


ABSTRACT
Background: The present study intended to identify debris in the spine surgical field that frequently rises to the level of the surgeon's face during several different elective spine procedures. Unlike other areas of orthopedic surgery where infection risk is of high concern, in spine surgery the surgical team usually uses a nonsterile face mask instead of a protective space suit with a sterile face shield. It is possible that blood or bone burr particles striking the surgeon's face mask represent a potential source of infection if they ricochet back into the operative field.
Methods: We reviewed 46 consecutive, elective spine surgeries between May 2015 and August 2015 from a single-surgeon practice. For each surgery, every member of the surgical team wore sterile (space suit) personal protective equipment. After each procedure, the face shield was carefully inspected by 2 members of the surgical team to identify patient blood, tissue, or bone burr dust present on the face shield.
Results: The rate of surgeon face shield debris inspected for each case overall was 38/46 (83%). The rate of first assistant face shield debris inspected per case was 16/46 (35%). The scrub technician had a 0% rate of face mask debris on inspection. The highest debris exposure rates occurred with transforaminal lumbar interbody fusions (100%), open laminectomy and fusions (100%), and anterior cervical discectomy and fusions 43/46 (93%).
Conclusions: There is a high rate of blood and tissue debris contact that occurs during spine surgery, and it is procedure dependent. Spine surgeons may consider using sterile shields particularly in high-risk cases to protect themselves and their patients.
Level of Evidence: 4.
INTRODUCTION
Surgical protective equipment, including scrubs, gloves, and face masks have a dual purpose. The equipment protects patients from wound contamination, as well as serves to protect the surgical team from exposure to patient-specific pathogens. Blood or tissue debris from the surgical field can and frequently does land on the protective equipment, including nonsterile surgical loupes and facemasks, exposing the surgical team to these pathogens. Additionally, some of this material may ricochet off the unsterile protective equipment and reflect onto the operative field, leading to legitimate contamination. Such contamination is particularly likely to occur in spine surgery as surgeons often lean into and over the surgical wounds to access deeper structures.
In other areas of surgery, particularly in joint arthroplasty, where aerosolization of blood, bone burr dust, and tissue debris are common, “space suits” have emerged to create a sterile surface across the surgeon's face and neck. Sir John Charnley designed the body exhaust system (BES) with the hope to isolate the surgical site from operating room personnel. The BES was designed as a negative-pressure system with intake and outtake tubing blowing air away from the surgical site, in hopes to keep any bacterial shedding that does occur away from the field. Routine use of the BES began after the publication of a large multicenter prospective randomized study by Lidwell et al1 in 1982. This study showed that, when combined with an ultraclean-air system, incidence of joint sepsis was approximately 25% of operations performed with conventional ventilation.1 The BES tubing was later replaced by the less cumbersome surgical helmet system (SHS), consisting of a portable helmet and hood. Today, this SHS, or what is commonly referred to as the orthopedic “space suit,” is used almost uniformly in orthopedic joint replacement surgery. These suits require specialized ventilated helmets and clear facial coverings. Traditionally, such space suits are not utilized in spine surgery due to difficulty with light illumination and potential reflection of light from the facial covering. Recently, a new helmet/space suit system was developed that is lightweight and features an integrated, adjustable headlight (Figures 1a–c). The integrated headlight offers a comparable illumination to the headlights commonly worn in spine surgery. The sterile face shield and attached hood covers the surgeon's face (including loupes), chin, and neck.

Lateral (a), oblique (b), and axial (c) images of a space suit with integrated headlight. The face shield is far enough anterior that it does not contact or impede the loupes. The orientation of the headlight and relative posterior position of the light relative to the loupes prevent glare by the light from impeding the visualization of the loupes.
The purpose of this study was to evaluate the percentage of spine cases in which debris from the spine surgical field rises to the level of the surgeon's face. Such debris poses an immediate danger to the surgeon and other members of the operative team, and as described above, may reflect a potential source of wound contamination if it ricochets back into the surgical field off a nonsterile facial covering.
METHODS
A collection of 46 consecutive elective spine surgeries between May 2015 and August 2015 were included from a single-surgeon practice. Surgeries included 15 anterior cervical discectomy and fusions (ACDF), 8 posterior cervical discectomy and fusions (PCDF), 4 transforaminal lumbar interbody fusions (TLIF), 6 microdiscectomies, 6 lumbar laminectomies with fusion, and 5 lumbar laminectomies without fusion.
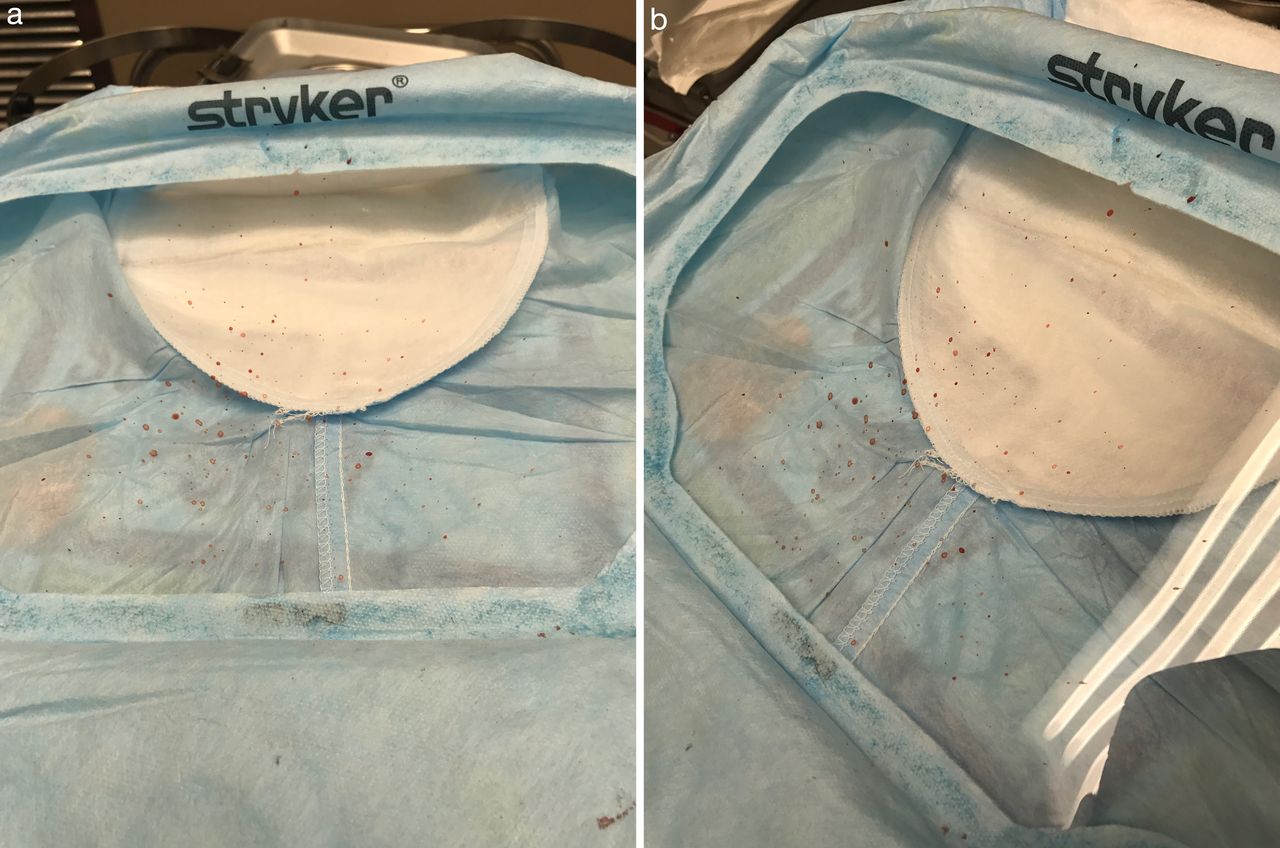
For each surgery, every member of the surgical team wore an orthopedic SHS and gown, with a sterile protective face shield. After each procedure, the face shields of the operative surgeon, first assistant, and scrub technician were carefully examined by 2 independent observers on the surgical team to identify blood, tissue, or burr dust present on the face shield (Figures 2a, 2b). Blood or tissue debris in the upper right corner of the hood (where the handle to adjust the headlight is located) was excluded as it may have been deliberately caused by the surgeon during the case. For the purposes of this study, the presence of tissue debris was considered to represent contamination to the sterile field, carrying with it the potential of becoming an infectious agent.
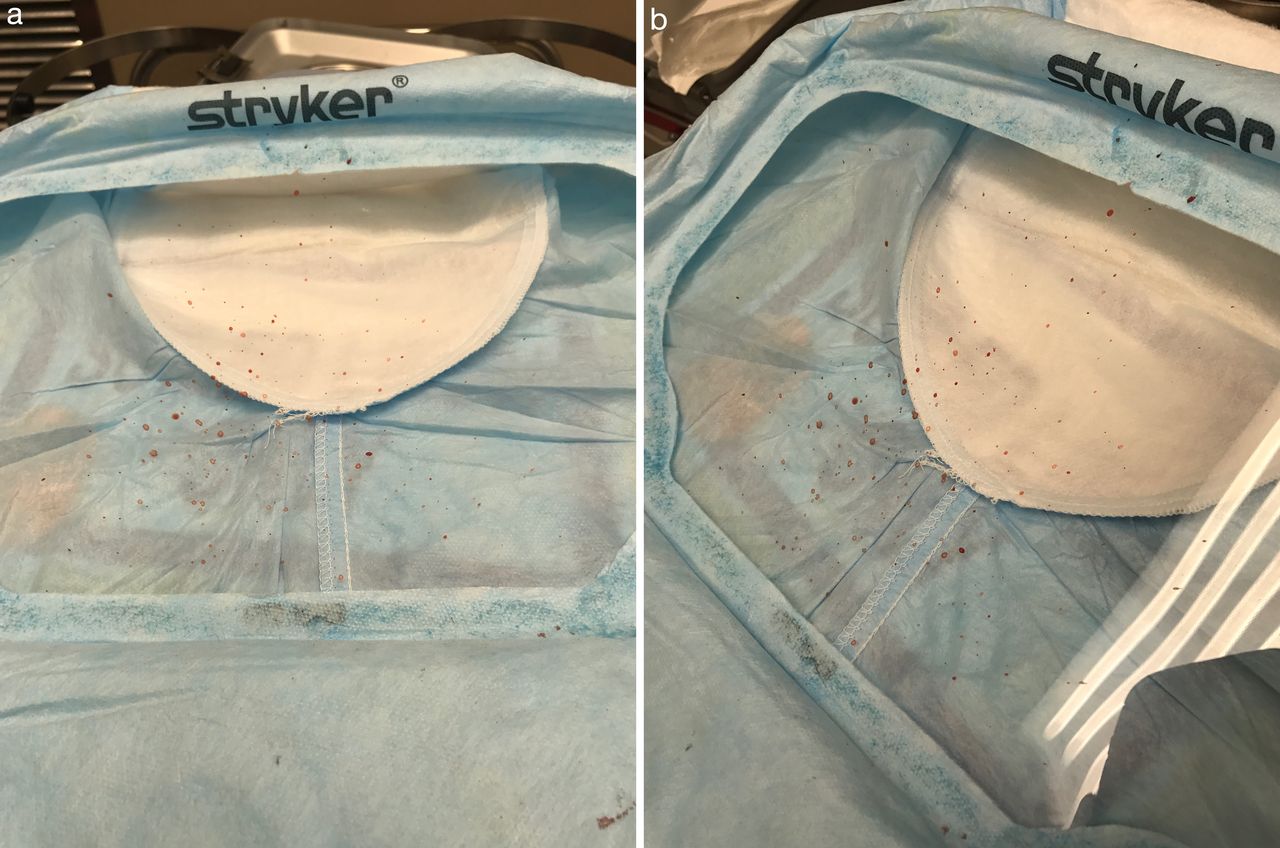
Frontal view (a) of a face shield inspection following a transforaminal lumbar interbody fusion. There is abundant gross blood splatter visualized on the part of the gown underneath the face shield (covering the surgeon's neck). An oblique view (b) demonstrates that the blood splatter goes up to the top of the face shield corresponding to the surgeon's upper forehead and hairline.
RESULTS
The orthopedic space suits were successfully used in all 46 cases (ie, there were no cases requiring removal of the helmet for completion). There were no complications specific to the helmet that were identified (eg, fogging, discomfort, unavailability, or the inability to accommodate the loupes beneath them). The overall rate of blood and/or tissue debris on the operative surgeon's face shield was 38/46 (83%). The overall rate of blood and/or tissue debris on the first assistant's face shield was 16/46 (35%). The face shield of the scrub technician was not found to have blood or tissue debris in any of the cases (0%).
There were differences in the rate of tissue debris on the face shields between specific procedures. The highest rates occurred with TLIF (100%), open lumbar laminectomy and fusion (100%), and ACDF 43/46 (93%). Of all the cases in which debris was identified, 16 included blood and 14 had bone burr dust, and most cases had dual presence of both. Debris was noted most often in cases that involved the use of a burr, osteotome, or an interbody cage.
DISCUSSION
There is a great deal of biological debris that reaches the level of the surgeon's face during spine surgery. The likelihood of facial debris reflecting from the operative field and onto the surgeon's face is procedure-dependent. Procedures that rely upon a high rate of high speed burr utilization, osteotome bone resection, or interbody cage impaction tend to have the highest rate of face shield debris. Theoretically, in surgeries in which space suits are not used, some of the debris may ricochet from the surgeon's mask and/or loupes, and back into the operative field, introducing a contaminant. Based upon the results in this study, we recommend that spine surgeons consider using these suits, particularly in high-risk cases for the protection of both patient and surgical team.
Intraoperative contamination has been shown to be a serious, inevitable problem that is specific to spine surgery. There is a time-dependent, procedure-independent rate of contamination of the surgical field in most spine surgeries.2,3 Surgical implants and instruments have also been demonstrated to become contaminated in a progressive, time-dependent manner in spine surgery.4,5 The posterior elements themselves (spinous processes, lamina, facets) have even been demonstrated to become contaminated in a time-dependent manner.6–8 Contamination can occur after both simple and complex spinal surgery,9 and has been demonstrated to occur more frequently at the surgical field than at a control location in the operating room, such as at an air conditioner vent or near the doorway.10 Although there has been a substantial amount of research on the treatment of intrawound contamination to prevent infection,11–13 including the use of irrigation14–17 and topical antibiotics,18,19 there has been much less research examining the causes and prevention of intraoperative contamination. Previous studies have also demonstrated that specific tools frequently utilized in spine surgery create aerosolized particles and material that can spread and potentially contaminate the entire room. One such tool, the high-speed burr, creates a cloud of blood, irrigation fluid, and bone/tissue debris that travels through the air above the surgical field.20,21 It is our opinion that the use of surgical space suits may mitigate the effects of contamination from these instruments, thereby lowering the overall infection rate.
Weiner and Kilgore22 examined contamination rates of headlamps/loupes and operative microscopes in 70 lumbar microdiscectomies. Contamination was determined by bacterial growth on blood agar plates placed in the center of the surgical field through a 2-stage air sample/settle technique. It was found that both the headlamp/loupe interface and microscope grew out statistically significant more bacteria than a control group (most common organism being coagulase negative Staphylococcus). Our results may shed some light on the mechanism of eyewear and microscope contamination, as there was a high rate of splash contamination at the level of surgeons' eyewear. Another study by Butt et al23 examined bacterial contamination of samples from the nose pad and earpieces of eyeglasses worn by orthopedic surgeons during surgery. The investigators reported contamination by both Staphylococcus epidermidis and Staphylococcus aureus. They attributed contamination to saline irrigation splash, as well as eyewear accidentally falling into the surgical field.23
Davies et al24 investigated the rate of splash contamination on a surgeon's mask and wrap-around protective eyewear in a single-surgeon prospective study over a 1-year period. Recorded blood and body fluid splash contamination rates were found to be 45% on the surgeon's eyewear, and 24% on the surgeon's mask.24 In comparison to the study in 2007 by Davies et al,24 it would appear that splash contamination rates in this current study are twice that of those reported in the Davies et al24 study. However, the surgeries examined in the Davies et al24 study were various vascular surgeries, which by their nature do not involve work with a bur, osteotome, or the more aggressive instruments used in orthopedic spine surgery. The operations in the 2007 study that most closely compare with the operations performed in this current study were below-knee and above-knee amputations, which did incur a 100% rate of splash contamination on either the glasses or mask worn during the surgery. When looking at these types of procedures specifically, it would appear that the data from this current study match the results found in the Davies et al24 study.
Even in situations in which the surgeon's mask and loupes are clean, debris from the surgical field can become contaminated due to contact with sweat on the surgeon's face.25 Mills et al26 looked at contamination of the surgical site from sweat on the surgeons' face. Normal skin flora was grown out in the sweating phase, demonstrating that exposed regions of the surgeon's face and mask can contribute to contamination of the sterile field.26 Other studies using fluorescent particles have demonstrated a reduction in the exposure of surgeon-fomites onto the surgical field with the use of surgical space suits.27 The sterile face shields on these space suits likely help to prevent contaminants from the surgeon's face (eg, sweat and hair) from reaching the level of the sterile field.
There is a dual advantage of utilizing surgical space suits in spine surgery with regards to preventing surgical team contact with a patient's blood and/or tissue debris. Previous studies have demonstrated that standard surgical eyewear, including loupes, do not confer 100% protection from contamination of surgeon conjunctive during simulated femoral osteotomy.28 The face shields used in this study would presumably confer 100% splash protection from patient biomaterial reaching the surgical team's face and eyes. The surgical team reported no instances of direct contamination of the face or eyes during data collection.
A potential problem with surgical space suits is contamination of the surgical field from a positive pressure outflow of material from the surgeon via unsealed areas in the suit. Young et al29 investigated the potential of contamination via protective suits. Investigators found that contamination, as measured by migration of fluorescent powder applied to the surgeon's hands prior to gown and gloving, was increased with the use of body protective suits compared with standard sterile gowns. Migration of fluorescent powder was greatest at the flexor surfaces of the surgeon's arms and at the level of the sleeve cuff and glove interval, with the dominant hand having a greater amount.29,30 Of note, there was no obvious contamination in the gown-glove interface seen in study.
Limitations to this study include a smaller number of cases performed, and the lack of direct quantification of infection as cultures of any face shield contaminant were not collected. Although tissue debris collected on or near the face mask poses an immediate danger to the surgical team, the real area of interest clinically is the theoretical chance of wound contamination, and ultimately a surgical site infection. The authors recognize that not all cases of wound contamination cause surgical site infection, as well as the fact that adjuvant methods, such as irrigation and topical antibiotics, reduce the rate of surgical site infection. Contamination as well is not necessarily associated with a biological state of infection, as this implies the presence of a microorganism causing damage to body tissue. The authors understand that surgical site infection is a multifactorial process that does not always occur due to bacterial inoculation of the surgical site during surgery. However, the results of this study provide compelling, intuitive evidence of a simple, modifiable risk factor. Although only gross, macroscopic contamination of the face shields was assessed, it is not unreasonable to suspect that contamination of face shields on a microscopic level was just as prevalent in the collected cases. The addition of space suits in this study were not found to severely impact the overall cost of the procedure itself, nor did it limit the operating surgeon during the surgery with the sole exception that it was impossible to use an operating microscope. The senior surgeon uses loupe magnification exclusively. Surgical loupes (3.5×) were worn under the space suits in all cases in this study, and there was no impingement of the loupes on the face shield. At our institution, the average cost of a space suit is approximately $65 US currency (disposable). Additional costs include the helmet and reusable batteries that are reused between cases. However, the reusable helmets are used often in orthopedic surgery so, in our case, there was not a specific expenditure for a helmet purchase. We acknowledge, however, that these results are applicable for open surgeries only without the use of an operating microscope. We suspect that an operating microscope would significantly reduce the surgeon's face shield contamination and ricochet of material back into the operative field. Additionally, we suspect that minimally invasive, tubular surgeries may reduce the exposure to the surgeon's face. We hypothesize that the ergonomics of the surgeon's head position contribute to the lower infection rate observed in minimally invasive spine surgery compared with open surgery.
With the advent of newer, more minimally invasive procedures (ie, tubular spine surgeries), this may also significantly decrease the need for sterile protective shields as these procedures are more contained in their general field of view. Follow-up studies are needed to comment more regarding this question.
In conclusion, wearing a protective, sterile space suit may be efficacious in at least some spinal surgeries to reduce exposure of the surgical team to tissue debris. It is probable that these suits also reduce contamination of the operative field; however, additional controlled, randomized studies are needed to expound upon this. Furthermore, relevant clinical outcomes, such as postoperative surgical site infections and revision surgeries are an important focus for future research endeavors.
Footnotes
Disclosures and COI: The authors have no financial conflict with regards to the manufacturers of the orthopedic body suits utilized. No funds were received in support of this work.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2019 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.