


Abstract
Background Whether kyphoplasty or vertebroplasty is better for painful osteoporotic vertebral compression fracture is a widely debated issue. Studies on the comparison of the 2 approaches are relative limited and a wide variation exists in the patient population, study design, and results. These factors make it difficult for workers in this field to know the exact value of the 2 approaches.
Objective To perform a systematic review and meta-analysis to compare the clinical outcomes and complications of kyphoplasty versus vertebroplasty for painful osteoporotic vertebral compression fractures (OVCF).
Study design A systematic review and meta-analysis.
Methods MEDLINE, EMBASE, and other databases were searched for all the relevant original articles published from January 1987 to September 2012 comparing kyphoplasty with vertebroplasty for painful OVCF. The following outcomes were mainly evaluated: visual analog scale (VAS), vertebral height, kyphosis angle, new vertebral fractures, and cement leakage.
Results A total of 15 articles fulfilled all the inclusion criteria. The baseline characteristics such as sex, age, and number of prevalent fractures were comparable for both groups (P > .05). VAS score for the kyphoplasty group was significantly more than that for the vertebroplasty group at 1-3 days, 3 months, 6 months, 1 year, and 2 years after surgery (P < .05). Vertebral height in the kyphoplasty group was significantly higher than the vertebroplasty group at 3 months, 6 months, and 2 years (P < 0.05). Kyphosis angle in the kyphoplasty group was significantly lower at 3 months, 6 months, and 2 years (P < 0.05). The occurrence of new vertebral fractures in the kyphoplasty group had no significant difference with the vertebroplasty group at 3 months, 6 months, and 2 years (P > 0.05). The occurrence of cement leakage was significantly lower in the vertebroplasty group (P < 0.05).
Limitations The main limitations of this review are that the demographics and comorbidities of study participants were not reported. These possible sources of heterogeneity could not be examined.
Conclusions Percutaneous kyphoplasty is better than vertebroplasty in the treatment of painful OVCF. Kyphoplasty had better improvement at VAS score, vertebral height, and kyphosis angle with lower occurrence of cement leakage.
Osteoporotic vertebral compression fractures (OVCF) are one of the most common skeletal fractures1 and are increasing in frequency in our ageing population because of the growing prevalence of osteoporosis. Vertebral fractures often result in significant pain that often leads to decreased mobility, loss of independence, and subsequent loss of bone density associated with inactivity. Vertebral fractures can also have negative effects on the respiratory and digestive systems owing to resultant postural deformity.2 There is a significant increased mortality rate in patients with vertebral fractures treated conservatively compared with age-matched controls in the literature.3 The 5-year survival rate for patients with compression fractures is 61%, as compared with 76% in age-matched peers.4
The treatment for OVCF is essential, but it is a difficult problem. The traditional conservative treatments such as bed rest, pain-killers, and osteoporosis drugs and the use of orthopedic appliances, etc,1 can cause hypostatic pneumonia, bed sores, urinary tract stones or deep vein thrombosis, which increase the suffering of the patients,5 and cannot improve the vertebral height of the fractured. The open surgery such as posterior short-segment pedicle screw fixation may lead to bigger surgical trauma, longer surgical time, and more blood loss. Because of osteoporosis, the grip force for pedicle screw is not strong enough. The internal fixation is prone to loosening, displacement, or settlements which often lead to fixation failure.4, 6 Therefore, open surgery is a relative contraindication for patients with OVCF.
Since the late 1980s, 2 minimally invasive surgical treatments: vertebroplasty (VP) and kyphoplasty (KP) have been gradually introduced that changed the treatment of OVCF. In 1987, Galibert et al.7 used vertebroplasty for the first time to treat vertebral hemangioma, and later in 1988, percutaneous vertebroplasty (PVP) was widely used in primary and secondly painful osteoporotic vertebral fractures around the world.8 Guided by X-Ray, vertebroplasty involves injecting polymethylmethacrylate (PMMA) bone cement into the fractures of the vertebral body percutaneously to enhance the strength of the vertebra and stiffness and prevent further vertebral collapse and deformity, and effectively relieve pain. Kyphoplasty was introduced in 1998 as an alternative. Unlike VP, it created a cavity in the vertebral body with a balloon (inflatable bone tamp) before injecting PMMA bone cement. Both PVP and percutaneous kyphoplasty (PKP) can quickly relieve spinal compression fractures in osteoporotic patients with pain, reduced analgesic drug dependence and improve the quality of life in patients with OVCF.1–7, 9 PVP and PKP become the main surgical treatment for OVCF patients.
Although extensive research on the 2 approaches has been done, no consensus has been reached as to whether kyphoplasty or vertebroplasty is better. Furthermore, studies on the comparison of the 2 approaches are relatively limited and a wide variation in patient population, study design, and results exists. These factors make it difficult for workers in this field to know the exact value of the 2 approaches. Meta-analysis represents a powerful tool to summarize the findings in the literature by taking into account and enabling analysis of the differences between studies.10, 11 Thus, the purpose of our study is to perform a systematic review and meta-analysis to compare the clinical outcomes and complications of kyphoplasty versus vertebroplasty for painful OVCF.
Materials and methods
Literature search
A comprehensive computer literature search of abstracts12 of studies in human subjects was performed to identify articles about kyphoplasty and vertebroplasty for painful OVCF. The MEDLINE and EMBASE databases, from January 1987 to September 2012, were searched with the following keywords: (“Kyphoplasty” OR “Vertebroplasty”). No language restrictions were applied.
Other databases, such as Web of Knowledge, EBSCO, ScienceDirect, SpringerLink, Scopus, and The Cochrane Library, were also checked for relevant articles with the same keywords. We also searched the abstracts of American Academy of Orthopaedic Surgeons annual meeting (2006–2011: <http://www.aaos.org/education/anmeet/libscip.asp>). The list of articles was supplemented with extensive cross-checking of the reference lists of all retrieved articles.
Selection of studies
Two reviewers (L.T. and X.W.) independently assessed potentially eligible studies. The study selection was accomplished through 2 levels of study screening. At the level 1 screening, abstracts were reviewed for the following exclusion criteria: case reports, letters, editorial, comments, reviews, and articles that did not include raw data. Full articles were then obtained for all studies accepted at level 1 screening and any citations for which a determination could not be made from the abstract. If the study was not reported in full journal publications, we contacted the authors for the full text or additional information needed. For level 2 screening, the inclusion criteria were as follows: any randomized, quasi-randomized controlled clinical trials, prospective or retrospective cohort study of KP versus VP for painful OVCF in adults.1, 2 The aim of the study was to compare KP with VP for painful OVCF.3 The patients included were all patients with OVCF. If the study included not only patients with OVCF but also other patients, such as those with metastasis, only patients with OVCF were selected if the results could be differentiated. When data or subsets of data were presented in more than one article, the article with the most details or the most recent article was chosen. The studies were excluded if the results were presented in combination and could not be differentiated for performance assessment.
Data extraction
The same observers independently extracted relevant data from each article by using a standardized form. Observers were not blinded with regard to the information about the journal name, the authors, the authors’ affiliation, or year of publication, as this had been shown to be unnecessary.13 To resolve disagreement between reviewers, a third reviewer (C.T.) assessed all discrepant items, and the opinion of the majority was used for analysis.
Common characteristics about studies
Author's country; year of publication; number of patients; mean age; study design; research center; and duration of fracture.
Study design characteristics
A methodological quality assessment scheme recommended by the Cochrane library14 was used to extract relevant study design characteristics for each study. In this scheme, there are 11 items and the answer to each item was graded as “Y,” “?,” or “N,” respectively indicating that the quality criteria were met for the item (“yes”), or possibly or only partially met for the item (“Possible, partial”), or not met (“No”).
Clinical characteristics about studies
Perioperative outcomes: these included volume of cement and operative time.
Clinical outcomes: these included VAS, Oswestry Disability Index (ODI), and Euro Quality of Life–5 Dimensions (EQ-5D).
Radiographic outcomes: these included vertebral height (mm), vertebral height rate (%) (It was expressed as the percentage of the vertebra height for the fractured vertebra compared with the height for the adjacent normal vertebrae(%)), and kyphosis angle.
Complications outcomes: these included adjacent new vertebral fractures and cement leakage.
The primary outcomes were VAS, vertebral height, kyphosis rate, adjacent new vertebral fractures, and cement leakage.
Subgroup analysis
Analysis of the outcomes was divided to subgroups according to the time of outcome assessment, if possible. The times of outcome assessment were 1 day, 3 days (or 1– 3 days), 1 week, 2 weeks ( or 1–2 weeks), 1 month, 2 months, 3 months, 6 months, 1 year, and 2 years.
Statistical analysis
Common characteristics were summarized by using basic descriptive statistics (simple counts and means). Clinical characteristics were synthesized via meta-analytic pooling of each group results. Meta-analysis was performed in line with recommendations from the Cochrane Collaboration and the Quality of Reporting of Meta-analyses guidelines.15–17 Statistical analysis of dichotomous variables was carried out using odds ratios (ORs) as the summary statistic, whereas continuous variables were analyzed using the weighted mean difference (WMD); both were reported with 95% confidence intervals (CIs). The Mantel-Haenszel method was used to combine the ORs and the inverse-variance method was used to combine the WMDs for the clinical characteristics.
Heterogeneity was assessed by χ2 test and the I 2 statistic. A fixed-effects model was used to calculate summary statistics if no statistically significant (P < .05) heterogeneity was found among similar comparisons, whereas if statistically significant (P > .05) heterogeneity was found, a random-effects model was used. We constructed a funnel plot to explore the possibility of publication bias. All P values are 2 sided. Results were considered to be statistically significant at a P value of less than 0.05.
All analyses were performed by using Microsoft Excel 2003 (Microsoft, Seattle, Wash), SPSS 13.0 for Windows (SPSS, Chicago, III), and RevMan5.0 (Review Manager (RevMan) [Computer program]. Version 5.0. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2008.). RevMan5.0 is a freeware software produced by The Cochrane Collaboration, and can be downloaded from the website “<http://www.cc-ims.net/RevMan/RevMan5>.”
Results
Literature search and selection of studies
After the computerized search was performed and reference lists were extensively cross-checked, about 3034 abstracts were identified. Of these, 2951 were rejected after level 1 screening (reviewing the abstracts). Of the remaining 83 articles, 67 relevant articles were excluded after we read the full texts or additional information of these articles because (a) the articles were not randomized, quasirandomized controlled clinical trials, perspective, or retrospective cohort study (n = 50); (b) The aim of the articles was not to compare KP with VP for painful OVCF (n = 9); (c) The patients included were not patients with OVCF or the relevant data could not be extracted (n = 4); (d) The studies did not include raw data (n = 5). At last 15 articles18–32 including 15 studies fulfilled all the inclusion criteria and were selected for data extraction and analysis.
Common characteristics of studies
The studies took place in one of 9 countries (China,3 Australia,1 Canada,1 Spain,1 Japan,1 Germany,3 Italy,3 USA,1 and Slovenia1. All the studies were single-center studies including 1RCT, 5 NRCT, 4 prospective cohort studies, and 5 retrospective cohort studies. There were total 1151 patients in the selected studies. Of them, 627 patientss were treated by vertebroplasty and 524 patients underwent kyphoplasty. The age ranged from 62 to 78 years for the vertebroplasty group and 64 to 76.9 years for the kyphoplasty group.
Table 1 presents the detail information about the common characteristics of the included data sets.
Common characteristics about the included data sets
Study design characteristics
Most studies had a suboptimal design with regard to treatment concealment (question 1:93.3% for “no” responses), the intention to treat analysis (question 2:93.3% for “no” and “?” responses), outcome assessors blind (question 3:80% for “no” responses), and doubleblind (questions 5 and 6, 100% for “no” and “?” responses). But, as for baseline characteristics, care programmes other than the trial options, inclusion and exclusion criteria, outcome measures and follow-up time etc, most studies were optimally designed (60% for “yes” responses to question 4; 53% to question 7; 60% to questions 8 and 9; 86.7% to questions 10 and 11). In fact, questions 1–3 and 5–6 were more concerned with study method whereas questions 4 and 7–11 were more concerned with clinical data, so questions 4 and 7–11 were more important. If the studies were ideally designed according to these questions, the clinical result would be correct and credible.
Table 2 presents the detail information about study design characteristics of the included data sets.
Study design characteristics of the included data sets
Perioperative outcomes
(1) Volume of cement
The volume of cement injected for the vertebroplasty group was significantly less than the kyphoplasty group (P < .05, WMD −0.75 [−0.93, −0.57]).
(2) Operative time
The operative time for the vertebroplasty group was significantly less than the kyphoplasty group (P < .05, WMD −3.44 [−4.94, −1.94]).
Table 3 presents the results of meta-analysis of perioperative outcome measures.
Results of meta-analysis of perioperative outcome measures
Clinical outcomes
(1) VAS
At baseline, the VAS score was similar in both groups (P > .05, WMD 0.14 [−0.01, 0.28]). At 1–3 days, 1–2 weeks, 1 month, 3 months, 6 months, 1 year, and even 2 years after operation, the VAS score for the vertebroplasty group was significantly more than the kyphoplasty group (P < .05, WMD was 0.18 [0.02, 0.34], 0.45 [0.15, 0.75], 0.42 [0.14, 0.70], 0.89 [0.72, 1.06], 1.24 [1.07, 1.41], and 1.01 [0.41, 1.60], respectively) (Fig. 1).

The forest plots of meta-analysis of VAS score.
(2) ODI
ODI: The ODI for the vertebroplasty group was significantly more than that for the kyphoplasty group at baseline (P < .05,3.56 [1.61, 5.51]). At 1 week 1 month, 3 months, and 1 year after operation, it was also significantly more than that of the kyphoplasty group (P < .05, WMD was 10.40 [8.06, 12.74], 2.82 [0.72, 4.91], 4.31 [1.95, 6.67], and 4.43 [−1.27, 10.13] respectively). At 6 months and 2 years after operation, there was no significant difference between both groups (P > .05, WMD was 0.45 [−0.82, 1.72] and −4.00 [−11.57, 3.57], respectively).
(3) EQ-5D
The EQ-5D score for the vertebroplasty group was significantly less than the kyphoplasty group at baseline, 1 week, 3 months, and 10 months after operation (P < 0.05, WMD was −0.08 [−0.12, −0.03], −0.37 [−0.41, −0.33], −0.15 [−0.18, −0.12], and −0.24 [−0.28, −0.21] respectively).
Table 4 presents the results of meta-analysis of clinical outcome measures.
Results of meta-analysis of clinical outcome measures
Radiographic outcomes
(1) Vertebral height (mm)
The vertebral height for the vertebroplasty group was similar to that of the kyphoplasty group at baseline (P > 0.05, WMD 0.06 [−0.22, 0.33]), but after the operation, it was significantly less than that of the kyphoplasty group (P < 0.05, WMD −2.38 [−2.67, −2.08). The improvement in the vertebral height for the vertebroplasty group was significantly less than the kyphoplasty group (P < .05, WMD −2.00 [−2.75, −1.25]).
(2) Vertebral height rate (%)
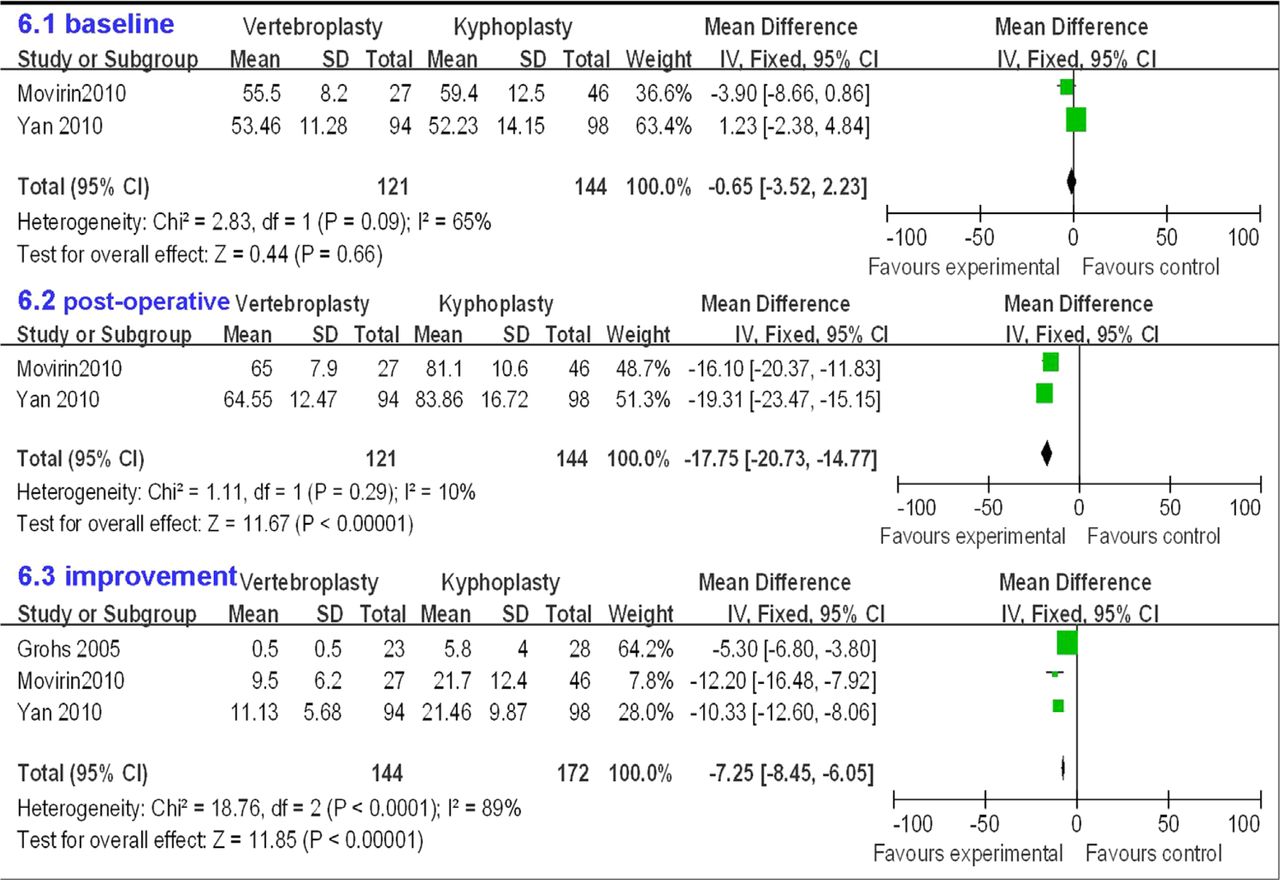
The vertebral height rate for the vertebroplasty group was similar to the kyphoplasty group at baseline (P > .05, WMD −0.65 [−3.52, 2.23]), but after the operation, it was significantly less than the kyphoplasty group (P < 0.05, WMD −17.75 [−20.73, −14.77]). The improvement in the vertebral height rate for the vertebroplasty group was significantly less than the kyphoplasty group (P < 0.05, WMD −7.25 [−8.45, −6.05]) (Fig. 2).
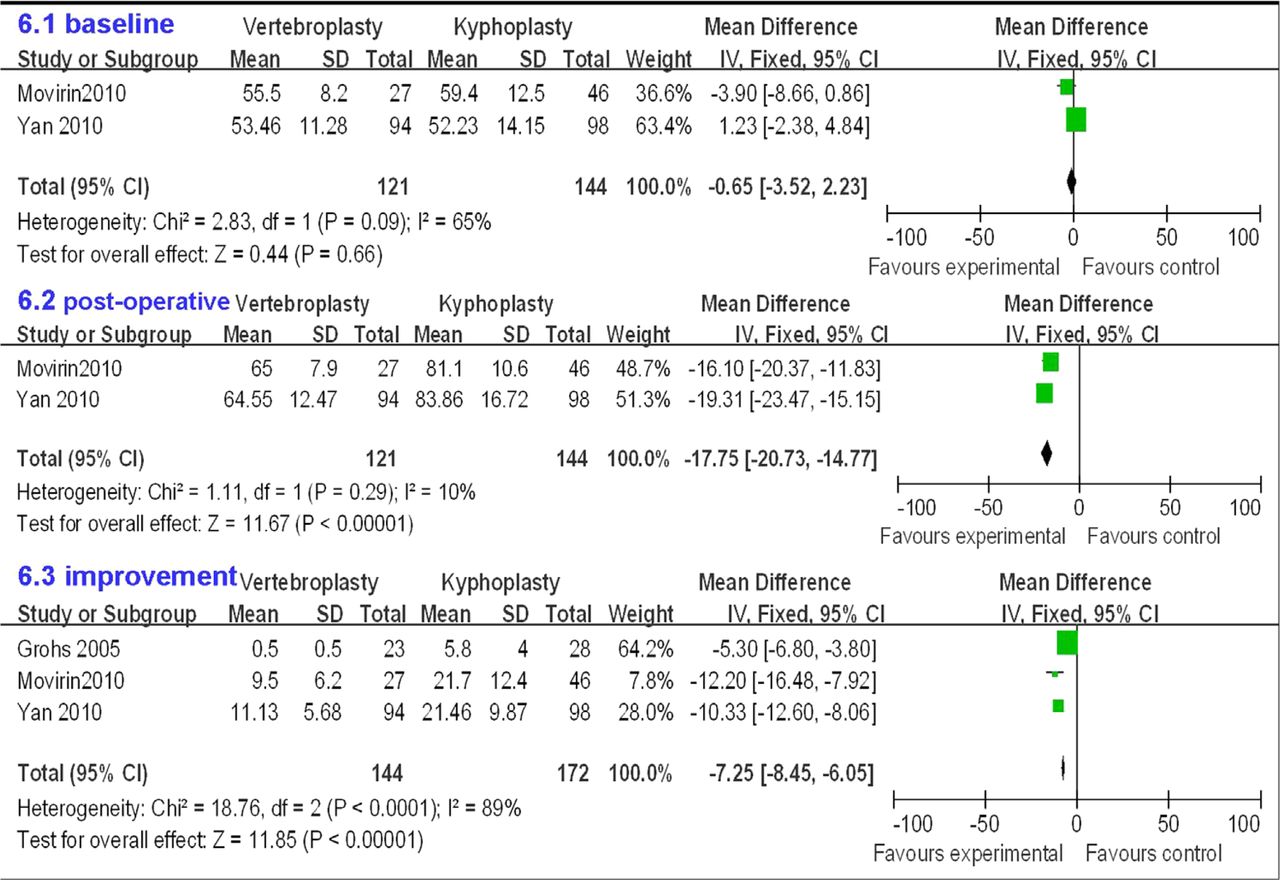
The forest plots of meta-analysis of vertebral height.
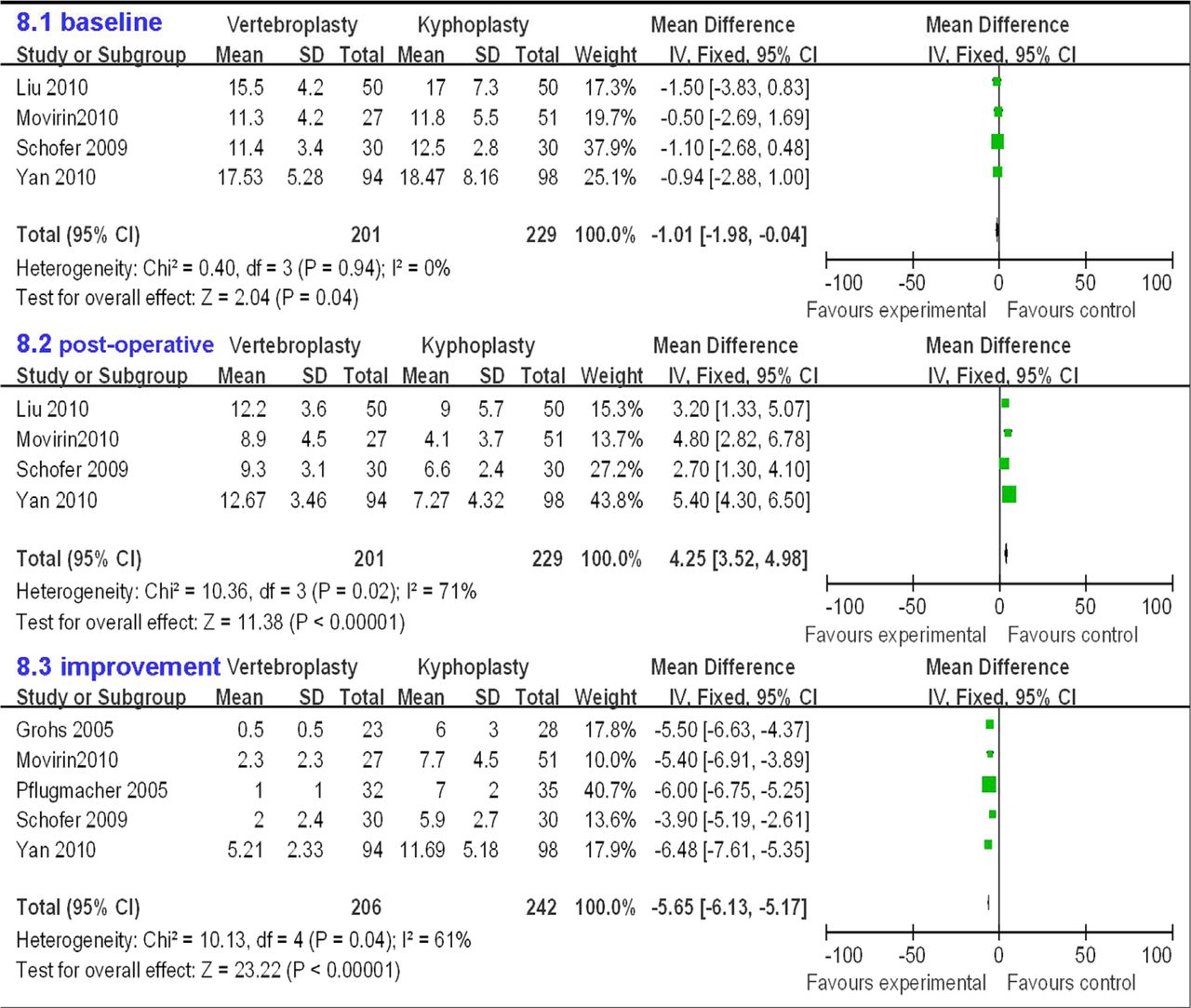
(3) Kyphosis angle
The kyphosis angle for the vertebroplasty group was similar to the kyphoplasty group at baseline (P > .05, WMD −1.01 [−1.98, −0.04]), but after the operation, it was significantly more than the kyphoplasty group (P < 0.05, WMD 4.25 [3.52, 4.98]). The improvement in the kyphosis angle for the vertebroplasty group was significantly less than the kyphoplasty group (P < .05, WMD −5.65 [−6.13, −5.17]) (Fig. 3).
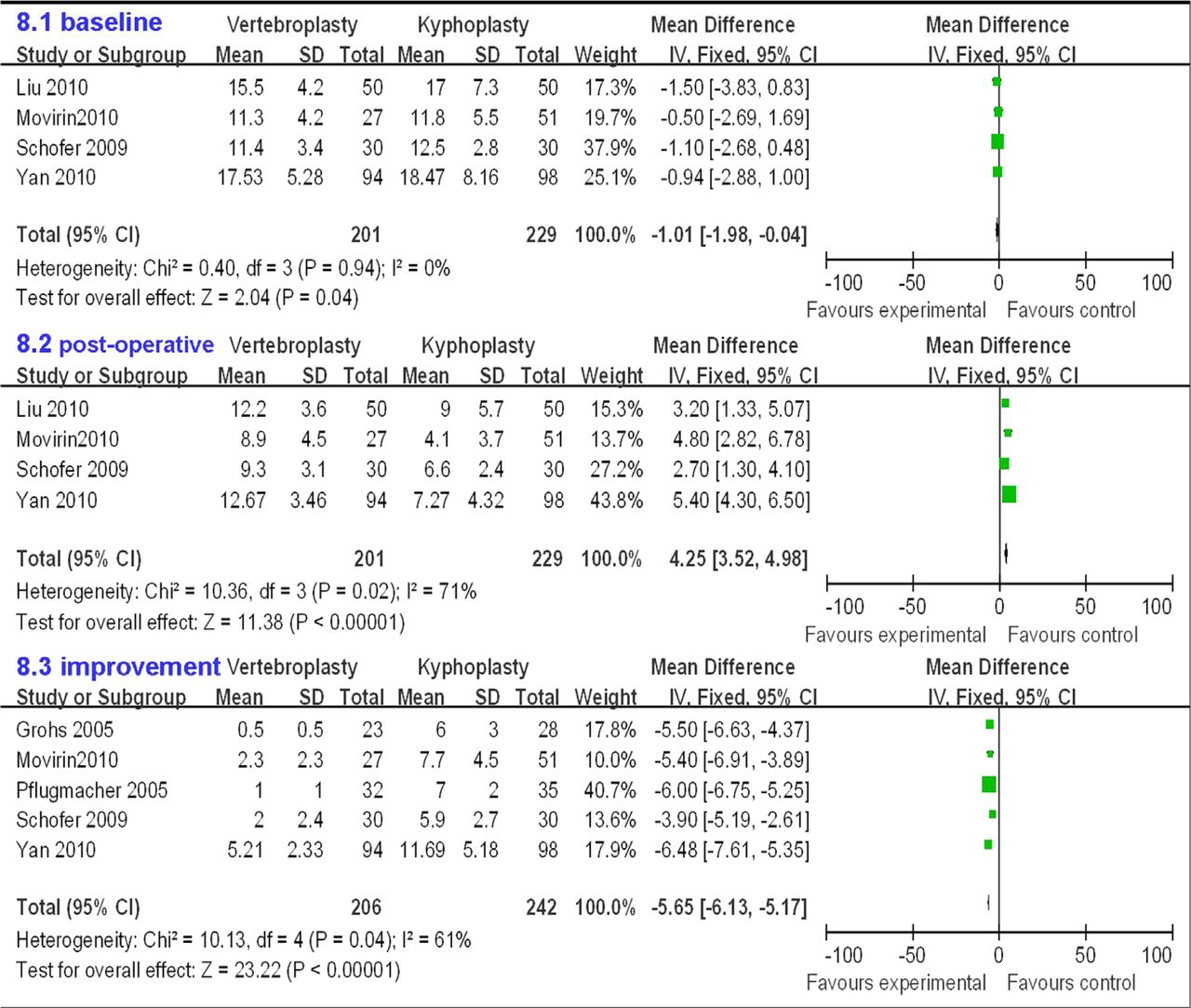
The forest plots of meta-analysis of kyphosis angle.
Table 5 presents results of meta-analysis of radiological outcome measures.
Results of meta-analysis of radiological outcome measures
Complications outcomes
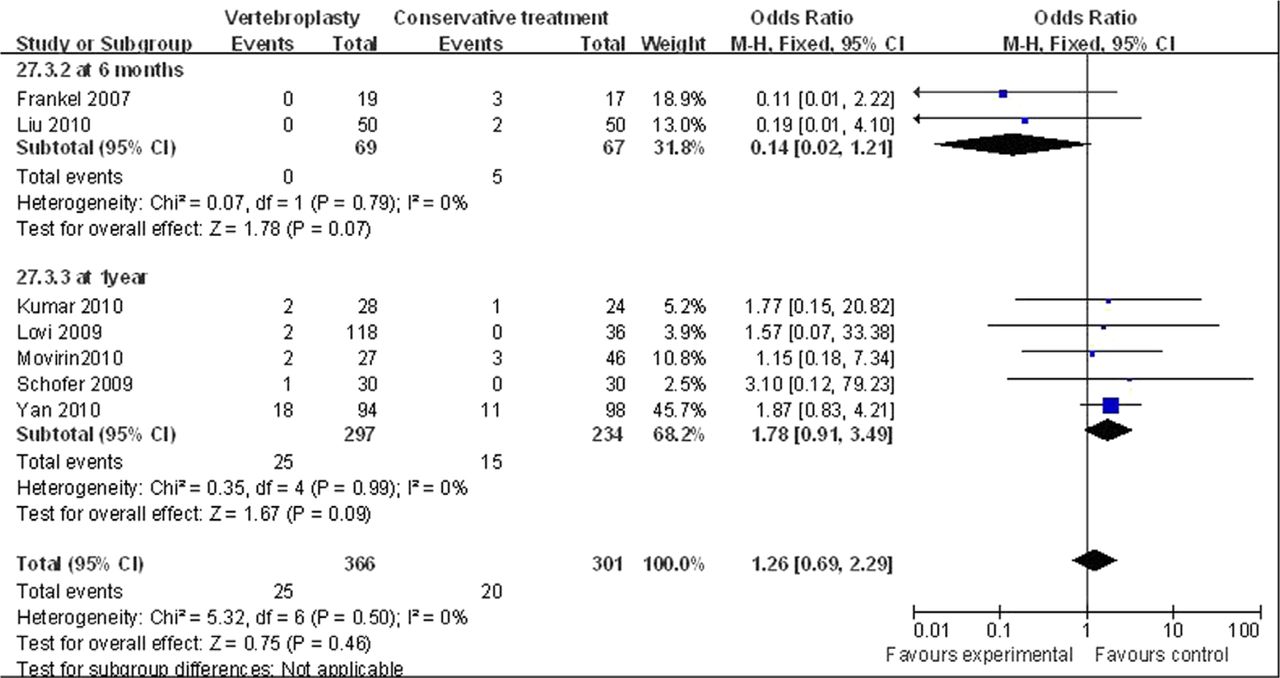
(1) Adjacent new vertebral fractures
There was no significant difference between both groups at 6 months and 1 year after operation (P > .05, WMD was 0.14 [0.02, 1.21] and 1.78 [0.91, 3.49], respectively) (Fig. 4).
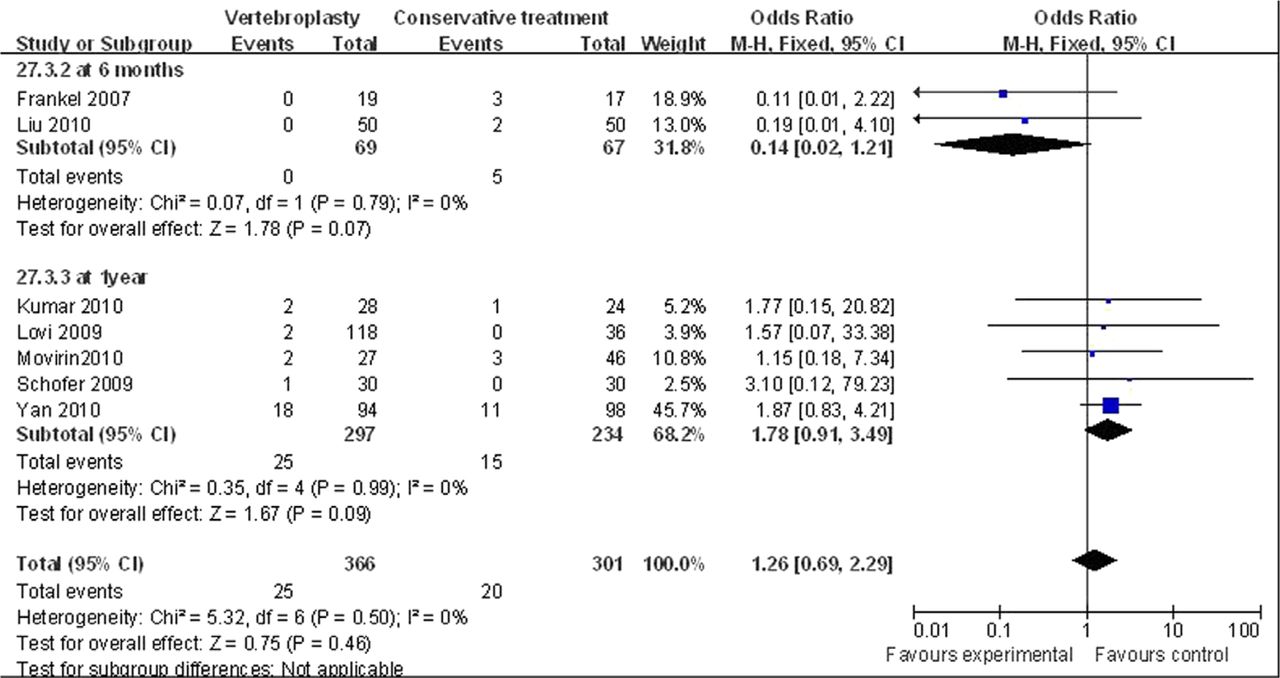
The forest plots of meta-analysis of adjacent new vertebral fractures.
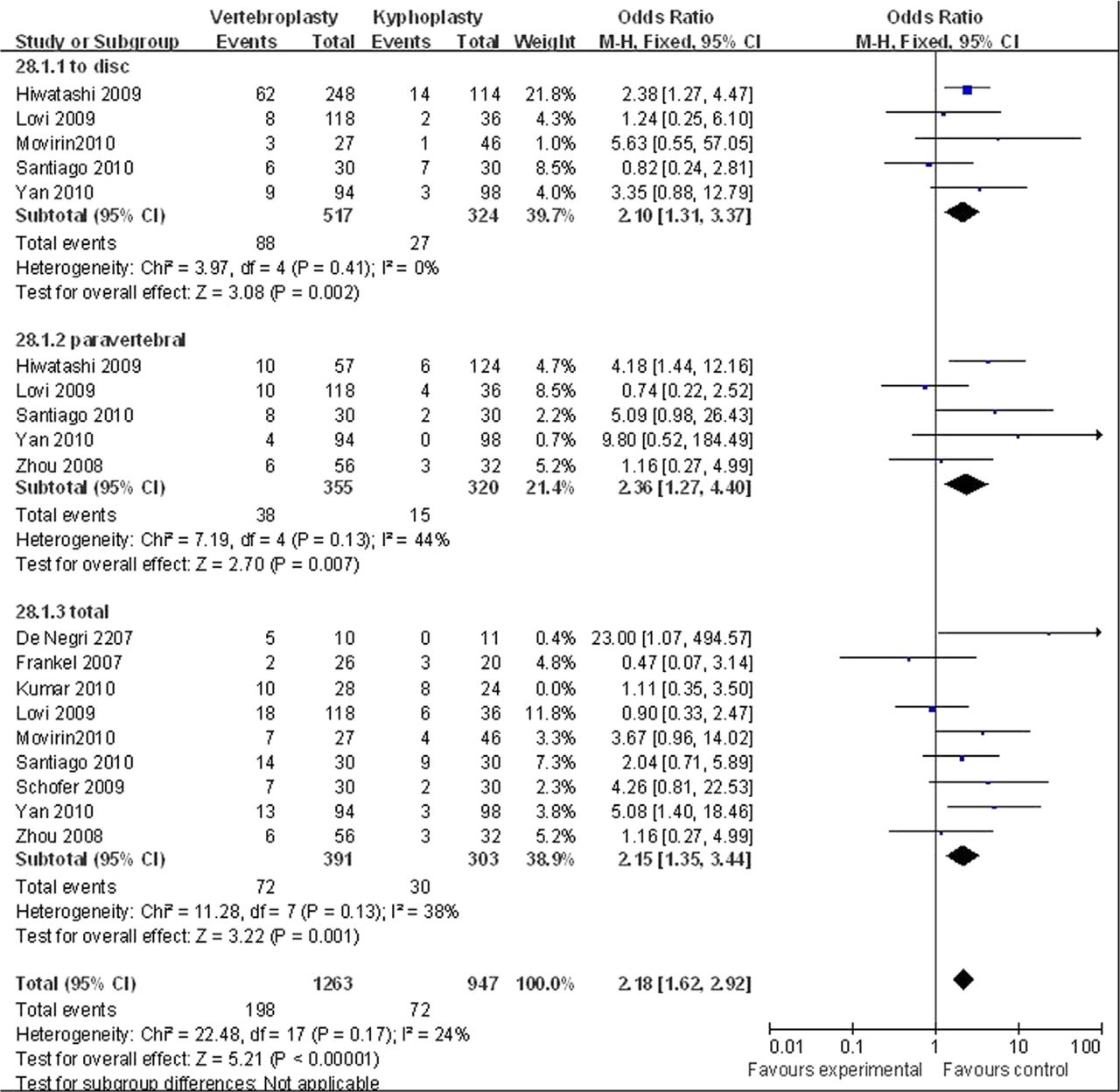
(2) Cement Leakage
To disc: The cement leakage to disc for the vertebro-plasty group was significantly more than the kyphoplasty group (P < .05, OR 2.10 [1.31, 3.37]).
Paravertebral: The paravertebral cement leakage in the vertebroplasty group was significantly more than the kyphoplasty group (P < .05, OR 2.36 [1.27, 4.40]).
Total: The total cement leakage in the vertebroplasty group was also significantly more than the kyphoplasty group (P < .05, OR 2.15 [1.35, 3.44]).
Fig. 5 presents the forest plots of the meta-analysis of cement leakage.

The forest plots of meta-analysis of cement leakage.
Table 6 shows the results of meta-analysis of complication outcome measures.
Results of meta-analysis of complication outcome measures
Discussion
The results of this meta-analysis have shown that the volume of cement injected and the operative time for the vertebroplasty group was significantly less than the kyphoplasty group. At baseline, the VAS scores were similar in both groups. At 1–3 days, 1–2 weeks, 1 month, 3 months, 6 months, 1 year, and even 2 years after operation, the VAS score in the vertebro-plasty group was significantly more than the kyphoplasty group. These results mean that pain relief after kyphoplasty is significantly greater than that achieved with vertebroplasty. The benefits can be sustained for at least 2 years.
The vertebral height and kyphosis angle for the vertebroplasty group was similar to the kyphoplasty group at baseline, but after operation, the vertebral height was significantly less and the kyphosis angle was significantly more than the kyphoplasty group. The improvement in the vertebral height and kyphosis angle for the vertebroplasty group was significantly less than the kyphoplasty group. As for complications, the adjacent new vertebral fractures were similar in both groups at 6 months and 1 year after operation. The cement leakage to disc, paravertebral cement leakage, and the total cement leakage for the vertebroplasty group were all significantly more than the kyphoplasty group.
To avoid selection bias, we searched MEDLINE, EMBASE, Web of knowledge, Sciencedirect, EBSCO, Springlink, Scopus, the Cochrane library, and any other database that may possibly contain useful studies for relevant articles in this meta-analysis. Moreover, all reference lists were checked manually. Only “vertebroplasty” or “kyphoplasty” were selected as keywords and no language restrictions were applied. In this way, we avoided losing any useful studies even it lead to more ineligible studies received and more work. Because the first study about vertebroplasty was published at 1987, we searched the studies from January 1987 to July 2011. Reviewers independently selected articles on the basis of the inclusion criteria to minimize bias in the selection of studies and data extraction. Any disagreement was resolved by discussion. Scores were assigned to study design characteristics by using a standardized form recommended by the Cochrane library.14 Other characteristics were also extracted by using a standardized form.
As we all know, for an ideal meta-analysis, it is better that all the studies enrolled are randomized controlled trials (RCT) with homogeneity. However, in practice, RCT is very rare, especially for surgery.33, 34 It is because treatment with surgery is different from that with drugs. Every surgeon has his personal preference and familiarity with the various surgical options. In addition, the patients always take the selection of operation more seriously and seldom agree to receive a randomized surgical option. In this meta-analysis, not only randomized controlled clinical trials, but also quasi-randomized controlled clinical trials, perspective cohort study, and retrospective cohort study were enrolled in this meta-analysis. It would not influence the credibility of the results for this meta-analysis. There were 2 major causes. One was that all the enrolled studies were relatively high-quality studies based on the methodological quality assessment scheme. The other was that almost all the studies reported that the baseline characteristics, such as age, sex, and duration of symptoms, were matched for each group.
We attempted to examine publication bias by using the Funnel plot analysis, because publication bias is a potential limitation of any meta-analysis. In particular, small studies with optimistic results may be published more easily than small studies with unfavorable results. Larger studies with optimistic results may also be published more easily than larger studies with unfavorable results, but this difference usually is smaller. The results show there was no obvious publication bias in this meta-analysis.
Since the late 1980s, 2 minimally invasive surgical treatments, vertebroplasty and kyphoplasty, have been gradually introduced that changed the treatment of OVCF. In 1987, Galibert et al.35 used vertebroplasty for the first time to treat vertebral hemangioma, and later in 1988, PVP was used to treat OVCF. Since then, this technology is being widely used in primary vertebral osteolytic tumors, vertebral metastases, and painful osteoporotic vertebral fractures around the world.36, 37 Guided by X-Ray, vertebroplasty involves injecting PMMA bone cement into the fractures of the vertebral body percutaneously to enhance the strength and stiffness of the vertebra and prevent further vertebral collapse and deformity, and effectively relieve pain.
PKP was first performed in the 199838 and involves fracture reduction using inflation bone tamps (balloon) to restore vertebral height. The 2 bone tamps used bilaterally create a void in the vertebral body that can be filled under fine manual control and low pressure with high-viscosity bone cement. Unlike vertebroplasty, PKP aims to not only secure fracture fixation and stabilization but also to correct and prevent the spinal deformity, thereby reducing the negative burden of VCFs.39, 40 Balloon inflation compacts the cancellous bone and pushes the end plates apart, which might partly restore height and correct angular deformity. Once the balloons have been removed, the resulting void is filled with viscous bone cement to stabilize the vertebral body. The procedure can be done under general anesthesia or conscious sedation, either as a day case, or with an overnight stay, depending on the medical need.
VP has an advantage for certain patients because it usually is a quicker procedure. Usually, it can be performed through a unipedicular approach, which reduces the overall procedure time. This is an important factor for elderly patients with multiple medical problems, who have an increased anesthesia risk, even with conscious sedation.
KP has the advantage of reduced cement leakage. The insertion of the bone tamp before PMMA injection significantly reduces cement leakage. This becomes an important safety factor in fractures with multiple fracture linesand retropulsion, and when a fracture extends into the end plates and the posterior wall. KP is safer than VP for 2 principle reasons: firstly, KP involves cement injection with a lower pressure, and secondly, it is in a more viscous state when injected, which make KP feasible for the treatment of OVCF with vertebral wall deficiency41 and OVCF nonunion without neurological deficit.42 The cement is often injected in a less-viscous state and under high pressures for VP, which often leads to cement extravasation outside of the vertebral body either into the disc space, outside the margins of the body, or into the epidural space. In addition, the creation of the cavity with the balloon during a kyphoplasty facilitates the safe introduction of the cement into this defined cavity. Both procedures carry the risk of cement extravasation; however, there is significantly less risk for kyphoplasty. Compared with the 19.7%-41% cement leakage for VP, the cement leakage for KP is only 7%-10.6%.43–45 The lowest cement leakage rate for KP reported is about 2.0% for 1257 patients in a study in which the author used a special injection technique called incremental temperature cement delivery system (ITCDS).46
The main limitations of this review are that the demographics and comorbidities of study participants were not reported. These possible sources of heterogeneity could not be examined and most of the studies had suboptimal design which would influence the outcome of this meta-analysis to some extent.
Based on the result of this meta-analysis, we can conclude that pain relief after kyphoplasty is significantly greater than that achieved with vertebroplasty. The benefits can be sustained for at least 2 years. Kyphoplasty can improve the vertebral height and kyphosis angle much more than vertebroplasty with lower occurrence of cement leakage.
Footnotes
Dr. Yang et al. have performed a valuable service to China by bringing research about the newest treatment methods for vertebral compression fractures to their region. Perhaps there will come a time when globalized standards in healthcare will allow for the cutting edge of techniques and technologies to arrive to all corners of the globe simultaneously. In the meantime, however, pioneers like Dr. Yang and his colleagues are working hard to bring the best possible care to patients in their own locale. The Yang group has conducted both basic and clinic researches on kyphoplasty (KP) and put forward a series of SUZHOU theories, such as concept and diagnosis of osteoporotic vertebral compression fracture nonunion and incremental temperature cement delivery system (ITCDS). They have contributed a lot to advancement of KP by promoting the popularization and application of these new ideas. They are to be commended for this and we at the Journal encourage other authors interested in documenting their own experiences with blazing a trail for new treatments to share their observations with us. Hansen Yuan, MD, Editor-in-Chief, International Journal of Spine Surgery.
- © 2013 Published by Elsevier Inc. on behalf of ISASS - The International Society for the Advancement of Spine Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.