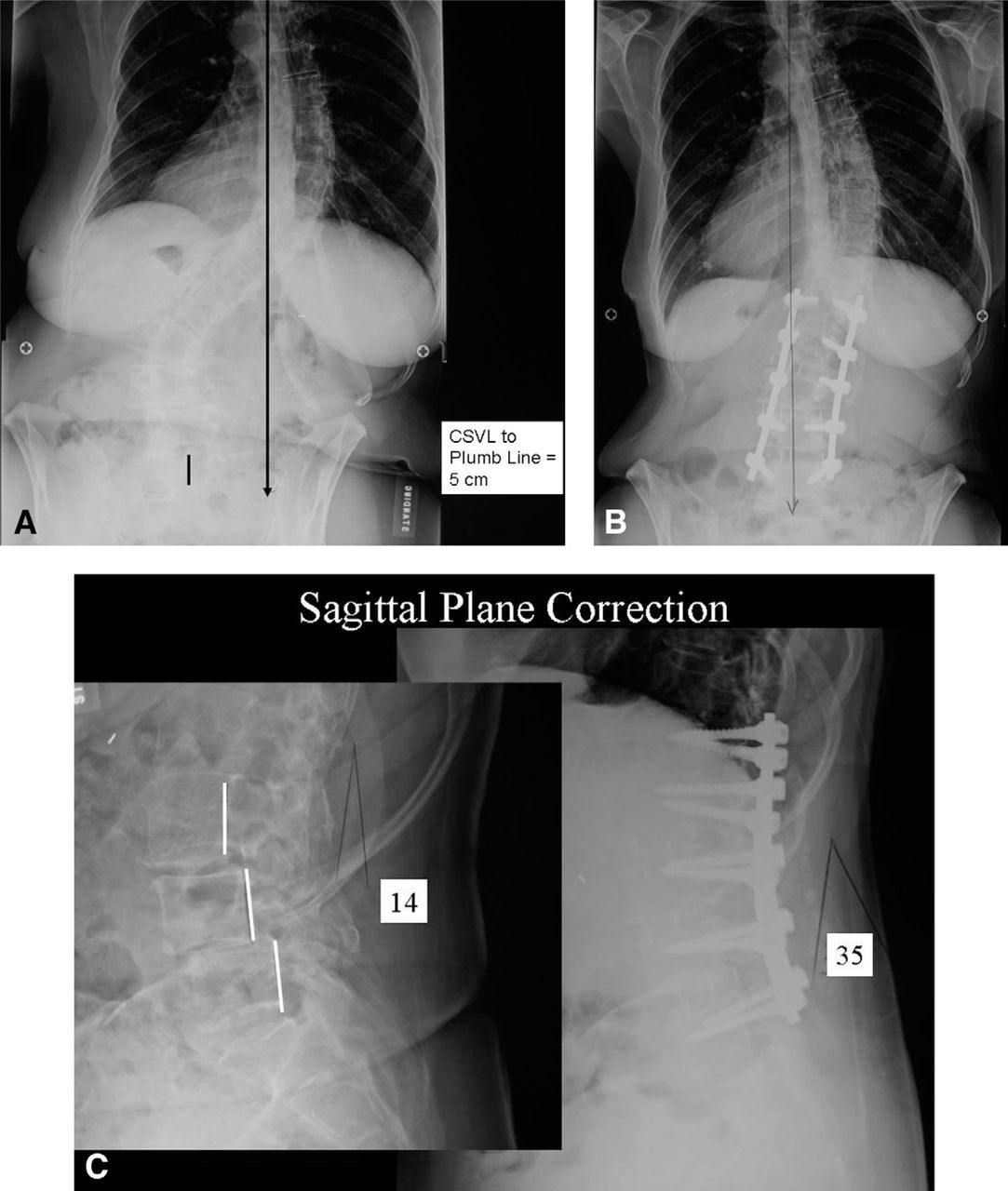
Case 8. (A) A 63-year-old woman presented with a 55° lumbar scoliosis, grade I L3–4 spondylolisthesis, and grade I L4–5 spondylolisthesis, and the central sacral vertical line (CSVL) distance to the vertical plumb line equaled 5 cm. (B) Postoperatively, the patient's sagittal vertical plumb line directly bisected her pelvis. Her scoliosis has been corrected to 15°. (C) Her lumbar lordosis of 14° was corrected to 35°.
Side of surgical approach for lumbar scoliosis
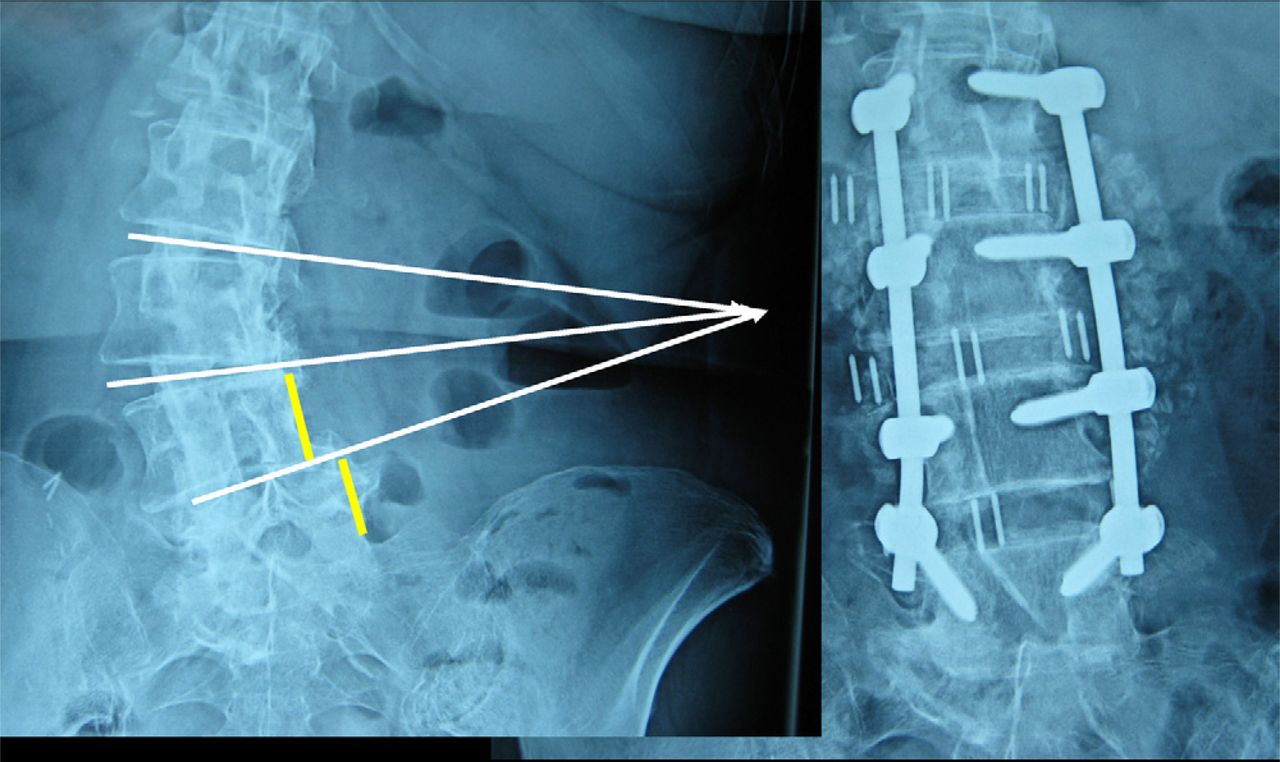
A clear exposure advantage is afforded by the concave side because the lumbar intervertebral disks all point toward a converging area on the concavity of the patient's flank. In contrast, the intervertebral disks and end plates on the convex side diverge, and if orthogonal line of sight is required for diskectomy and osteotomy, a less minimally invasive approach is required (Fig. 6).
Case 3. The preoperative and postoperative lumbar radiographs show effective correction of both the lateral L4–5 listhesis and the 40° lumbar scoliosis using 3-level XLIF and L2–5 posterior instrumentation and fusion. One should note the convergence, or “pointing,” of the scoliotic disk spaces toward a confined area on the concave flank—this provides for a more minimally invasive surgery than the historical convex “extensile” approach.
The third major exposure advantage to approaching a scoliosis from the side is that the operating table can be hinged with the patient in the lateral position. Bending the incision open if the convex side is up serves to increase the deformity. On the other hand, hinging open the operating table with the concavity in the upward direction serves to reduce the scoliosis (same mechanism as a side-bending radiograph), and the table positioning helps reduce any subluxation present in the lower L3–4 and L4–5 levels. The lateral osteotomies resecting the concave bridging osteophytes can be more readily accessed and addressed under direct vision from the concavity in an adult degenerative scoliosis. The 3 technical features that facilitate the evolution of deformity surgery are (1) Neurovision with hunting algorithms and step-wise running electromyographic surveillance; (2) operative positioning on a radiolucent table capable of hinging (Jackson Lateral Access Table, MIZUHO OSI, Union City, CA), which assists in deformity reduction, before the skin incision is even made; and (3) much larger intervertebral load-bearing polyetheretherketone spacers with rectangular footprints that can be inserted from the concave side (50–60 mm in length and 22–28 mm in width).
The published literature supports an improvement and maintenance in lumbar lordosis, as well as sagittal and coronal alignment, after an XLIF procedure.5–8, 15, 17 Kepler et al.22 reported a 3.6° increase in mean lordosis at each instrumented level at 1-year follow-up. Rodgers et al.21 found that the coronal angle was significantly corrected from 24.3° to 12.9° and maintained at the 1-year follow-up. Sagittal angles were also maintained through the 6-month follow-up period from 16° preoperatively to 25° postoperatively. Tormenti et al.20 conducted a study in which patients underwent a transpsoas procedure with posterior instrumented fusion versus posterior-only correction using transforaminal or posterior lumbar interbody fusion technology. At a mean follow-up of 10.5 months, the study results found that the combined lateral transpsoas and posterior procedure had a mean curve correction of 70.2% and a mean Cobb angle of 10°, which had decreased from 38.5° preoperatively. The posterior-only group was found to only have a mean curve correction of 44.7% and a mean Cobb angle of 11°, which had decreased from 19°.
Positive conclusions could be drawn that the XLIF procedure results in postoperative improvement in VAS scores.1, 7, 14, 15, 17, 22, 24 Specifically, Pimenta et al.7 reported VAS scores averaging from 8.33 at preoperatively to 3.16 at the 2-year follow-up (10 point scale) whereas Oswestry Disability Index scores increased from a mean of 51.2 preoperatively to 27.3 (100 point scale). At a mean follow- up of 11 months, Dakwar et al.19 observed a 5.7-point improvement in VAS scores and a 23.7% increase in Oswestry Disability Index scores.
Much of the literature found on XLIF focuses on complications perioperatively and postoperatively, along with the radiographic results. The complications reported to be associated with XLIF included subsidence, hardware failure, transient lateral thigh weakness, cage migration, anterior longitudinal ligament rupture, permanent femoral injury, bowel perforation, infection, pulmonary embolism, durotomy, hemodynamic instability, pleural effusion, vertebral body fractures, pseudarthrosis, and dysesthesia.2, 3, 7, 19, 21, 23 The complications remained minimal in our series and did not adversely influence the neurologic outcome5 at follow-up. Smith and Malone13 focused on a large number of patients at a single site to determine the occurrence rate for complications. The greatest percentage of complications was attributed to transient lateral thigh weakness, 100% of which resolved by 6 to 12 weeks after surgery. Fewer than 1% of the complications reported in the study were due to intra-psoas nerve damage.13, 15
The objective of minimally invasive surgery is to decrease dissection- and approach-related muscle trauma, decrease blood loss, decrease length of hospital stay, and promote early mobilization of patients.1 Our data suggest that with the XLIF approach in treating lumbar spine deformity, patients with deformity in 1 plane can have effective reduction with stand-alone anterior XLIF and anterior instrumentation.2 However, if a patient has a combined 3-dimensional deformity such as combined lateral subluxation and multiple-level rotational scoliosis, this requires posterior supplemental decompression and pedicle screw stabilization (Table 3). All 25 of our cases had intraoperative radiographs after the anterior XLIF procedures but before the second stage. The lateral listhesis and the anterior listhesis were reduced, but with combined deformities, the lumbar lordosis was not optimally corrected. The posterior approach provided a more thorough canal decompression of soft tissue and allowed posterior column shortening by facet resection and posterior osteotomies, mainly through Smith- Peterson osteotomies. The addition of posterior pedicle screw instrumentation further enhanced the stabilization, evidenced by the reduction of lumbar scoliosis to less than 15° in 25 consecutive cases.
Two major types of adult scoliosis
Conclusion
The XLIF minimally invasive approach offers numerous benefits over traditional anterior procedures to the lumbar spine. Some of these include the following: not requiring a general access surgeon, not requiring retraction or violation of the peritoneum, eliminating the need for mobilization of the great vessels, and preserving the anterior and posterior longitudinal ligaments.5, 18, 22 Although complications of XLIF are not insignificant and have been the focus in the literature, they remained minimal in our group of patients, considering the magnitude of the deformities and degree of preoperative stenosis. The data presented in this article parallel those from the published studies concerning less severe deformities that used the XLIF procedure to obtain disk space height correction. We achieved, on average, 88% correction of the scoliotic deformity and improvement in VAS scores by 64%. Thus we have shown the effectiveness of XLIF in combination with posterior pedicle screw stabilization to correct 3-dimensional lumbar spinal deformities.
- © 2013 ISASS - International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}