


Abstract
Background Chronic low-back pain is a widespread condition whose significance is overlooked. Previous studies have analyzed and evaluated the medical costs and physical symptoms of chronic low-back pain; however, few have looked beyond these factors. The purpose of this study was to analyze and evaluate the personal and psychosocial costs of chronic low-back pain.
Methods To measure the various costs of chronic low-back pain, a questionnaire was generated using a visual analog scale, the Depression Anxiety and Stress Scale, the Short Form 36 Health Survey, and the 1998–1999 Australian Bureau of Statistics Household Expenditure Survey (for demographic questions). The comprehensive survey assessing physical, mental, emotional, social, and financial health was administered to 30 subjects aged 18 years or older who had visited a tertiary spine service with complaints of chronic low-back pain.
Results It was found that subjects scored significantly higher on scales for depression, anxiety, and stress after the onset of chronic low-back pain than before the onset of back pain. Subjects also reported a reduction in work hours and income, as well as a breakdown in interpersonal relationships, including marital and conjugal relations.
Conclusion Chronic low-back pain affects the ability of a patient to work, creating both financial and emotional problems within a home. Relief is delayed for patients because of the sparse allocation of resources for chronic spinal care and inadequate prevention education. Despite this, many patients are exhorted to return to work before they are physically, mentally, or emotionally free of pain, resulting in poor outcomes for recovery. Ultimately, this aggregates into an adverse macrosocial effect, reducing not only the quality of life for individuals with chronic low-back pain but also workforce productivity.
An often overlooked medical condition, chronic lowback pain, debilitates many people and contributes to the number of disability-adjusted life-years globally. Work-related low-back pain alone results in approximately 800,000 disability-adjusted life-years annually.1 In 2004–2005, 15% of Australians reported having chronic low-back pain2; Walker et al.3 estimated that approximately 8 of 10 Australians (79.2%) will have back pain at some point during their lifetimes. Furthermore, 10% of Australian adults have debilitating low-back pain. Globally, there has also been an increase in the prevalence of chronic low-back pain, highlighting the need for action.4
The vast majority of low-back pain cases consists of low-intensity back pain; however, the aggregate economic burden of this condition is staggering: $8.15 billion in lost productivity (certificated and non-certificated costs included)5 was estimated for the year 2001 in Australia alone. The documented and recorded costs comprise the certificated costs; those not explicitly recorded comprise the non-certificated costs. Most of the cost is attributable to indirect costs rather than direct costs. Direct costs include expenses for diagnosis, treatment, and rehabilitation; indirect costs include all other costs, such as lost productivity.6 This economic burden underscores the need to retrench lost hours in productivity and to prevent the onset of chronic low-back pain. A focused effort on chronic low-back pain will likely address other issues as well because it has a high comorbidity, often associated with conditions such as depression.7
Chronic low-back pain poses unique problems because over one-third of patients do not achieve a full recovery from an episode of chronic low-back pain, and most of these individuals return to the workforce a mere 12 months after the first episode of pain.8
In examining the degree of cost attributable to chronic low-back pain, Dagenais et al.6 performed a systematic review of the cost of illness studies related to low-back pain. Their publication dealt with the direct and indirect costs of low-back pain and identified, as a third type of cost, the intangible costs of illness, which are inherently more difficult to quantify because they reflect a reduced enjoyment of life because of illness. This often-overlooked category comprises the attendant costs on the individual and his or her household—including costs, such as an inability to interact meaningfully with others. A limited number of studies have focused on the aspects of chronic low-back pain contributing to the personal burden of the condition and one's psychological well-being—in addition to the commonly assessed financial costs. Buchbinder et al.9 argue that although the burden of a disease is defined in terms of death, morbidity, cost, disability, and quality of life, none of these suffice for assessing the overall burden of chronic low-back pain from the perspective of affected individuals. Buchbinder et al. sought to create a more accurate conceptual framework with which one could analyze the impact of chronic low-back pain, through the concept mapping and cluster analysis. Statements were first collected from individuals with chronic low-back pain regarding its effects on the lives of people around them, as well as their own. These individuals were then asked to group their statements into clusters. The issues in each cluster were to be more closely related to each other than they were to issues in other clusters. The participants were then asked to repeat the entire process, this time working in groups of individuals with chronic low-back pain. The clusters made by the groups of patients were analyzed by multidimensional scaling and cluster analysis and made into 2-dimensional graphs depicting the statements and their relationships. The process was repeated at an international forum of various health specialists. After collecting their concept maps, Buchbinder et al. integrated these clusters together to produce a concept map that contained 4 overarching clusters—psychosocial, treatment, employment, and physical—each with anywhere between 2 and 6 subclusters. The study demonstrates how chronic low-back pain affects individuals, highlighting a loss of independence, anxiety about the future, and negative or discriminatory actions by others as major areas of concern to patients. However, lacking is a quantitative-analysis method of the problems associated with chronic low-back pain. The study of Buchbinder et al focuses on identifying problems associated with chronic low-back pain and creating a valid theoretic model for questionnaires to measure pain; although it did identify what lines of questioning are necessary, the study did not illustrate the extent to which individual persons are affected and/or continued to be affected because of back pain. Providing a quantitative analysis of these costs will enhance the understanding of chronic low-back pain and how it manifests.
The aims of this article are to analyze not only monetary but also psychological and social costs to individuals with chronic low-back pain—a number of which were identified in the 2011 study by Buchbinder et al.9
Methods
This prospective study based on patient recall was conducted after we received the approval of the Human Research Ethics Committees of the University of New South Wales and Harvard University. Thirty consecutive eligible patients were randomly recruited from the Spine Service at St George Hospital Campus in Sydney, Australia, in February 2008. To be eligible, all subjects must have been at least 18 years old, able to read and speak English, and have had chronic low-back pain with or without leg pain in excess of 3 months. Chronic low-back pain was defined as pain exceeding 3 months in the area bounded superiorly by T12 and inferiorly by the gluteal crease.10 Within the sample population, the duration of symptoms before the study ranged from 6 to 712 months; on average, patients had pain for 161 months before the study.
An 8-page questionnaire, which included questions from 4 different scales and profiles for physical and mental health, was administered. The visual analog scale measured a subject's perceived intensity of back and leg pain. The Short Form 36 Health Survey measured the physical and mental health of patients across 8 dimensions: physical functioning, role limitations because of health problems, bodily pain, social functioning, general mental health, role limitations because of emotional problems, vitality, and perceptions of general health.11 The Depression Anxiety Stress Scale (DASS-21) assessed the psychological and emotional states of the subject before and after the onset of pain. The questionnaire incorporated questions that evaluated the extent to which a subject's interpersonal relationships had changed since the onset of chronic low-back pain. Also included in the questionnaire were demographic questions (age, sex, number and ages of children, occupation, income, etc.), as well as an excerpt from the 1998–1999 Australian Bureau of Statistics Household Expenditure Survey to measure financial stress and hardship. Each of these tools identified changes in the physical, mental, social, and financial health of the subject that can be attributed to chronic low-back pain to determine both the direct and indirect costs of the condition.
Statistical analysis was performed on the data from the questionnaire in the form of t tests for the sample mean difference between subject ratings before and after the onset of chronic low-back pain. The differences were evaluated for significance at the α = .01 level.
Furthermore, structured questionnaires were not expected to provide individual stories of life with chronic low-back pain. To better understand the impact of pain on individual patients with chronic low-back pain, additional face-to-face interviews were conducted in January 2012 with new subjects (n = 5) who were not part of the original cohort. These subjects offered insight into life before and after the onset of chronic low-back pain. The interviews were conducted based on the availability of interviewers and subjects with an appointment on that day. Both open- and closed-ended questions were used.
Results
Financial costs
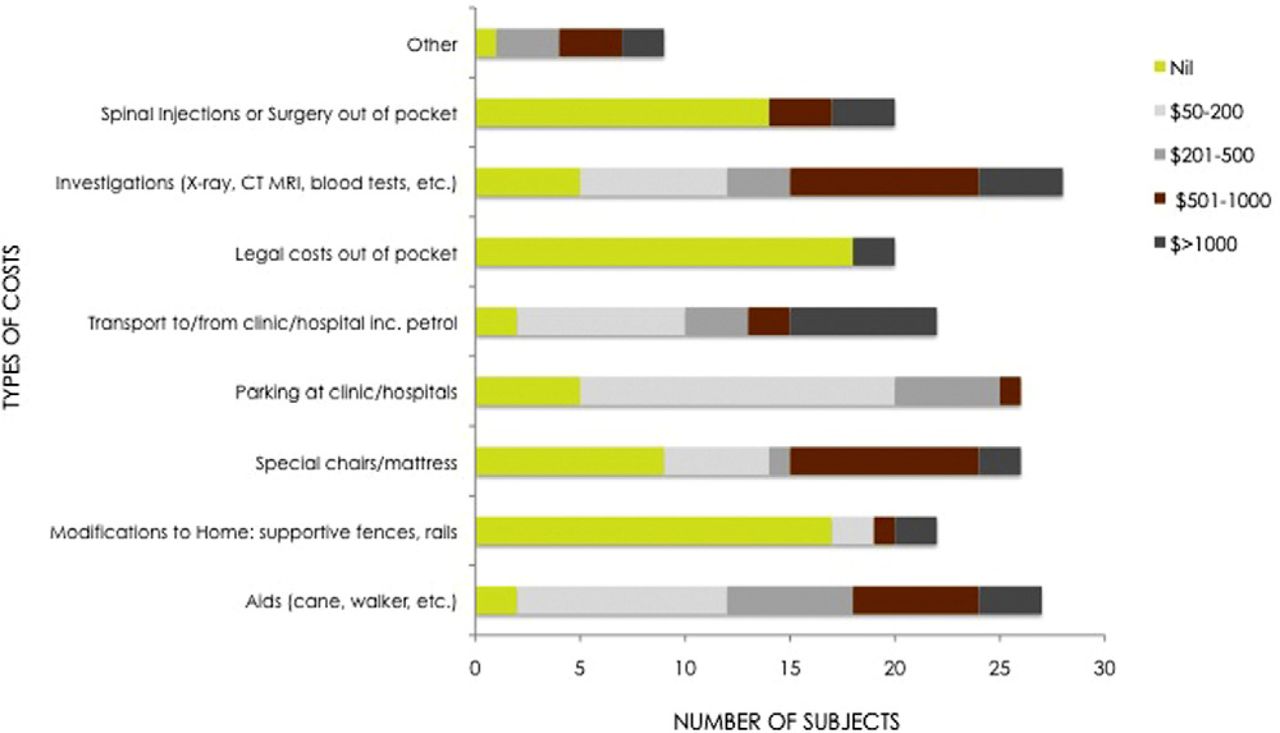
This study indicates a number of out-of-pocket costs to the subjects. Examples of costs include costs of spinal injections or surgery, investigations, legal fees, transportation, specialized chairs/mattresses, home modifications, and aids. Overall, the most frequently reported cost over $1000 was for transportation to clinics and hospitals (Fig. 1). For parking at clinics and hospitals, subjects most commonly spent $50 to $200, as spent by 15 of 26 subjects. For transportation costs to and from the clinic, subjects most commonly spent $50 to $200, as spent by 8 of 22 subjects; however, nearly as many subjects spent much more: 7 of 22 subjects spent over $1000. For physical aids, subjects most commonly spent $50 to $200, as spent by 10 of 27 subjects. For modifications to their homes, subjects most commonly spent up to $50, as spent by 17 of 22 subjects. For special chairs and mattresses, 9 of 26 subjects spent $501 to $1000. For legal costs related to chronic low-back pain, subjects most commonly spent up to $50, as spent by 18 of 20 subjects. For medical scans, subjects most commonly spent $501 to $1000, as spent by 9 of 28 subjects. For spinal injections, subjects most commonly spent less than $50 out of pocket.
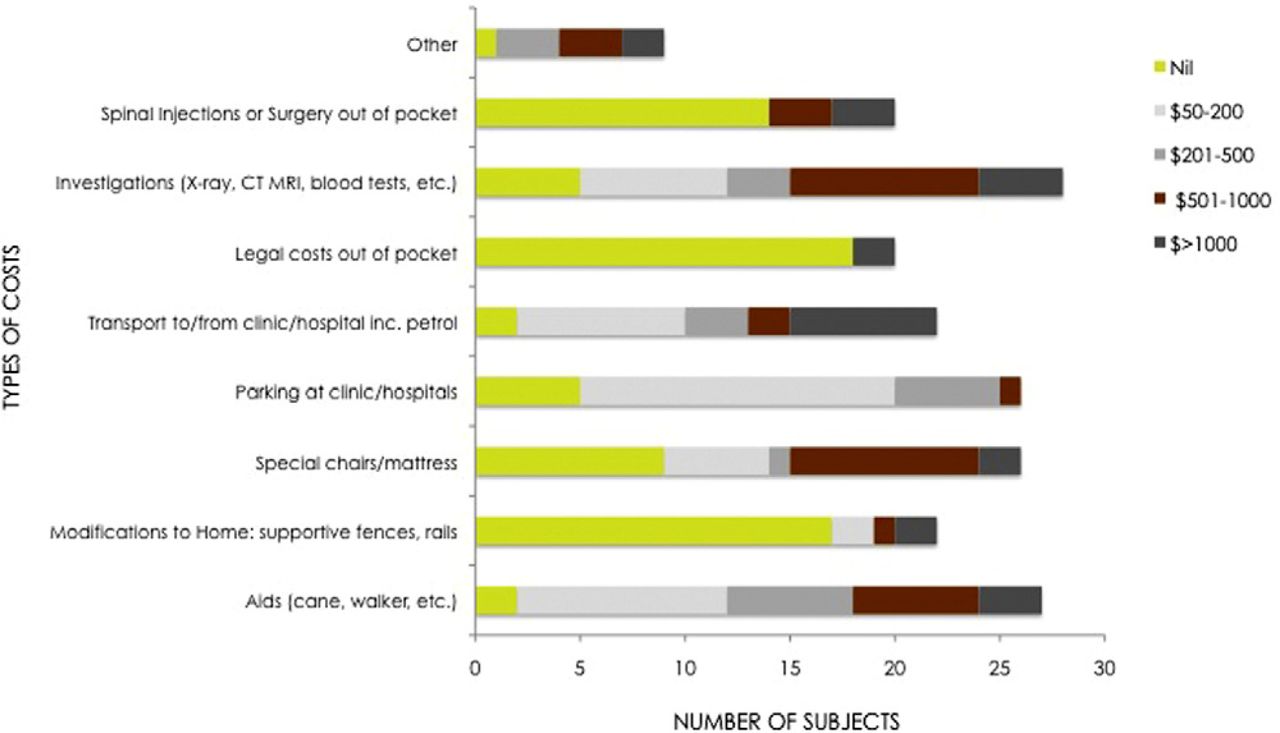
Graphed visualization of cost distribution for services related to care of chronic low-back pain. (CT, computed tomography; MRI, magnetic resonance imaging.)
Productivity
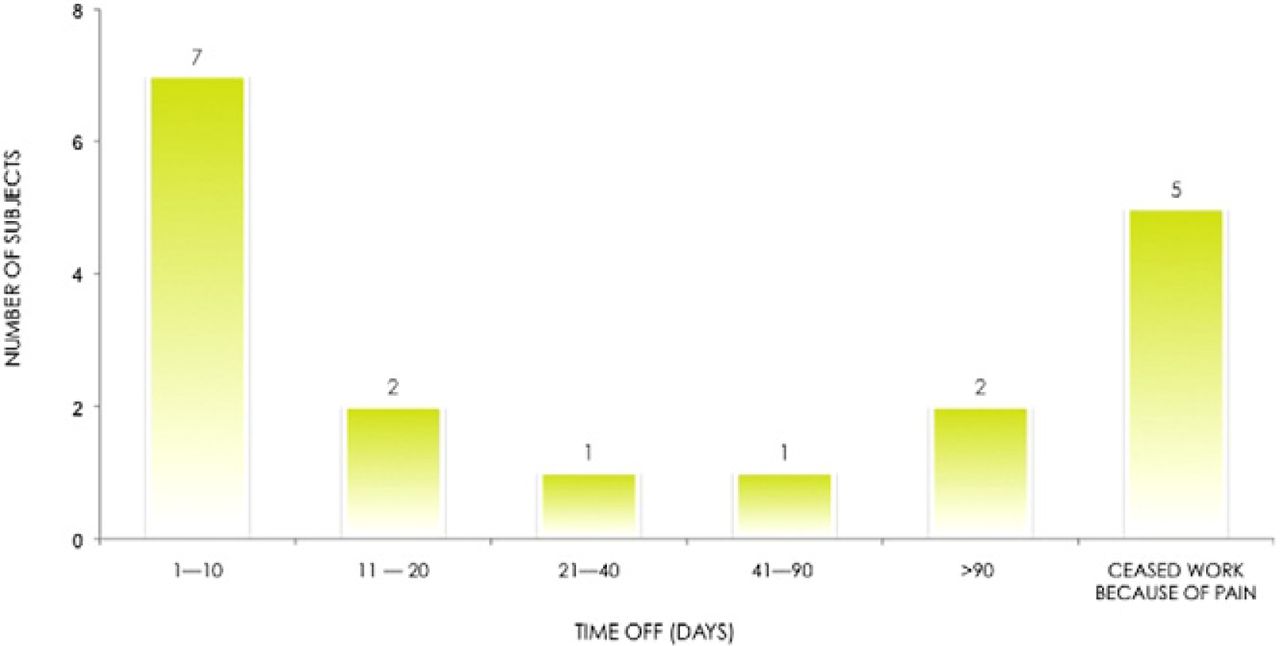
Before the onset of chronic low-back pain, subjects with paid jobs were working an average of 40 hours a week. After the onset of chronic low-back pain, subjects reported an increase in the number of days of absence from work that had to be taken per year because of back pain alone. Of 18 respondents, 40% (7 of 18) reported taking between 1 and 10 days of absence because of chronic low-back pain (Fig. 2). Almost 30% of respondents (5 of 18) reported having to cease work altogether after the onset of chronic lowback pain. Over 10% of subjects (2 of 18) reported taking 11 to 20 days of absence. Over 20% of subjects (4 of 18) reported taking more than 3 weeks of absence from work, with over 50% of them (2 of 4) taking more than 3 months of absence. A 10% (4-hour) average decrease in productivity, as compared with levels of production before chronic low-back pain, was found for subjects who continued working after the onset of chronic low-back pain (P = .0001). Nearly 45% of subjects (13 of 30) reported the loss of a promotion opportunity, including salary raises and business opportunities, after the onset of chronic low-back pain. In response to open-ended questions, subjects reported being “out of the loop” in terms of workplace changes and additional training because they were classified as “unfit for work.” Subjects also reported being demoted and even being unable to continue in the field for which they were trained after the onset of pain. Moreover, subjects reported a loss of overseas opportunities because of travel limitations attributable to chronic low-back pain, as well as a fear of termination because of their attendance records or productivity. One subject in particular responded, “[My] employer [was] seeking to promote me this year [but] hesitated due to [my] attendance record. [My] previous employer asked me to resign due to amount of time off due to back pain.”

Distribution of number of days of absence subjects have taken because of issues related to chronic low-back pain.
F.L., injured on her job as a nurse, now works reduced hours. Before her injury, she was a manager working on the plans for upcoming renovations, to which, because of her injury, she can no longer contribute. She felt excluded because the plans progressed without her and now resents her limited abilities and involvement.
Psychological costs
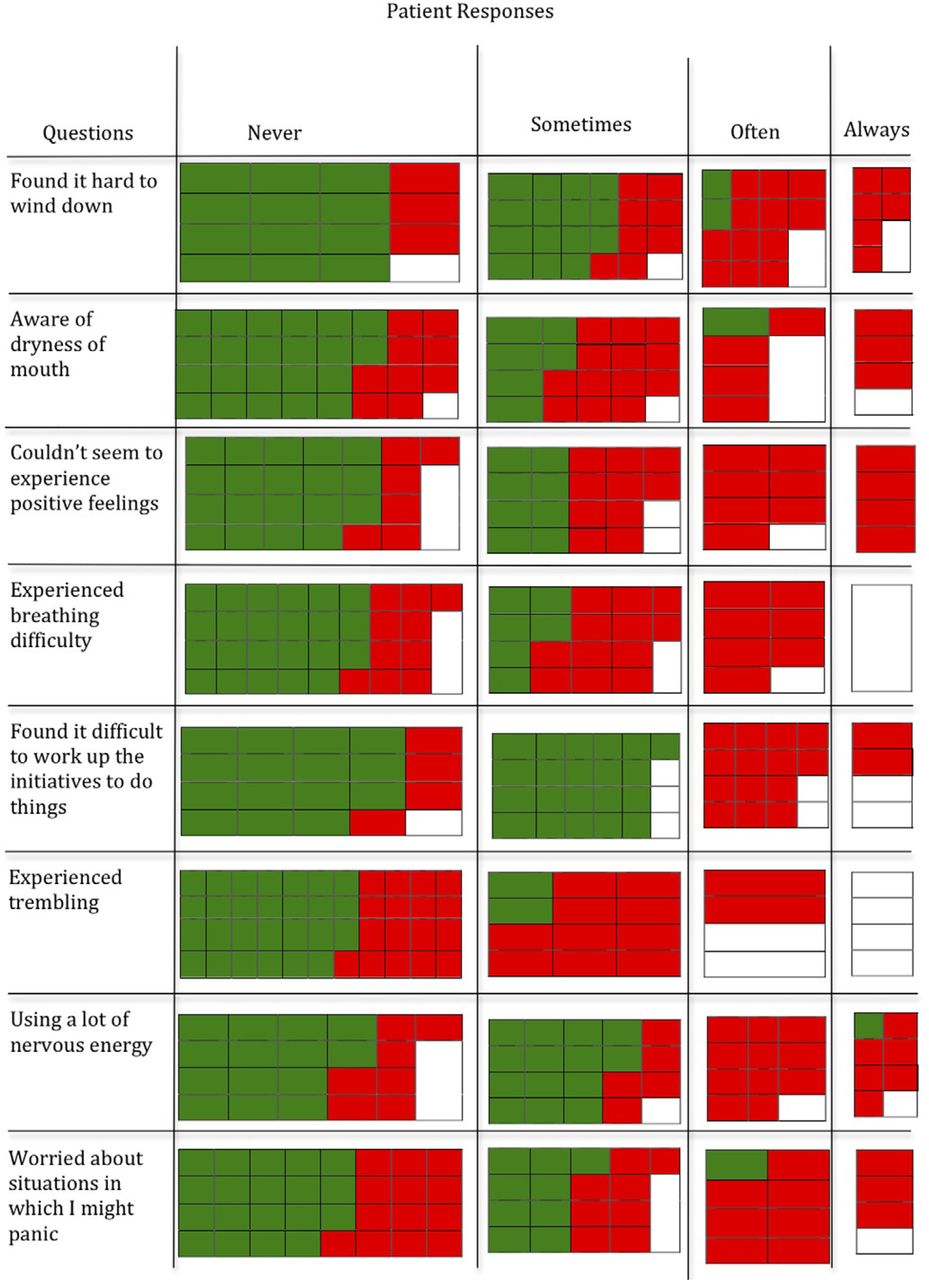
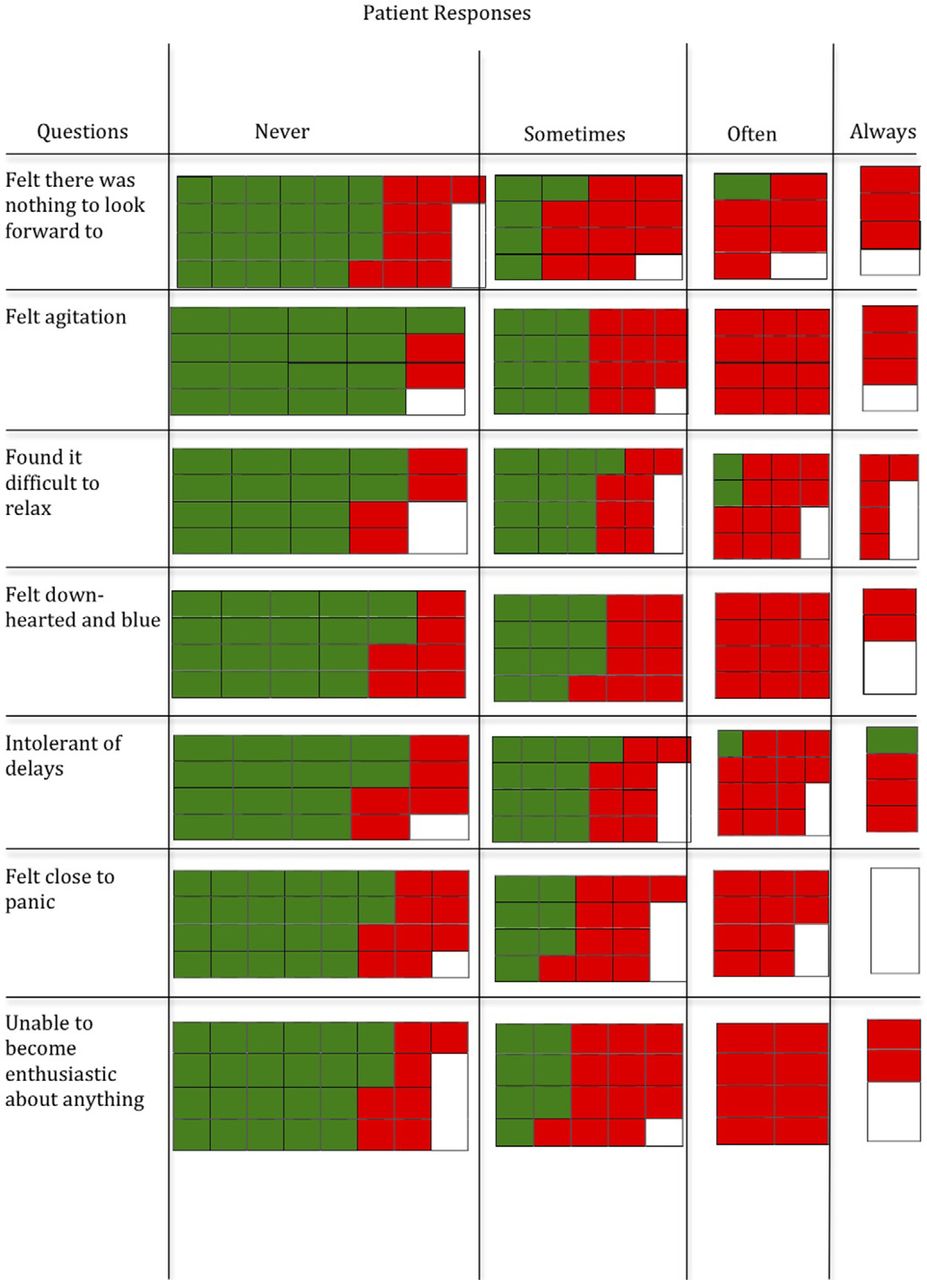
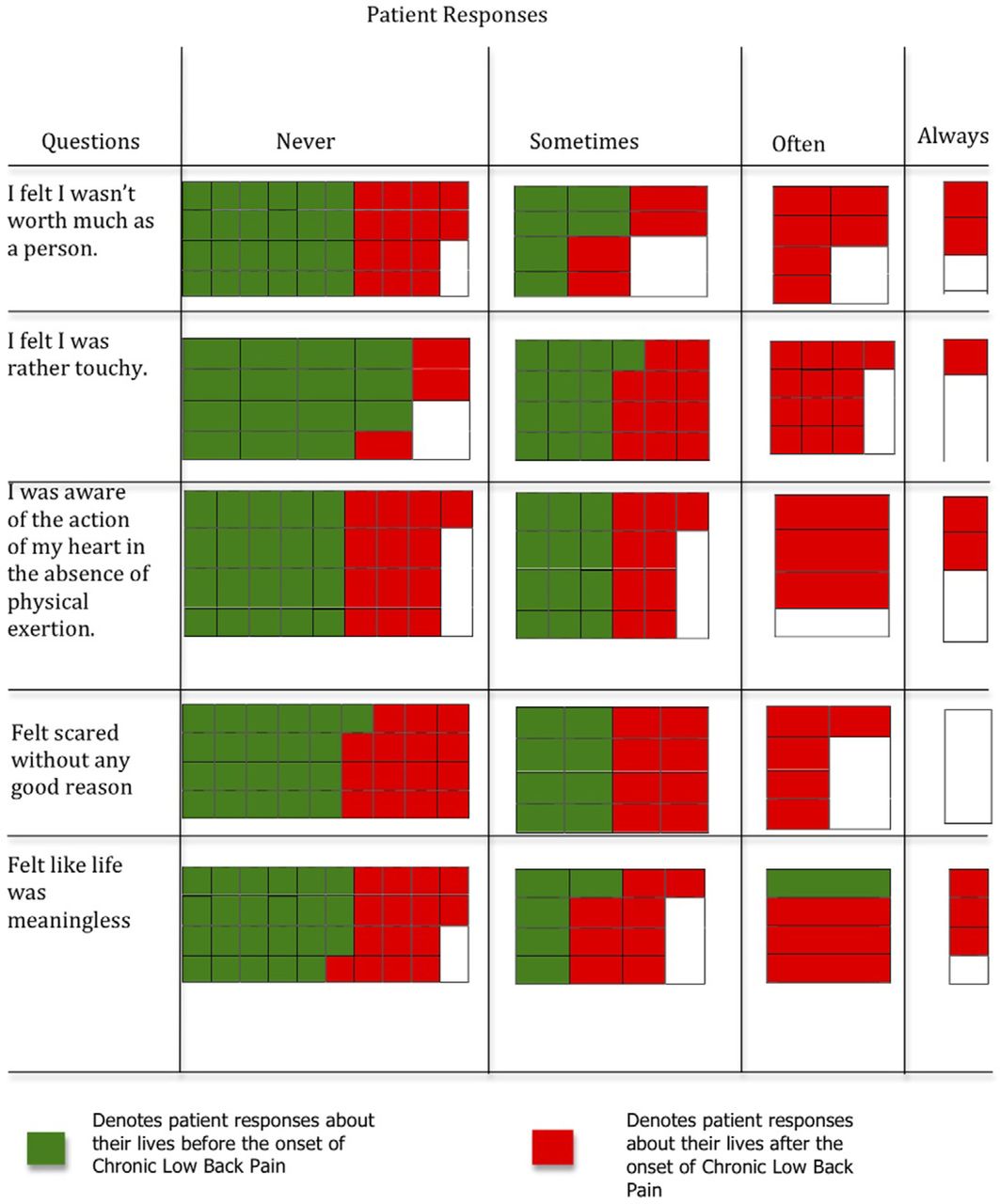
Individual responses to questions on the Depression Anxiety and Stress Scale before and after the onset of back pain are presented in a novel pictoarray (Fig. 3). This showed a rightward shift of response ratings after the onset of chronic low-back pain. The pictoarray analysis of the psychosocial profile detailing the specific answers shows that before the onset of chronic low-back pain, nearly all subjects indicated that they would respond to the Depression Anxiety

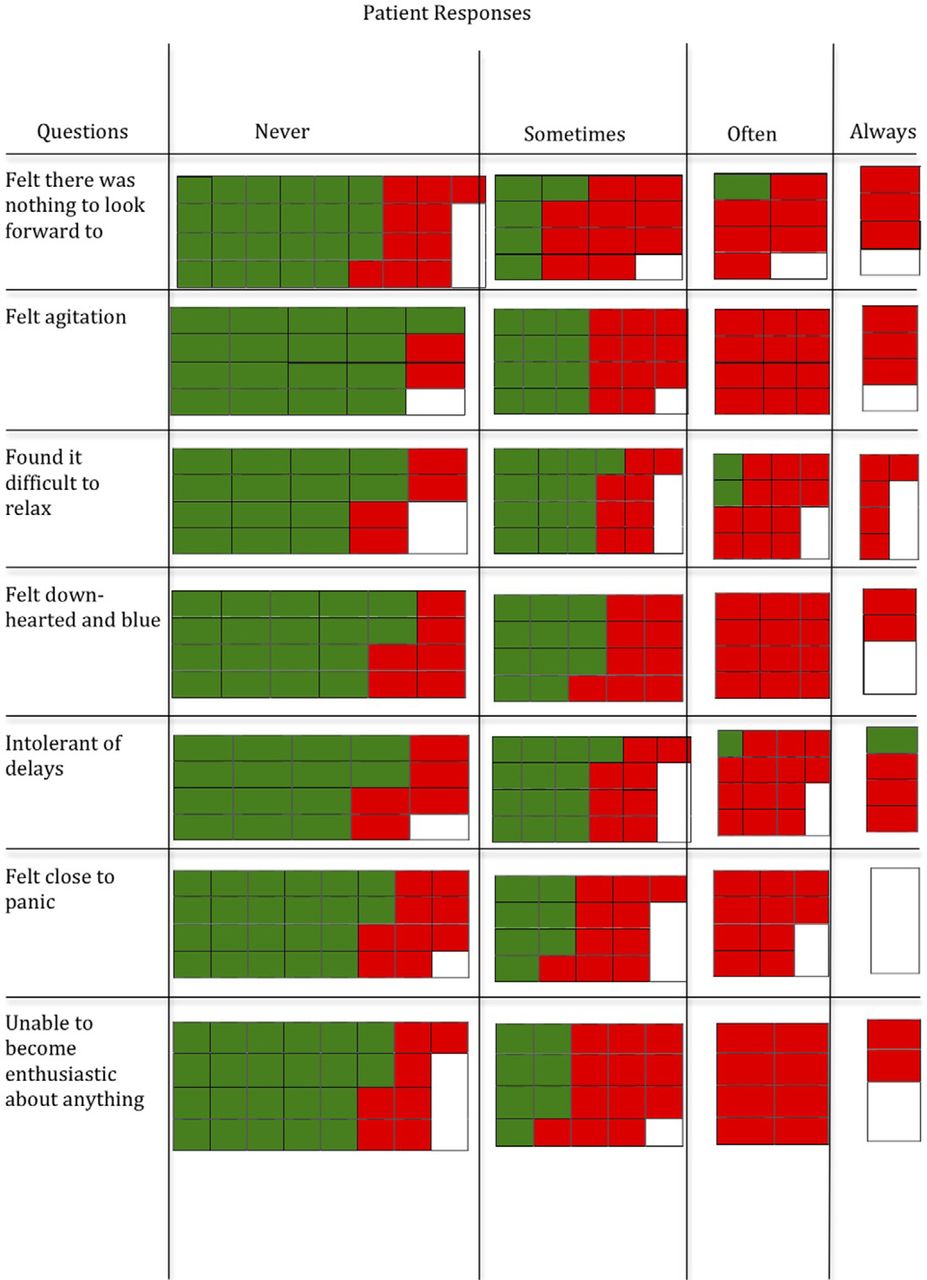

Visual representation of psychosocial profile differences before and after onset of chronic low-back pain.
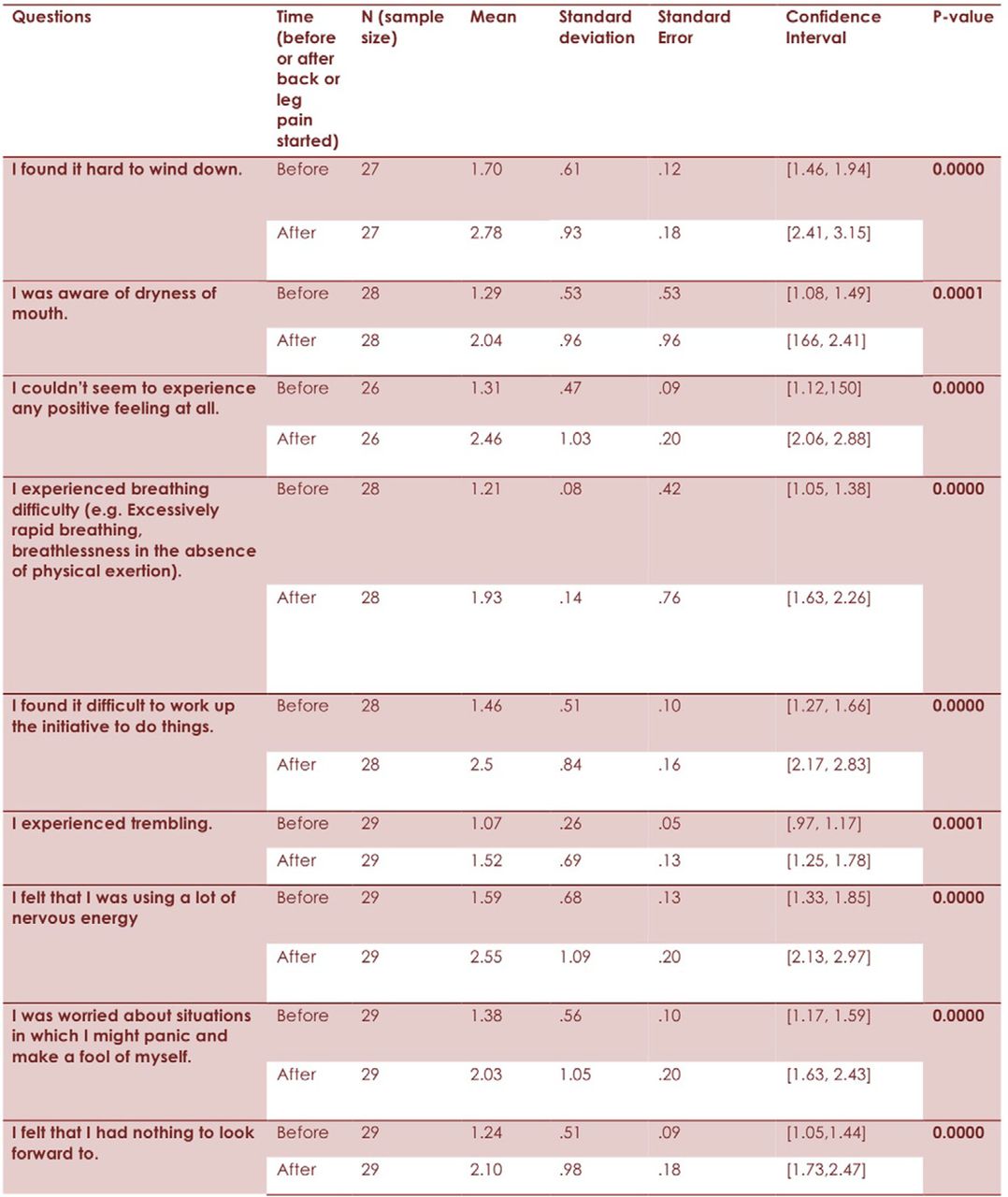
Stress Scale questions with “never” or “sometimes”; however, nearly all recorded answers of “often” or “always” corresponding to one's state after the onset of chronic low-back pain. The numeric equivalent of these responses shows a significant difference, where P < .01 for all 20 questions posed to subjects (Fig. 4). The responses indicate that there is a significant deterioration of patient mental states related to stress, depression, and anxiety after the onset of back pain.
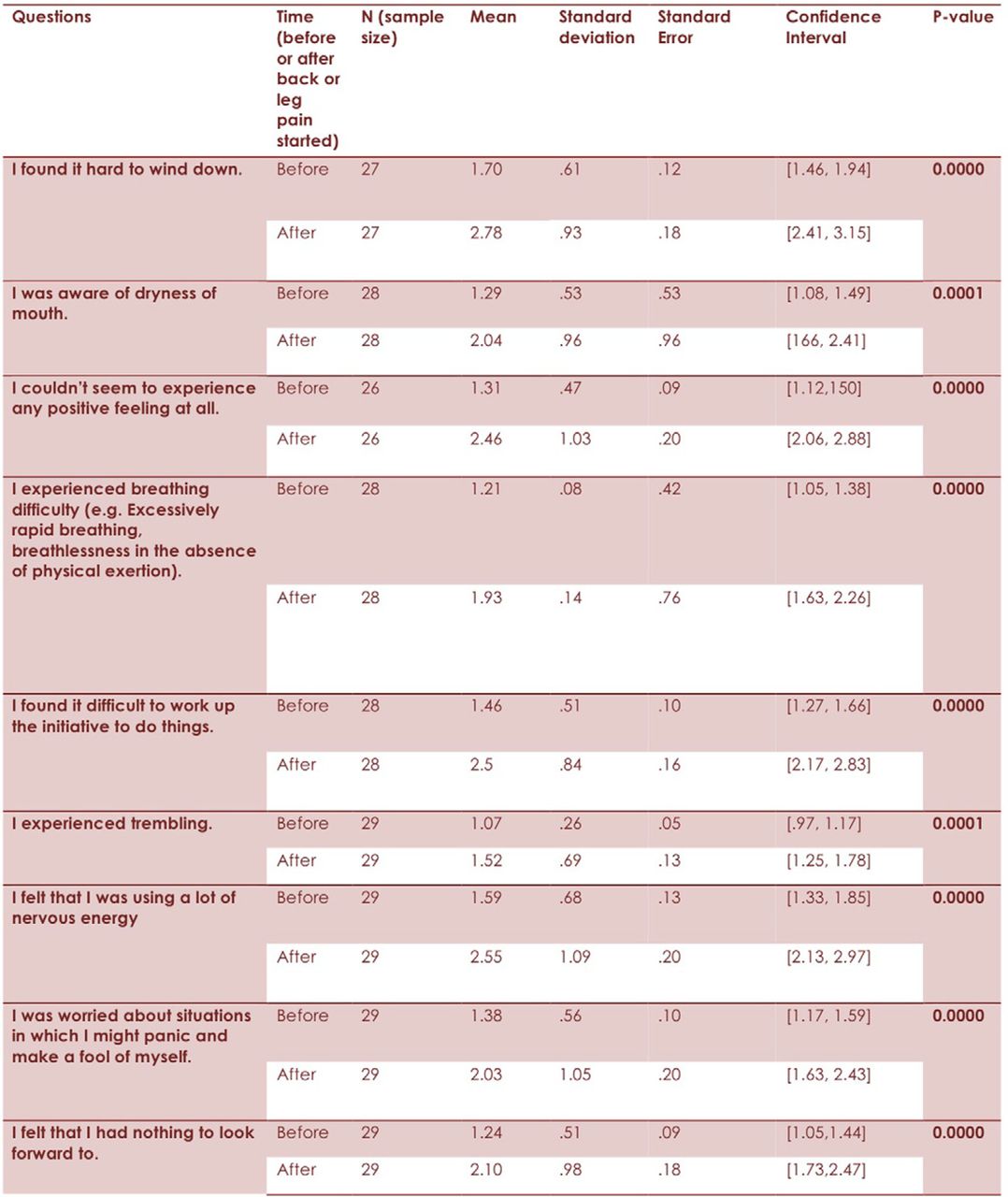

Statistical results of psychosocial profile questions before and after onset of chronic low-back pain. The psychosocial profile questions comprise statements primarily about an individual's mental health.
A.M. described being in constant pain, bedridden at times. Severe depression was not far off because he recalled, “I almost offed myself even.” Another subject, R.R., stated that her back pain would prevent her leaving bed. She felt guilty for no longer being able to contribute as much to her household or family business because of her injury. One of the greatest setbacks for her was the increased difficulty of pursuing her hobby, gardening. An hour of gardening caused her many hours of pain, but it was a pastime she refused to give up.
Social networks
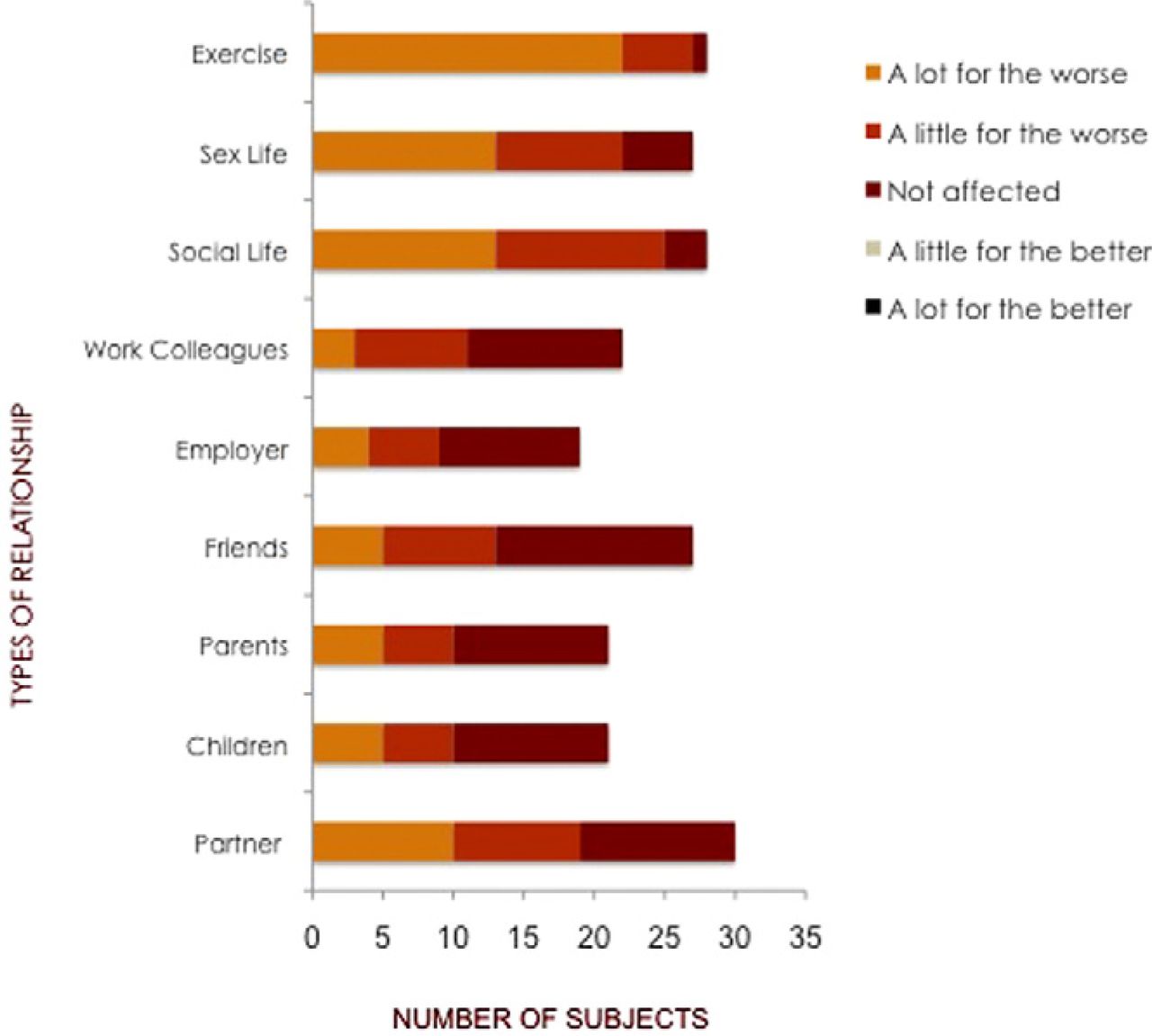
When asked about their relationships with their partners, one-third of subjects (10 of 30) said it had changed “a lot for the worse” and almost another third of subjects (9 of 30) said it had changed “a little for the worse” after the onset of chronic low-back pain as compared with their relationships with their partners before the onset of pain (Fig. 5). In response to open-ended questions, subjects commented on “tension in the relationship” created by the “emotional stress” of chronic low-back pain. When asked how their ability to engage in sexual activity had been affected, 50% of subjects (13 of 27) reported that their sex lives had changed “a lot for the worse,” whereas one-third of subjects (9 of 27) stated that it had changed “a little for the worse” after the onset of chronic low-back pain. Almost 20% of subjects (5 of 27) reported no change in their sex lives after the onset of back pain. No subject reported an enhanced ability to engage in sexual activity after the onset of back pain.

Perceived changes in various interpersonal relationships after onset of chronic low-back pain.
Nearly 50% of subjects (10 of 21) with children indicated that their relationships with their children had been affected for the worse after the start of their chronic low-back pain (Fig. 5). In response to open-ended questions, subjects commented on being unable to play with their children or grandchildren, being unable to sit, stand, run, or jump long enough to entertain the children after the onset of their back pain. They reported guilt at being unable to pick them up or to care for them properly after the pain started. One subject specifically commented on being “upset that children had to see their father like this.”
Approximately 50% of subjects (10 of 21) reported a relationship change for the worse with their parents after the onset of chronic low-back pain (Fig. 5). “Because I couldn't help around the house and they really didn't understand the pain I was going through, they would say I was lazy and I need to move more. It took a few years for them to understand,” described one subject. Another subject reported feeling “more pressure to fix her back pain” because of the stress and worry voiced by her parents. Other comments included feelings of guilt at being unable to care for older parents, as well as guilt at having to ask for money from their parents after the onset of chronic low-back pain.
Approximately 20% of subjects (5 of 27) reported that their relationships with their friends had changed “a lot for the worse” since chronic low-back pain began, whereas approximately one-third of subjects (8 of 27) reported that their relationships had changed “a little for the worse” (Fig. 5). Subjects cited irritability and an inability to travel long distances without pain as reasons that prompted a decrease in outings and other social events with their friends after the onset of chronic low-back pain. Accordingly, approximately 50% of subjects (13 of 28) reported a change “a lot for the worse” in their social lives, whereas over 40% of subjects (12 of 28) reported a change “a little for the worse” in their social lives since the beginning of their back pain.
Almost 50% of subjects (9 of 19) reported a change for the worse in their relationships with their employers, whereas another 50% of subjects (11 of 22) reported a change for the worse with their colleagues since the onset of their pain (Fig. 5). Subjects cited their poor attendance records as a point of tension between themselves and their employers, as well as their colleagues, who were often asked to do additional work because of the subjects’ back pain–related absences. Subjects also cited a disconnect between themselves and their colleagues because the subjects were often unable to attend workplace social events after their pain started. Also noted by subjects in response to open-ended questions were feelings of agitation and irritability at work after the onset of chronic low-back pain, which affected both concentration and attitude in dealing with others at their workplaces.
F.L. mentioned not being around people much anymore because it has become increasingly difficult to go out with friends or invite them over. Her nearest family is a 6-hour drive away. She has given up on the prospect of getting married and now worries most about her work-related performance.
A.M., injured on his job as a tour guide assisting a client out of a shuttle bus, attributes the demise of his marriage to his injury: “It ruined my marriage and ruined my life.”
Discussion
The study shows that after the onset of chronic low-back pain, there was an adverse impact on subjects’ finances, productivity, psychological health, and social networks.
After the onset of chronic low-back pain, subjects incur additional medical costs for extra treatments including, but not limited to, injections, investigations, and surgeries. Given the chronic nature of the condition in these subjects, presenting for tertiary care results in additional monetary costs, as well as the physical and mental costs of traveling for long periods in pain.
Productivity was adversely affected after the onset of chronic low-back pain at both the individual level and the macroeconomic level. Individual subjects lost full pay or opportunities for career advancement. Subjects used their days of absence for medical appointments for their chronic low-back pain, leaving themselves with few or no options to take days of absence for other reasons, such as caring for a sick child or parent, funerals, vacations, or sickness unrelated to their chronic low-back pain. Meanwhile, economies lost sources of productivity while still having to pay partial incomes.
The study shows a direct negative impact on the psychological health after the onset of chronic low-back pain. Subjects in the study have greater scores on the Depression Anxiety and Stress Scale, indicating that their psychological states have worsened. Typically, these adverse changes in mental health parallel declines in physical health as well because immunity is subject to mood and mental wellbeing.
A number of questions underscored the adverse effects on individuals’ social networks. Individuals with chronic low-back pain cited numerous costs, including the inability to play with children and grandchildren, gratuitous guilt over being unable to contribute to society, and the inability of close relatives to understand the reality of their pain. The cumulative effect of individual chronic low-back pain is an adverse, macrosocial effect. It is costs like these that are underrepresented in the field of chronic low-back pain, as well as in other areas of specialized medicine and pain management. It is costs like these that constitute the true costs of chronic low-back pain—the costs only the patients ever know about.
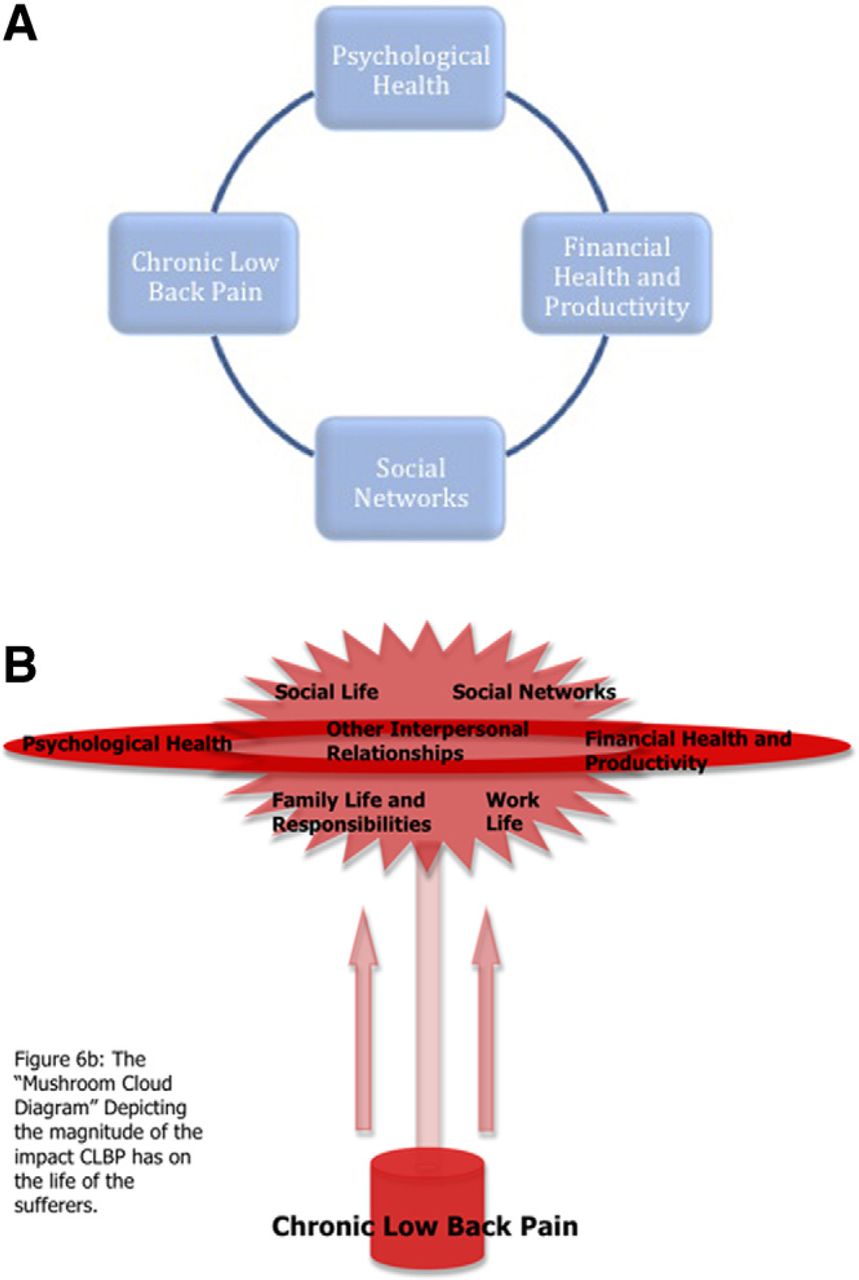
That the circles of human biology, psychology, social networks, and finances are connected is a ubiquitous view in health care—no less true in the world of chronic low-back pain. The current view asserts that a change in one will cause a subsequent change in all the other circles (Fig. 6A). However, the results of this study compel us to argue that this view is not entirely accurate. The results of this study show that subjects have problems in all 4 major areas: finances, productivity, psychological health, and social networks. The current model shows a series of connected circles depicting each issue as affecting the others equally. We argue that the relationship of back pain to finances, productivity, psychological health, and social networks more closely resembles a mushroom cloud in which chronic low-back pain is akin to a bomb that detonates, creating the subsequent cloud of problems spilling over into all areas of life (Fig. 6B). This model offers a more appropriate weighting scheme because the ensuing problems stem directly from the chronic low-back pain. The alternative models are flawed in illustrating a dynamic web of interrelated factors; these models overlook chronic low-back pain's role as the operative factor generating the others.
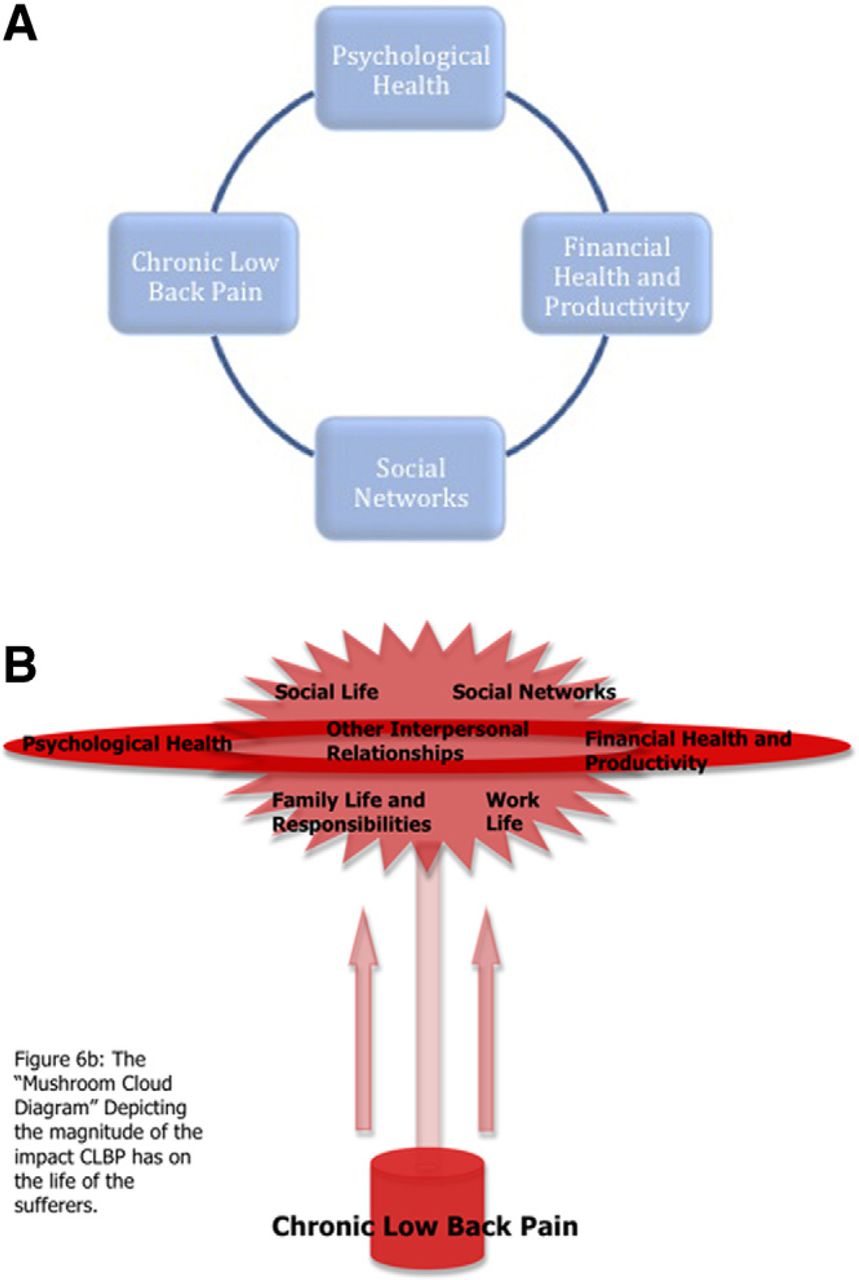
(A) Representation of currently held view of chronic low-back pain, in which chronic low-back pain, financial health, psychological health, and social networks all have an equal effect on each other. According to this view, a change in any 1 field will impact the other 3 realms to the same degree. (B) Mushroom-cloud diagram, depicting the magnitude of the impact chronic low-back pain has on the life of the patients.
One may argue that the small sample size of the study, as well as the use of subjects referred to a tertiary spinal care center—subjects who were already in tremendous amounts of pain—may weaken the study. However, the statistical significance of the results, especially with regard to the psychosocial profile, is unequivocal. The skewed results indicate that a larger sample size is not necessary to suggest a strong, negative change after the onset of chronic low-back pain. Another criticism of this study is the potentially large bias of the results because they are based on patient recall. Despite the reliance on patient recall, a large portion of the results address the psychological harm that results from chronic low-back pain. The perception of harm corroborates psychological harm. Coupled with the difficulty of obtaining more objective forms of data, patient recall is held as adequate for the purposes of the study.
Schofield et al12 defined poverty as a household income (unit) being below 50% of the national median. Using the Survey of Disability, Aging and Carers data collected by the Australian Bureau of Statistics, they discovered that 72% of the people not in the labor force because of chronic low-back pain were poor, as opposed to 55% who were not in the labor force because of other chronic disorders, whereas only 21% of people who were employed part time and had no chronic illness were poor. Although the data of Schofield et al show the extent to which chronic back pain contributes to the malaise of poverty, our study shows how this occurs gradually but in many domains in a cohort of individuals after the onset of back pain.
Future areas of study may involve studies of larger cohorts of patients selected randomly from different clinical settings. In addition, studies focusing on a progression of chronic low-back pain over time will shed light on management of the condition over time. Studies probing ulterior and other indirect costs will also be fruitful; specifically, studies focusing on questioning the relatives of subjects with chronic low-back pain will elucidate the costs of chronic low-back pain to family members.
Acknowledgments
Dr Thomas D. Cha acted as the Harvard Faculty Mentor on this project, providing support and working with the authors to make funding for the project possible. Dr Abby Bloom acted as a mentor for Sally Garis in the early stages of the study. Milowa Rodriguez provided assistance in enhancing the quality of the figures presented in this article.
Footnotes
The Harvard Global Health Initiative provided funds to Justin Mathew and Samantha Singh, and Synthes Asia Pacific provided a research grant to the University of New South Wales for this study.
Justin Mathew, Samantha Singh, and Sally Garis contributed equally to this article.
- © 2013 Published by Elsevier Inc. on behalf of ISASS - International Society for the Advancement of Spine Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.