


Abstract
Background Prior studies of multilevel ProDisc-L (PD-L) implants (Synthes Spine, Inc., West Chester, Pennsylvania) using the standard US technique have used conventional radiography postoperatively. We found vertebral body–splitting fractures (VB-SFs) in interposed vertebral bodies after 5 sequential multilevel PD-L device implantations using the standard US technique. These were identified with postoperative computed tomography (CT) but were not visible on plain radiographs. In an additional patient, we found that a stress-relieving, pilot holes–only technique did not prevent VB-SFs. The 5 patients operated on with the standard technique composed the background series against which we compared the incidence of VB-SFs in patients operated on with a modification of the standard US technique—a combination of stress-relieving pilot holes, removal of cortex in the chisel path, and a fenestrated chisel (PH/CR/FC)—intended to reduce the incidence of VB-SFs in multilevel PD-L constructs.
Methods Patients receiving multilevel PD-L implants at 2 sites—1 in the United States and the other in Germany—were operated on with the PH/CR/FC technique and their postoperative CT scans evaluated for the presence of VB-SFs. The frequency of VB-SFs in these patients was compared with that of the 5 patients from the background series who were operated on by the standard US technique. The groups’ mean sex, age, body mass index, and vertebral body height, as well as average spinal T score, were also compared.
Results No fractures were found in 13 interposed vertebral bodies in 11 patients operated on with the PH/CR/FC technique, as compared with 4 VB-SFs and 1 anterior keel cut–to–anterior keel cut fracture in 5 interposed vertebral bodies in 5 patients operated on with the US technique (P ≤ .001). Although the sample sizes were small, this difference in fracture rate was not associated with sex, age, body mass index, or average spinal T score. At up to 13 months of follow-up of patients in the background series, we found that VB-SFs tend not to bridge with bone, instead forming sclerotic margins.
Conclusions The PH/CR/FC technique studied reduced the incidence of VB-SF in multilevel PD-L implants. Because previously published multilevel studies did not use postoperative CT scans and because VB-SFs are not visible on conventional radiography, the incidence of VB-SFs in multilevel PD-L applications may be higher than previously reported. Our findings may contribute to prevention of complications in total disc replacement.
Total disc replacement is a surgical procedure gaining acceptance as an alternative to spinal fusion in the treatment of symptomatic degenerative disc disease.1 The ProDisc-L (PD-L) implant (Synthes Spine, Inc., West Chester, PA) has been used for total disc replacement in the treatment of symptomatic degenerative disc disease in this report. PD-L implants have produced beneficial outcomes in both single-level and multilevel disc replacements. 2–4
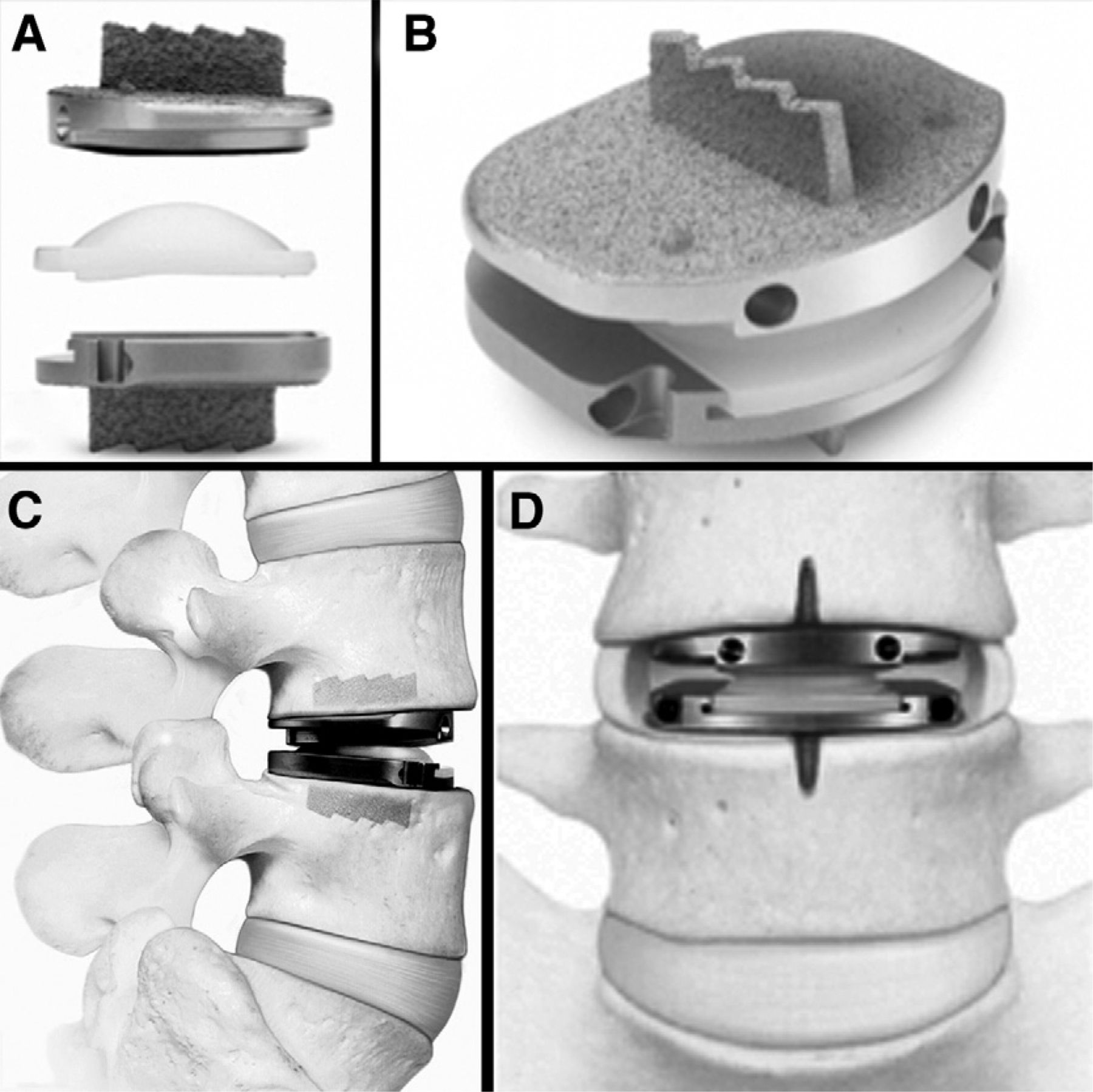
The PD-L implant is a semiconstrained device composed of 2 cobalt-chromium-molybdenum endplates covered with a titanium plasma spray coating to promote bony ongrowth into the surface of the implant (Fig. 1). The articulating surface is composed of ultrahigh-molecular-weight polyethylene inlay contacting metal. A keel at each endplate aids proper orientation of the device during surgical placement and provides fixation for immediate and long-term stability. The standard Food and Drug Administration (FDA)–approved US surgical technique for implant placement requires that chisel cuts to receive the keels are made above and below the instrumented disc space. The implant is available in 2 endplate sizes, 2 lordotic angles, and 3 heights. Including titanium coating, the keel thickness at its base is 2.3 to 2.5 mm, and there is a 5° taper on each side. The width of the chisel cut is 2 ± 0.05 mm at the base of the chisel. Thus, at the base, the keel could be 0.55 mm wider than the chisel cut. Without the titanium coat, the keel is 6.5 mm in height. Thus the minimum total height of 2 keels that are facing each other is 13 mm. In other words, when the sagittal height of a vertebral body falls to less than 26 mm, over half of the vertical dimension in the midsagittal plane is occupied by keel. The 2 keels driven into smaller opposing chisel cuts create opposing wedges that may tend to split the interposed vertebral body. To our knowledge, vertebral body–splitting fractures (VB-SFs) have not been previously reported in multilevel PD-L applications.
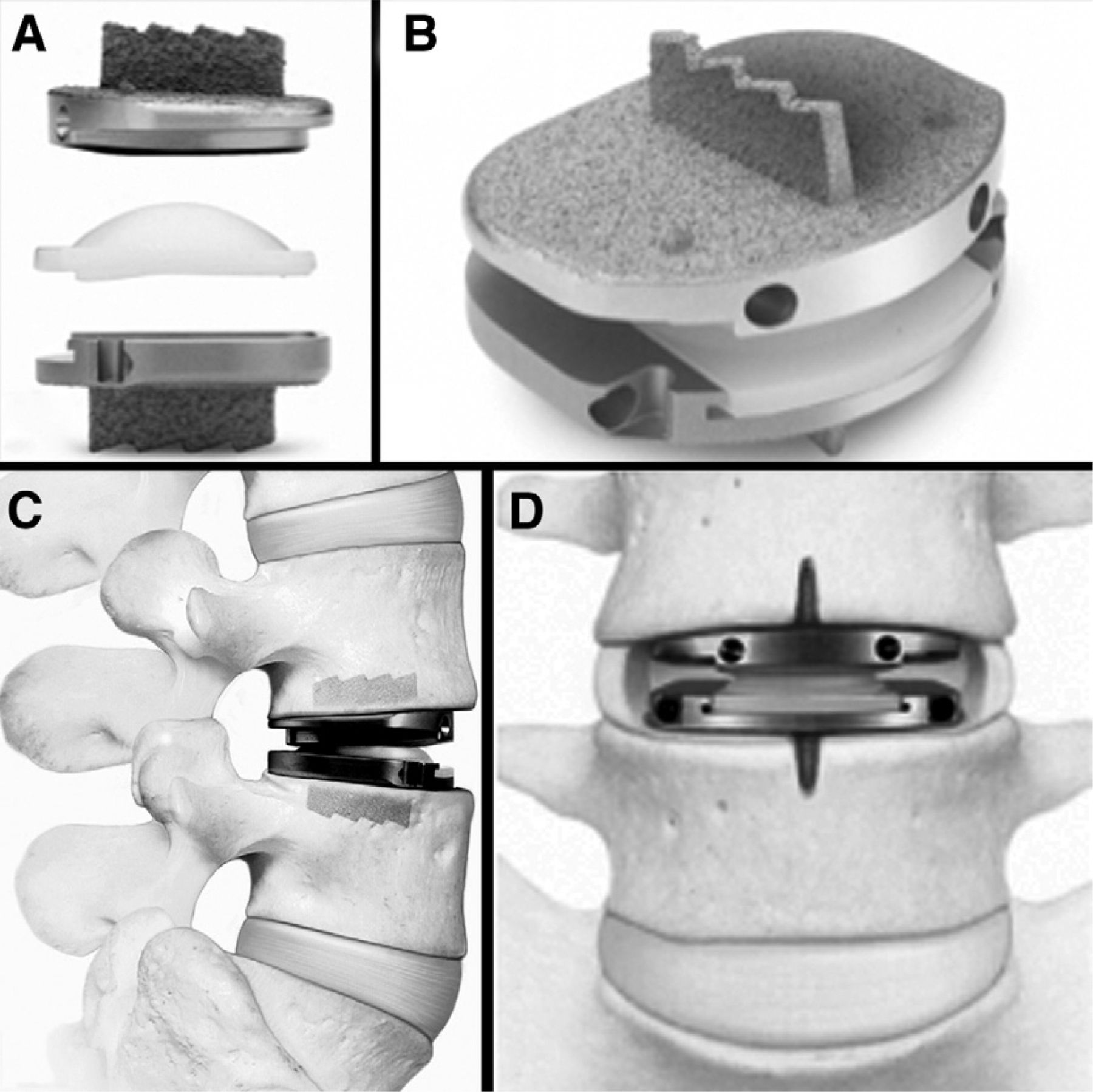
PD-L components (A). PD-L device assembled (B). PD-L device implanted: lateral view (C) and anteroposterior view (D). One should note the keels and associated chisel cuts. (Images reproduced with permission of Synthes Spine, Inc.)
At the US center, preoperative computed tomography (CT) scans were obtained to rule out facet degeneration and pars defect at the index levels for patients receiving PD-L device implantation. CT scans were also taken on postoperative day 1 to verify proper device position.
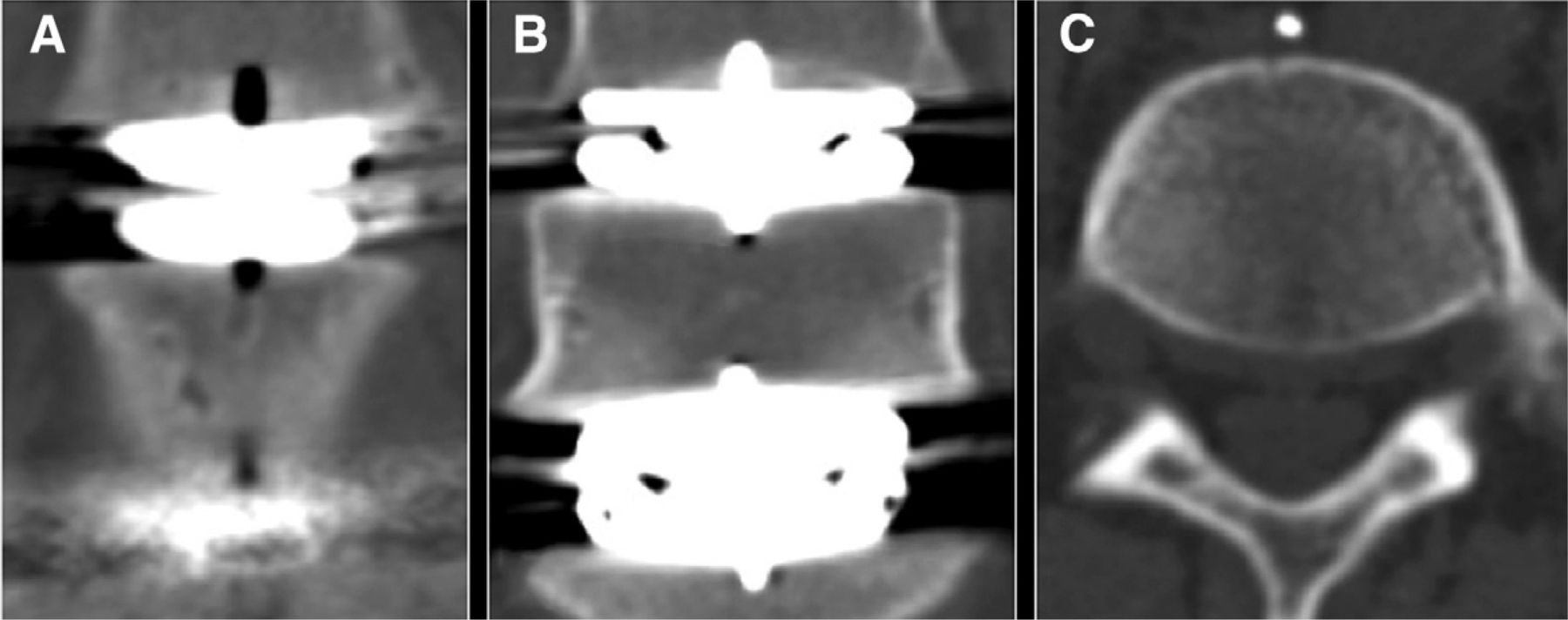
The pilot holes–only (PHO) technique was our first attempt to prevent VB-SFs in multilevel patients. The PHO technique followed the standard US technique, except for the use of 3-mm-diameter pilot holes parallel but slightly distal to the anticipated chisel path to block vertical stress transmission. The depth of the pilot hole shielded the anticipated location of the anterior two-thirds to three-quarters of the keel. This technique failed to prevent a VB-SF in 1 of the 2 interposed vertebral bodies of the only patient in whom it was used. This patient (with implants at L3-4, L4-5, and L5-S1) had a VB-SF of L4, with no fracture identified at L5. A typical VB-SF, as observed in 5 patients, is shown in Fig. 2.

Typical appearance of a VB-SF (patient 6, PD-L implants at L3-4, L4-5, and L5-S1). Coronal CT reconstruction of L4. The fracture connects the keel cuts in L4 (A). Coronal CT reconstruction through the midbody of L4 (B). The fracture connects the keels of adjacent PD-L implants. Axial CT reconstruction of L4 (C). The fracture extends from the anterior cortex to the posterior venous drainage.
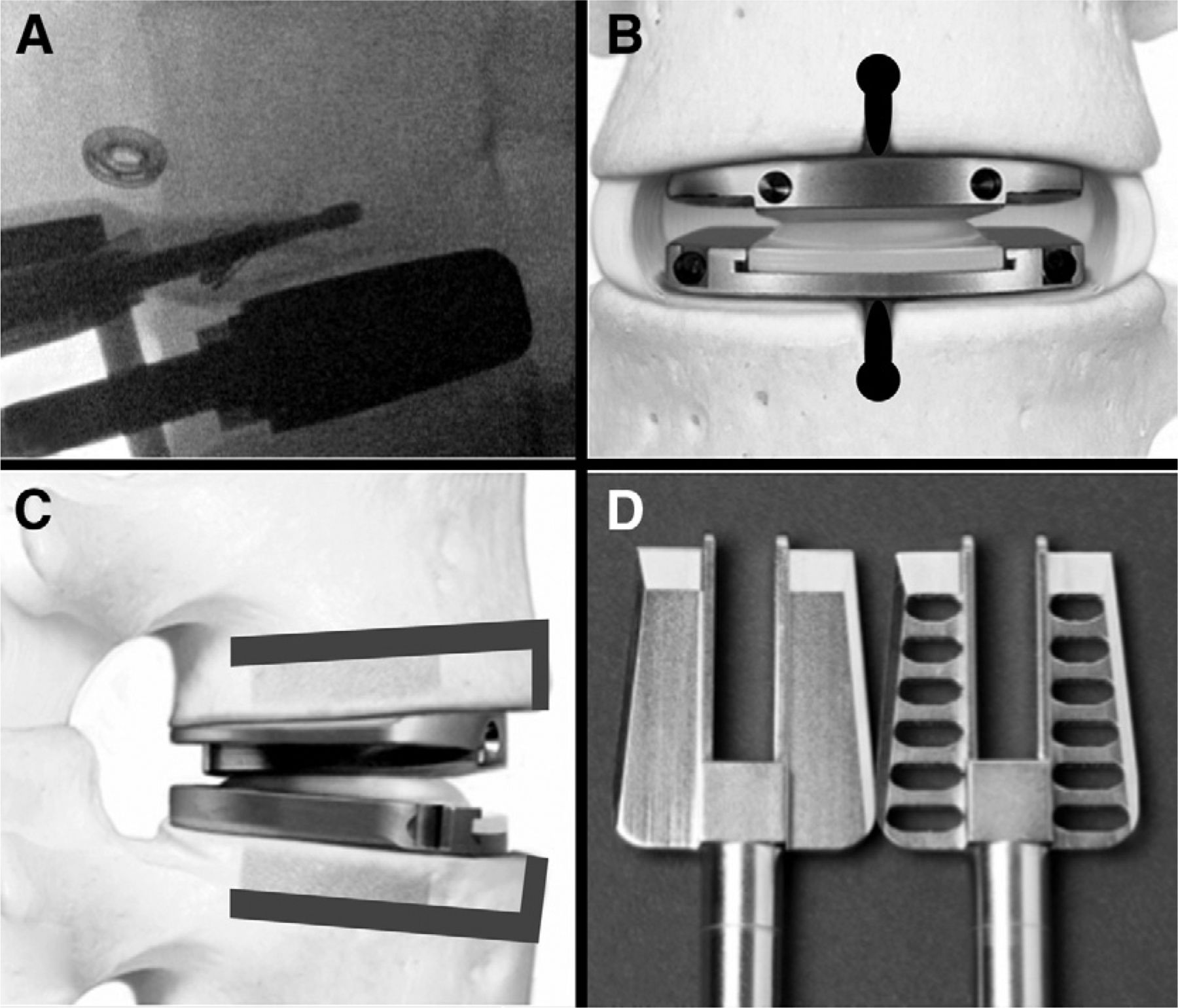
In a further attempt to prevent VB-SFs, we used the pilot holes/cortex removal/fenestrated chisel (PH/CR/FC) technique. First, to block the spread of sagittal shear forces, 3-mm-diameter pilot holes were drilled immediately distal and parallel to the anticipated chisel cuts so that each hole terminated either at the limit of the drill or, more optimally, anterior to the posterior one-third of the planned keel cut. Second, to prevent spreading of cortical bone by the chisel and keel, a linear region of the anterior cortex 3 mm in width was removed with a high-speed drill, thus connecting the pilot holes to the disc space along the anticipated site of keel entry into the cortex of the vertebral body. Because the keel of the implant is slightly tapered from base to tip, fixation of the implant occurs primarily at the base of the keel. The pilot hole is slightly distal to, or impinges on only the apex of, the chisel cut. Therefore widening the keel cut in this manner does not increase the risk of implant migration. Cortical removal would have no effect on implant migration because the implant sits well posterior to the site of cortex resection. Third, to diminish vertical spreading forces from the chisel by allowing cancellous bone to collapse into the chisel as it advances from anterior to posterior, a chisel with fenestrations was used in place of the standard US chisel. The PH/CR/FC technique is illustrated in Fig. 3.

PH/CR/FC technique for PD-L device implantation. Drilling of pilot hole in superior vertebral body as seen on intraoperative lateral fluoroscopy (A). Anteroposterior diagram of implanted PD-L device with location of pilot holes and anterior cortex removal in heavy black overlay (B). Lateral diagram of implanted PD-L device with gray overlay depicting the location of pilot holes and anterior cortex removal (C). Comparison of standard US chisel (left) with fenestrated chisel (right) used in modified surgical technique (D). The reverse-cutting horizontal surfaces in the fenestrated chisel should be noted. (B and C, excluding the overlays, are reproduced with permission of Synthes Spine, Inc.)
Methods
After approval of a Health Insurance Portability and Accountability Act waiver by the US center's Institutional Review Board, we retrospectively reviewed the medical records of all patients with complete radiologic data who received multilevel PD-L device implantation (between levels L3 and S1) using the standard US surgical technique at the US center from July 1, 2008, to March 3, 2009 (group I). Age, sex, body mass index (BMI), and average L1 to L4 T score of the lumbar spine were captured from electronic medical records. Preoperative and postoperative day 1 CT scans were examined for the presence and classification of fracture and vertebral body height (VBH). In addition, to evaluate fracture evolution over time, follow-up CT scans were performed at various intervals and at the termination of the study. We excluded the 3-level case because the technique deviated from the standard technique used to compare group I and group II.
Group II consisted of consecutive multilevel PD-L cases from both the German and US centers operated on with the PH/CR/FC technique. The US patients in this group were operated on by H.G.S. between August 4, 2009, and July 9, 2010, and were selected using the same criteria as group I. The German center patients were consecutive patients consenting to postoperative CT scans operated on by R.B. between October 8, 2009, and November 17, 2009, with complete radiologic data. Patients were required to be skeletally mature, have 2 or more levels showing clear morphologic changes on lumbar T2-weighted magnetic resonance imaging scans, and be symptomatic for a minimum of 6 months. The German center did not require preoperative CT scans. Exclusion criteria included pregnancy, osteologic disease other than primary osteopenia, rheumatoid arthritis, and perioperative bone infection. Furthermore, because the effect of staging on fracture is unknown, patients whose procedures were staged were excluded. Age, sex, BMI, and average L1 to L4 T score for the spine were collected retrospectively. One patient did not have T-score data. For statistical analyses, the remaining T scores were taken as representative of the group.
Imaging evaluation
CT images were obtained for all patients in group I preoperatively, on postoperative day 1, and as required for follow-up. CT images for group II were obtained in the immediate postoperative period. Radiographic images for groups I and II were studied at the US center by use of Synapse (version 3.1.1; Fujifilm Medical Systems, Stamford, Connecticut), a picture archiving and communications system and a DICOM (Digital Imaging and Communications in Medicine)–compliant viewing system. Original axial images, as well as reconstructed axial, coronal, and sagittal images, were analyzed for the presence of fracture by use of Intellilink (Synapse) to link a specific location in multiple reconstructions as supplied by the picture archiving and communication system.
A CT scan algorithm was developed to aid in fracture identification. This algorithm consisted of a set of coronal reconstructions parallel to the anterior surface of each vertebral body associated with an implant, a set of axial reconstructions perpendicular to the anterior cortex of each vertebral body associated with an implant, and the use of high kilovoltage to minimize artifact. The coronal image began anterior to the target vertebral body and extended through the posterior cortical margin; the axial reconstructions began within the superior implant/disc and ended in the inferior implant/disc. If CT scans are not performed in this fashion, artifact from the implants may obscure the VB-SFs in some cases.
All CT scans in group I were independently reviewed at the US center by the surgeon, a radiologist, and 2 student research fellows, as well as by the surgeon from the German center. CT scans in group II were independently reviewed by the US surgeon, the German surgeon, and the US radiologist. To determine whether fractures noted on CT scan were evident on conventional radiography, the radiologist also reviewed all postoperative lumbar spine radiographs and/or intraoperative fluoroscopic images of group I patients.
By use of the ruler tool (Synapse), the VBH of each vertebral body that received a PD-L implant was measured in millimeters along the midline of the vertebral body when viewed on a midsagittal cut.
Classification of fractures
Independent evaluation of the CT scans resulted in complete agreement among all evaluators. Upon retrospective review of postoperative day 1 CT images in group I, 2 fracture types were noted: VB-SFs and an anterior keel cut–to–anterior keel cut fracture in an interposed vertebral body. All fractures shared the following criteria: there was no sclerotic margin on the immediate postoperative CT scan; they were identifiable on both axial and coronal views with digital cross checking of location in image space; they were not present on the preoperative CT scan; they were visible outside of the keel/chisel cut region; they connected the chisel cuts and were oriented cranial-caudally; and they were visible at surgery only if the anterior longitudinal ligament and periosteum were removed so that the anterior cortex of a vertebral body was directly visualized. In addition, VB-SFs extended cranial-caudally through the entire vertebral body; were present on all axial cuts; connected the keels on coronal cuts; and extended through the site of central, posterior vertebral body venous drainage.
An interesting feature of the VB-SF is that it is a ring fracture with only 1 break in the ring; most ring fractures break the bone in 2 places. When the spread between fracture fragments is only a few millimeters, there could be sufficient elasticity in the posterior vertebral arch to allow only a single break in the ring. Another possibility is that these fractures are more like a saw cut in a ring as compared with other ring fractures seen clinically.
Bone densitometry
Bone density measurements for patients at the US center were obtained for L1 through L4, as well as for the average T-score value for this region. The average T-score values were used for this study. Bone density measurements for patients at the German center were obtained using various units and collected from electronic medical records.
Statistical analysis
Analysis included descriptive statistics of patient characteristics and demographics. Continuous variables were compared by use of t tests, and discrete variables were compared by use of χ2 analyses. P < .05 was considered significant. We compared the incidence of fracture in group I and group II using Fisher exact tests.
Results
Details regarding levels operated on, technique, surgeon, and site are provided in Table 1. Groups I and II were not significantly different in age, sex, BMI, or average T score of the spine; however, the vertebral bodies were significantly taller in group II than in group I (P = .005, t test) (Table 2).
Patient-specific surgical and fracture details for group I, transitional, and group II patients
Group I and II comparisons
Fracture incidence
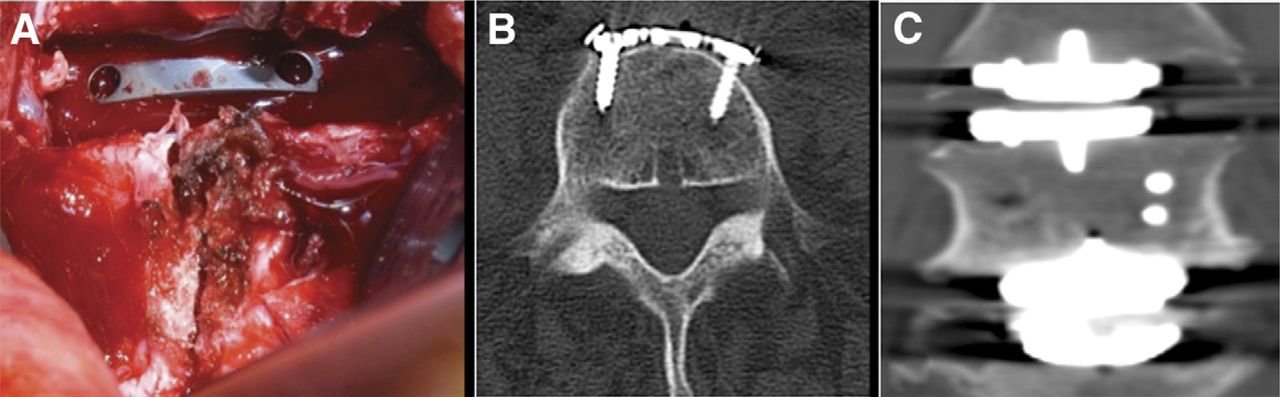
Five fractures were identified on postoperative CT scans in group I patients (Table 1), none of which were visible on routine anteroposterior or lateral lumbar spine radiographs. The cortical portion of the lone anterior keel cut–to–anterior keel cut fracture (Fig. 4) was observed after removal of the anterior periosteum and anterior longitudinal ligament between the keel cuts in patient 4 in the interposed vertebral body during surgery. This fracture was plated at surgery. As shown in Figs. 4A and 4B, this fracture connected the inferior and superior chisel cuts but was not visible within the vertebral body on postoperative CT scan (Fig. 4C). The 4 remaining 2-level cases in group I had VB-SFs of the interposed vertebral bodies.
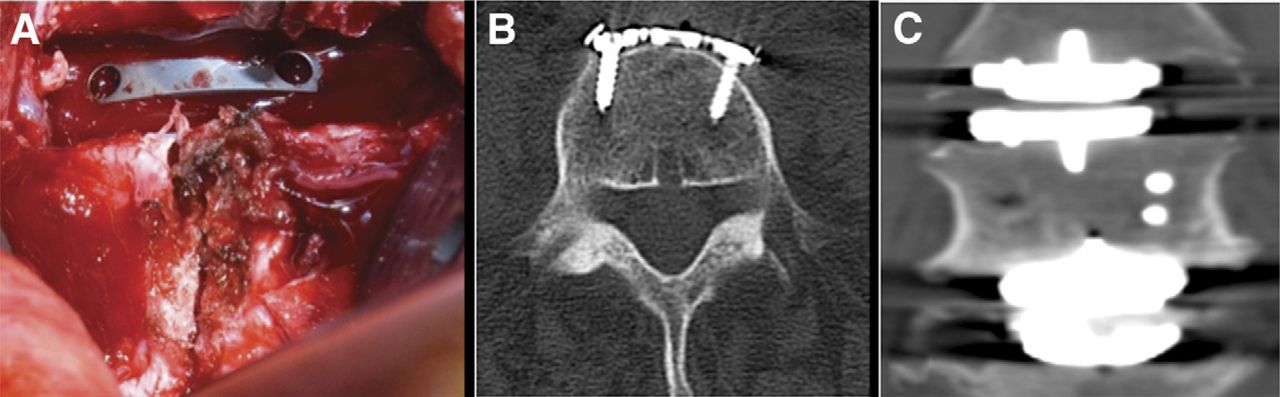
Patient 4, a 2-level PD-L case with a cranial-caudal anterior keel cut–to–anterior keel cut fracture. Intraoperative photograph taken after removal of the anterior periosteum between the keel cuts, showing a fracture connecting adjacent keel cuts (A). Axial (B) and coronal (C) CT reconstructions showing no evidence of fracture within the L5 vertebral body.
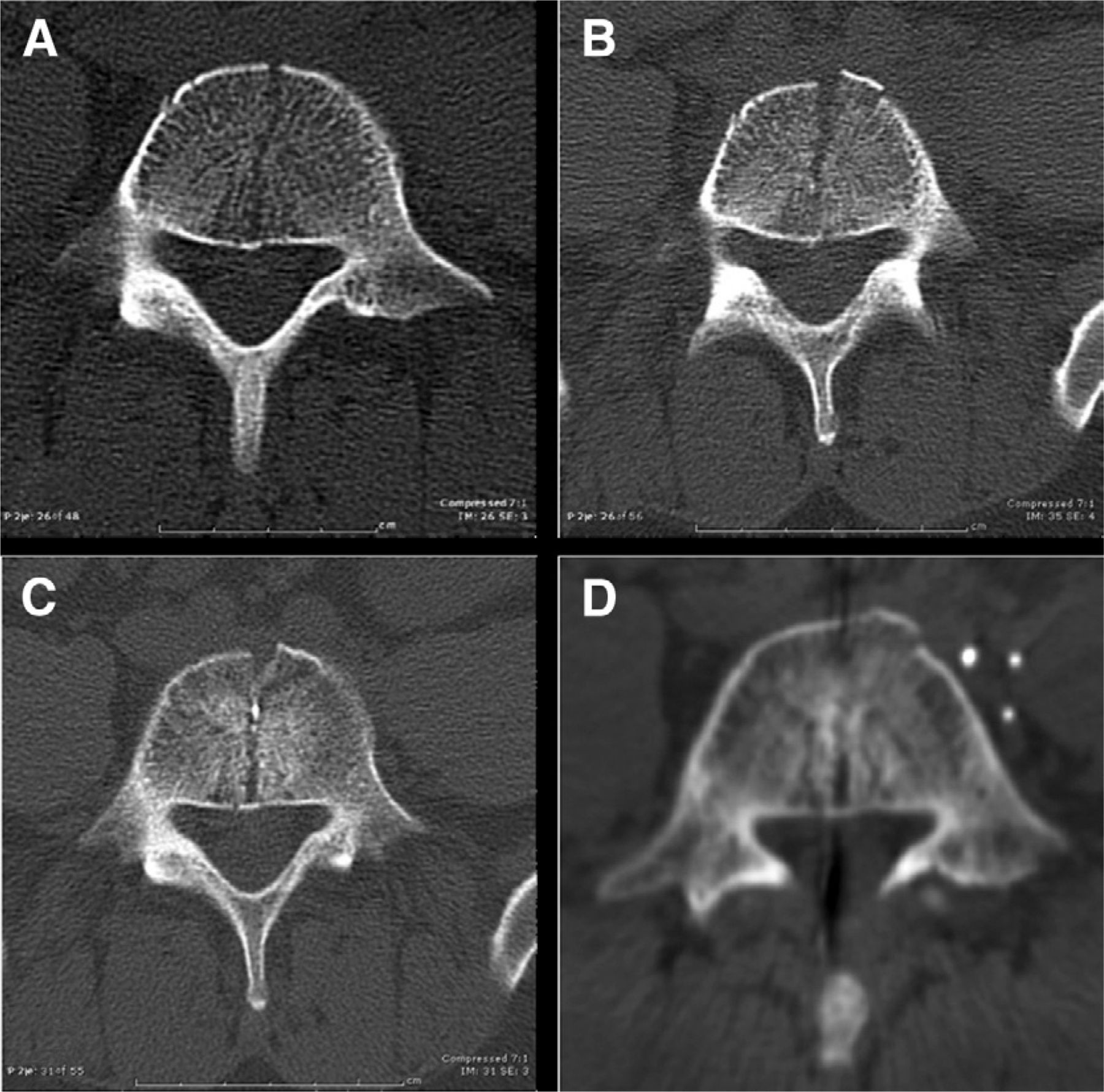
Of the 5 multilevel patients with fractures, 4 were asymptomatic. Patient 5, however, was involved in an off-road vehicle accident with severe axial spinal loading 10 days after surgery, creating a potentially adverse outcome related to a VB-SF (Fig. 5). This patient had initially achieved complete early postoperative low-back pain relief. After the accident, the patient immediately had severe lowback pain. A post-accident CT scan showed fracture separation and anterior extrusion of a wedge of bone along the margin of a fracture that was present on the postoperative day 1 CT scan (Figs. 5A and 5B). The injury also resulted in lateral displacement and rotation of the superior endplate of the inferior prosthesis into a nonfunctional position. The patient was managed with bracing and pain medication. At 4 weeks, a CT scan showed either healing through the anterior portion of the fracture or shift of the anterior bone fragments into a more contiguous position along with posterior fracture persistence (Fig. 5C). An additional CT scan at 8 months showed anterior healing and sclerosis with continued posterior fracture persistence (Fig. 5D).

Axial CT reconstruction of the L5 vertebral body from patient 5, who may have had an adverse outcome related to a VB-SF. Postoperative axial CT showing the VB-SF (A). Axial CT scan 10 days postoperatively, immediately after an accident with extreme vertical and rotational loading of the spine (B). One should note the fracture separation and the anterior wedge of bone that has been extruded. Axial CT scan 4 weeks after injury showing anterior healing or fragment migration with posterior fracture persistence (C). Axial CT scan 8 months after injury showing continued anterior fracture healing with sclerosis around the posterior portion of the fracture, which remains open (D).
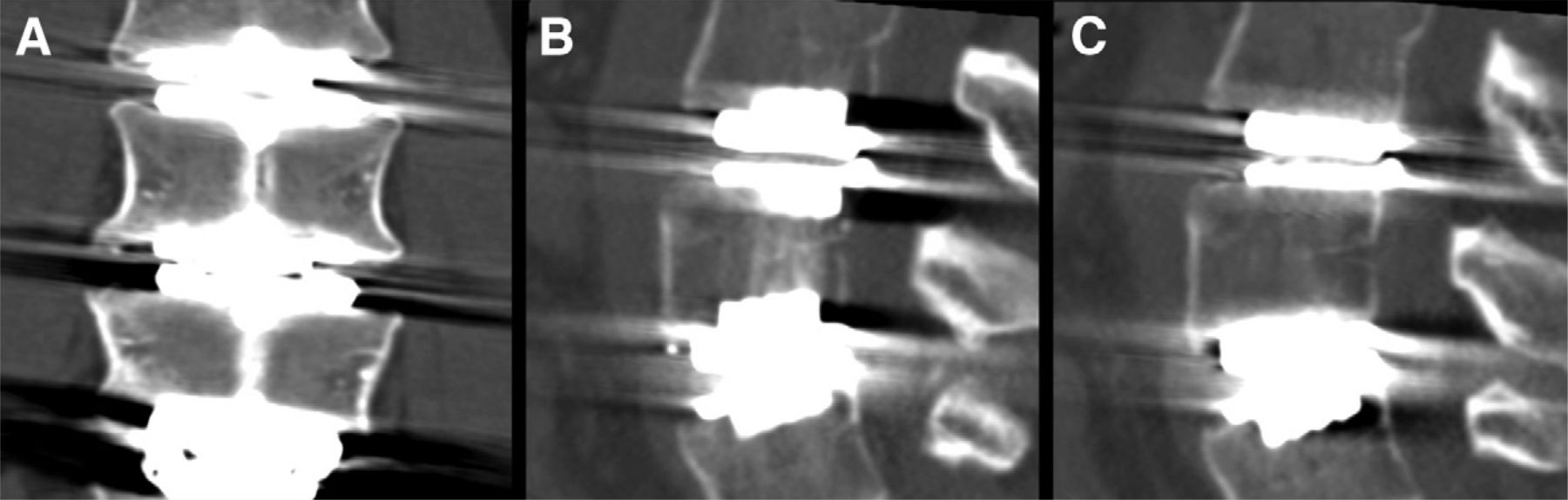
No fractures of any type were found in any of the 13 interposed vertebral bodies in the 11 group II patients. A typical interposed vertebral body from group II is shown in Fig. 6.
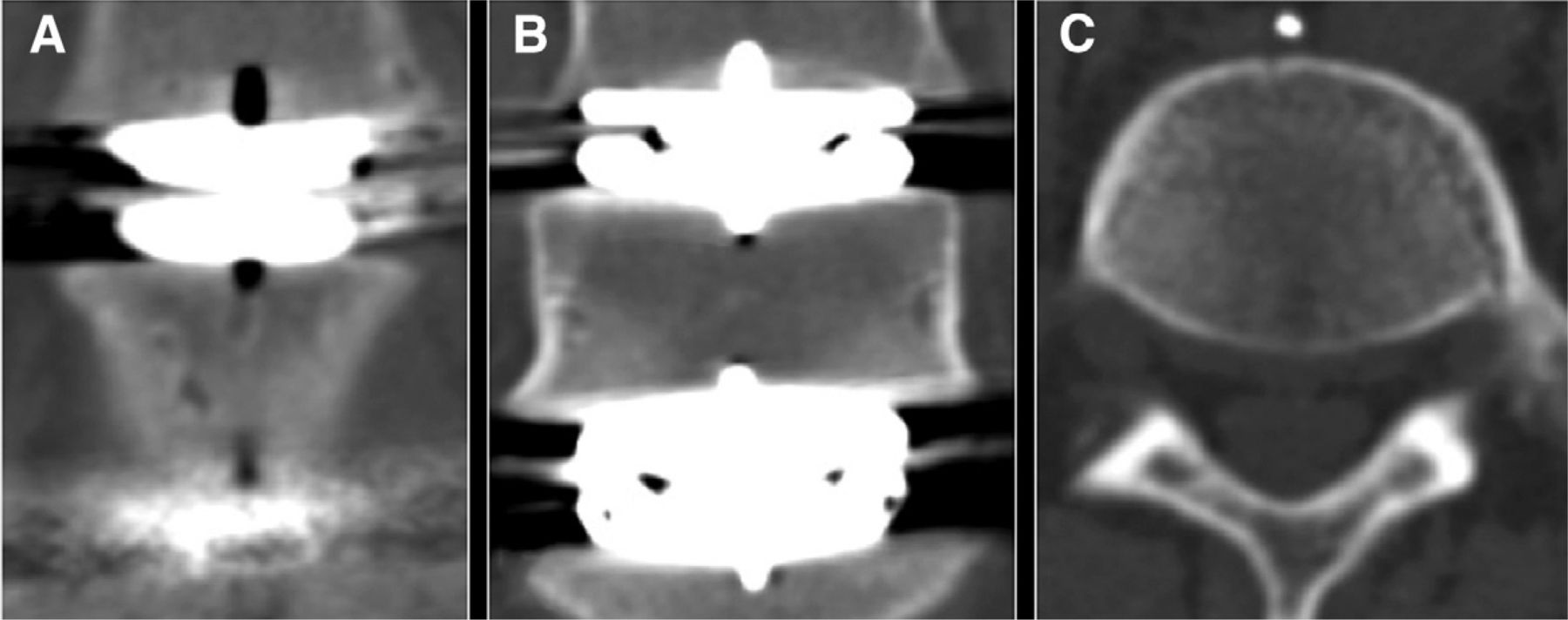
Postoperative CT scans of patient 7 centered on L5 with no evidence of fracture. Anterior coronal cut (A). Midcoronal cut (B). Midbody axial cut (C).
In the 5 interposed vertebral bodies from group I operated on with the US technique, there were 4 VB-SFs and 1 anterior keel cut–to–anterior keel cut fracture, compared with 0 fractures in the 13 interposed vertebral bodies of group II operated on with the PH/CR/FC technique (P < .001, Fisher exact test). A comparison considering only VB-SFs (4 of 5 fractures) showed a significant difference with respect to the occurrence of VB-SFs in groups I and II (P = .002, Fisher exact test).
The 11 group II patients with 13 interposed vertebral bodies retained for fracture comparison analysis and group I patients did not differ significantly in age, BMI, or average T score (P = .909, P = .125, and P = .491, respectively; t tests). Group I patients had 4 interposed vertebral bodies at L5 and 1 interposed vertebral body at L4, whereas group II patients had 5 interposed vertebral bodies at L5 and 8 interposed vertebral bodies at L4 (P = .294, Fisher exact test). There was a 2.9-mm difference in mean VBH in group I versus group II patients (24.5 ± 1.3 mm vs 27.4 ± 1.8 mm; P = .005, t test). A subset of 3 group II patients with 4 interposed vertebral bodies had VBHs similar to those of the group I patients operated on with the US technique (P = .266, t test).
Sclerotic development in nonfractured vertebral body
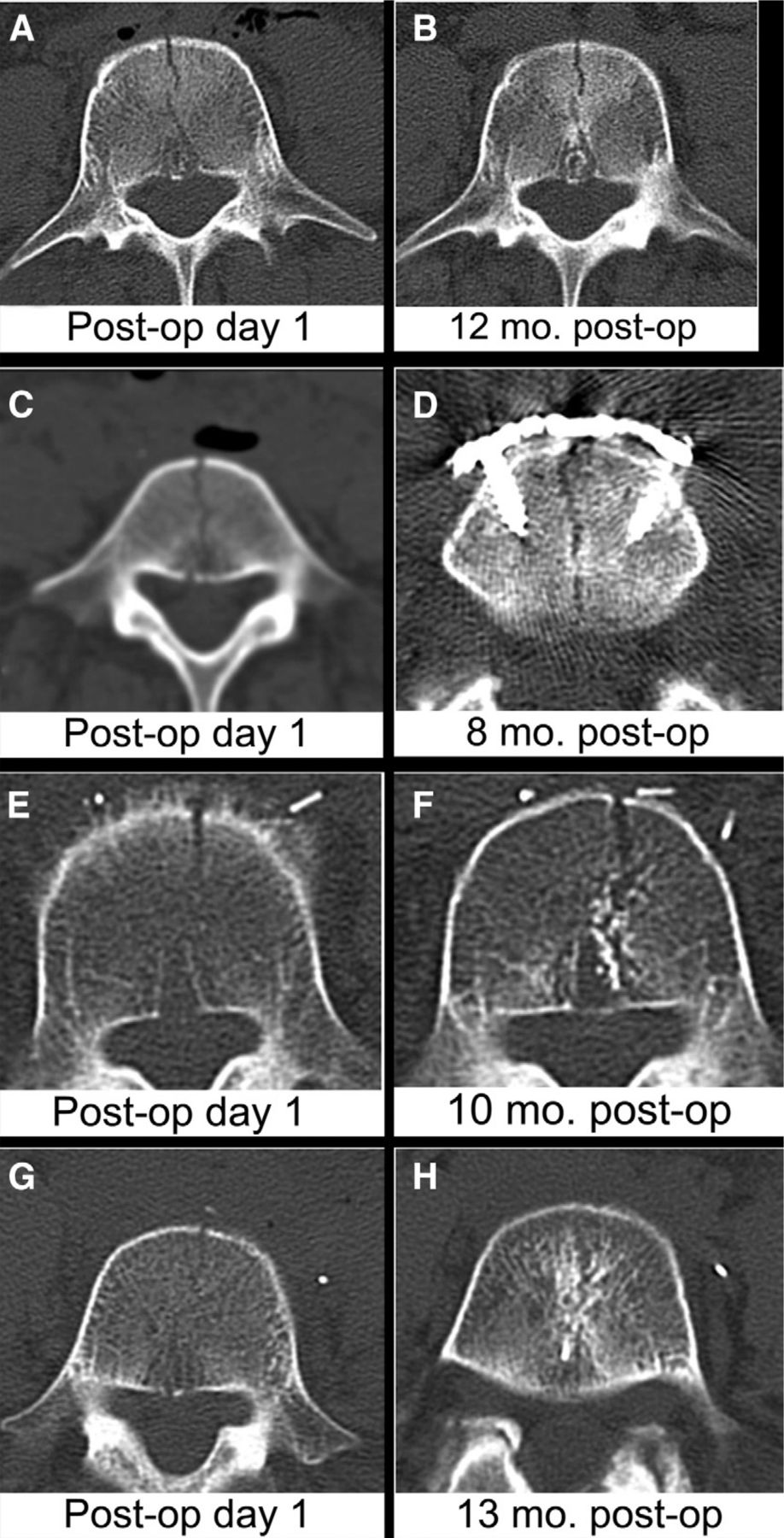
Further review of the CT scans uncovered an unexpected phenomenon in the follow-up of patient 6, the transitional 3-level patient operated on by the PHO technique who had a VB-SF in 1 interposed vertebral body and no fracture in the other interposed vertebral body. A central vertical column of bony sclerosis, similar to what was observed around VB-SFs on follow-up CT scans, appeared connecting the keels in an area of the vertebral body previously thought to be normal (Fig. 7A). At 5 months, a dense band of sclerosis was observed connecting the 2 keels, although no fracture was apparent on the immediate postoperative CT scan. This sclerotic band in the nonfractured vertebral body is similar to the sclerosis paralleling the fracture in the fractured vertebral body at the level above. Similar sclerosis was observed connecting the keels of adjacent PD-L implants in group I patients (Figs. 7B and 7C). This sclerotic band tended to be on either side of the fracture. Follow-up imaging at 12 months (patient 6), 8 months (patient 3), and 10 months (patient 2) showed sclerotic margin development accompanied by minimal bone bridging (Figs. 8A and 8B, Figs. 8C and 8D, and Figs. 8E and 8F, respectively). Only patient 1 displayed cortical defect closure along with fracture bridging at 13 months’ follow-up (Figs. 8G and 8H).
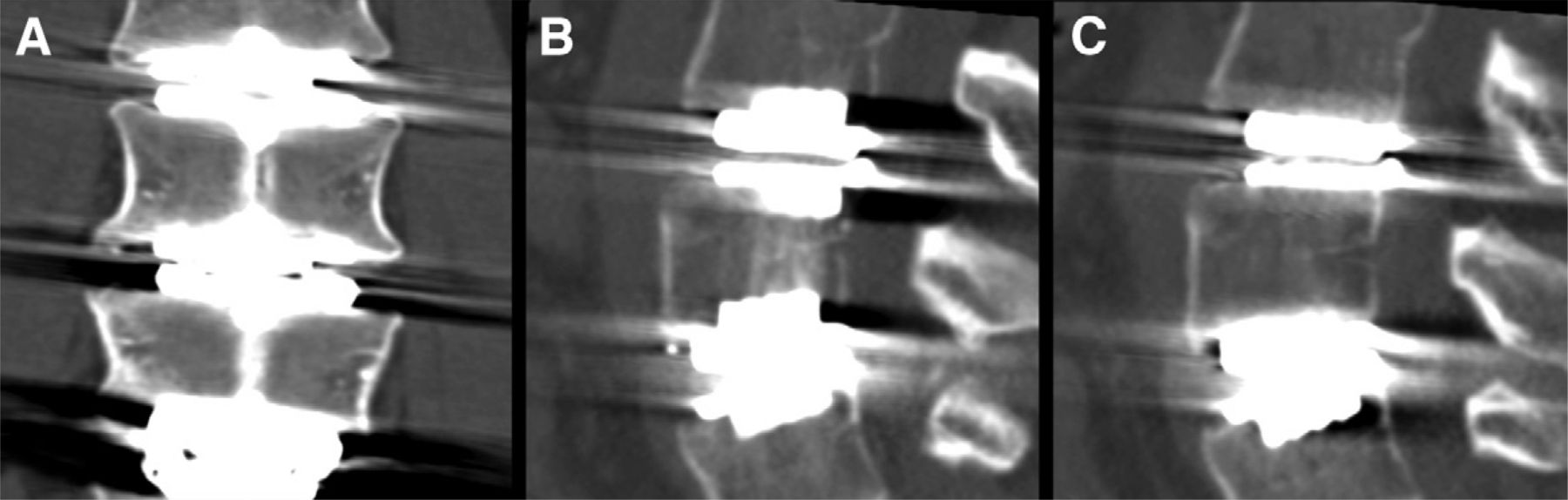
Twelve-month follow-up CT scan of patient 6, a 3-level PD-L case operated on by the PHO technique, showing late formation of a vertical sclerotic band in the nonfractured L5 vertebral body on axial CT reconstruction (A). One should note the similarities between the sclerosis at this level and what is seen in the fractured L4 vertebral body at the level above. Twelve-month follow-up CT scan of patient 1 (B). One should note that the sclerotic development is seen only between 2 adjacent keels. Off-midline sagittal CT cut depicting absence of sclerotic band (C).

Initial and final follow-up axial CT images of the multilevel PD-L cases with VB-SFs without clinical sequelae. In patients 6 (A and B), 3 (C and D), and 2 (E and F) with 12, 8, and 10 months’ follow-up, respectively, the fractures remain open and show sclerotic margins without evidence of bridging of the fracture. One should note the unhealed fracture in D, where a plate was placed across the fracture on the second postoperative day. On these images, the fractures are more obvious at late follow-up. In patient 1 (G and H), a 13-month follow-up axial CT reconstruction shows cortical bridging at the fracture and sclerosis around the fracture path.
Discussion
To our knowledge, only 2 CT-documented VB-SFs have been reported previously.5 Both were single-level cases in Asian women, who likely had small vertebral bodies, although no actual VBH measurements were provided in the report. Although they lacked the 2 connecting keels, these VB-SFs had the same appearance on CT scans as those described in our report. No definitive report of the cause or clinical consequence of VB-SFs has been presented. The fact that only 2 single-level VB-SFs have been previously reported supports the notion that single-level PD-L device implantation using the standard US surgical technique and performed in accordance with FDA exclusion criteria carries a low risk of VB-SFs. Further supporting their conclusion, we have examined postoperative CT scans of 14 single-level PD-L patients operated on by the standard US technique, none of whom had VB-SFs.6
Our data suggest that VB-SFs may commonly occur in multilevel PD-L cases when the US technique is used. In this series all but 1 such case had a VB-SF in the interposed vertebral bodies, and the remaining case had an anterior keel cut–to–anterior keel cut fracture in the interposed vertebral body. VB-SFs and keel cut–to–keel cut fractures are not apparent on plain radiographs of the lumbar spine; therefore postoperative CT scanning with attention to the reconstructions used in this report is required to detect these fractures. In previous studies of multilevel PD-L applications, patients have been followed up with plain radiographs of the lumbar spine.2, 3, 5, 7, 8 In the absence of site- or patient-specific differences that could increase the likelihood of VB-SFs at the US center, our data suggest that fractures could have been present in previous studies of multilevel PD-L device implantation but not identified because of follow-up using plain radiography or inadequate CT technique.
We considered a variety of site-specific differences that might explain the incidence of VB-SFs at the US center—some unusual characteristic of the patients’ spines, due to common geographic locale, ethnic heritage, or occupation; local variation in surgical technique; or a flaw in the instruments or PD-L implants used—but we found no discernible pattern.
Although the variable did not reach statistical significance because of the study's small sample size, the VB-SF patients in group I were predominantly women (4 women and 1 man) compared with the group II patients (5 women and 6 men). We believe that there were enough women in group II to rule out a uniquely female characteristic of bone, other than smaller size, that would make them more prone to fracture. On average, the interposed VBH of group II patients was 2.9 mm larger than that of group I patients with VB-SFs. Even though this difference was statistically significant, one could argue that 1.45 mm distributed on either side of the midline might not be large enough to make a mechanical difference. On the other hand, the difference in height between the uncut vertebral body in group I (11.5 mm) and the uncut vertebral body in group II (14.4 mm) is more impressive, at 20%. Whether height was a significant factor in causing the fracture difference between group I and group II can be addressed from our data by evaluating the subset of 3 group II patients (2 women and 1 man) with 6 small interposed VBHs (VBH ≤ 26.5 mm, the largest VBH in group I) (not statistically different from the height of the fractured interposed vertebral bodies using the standard technique in group I). No fractures were seen in these group II patients with small VBHs, which suggests that the PH/CR/FC technique may have been effective in preventing VB-SFs in these patients with small vertebral bodies. We concede that these comparisons are based on very small samples and that a follow-up study with a larger sample size of patients with small VBHs would be required to resolve this issue.
A disturbing feature of the VB-SFs is the lack of bone bridging across the fracture site evident at up to 13 months of follow-up. In fact, our data suggest that VB-SFs tend to develop sclerotic margins around the fracture over time, similar to a pseudarthrosis. It is possible that these fractures could persist indefinitely without healing; however, additional long-term follow-up is required to substantiate this hypothesis. We hypothesize that the persistence of these fractures could be a reflection of Wolff's law of bone remodeling.4 The major mechanical loading of a vertebral body is directed parallel to the VB-SF rather than across the fracture, and this lack of stress patterns typically associated with bone healing may account for the persistence observed with the fractures in this study. This is supported by the localization of the sclerotic bands between adjacent keels and parallel to the VB-SFs in our follow-up series, consistent with significant loading vertically along the fracture line. Similarly, this may account for the late-appearing sclerotic band noted between keels of the nonfractured interposed vertebral body vertebrae. It is also possible that the keel of the implant simply prevents the fracture from closing.
As shown, VB-SFs may not heal and, therefore, could become clinically significant over time; however, the clinical consequences are uncertain at best. According to Synthes Spine, Inc., over 6000 multilevel PD-L implant cases have been performed worldwide. Until now, no VB-SFs in multi-level applications have been reported in the literature, and only 2 VB-SFs in single-level cases have been documented.5 Adverse clinical sequelae due to VB-SFs in multilevel PD-L implants have not been reported in over 10 years of worldwide use and in over 8 years’ experience in the United States. In the absence of postoperative CT evaluation, poor outcomes due to VB-SFs may have remained unexplained.
By clinical criteria, VB-SFs should be stable. All of the patients in this report with VB-SFs were asymptomatic, with the exception of the patient with severe vertical loading trauma. This case may offer insight into the clinical importance of VB-SF, in that severe consequences may occur only when a split interposed vertebral body is subjected to extreme axial and rotational loads. Of course, it is impossible to discern whether the same injury would have occurred if a VB-SF were not already present at the time of injury. We speculate that the sclerotic bone formation along the fracture line and endplate noted during other patients’ follow-up (Fig. 7) might have protected this patient had the trauma occurred at a later time postoperatively. Therefore we argue that a conservative approach with bracing and activity limitations should be taken postoperatively, especially in multilevel PD-L implant patients.
Because of the possibility of severe unintended consequences, changes in any established surgical technique must be undertaken with extreme caution. We have shown to a high level of statistical significance, albeit in a small sample size, that the PH/CR/FC technique described in this report seems to eliminate or reduce the occurrence of VB-SFs. The technique is simple and easily accomplished in skilled hands. The accuracy of the pilot holes and cortical cut could be ensured—and vascular structures protected—through use of a drill guide, that is, a protective tube anchored to the vertebral body and to the trial. It is our opinion that the fenestrated chisel adds no risk and it should be made available in the United States when multilevel PD-L applications are FDA approved. We believe that anyone wishing to perform multilevel arthroplasty with PD-L implants (or any other arthroplasty device with opposing keels in multilevel applications) should consider adopting the PH/CR/FC technique reported in this study.
The major limitations of our study are the small sample sizes used for comparison and the fact that a randomized design was not used. The prospective arm of this study did not use a randomized design because we did not believe that it would be ethical to knowingly subject patients to an increased possibility of VB-SFs. Despite these limitations, we believe that our findings suggest that the PH/CR/FC technique significantly diminishes the likelihood of VBSFs. The major complements to this study would be a prospective evaluation of postoperative CT scans in women with small vertebral bodies by the described method and a callback of patients from the multilevel investigational device exemption study to evaluate for persisting evidence of VB-SFs using CT.
Conclusions
VB-SFs such as those described in this report may be under-reported and could be relatively common when the US technique is used in multilevel applications of PD-L implants. Most importantly, the occurrence of VB-SFs may be eliminated or significantly reduced by using the PH/CR/FC technique described in this report.
Potential risks must be evaluated by the operating surgeon before the PH/CR/FC modification is adopted. Centers continuing to use the standard US surgical technique in multilevel applications of PD-L implants may wish to consider screening for VB-SFs by obtaining postoperative CT scans according to the protocol suggested in this study. We believe such screening might be especially important in women with small vertebral bodies. We recognize that a scientifically rigorous answer to questions of incidence and clinical significance of split fractures in multilevel PD-L applications can be addressed only by exploration of the issue in larger sample sizes with the standard technique. Before such a trial, the problem must be identified and appropriate questions raised. If nothing else, this manuscript serves that purpose.
Footnotes
Nicholas R. Ladwig's work was supported by the Joan Curran Memorial Summer Fellowship, Gundersen Lutheran Medical Foundation.
Rudolf Bertagnoli consults for Synthes Spine, Inc. In addition, Humbert G. Sullivan, Molly M. Cerniglia, Michelle A. Mathiason, and Vicki L. McHugh receive support from Synthes Spine, Inc. for research unrelated to this study. The other authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this article. Synthes Spine, Inc. had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript.
Presented at the 11th Annual Meeting of the International Society for the Advancement of Spine Surgery, April 26–29, 2011, Las Vegas, Nevada.
- © 2012 ISASS - International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}