


ABSTRACT
Background: We report a case of an elderly patient who was diagnosed with lateral atlantoaxial subluxation with type II odontoid fracture, an extremely uncommon upper cervical spine injury that has not been previously reported in the literature to the knowledge of the authors.
Methods: An 87-year-old male reported to the emergency room following a syncopal episode after sustaining a fall. He complained of dizziness, fatigue, disruption of vision and audition, and worsening neck pain. Computed tomographic scans were positive of partial dislocation of the C1 relative to C2 and chronic fracture of dens classified as type II according to the Anderson and D'Alonzo classification system. Magnetic resonance imaging further revealed large fracture pannus tissue at the level of the dens, reducing the space in the spinal cord. There was no evidence of spinal cord injury. Atlas-axis fusion with instrumentation was performed to manage the injury. A review of the classification, occurrence, and management of upper cervical spine surgeries was performed.
Results: An acute injury to a previously unrecognized type II odontoid fracture with partial C1-C2 dislocation was identified as a rare upper cervical spine injury and classified based on the Anderson and D'Alonzo and Fielding and Hawkins classification systems. The decision was made to perform instrumented spinal fusion by inserting mass screws into C1, pars screws into C2, and locking rods to realign the vertebral bodies and address the atlantoaxial instability. Follow-up scans indicated good postsurgical reduction and fixation, including resolution of the pannus overgrowth without direct intervention.
Conclusions: Lateral atlantoaxial subluxation with chronic type II fracture of the dens constitutes a rare injury of the upper cervical vertebrae. Posterior instrumented spinal fusion was used to effectively manage the injury, leading to reabsorption of retro-odontoid pannus tissue.
INTRODUCTION
Lateral subluxation of the atlas (C1) and axis (C2) associated with type II odontoid fracture of the dens is very rare. Fractures of the dens, however, are the most common injury to the C2 vertebra.1 Of these, type II fractures are the most prolific.2 Among combined injuries of the cervical spine, rotational atlantoaxial subluxation with type II dens fracture were reported in <0.3% of cases.3 After conducting a literature search of PubMed, Scopus, Google Scholar, and relevant reference lists, we found only 1 other published case of lateral C1 subluxation.4 Therefore, the reported case of lateral subluxation of C1 relative to C2 is a rare injury. Traumatic atlantoaxial dislocation is an often lethal injury involving atlas-axis fractures, fracture of odontoid process, and/or other cervical spine fractures that result from high-velocity trauma.5 Furthermore, fractures of the odontoid process are usually more common in the elderly and may go unnoticed due to a lack of neurological deficit.6 Odontoid fractures are known to predispose toward atlantoaxial instability.7 In this case, the type II fracture of the dens was an old injury. Retro-odontoid pannus tissue, which was discovered in the spinal canal at the level of the dens, had significantly narrowed the canal. Pannus overgrowth is of concern due to the potential for inducing spinal stenosis and consequent myelopathy.8 Posterior instrumented fusion has been reported to effectively correct these injuries and lead to dissolution of pannus tissue.9–10 The injury was treated by initial stabilization with hard collar, followed by posterior fusion with pedicle screws, pars screws, and locking rods.
CASE REPORT
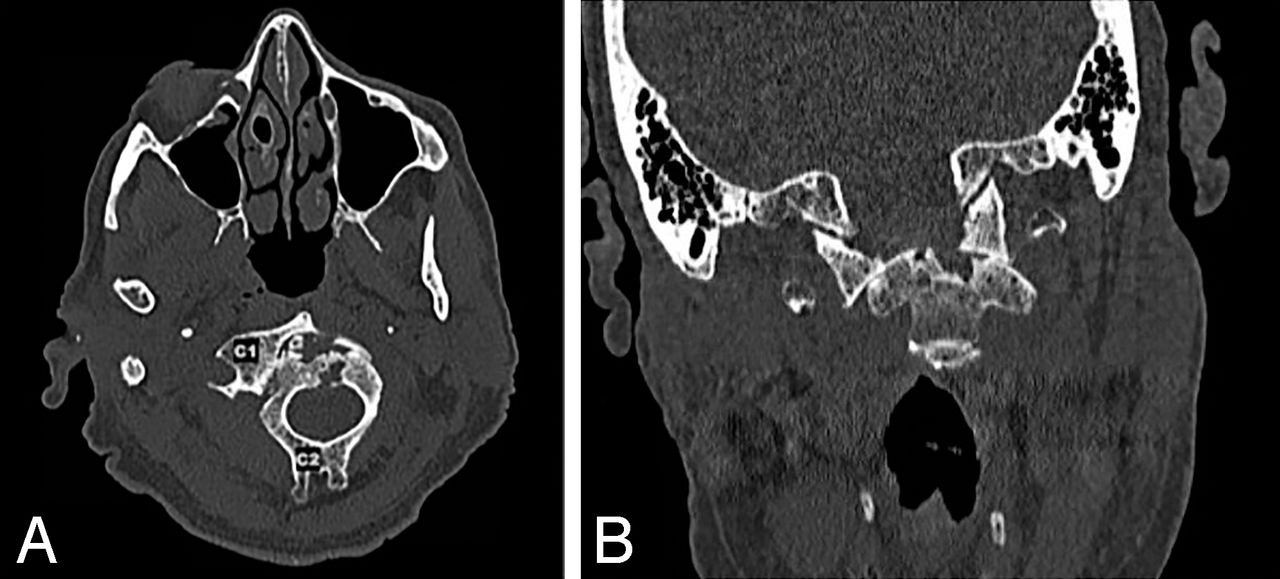
In July 2016, an 87-year-old man was admitted to the emergency room with a chief complaint of syncopal fall in the shower. The patient reported dizziness and fatigue, and the physical exam revealed disruption of visual and auditory perception. He also noted worsening neck pain that had begun after a fall he had sustained in December 2015. His past medical history included diabetes mellitus, hypertension, liver cirrhosis, and atrial fibrillation. Radiographic evaluation revealed a chronic odontoid fracture identified as type II according to the Anderson and D'Alonzo classification system.1 Computed tomography of the cervical spine also revealed an acute nondisplaced fracture of the right C2 transverse process involving the transverse foramen (Figure 1).

Atlantoaxial subluxation and chronic odontoid fracture. Computed tomographic (CT) scan showing fracture of the C2 transverse process and subluxation of C1 relative to C2 (A). CT scan showing old type II odontoid fracture (B).
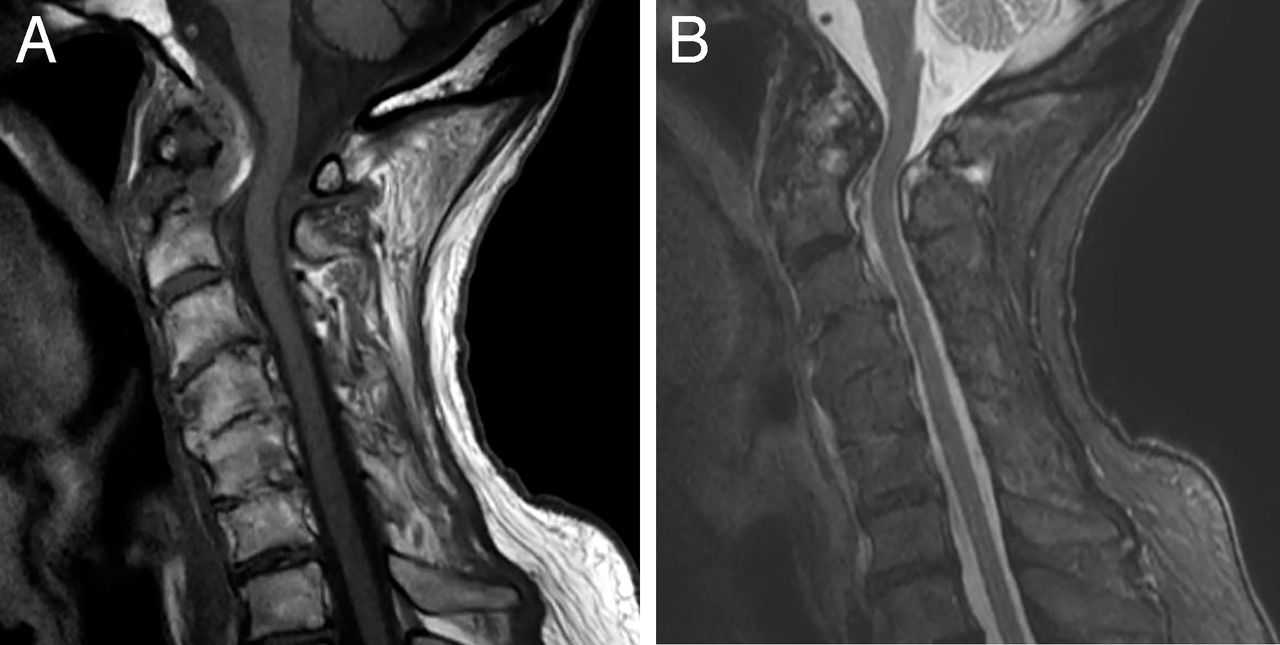
Significant subluxation (7 mm) of C1 and the odontoid tip was discovered to the right relative to C2. It was possible that the initial fall in December 2015 produced the fracture in the odontoid process, which is known to predispose toward atlantoaxial instability.7 Magnetic resonance imaging of the cervical spine was performed to investigate the potential of spinal cord injury (SCI). Findings were consistent with a chronic unstable C2 dens fracture with a large pannus at the dens level in the spinal canal (Figure 2). Although the space available for the spinal cord was significantly reduced, the spinal cord was not under compression, and results were negative for SCI.

Retro-odontoid pannus tissue. T1-weighted magnetic resonance image of spine displaying retro-odontoid pannus (A). T2-weighted scan showing old type II odontoid fracture (B).
His neck was initially stabilized with a hard collar. Posterior pedicle screw fixation of C1-C2 with bone graft fusion has been recommended as a safe and effective surgical treatment of atlantoaxial dislocation associated with old odontoid fracture.9 We performed C1-C2 fusion with instrumentation with careful reduction of the dens in both planes under C-arm control. Postoperative x-rays indicated improved atlantoaxial alignment and reduction of the subluxation, which included improvement in the alignment of the odontoid fracture. There were no intraoperative complications, and the patient's hospital stay was uncomplicated. Follow-up x-rays at 1.5 years after surgery revealed adequate fixation (Figure 3). The patient had full range of motion, no functional restrictions, and no lingering neck pain.

Postoperative images. X-ray demonstrated adequate fixation of instrumentation.
DISCUSSION
Literature Review
We conducted a review of the literature pertaining to traumatic cases of odontoid fractures with concomitant atlantoaxial dislocation by searching the following databases: PubMed, Scopus, and Google Scholar. Reference lists were also searched for relevant articles. We identified several case reports and case series describing the occurrence and management of combined C1-C2 dislocation and fracture of the dens.4,9,11–24 Corner described 2 of the earliest cases of rotatory dislocation of C1 relative to C2 with accompanying fractures of the odontoid process.25
Classification
Odontoid fractures are classified according to the Anderson and D'Alonzo system, which delineates 3 fracture types (Table 1).1,26 Atlantoaxial subluxation may be translational, rotatory, or distractive and is commonly classified according to the Fielding and Hawkins criteria (Table 2).15,26,27 A fifth category was described by Levine and Edwards.26,28 For this case, the partial translational atlantoaxial luxation could not be classified according to the Fielding and Hawkins criteria, but the associated fracture of the dens was determined to be type II based on the Anderson and D'Alonzo system. Furthermore, the presence of pseudotumor pannus tissue was confirmed within the spinal canal at the level of the dens. Retro-odontoid pannus refers to a granulation tissue frequently encountered in cases of inflammatory disease, such as rheumatoid arthritis, but may also occur in noninflammatory cases.29 If left unchecked, retro-odontoid pannus may lead to spinal stenosis and myelopathy.8
Anderson and D'Alonzo classification of odontoid fractures.
Fielding and Hawkins classification of atlantoaxial subluxation.
Prevalence
Traumatic atlantoaxial dislocation is an often lethal injury involving atlas-axis fractures, fracture of odontoid process, and/or other cervical spine fractures that result from high-velocity trauma.5 Traumatic atlantoaxial dislocation may occur with concurrent fracture of the odontoid process.11–12,15–19,22–24 However, C1-C2 subluxation has also been identified in patients with old odontoid fractures.9,13,20,21 Fuentes et al13 reported a case of posterior subluxation associated with an old type II odontoid fracture. Li et al21 described a patient with dorsal subluxation and a chronic type II dens fracture. Both type II and type III odontoid fractures have been associated with C1-C2 dislocations along the antero-posterior axis.9 Our case of acute lateral atlantoaxial subluxation with chronic type II odontoid fracture has not been previously reported in the literature.
Management
Immobilization remains controversial, particularly in the case of type II odontoid fractures with concomitant C1-C2 fracture.2,30 Conversely, immobilization via collar is preferred in the elderly, but surgery may be required in the presence of significant instability.31 In this case, given the atlantoaxial instability, spinal stenosis secondary to pannus overgrowth, and myelopathy secondary to cervical spinal stenosis, surgery was performed. Posterior screw fixation of C1-C2 with bone graft fusion has been demonstrated as a safe and effective surgical management of atlantoaxial subluxation associated with old dens fractures.9 However, fixation of C1-C2 with the transarticular screw technique carries the risk of spinal cord injury, nerve injury, or injury to the nearby vertebral artery.32 Moreover, the vertebral artery may erode with age such that it is directly in the path of the screw. Biomechanical testing has shown that a C1 lateral mass screw with a C2 pars screw construct allows an average of 0.6 degrees more motion than does a C1-C2 transarticular screw.33
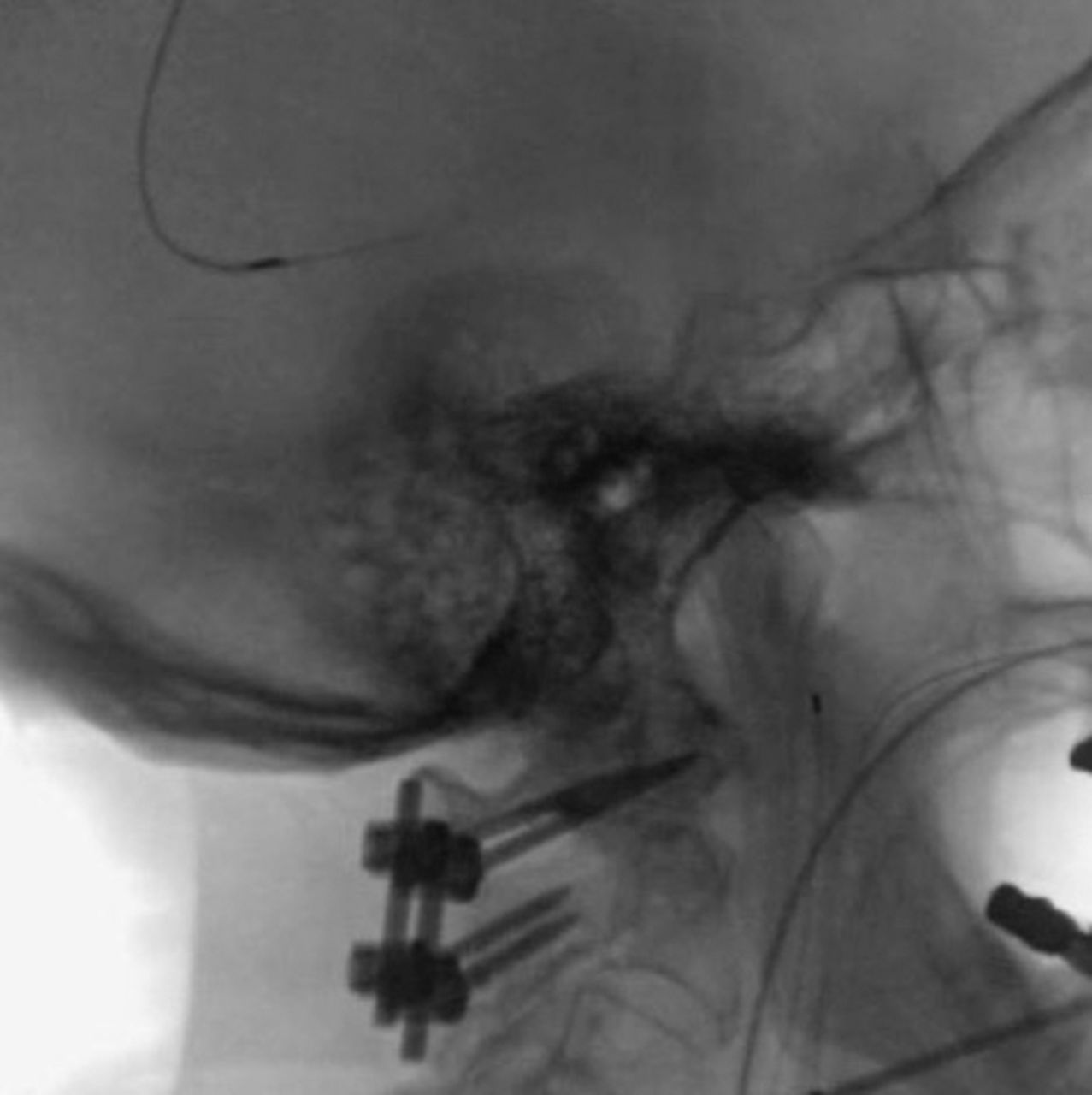
As a result, for this case it was decided to proceed with fusion by inserting lateral mass screws into C1 and pars screws into C2 and to place locking rods, similar to the technique first described by Goel et al.32–34 Intraoperative fluoroscopy was performed to ensure accurate placement of screws (Figure 4).

Intraoperative images. Fluoroscopic image of cervical spine demonstrating accurate fixation.
Reabsorption of pannus tissue and resolution of clinical symptoms has been reported in patients with atlantoaxial instability or subluxation following correction.29 For example, Shah et al10 reported 2 cases of atlantoaxial instability with retro-odontoid pannus tissue that resolved in the immediate postoperative period following surgical correction of the instability. Barbagallo et al29 reported gradual progressive reabsorption with disappearance at 6 to 13 months in 3 cases and significant resolution of pannus at 14 months in 1 case. It must be noted that in the 2 previously mentioned studies, pannus reabsorption occurred not with direct intervention but rather from correction of the underlying atlantoaxial instability.
CONCLUSIONS
Traumatic atlantoaxial subluxation with fracture of the dens is an exceedingly uncommon upper cervical spine injury. Lateral subluxation with an accompanying chronic type II odontoid fracture is rarer still. Posterior instrumented fusion was successful in addressing this traumatic injury and resulting in resolution of pannus tissue.
Footnotes
Disclosures and COI: The authors declare no conflicts of interest. The institutional review board (IRB) of the University of California, Irvine, deemed this study to constitute a nonresearch endeavor, which therefore did not require IRB approval. Patient confidentiality has been protected according to the US Health Insurance Portability and Accountability Act (HIPAA) and in accordance to the tenets established by the Declaration of Helsinki for human subjects. The patient provided verbal consent after being asked if the material in this case report may be published.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2019 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.