


ABSTRACT
Study Design: A retrospective case-series of revision sacroiliac joint (SIJ) fusions.
Objective: To provide a technique guide for revision minimally invasive SIJ fusion.
Summary of Background Data: SIJ dysfunction is a prevalent, yet underdiagnosed condition. This disparity exists as a result of diagnostic complexity and lack of a viable surgical treatment option. However, the advent of minimally invasive SIJ fusion has created a resurgence of interest in this debilitating condition. Multiple studies have reported on the increased use of minimally invasive SIJ fusion in recent years, but there is a paucity of literature on management in a revision setting.
Methods: A case series of 5 patients from a single academic tertiary referral center over a 3-year period will serve to highlight technical pearls and considerations in SIJ fusion revision. Revision SIJ fusions were identified through a retrospective review of a surgical database and demographic, surgical, and radiographic data were obtained through review of the electronic medical record.
Results: Five patients underwent SIJ fusion revision from 2015 to 2018. There were 3 main modes of failure, with indications for revision including nerve root irritation and SIJ pain recurrence. The mean age at time of revision was 48.8 ± 14.3 years, and the mean follow-up after revision was 2.0 + 0.9 years. Familiarity with SIJ anatomy and use of stereotactic navigation can improve implant position and purchase. Additionally, bone graft and bone morphogenetic protein can be used to fill in old implant tracks and to augment bony ingrowth and ongrowth of new implants.
Conclusions: Increased use of SIJ fusion creates a demand for comprehensive revision strategies and necessitates familiarity with SIJ anatomy. Preoperative planning to determine causes of failure and use of intraoperative navigation are essential to help surgeons better understand the preferential trajectory for each implant.
Level of Evidence: 4.
INTRODUCTION
The sacroiliac joint (SIJ) is a complex diarthrodial joint that translates forces between the axial skeleton and lower extremities. The SIJ has significant topographical variability across its articular surface, with the ventral joint surface composed of hyaline cartilage, and the dorsal surface composed of fibrocartilage with more rigid ligamentous structures.1 SIJ dysfunction can be a perplexing condition due to its numerous etiologies, spectrum of presentations and nonspecific examination findings, with 15% to 30% of patients presenting to a spine clinic for low back pain having pain of SIJ origin.2–4
These reasons have contributed to the historic underdiagnosis of SIJ dysfunction; however, improved recognition and treatment, with the advent of minimally invasive SIJ fusion, has created a resurgence of interest in this debilitating condition.5 Multiple studies have highlighted the increased use of minimally invasive SIJ fusion over the last decade and a recent randomized control trial showed significant improvements in pain, patient-reported outcomes and quality of life at 2 years, compared with nonoperative management.6 Long-term studies are still somewhat limited, but 1 study with 5-year follow-up showed significant and maintained improvement in pain and SIJ related disability.7
At the moment, the relative novelty of the procedure has contributed to a paucity of literature on associated complications and particularly on management in a revision setting. The purpose of this study is to use a case series of 5 revision procedures, to highlight technical pearls and considerations in SIJ fusion revision.
METHODS
The surgical scheduling database at a single tertiary referral center was retrospectively queried for sacroiliac fusion revision surgeries from 2015 to 2018. One fellowship trained spine surgeon performed 5 surgeries on 5 patients during this time period. Electronic medical records were reviewed for demographic, clinical, surgical, and radiographic data.
Technique
Preoperative Planning
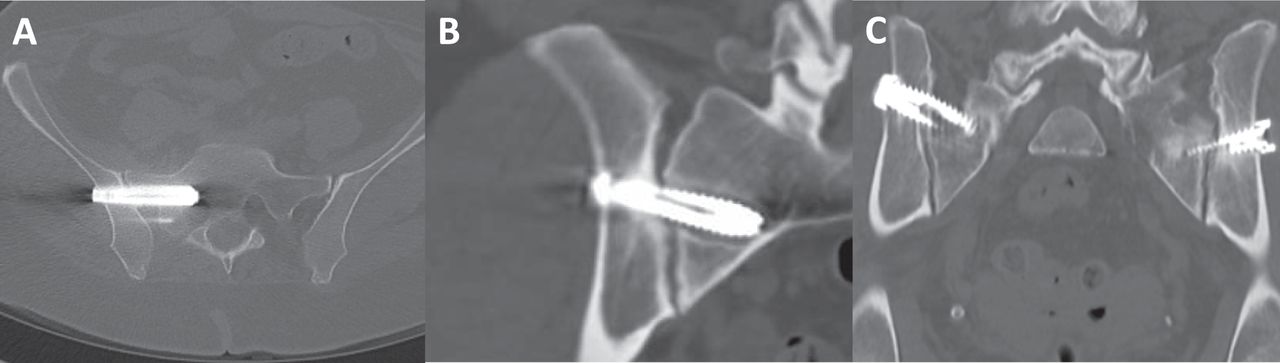
Consideration for a revision SIJ fusion starts with a thorough history and physical examination. Characterizing the preoperative and postoperative symptomatology, as well as ruling out other concomitant pathology is critical. If available, prior surgical records help to determine initial surgical indications and implant specifications while a computed tomography (CT) scan can help identify the exact cause of failure. The CT scan may identify implant violation of the sacral foramina and/or ala associated with radiculopathy (Figure 1A). Alternatively, it may show haloing around implants, indicative of loosening. Loosening of implants across the SIJ is often characterized by lucency about the sacral side of the component with a well-fixed ilium component, indicative of a windshield wiper phenomena (Figure 1B). However, it should be emphasized that radiographic findings must be correlated with clinical examination. Additionally, loosening typically presents 6 months to 1 year postoperatively as recurrence of SIJ pain after initial resolution. The other mode of failure that can also be readily identified on CT scan is related to an underappreciation of SIJ anatomy at the index procedure. The ventral one third of the SIJ is cartilaginous, whereas the dorsal two thirds is ligamentous in nature (Figure 2). Implants placed through the ligamentous portion of the joint span a larger intraarticular distance, decreasing the chance for bony bridging across the joint and decreasing implant purchase (Figure 1C). In cases of dorsally positioned implants, patients can fail to improve significantly or experience early recurrence of symptoms.

Three modes of failure in index sacroiliac joint (SIJ) fusion necessitating revision. (A) Violation of foramina causing radiculopathy. (B) Implant loosening about sacral aspect of implant. (C) Implant spanning the ligamentous portion of the SIJ.
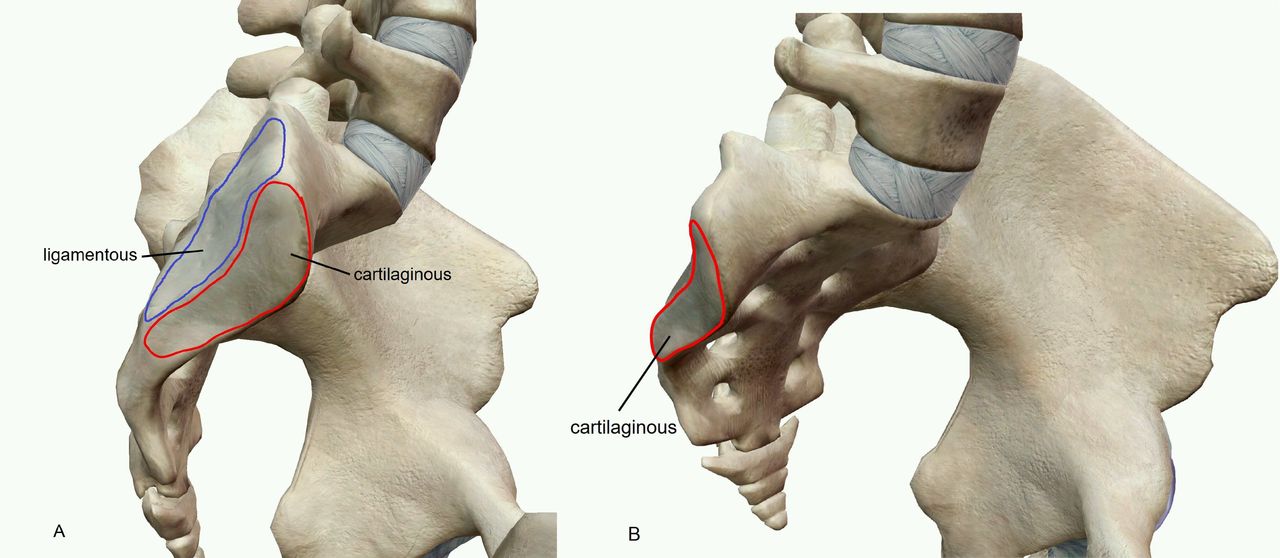
(A) Lateral graphic of the sacroiliac joint showing the posterior/dorsal ligamentous portion of the joint and the anterior/ventral cartilaginous portion of the joint. (B) Oblique graphic highlighting the narrow ventral true cartilaginous portion of the joint that is the target for implant placement. Image courtesy of Visible Body.
Intraoperative
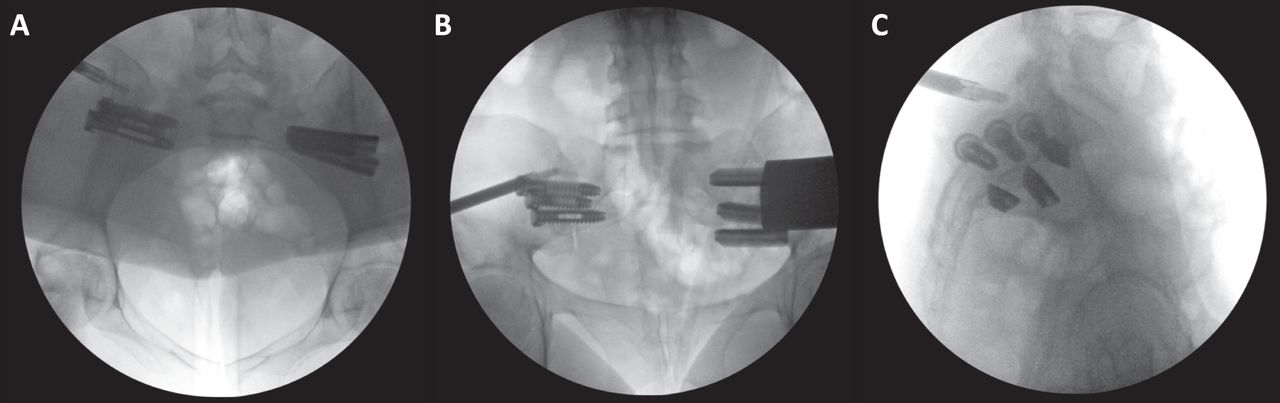
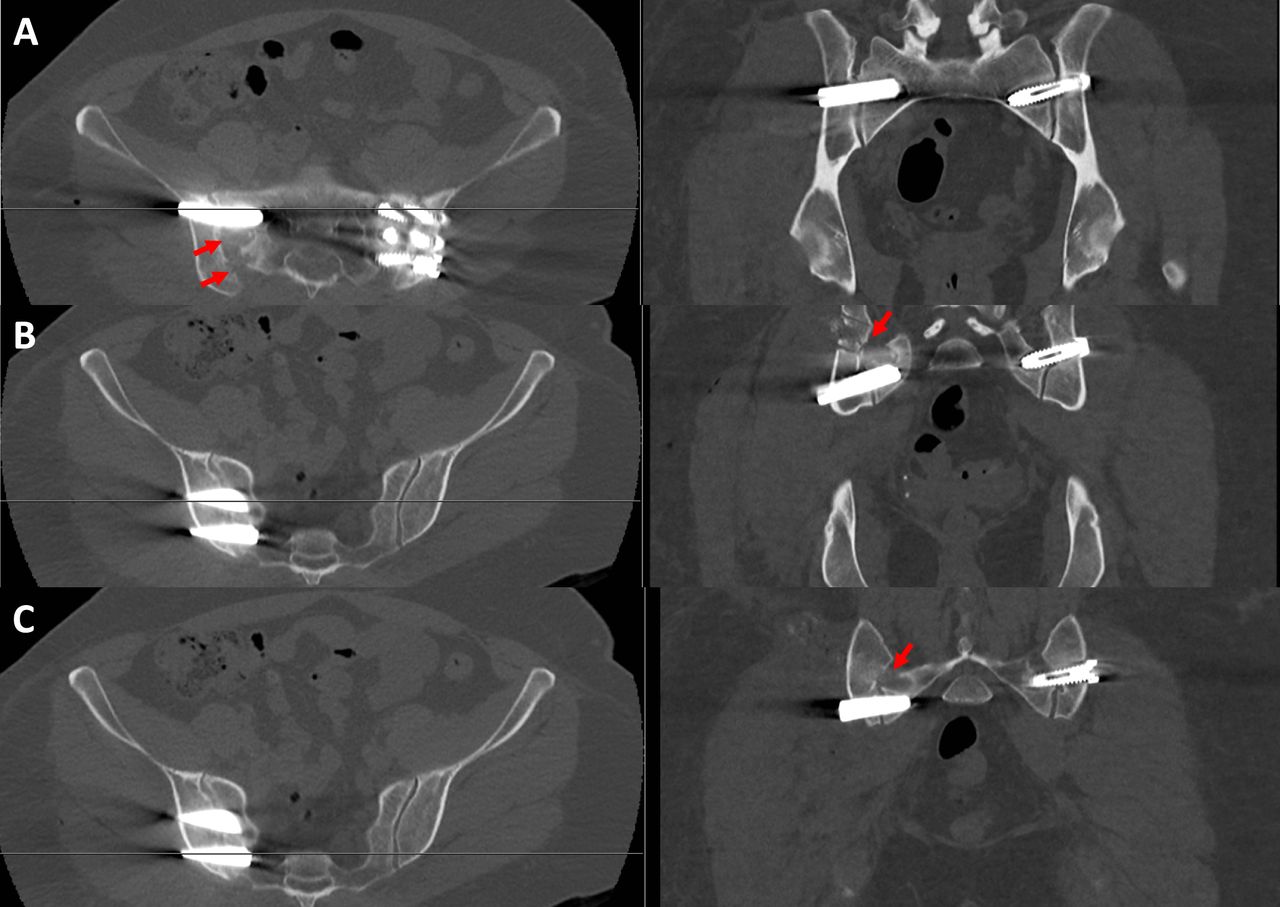
Fluoroscopic imaging is used to localize the previously identified loose and/or symptomatic implants. A 2-cm incision is made over the implant and blunt dissection is performed in line with muscle fibers of the gluteus maximus. A spine tubular retractor is placed through the incision and centered over the implant (Figure 3). The implant is removed with a screw removal set and/or osteotomes so that revision implants can be placed in a new trajectory across the SIJ without concern for implant convergence. Bone graft and bone morphogenetic protein are packed into the empty implant tracts. Of note, not all previous implants necessitate removal. Next, under stereotactic navigation, Steinmann pins are drilled across the ventral portion of the SIJ in new trajectories. Stereotactic navigation allows these trajectories to be placed in the narrow corridor of the cartilaginous SIJ, which is typically ventral to the old implant tracks. With the use of stereotactic navigation and an appreciation of SIJ anatomy, the orientation of trajectories tends to be more anterior to posterior and more inferior to superior than the previously placed implants (Figure 4). Ideally, the most cephalad implant is placed adjacent to the sacral ala, ventral to the S1 neuroforamen. The middle implant is directed at the S1 neuroforamen stopping short of the foramen, while the caudal implant is placed between the S1 and S2 foramina (Figure 5). Without navigation, this level of precision is challenging. In our series, triangular shaped titanium implants with porous titanium plasma spray coatings were used for SIJ fusion revision, passing each one over the previously drilled Steinmann pins.

Removal of loose implant with tubular retractor, screw removal set, and osteotomes.

Inlet (A), outlet (B), lateral (C) fluoroscopic views after navigation assisted placement of newly revised triangular implants with comparison to previously placed contralateral circular implants, highlighting the more ventral triangular implants. The ventral trajectory crosses the cartilaginous portion of the joint.

Axial and coronal postoperative computed tomography scans localized over the revised cephalad (A), middle (B), and caudal (C) navigated triangular implants, with previously placed contralateral circular implants. Red arrows: old implant tracts.
Postoperative
Patients are made protected weight bearing with crutches for 6 weeks postoperatively; however, pain typically resolves prior to the initial follow-up requiring continued emphasis on prescribed weight bearing status due to frequent noncompliance.
RESULTS
Five patients, including 2 military active duty members and 1 previously retired military member, underwent SIJ fusion revision from 2015 to 2018. Reasons for revision included SIJ pain recurrence from implant loosening/malposition and radiculopathy from nerve root irritation. The mean age at time of revision was 48.8 ± 14.3 years, and the mean follow-up after revision was 2.2 ± 0.9 years. Four of 5 patients were female. All patients reported improvement or complete resolution of their radiculopathy or SIJ-related pain at final follow-up. Additionally, when performed, follow-up CT imaging demonstrated interosseous bridging of the SIJ at 2 years (Figure 6).

Computed tomography scan demonstrating interosseous bridging anterior to the implant across the cartilaginous portion of the sacroiliac joint.
After revision surgery, 2 patients developed subsequent trochanteric bursitis and 2 other patients noted dissimilar low back pain. The trochanteric bursitis resolved in both patients with conservative management and injections. The low back pain in 1 patient was managed conservatively with injections, whereas the other patient underwent L1 to pelvis fusion by another surgeon. Both active duty service members separated from the military, with 1 now working as a prison guard and the other fully retired.
DISCUSSION
Implicit in a discussion of novel surgical techniques and management in the revision setting is the importance of appropriate initial surgical indications. In the case of SIJ dysfunction, there may be diagnostic uncertainty, highlighting the importance of preoperative identification of specific pain generators. Patients should undergo an exhaustive course of nonoperative treatment modalities, including diagnostic and therapeutic injection, prior to consideration of surgical management. In a potential revision case, understanding the index preoperative symptomatology and postoperative course can help guide management. Recurrence of pain, new or worsening radiculopathy, and continued pain after surgery should raise concern for pseudoarthrosis, malposition of implants, and/or missed concomitant pathology. Advanced imaging should serve in a confirmatory capacity.
Prior to performing SIJ fusion in any manner, index or revision, an understanding of the anatomic/histologic joint morphology is key. Implants should be placed across the more ventral cartilaginous portion of the SIJ to allow for interosseous bridging across the joint as described by Rudolf and Capobianco.5 Interosseous bridging is a radiographic marker for successful fusion, and it is hypothesized that the larger intraarticular distance spanned by more dorsal implants may inhibit interosseous bridging.
Visualization of SIJ anatomic landmarks is challenging, but there is an even higher degree of difficulty when targeting specific foraminal corridors in the ventral cartilaginous portion of the joint while attempting to avoid old implant trajectories. Considering this added complexity, stereotactic navigation becomes indispensable. There is no consensus on the superiority of stereotactic navigation over conventional fluoroscopy in SIJ fusion, but a systematic review of imaging modalities for percutaneous iliosacral fixation for pelvic fractures demonstrated decreased rates of implant malposition for CT navigation and a trend toward decreased malpositioned implant rates for other 2D or 3D navigation modalities compared with conventional fluoroscopy.8
Though there are likely other complications and considerations (ie, infection and loss of bone stock) not encountered in our cohort, this study provides a blueprint for revision minimally invasive SIJ fusion. The techniques described highlight how to safely revise (and avoid) a failed SIJ fusion with emphasis on appropriate surgical indications, preoperative planning, respect for SIJ anatomy, and use of intraoperative navigation.
Footnotes
Disclosures and COI: Anton Y. Jorgensen, MD, is a paid consultant for SI-Bone.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}