


Abstract
Background Use of computer-assisted insertion of pedicle screws has some advantages owing to the reportedly decreased incidence of pedicle breach and clinical events. Registration-based methods based on preoperative computed tomography imaging, 2D fluoroscopy, and 3D fluoroscopy are the most popular, however each has its limitations. O-arm–based navigation, which uses intraoperative acquisition and registration of navigated images, may overcome many of these disadvantages. We set out to study the clinical accuracy and navigational accuracy for pedicle screw insertion using our recently acquired O-arm and present our preliminary findings.
Methods The first 26 patients operated consecutively for L4-5 fusion were included in the study. O-arm–based navigation was used to insert the pedicle screws. Postoperative computed tomography images were acquired and assessed for pedicle breach and anterior cortical perforation. Planned trajectories of each screw were compared with the actual trajectories in the postoperative images to assess navigational accuracy in both axial and sagittal planes.
Results A total of 104 screws were inserted. One screw (1%) breached the pedicle laterally. Nonsignificant anterolateral cortical perforations were noted in 7 screws (6.7%), all of which occurred at L5 level. The mean axial and sagittal navigational error was 2.3° (±1.7) and 3.1° (±2.3), respectively. There were no significant differences in the errors between L4 or L5 level. The occurrence of anterior perforation correlated with the degree of axial (P = .02) but not sagittal (P = .12) navigational error. There were no clinical events related to the screw insertion.
Conclusion Use of O-arm–guided pedicle screw insertion was associated with low incidence of pedicle breach (1%) and a low range of navigational error in both sagittal and axial planes. Anterolateral vertebral body perforation was higher at L5 without any negative clinical events. Despite the high need for technical support, we found that O-arm was a very efficient tool for accurate pedicle screw insertion.
Introduction
Pedicle screw fixation to augment bony fusion is commonly performed in spine surgery. Although most pedicle violation errors are clinically irrelevant, nerve root injuries are not uncommon. cerebro spinal fluid leak, vascular injury, and visceral injury have also been reported.1–4 Over the last decade, the use of image-guided navigation for pedicle screw insertion is preferred by some surgeons owing to the reportedly decreased incidence of pedicle breach and clinical events. The 3 most popular navigation systems used are computed tomography (CT) navigation, 2D fluoroscopy, and 3D fluoroscopy.
CT-based navigation using paired point and surface registration is widely practiced. It requires the acquisition of preoperative CT images of the spine. Intraoperatively, selected anatomical points on the vertebra were matched to the computer-generated model on the work station. However, the process is time consuming and has a considerable learning curve, and the results are variable.5–8
Fluoronavigation relies on anteroposterior and lateral 2D images obtained intraoperatively. Although relatively inexpensive, the quality of 2D fluoroscopic images obtained at certain levels can be disappointing.
3D fluoroscopy-based navigation provides real-time intraoperative 3D imaging. Intraoperative images can be obtained while the digital reference array (DRA) is attached to the patient thereby automating the registration process. The O-arm (Medtronic Surgical Technologies, Louisville, Colorado) is a recent 3D fluoroscopy system that provides image quality similar to that of CT. The preliminary results are promising regarding accuracy of pedicle screw insertion with the O-arm.9–12 However, the reports on navigational errors using the O-arm are limited to axial errors.12, 13
The goal of our series was to describe axial and sagittal navigational errors, in addition to the clinical accuracy for O-arm–assisted pedicle screw insertion in L4-5 degenerative spondylolisthesis.
Methods
Twenty-six consecutive patients with degenerative spondylolisthesis underwent L4-5 instrumented fusion by the senior author (BG) from September 2011 to December 2012. All pedicle screws were inserted with help of the O-arm. All patients received high-resolution preoperative CT imaging for navigation planning (2-mm isotropic resolution, 1-mm overlap with anatomical coverage of L2-S2 vertebrae. The digital imaging and communications in medicine images were imported to the StealthStation (Medtronic Surgical Technologies, Louisville, Colorado), and 2D and 3D models were reconstructed to simulate L3-S1 fusion. Printouts of this simulation with screw sizes were displayed in the operating room.
We exposed the spinous processes from the inferior aspect of L3 spinous process to the superior aspect of L5, the L4 and L5 laminae, and the transverse processes till the tips. The integrity of L3-4 interspinous ligaments and facet joints was preserved. The passive DRA was fixed on the L3 spinous process. The O-arm was draped with sterile plastic and positioned around the patient on the Jackson table (Orthopedic Systems Incorporated). A 3D low-resolution image was acquired in 13 seconds while the breathing was stopped. A total of 392 single images were recorded in a full 3601 rotation of the radiation source and detector unit. The images were taken without the retractor (Crank, Codman) in place. The data set from the O-arm was automatically transferred to the StealthStation where 2D and 3D images were created. Planning of the screws was done by the senior author on the StealthStation (version 2.0). The navigation wand was registered on the divot of the passive DRA. The navigation wand with the ball tip was applied to the spinous process laminae and transverse process to check the accuracy of the system.
The screw image was reproduced on the patient to match the entry point, exit point, and angulation. In a few instances, the planning was changed to accommodate the limitation of the retractors. An air drill was used to traverse the outer cortex of the base of the mammillary process in line with the planned screw. A nonnavigated straight pedicle probe was inserted along the direction provided by the navigation probe. The trajectory and depth were confirmed by the navigation wand. The integrity of the pedicle walls and anterior cortex was tested with a ball point. A proper-sized tap was inserted along the pedicle. A pedicle screw (Stryker Xia 3 system, Hamilton, Ontario, Canada) was inserted after checking with the navigation probe. All screws were polyaxial. We attempted to use 6.5mm diameter screws but a few of them were 5.0 mm, 5.5 mm, or 6.0 mm screws owing to anatomical constraints. The screw length varied from 30–55 mm. The senior author placed all screws on the right side and 25% of the screws on the left side, while the fellow or resident placed the rest under supervision of the senior author.
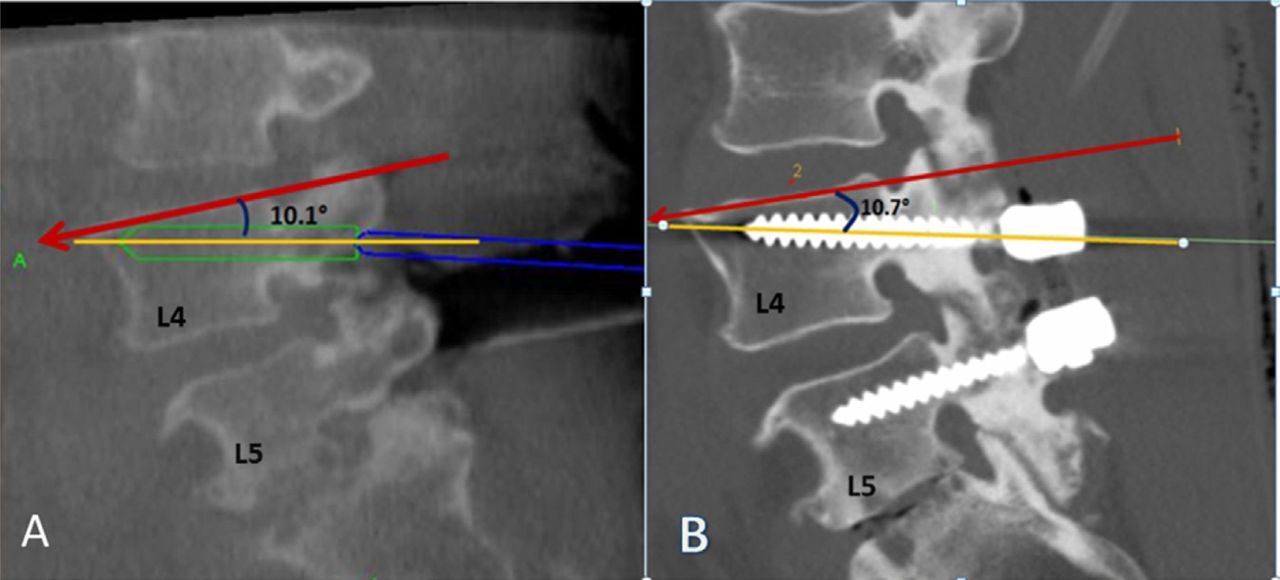
A thin-cut postoperative CT scan (Toshiba Aquilon One, Tochigi-Ken, Japan) from L3 to S1 was done. Errors were evaluated on axial (media and lateral) and sagittal images (cranial and caudal) for pedicle breach and anterolateral perforations of the vertebral body. The pedicle errors were graded using accepted definitions: grade I (0–2.0 mm), grade 2 (2.1–4.0 mm) grade 3 (4.1–6.0 mm), and grade 4 (6.1–8.0 mm).14, 15 Anterolateral perforations were quantified in millimeter as the distance traversed by the tip of the screw beyond the perpendicular of the cortical margin (Fig. 3).
Navigational errors
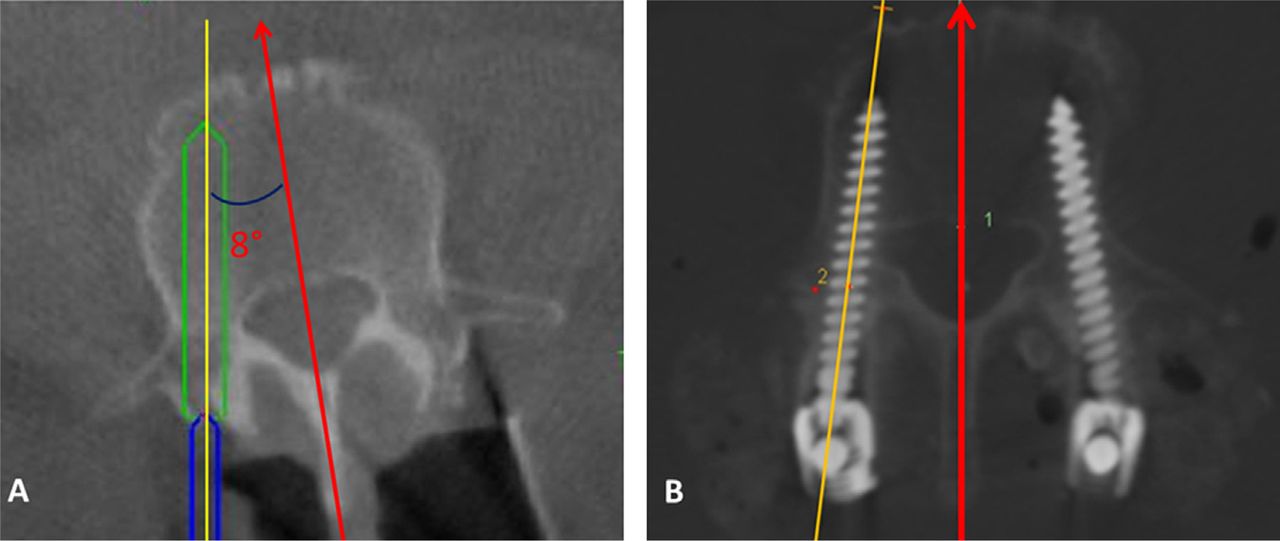
To study the navigational error, a snap shot of the planned screw images (virtual images) acquired by the O-arm on the StealthStation and the postoperative CT images on the picture archiving and communication system (Intelliviewer software version 4-2-1-P301, Intelerad Systems Inc., Montreal, Canada) were compared. The axial screw angle was defined as the angle made by the pedicle screw axis with the midsagittal vertebral axis (Fig. 1). The midsagittal vertebral axis is a line bisecting the vertebral body, midpoint at the base of the lamina, and tip of the spinous process, and it has been described earlier.16 The sagittal screw angle was defined as the angle made by the pedicle screw axis with the superior end plate of the respective vertebral body (Fig. 2).
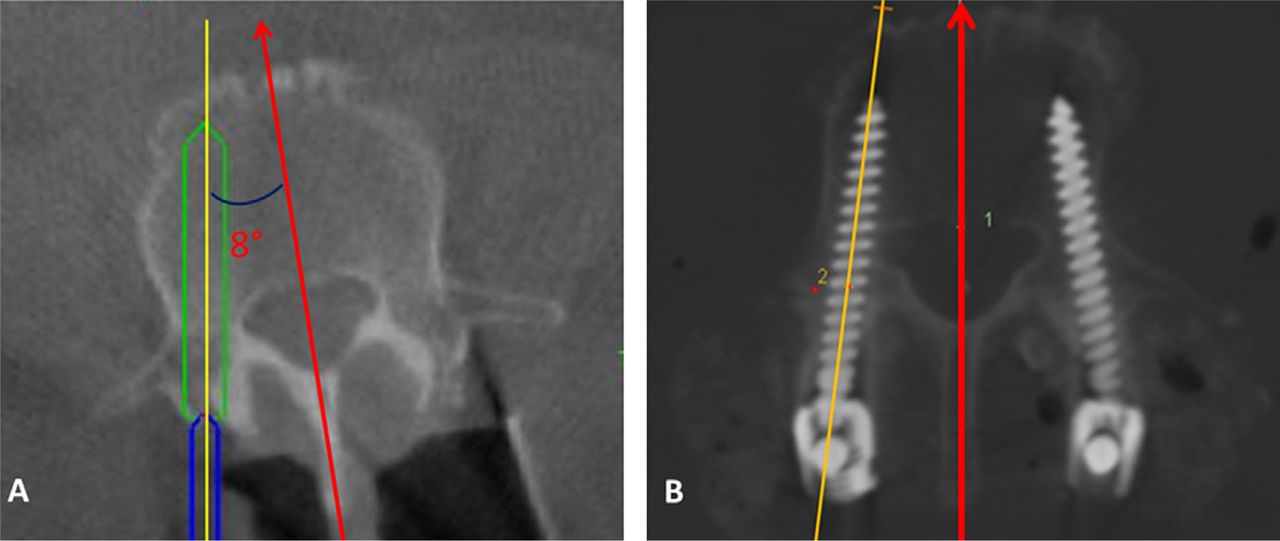
(A) Axial angle on the O-Arm images. The arrow represents the midsagittal plane of L4, which is defined as 0°. The planned screw makes a 13.1° angle with the midsagittal plane of L4. (B) Axial angle on the postoperative images. The actual screw made 11.2° angle with the midsagittal plane of L4. (Color version of figure is available online.)

(A) Sagittal angle on the O-Arm images. The arrow is the superior end plate of L4 defined as 0°. The planned screw makes a 10.1° angle with the end plate of L4. (B) Sagittal angle on the postoperative images. The actual screw makes a 10.7° angle with the end plate of L4. (Color version of figure is available online.)
The difference between the planned axial screw angle and the postoperative axial screw angle was defined as the axial navigational error (Fig. 1A and B). Similarly, the difference between the planned sagittal screw angle and the postoperative sagittal screw angle was defined as the sagittal navigational error (Fig. 2A and B). Statistical analysis was done using the JMP software (version 8.0).
Results
A total of 104 screws were inserted in 26 patients. None of the patients had complications from hardware misplacement. There were no new postoperative radiculopathy or vascular injuries.
Pedicle breaches
A single (1/104; 1%) pedicle breach occurred at right L5 grade 1 (lateral breach of 1 mm). No clinical effect was seen.
Anterior perforation
There was a total of 7 of 104 (6.7%) anterolateral perforations (mean: 2.2 mm and range: 1–4 mm). All these perforations were at the L5 level.
Degree of navigational errors
The planned angle and the postoperative angle for each level in axial and sagittal planes is given in the Table.
Axial navigational errors
The mean axial error for L4 screw was 2.1° (±1.6) whereas for L5 screw it was 2.7° (±1.9). There was no significant difference between right and left (P = .43) or between L4 and L5 screws (P = .10).
Sagittal navigational errors
The mean sagittal error for L4 screw was 2.8° (±2.1) whereas it was 3.2° (±2.6) for L5. There was no significant difference between right and left (P = .53) or between L4 and L5 screws (P = .69).
Correlation of anterior perforation with degree of navigational error
The correlation between the occurrence of anterolateral perforation and the axial error was statistically significant (P = .02). However, there was no significant correlation between anterolateral perforation and sagittal error (P = .12).
Discussion
Pedicle breach
In our study, we had a pedicle breach rate of 1% (a single lateral error of 1 mm). This is comparable to the available literature for thoracolumbar pedicle screw insertion using O-arm showing error rates between zero and 3%.9–12 It is better than in our previous study (unpublished data) where we used preoperative CT scan and conventional navigation with mainly paired point registration (SNN, Mississauga, Ontario, Canada). Those errors were mostly lateral.
The planned angle and the postoperative angle for each level in axial and sagittal planes. The mean navigational error in both planes is shown in column 4 and column 7. Standard deviation in parentheses
Anterolateral perforations
Anterolateral perforations are not routinely mentioned in the pedicle screw literature presumably because it is very rarely associated with any clinical events. There were 7 (6.7%) cortical perforations on the anterolateral surface of the vertebral body. Most perforations were 2 mm or less, except one case which had a 4-mm perforation. All perforations were at the L5 level. None of them was near blood vessels or visceral organs. There was a positive correlation between the extent of axial error and presence of a perforation. Though the L5 pedicle is the most angulated and has the most margin for rotational error, we found anatomical constraint to be a significant factor for error. We theorize that the major limitation for obtaining an L5 screw angle close to the anatomical pedicle angle is the constraints of the retraction. We observed that L5 is deeper in the field owing to lordosis. We minimized the dissection of L5 spinous process since the use of the O-arm. Previous preoperative navigation systems required more spinous process dissection for paired point registration and more lamina dissection for surface matching. The second factor involved is our paradigm to plan for a potential L3 to S1 fusion in the future. From our viewpoint, we also wanted to avoid the facet joint of L3-4. Respecting these constraints, the planning of L5 screws were less angulated than L4 screws (Fig. 3). This coupled with the triangular shape of the L5 vertebral body leaves almost no margin for error as the virtual screw invariably touched the anterolateral cortex. Unfortunately, these errors occurred despite feeling the anterior cortex with a ball tip. During surgery we occasionally had to alter the trajectory owing to the proximity of the screw heads. This adjustment was done mostly in the sagittal plane and might not be a significant factor in the rate of perforation.

Shows an example of anterolateral perforation. The adjacent image shows the planned L5 trajectory almost parallel to the midline sagittal vertebral axis. The triangle-shaped L5 body and proximity of the planned screw to the cortical margin can be noted. (Color version of figure is available online.)
Degree of navigational error (sagittal and axial angular deviation)
We believe estimating navigational accuracy is important as it helps to compare the accuracy of different systems. In 1999, Kamimura et al.13 first described the degree of angular deviation from the planned trajectory or the “virtual image” in vitro when using computer-assisted navigation using preoperative CT scan. Oertel et al.,12 in 2011, reported that the mean angular deviation was 2.8° for 94 thoracolumbar screws inserted with the help of O-arm. The aforementioned studies looked only at the angular deviation in the axial plane. Our study looked at both axial and sagittal angular deviations. This is useful to determine the inferior or superior deviation from the planned sagittal trajectory. Rampersaud et al.17 studied the maximum permissible axial error at different vertebral levels when reporting on the accuracy requirement for image-guided pedicle screw placement. This was estimated to be 9.8° and 12° at L4 and L5, respectively. Our study showed the axial error to be 2.1° at L4 and 2.7° at L5 and the sagittal navigational error to be 2.8° and 3.2°, respectively. This level of navigational accuracy is extremely useful when inserting screws at the midcervical, midthoracic, and thoracolumbar junction where the navigational accuracy requirements are much higher.
Reasons for navigational error
Although navigation-guided pedicle screw insertion is more precise, no guidance system is 100% accurate. There are multiple sources of error in image guidance systems. They include imaging errors, registration errors, tracking errors, distance of navigation probe from the DRA, movement of the DRA after registration, and surgeon error.13, 18 Another source of error could be the possible toggle at the polyaxial screw joints mentioned in an earlier report,12 However, in comparison with the paired point registration or surface matching, or both, using preoperative CT scan, the O-arm eliminates surface model registration errors and imaging data inaccuracy owing to changes in position of patient.
Use of other methods to insert pedicle screws
Most spine surgeons now use at least plain radiography or 2D fluoroscopy to insert pedicle screws. Navigation for inserting pedicle screws is not yet widely accepted owing to technical and time limitations. Freehand screw insertion has high rates of screw misplacement. Despite using fluoroscopy, the rates of screw misplacements are still high. They vary between 5% and 41% for lumbar screws.17, 21 One study compared conventional pedicle screw insertion with O-arm assistance and reported 16.5% pedicle perforation rate with freehand as compared with 1% with O-arm.9 Percutaneous insertion of lumbar screws showed 97% accuracy with O-arm as compared with 87.2% with fluoroscopy.11
Image-guided techniques have reported lower misplacement rates between 0% and 14% for thoracolumbar pedicle screws.9, 17, 19–23 Although screw misplacement does not always translate into neurologic injury, it could lead to a loss of stiffness of the implant and late spinal instability.24 Kosmopoulos and Schizas25 conducted a meta-analysis in which they reported 130 studies with a total of 37,337 pedicle screws inserted and concluded that the median placement accuracy of the assisted navigation group was 95.2% as compared with 90.3% in the unassisted group. The difficulties with the acceptance of navigation in the spine community can be explained by many factors: surgeon training and beliefs, increased time for screw insertion, requirement of expensive navigation equipment, and need for technical support.
CT-based navigation (using paired point or surface registration)
Preoperative CT-based paired point registration or surface registration method is a commonly used technique for navigation. The accuracy of this method depends on the quality of the preoperative images, on the algorithms of the computer systems, and on the skill of the operating surgeon. The preoperative CT data are obtained when the patient is supine; however, the patient is positioned prone on the operating table changing the alignment often, thereby requiring individual registration and prolonging the operative time. Although better than the conventional method, CT-based paired point registration is reported to be ciated with pedicle breach rates from 2%–28%.5–8
2D fluoroscopy (fluoronavigation)
Fluoronavigation uses intraoperative anteroposterior and lateral fluoroscopy while the DRA is fixed within the operative field. These images are then transmitted to a work station. The position of the navigation probe is then tracked on a virtual fluoroscopy image on the monitor. The pedicle breach rates by this method are reported to be between 8% and 15%.19, 20 The quality of the fluoroscopically generated images, the surgeon's ability to interpret them, and consequently, the accuracy are similar to those of conventional fluoroscopy.19 The images may be suboptimal in patients with obesity, complex anatomy, or spinal deformity and in spinal regions where fluoroscopy is difficult. Fluoromerge is similar to fluoronavigation except that in addition to the aforementioned, the preoperative CT images can be fused to the intraoperative images.
3D fluoroscopic imaging (O-arm and Iso-C3D)
Both the O-arm and the Iso-C3D (Siemens AG Medical Solutions, Erlangen, Germany) are examples of 3D fluoroscopic imaging, which provides real-time intraoperative images for navigation. However, the O-arm provides image qualities similar to that of a CT scan with lower radiation exposure. The high-quality postoperative images can be used to correct any significant error. The accuracy of these systems range from 93%–100%.9, 10, 12, 21, 22, 26
Tian et al.,27 in 2011, conducted a meta-analysis of in vivo and in vitro comparative studies of pedicle screw insertion accuracy between different navigation methods and reported that 3D fluoroscopy was superior compared with CT-based navigation or 2D fluoroscopy.
Radiation dose
The additional imaging acquired during the course of an image-guided procedure presents clinical, as well as radiation safety implications, involving additional radiation exposure to the patient and operator. The radiation exposure associated with the O-arm technique, however, is less or comparable to pedicle screw techniques using conventional fluoroscopy. In comparison with conventional fluoroscopy (C-arm), the effective radiation dose to a patient during a complete navigation CT scan of the abdomen (standard protocol) using the O-arm would be approximately equivalent to 56 seconds of regular fluoroscopy, or 19 seconds of higher-power (boost) fluoroscopy,28 under the conventional fluoroscopic approach, which takes on an average about 2–3 minutes.29, 30
In our practice, preoperative and postoperative CT imaging would be obtained in both O-arm–based technique and the fluoroscopy-based technique, and thus present comparable radiation exposure. Some phantom based studies have shown that under the same radiographic techniques (peak kilovoltage, milliampere second, scan length, and field of view), the amount of absorbed radiation dose attributed to a CT acquired on the O-arm is approximately half the dose from a 64-slice CT scanner.31 The bone tissue contrast provided by the radiographic technique on the O-arm system is inferior to conventional CT, although it is sufficient for localization of anatomical features during image-guided pedicle screw placement. In our experience, we have found that the O-arm dosage can be further lowered without a detrimental effect on the quality of the resultant CT image. In fact, this reduction of dosage from the standard protocol established on the O-arm system could possibly be up to 5–13 times.32 In addition, radiation exposure to the operating room personnel is negligible as they stay out of the room during the acquisition of O-arm images. However, it is recommended that the O-arm operator wear additional protection as the potential radiation dose is higher than standard fluoroscopy.
Study limitations
This study analyzed 104 screws inserted at the L4 and L5 levels with O-arm–assisted navigation. There was no comparison with other methods. Owing to the lack of a control group, definite conclusions cannot be drawn as to the superiority of this technique over other methods. The senior author has extensive experience with CT-based navigation using paired point and surface registration and had a pedicle perforation rate of 5.9% (49/836 screwsunpublished data). However, this is not an appropriate comparison as this was at a different time point before the acquisition of the O-arm. The images were analyzed by the primary author and the senior author and hence this may introduce some bias in the interpretation of images. Calculation of the sagittal and axial angles is not an accurate science because of the variations in anatomy of the vertebral bodies. Intraobserver and interobserver errors are possible, and this method has not been validated. We did not use the navigated pedicle finder and the navigated screw driver. This could have contributed to some of the errors.
Conclusion
Use of O-arm–guided pedicle screw insertion was associated with a low incidence of pedicle breach (1%) and a low range of navigational error in both sagittal and axial plane. Anterolateral vertebral body perforation was higher at L5 without any negative clinical events. Despite the high need for technical support, we found that O-arm was a very efficient tool for accurate pedicle screw insertion.
- © 2013 ISASS - The International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}