


Abstract
Objectives To identify the profile and management of patients with upper cervical spine injury.
Methods Retrospective cohort study of patients with upper cervical spine injuries managed at Hospital da Restauração between 2014 and 2020.
Results It presents the profile of 145 injuries recorded by location and classification among the 120 patients, and the management performed. Men are more affected than women, almost half of the patients (42.5%) were aged 16 to 29 years. Neurological deficit was present in 18 cases (15%). Twenty cases presented injury involving the level C1. Most injuries (109 [90.8%]) occurred at the C2 level, the most frequent of which were as follows: isolated type II odontoid fracture (29.2%), miscellaneous fracture of C2 (20%), and isolated hangman’s fracture (13.3%). The most used management in type II odontoid fracture was C1-C2 posterior arthrodesis (17/42) followed by odontoid osteosynthesis (12/42). Regarding isolated hangman’s fracture, conservative management was performed in 37.5% (6/16), and the technical approach most performed was anterior C2-C3 discectomy and interbody fusion (5/16).
Conclusions Upper cervical spine injury has a higher prevalence in young men and is most often caused by traffic accidents. The main level affected is C2, and type II odontoid fracture is the most frequent subtype. C1 injury is related to conservative treatment, while C2 or combined C1-C2 injury is related to surgical approach. The management of these injuries is mainly performed with surgical treatment, with C1-C2 posterior arthrodesis and anterior odontoid osteosynthesis representing most of the approaches.
Introduction
Upper cervical spine (UCS) injury is an important source of morbidity and mortality, especially in young populations, causing significant social and economic damage. UCS is commonly associated with high-energy trauma that affects the skull base, the atlas (C1), and the axis (C2). Patients with these injuries present peculiar characteristics owing to the complex bone, vascular, and ligament anatomy of the craniocervical junction, which substantially differ them from the lesions of the subaxial cervical spine.1–3
Traumatic injuries of the UCS can be classified into isolated ligament lesions, isolated bone fractures, or mixed ligament and bone lesions. Among the ligament lesions, there are atlanto-occipital displacement, transverse ligament injury, and atlantoaxial displacement. Regarding isolated bone fractures, there are atlas (C1), axis (C2), and combined fractures. Atlas fractures can be classified by following fracture pattern as described by Hadley et al (1988).4 Type I fractures are isolated to the anterior or posterior arch, a rare injury with intact transverse ligament. Type II injuries, also known as Jefferson’s fractures, are burst fractures with bilateral fractures of the anterior and posterior arch of C1. Type III fractures involve the lateral mass. Fractures of the axis have been divided into 3 general subtypes: fractures of the odontoid process, traumatic spondylolisthesis of the axis (hangman’s fractures), and miscellaneous (nonodontoid nonhangman’s fractures of the C2 vertebra). Each of these fracture subtypes has been further subdivided. Based on the Anderson and D’Alonzo classification, odontoid fractures present 3 subtypes. Type I fractures are oblique fractures through the upper portion of the odontoid process. Type II fractures cross the base of the odontoid process at the junction with the axis body. Type III fractures are fractures through the odontoid that extend into the C2 body.2,3,5–7 The management of these injuries varies according to the anatomic features and the functional significance of the individual fracture injury.1,3,8
The annual incidence of traumatic spinal cord injury in the United States is around 40 cases for each million people.9 Globally, the incidence ranges from 10.4 to 83 in developed countries, with 53.9% of those cases affecting the UCS.10 Recent data showed that accidents with motor vehicles correspond to the main mechanism, with 42.4% incidence, followed by fall (21.8%), and physical aggression (17.4%).10
The increasing prevalence of UCS injury is associated with increasingly high costs of hospitalization, rehabilitation, equipment, medications, loss of productivity, and retirements.3,11 Considering its high incidence and significant economic and social impact, the characterization of the epidemiological profile and management of UCS injury is a fundamental tool to optimize preventive actions and enable the most appropriate management of this group of injuries. Therefore, this study presents the profile and management of a series of 120 cases of UCS injury at the Hospital da Restauração in Recife, Brazil.
Methods
The present study is a descriptive retrospective study of 120 patients who had a diagnosis of UCS injury and were admitted for the management of UCS injuries over a 6-year period (2014–2020) at the Hospital da Restauração, a referral neurological trauma service in the state of Pernambuco, Brazil, in the northeast region of Brazil.
The following variables were analyzed: gender, age, trauma mechanism, neurological deficit assessed by Frankel Scale,12,13 injury classification, and instituted treatment. Imaging was used to classify the types of fractures. Radiological analysis included standard radiography, computed tomography with multiplanar reconstruction, and magnetic resonance imaging in all patients. Treatments included conservative and surgical methods.
Regarding the sample composition, the inclusion criteria were patients hospitalized with injuries related to traumatic events in the UCS. Exclusion criteria were patients whose records had incomplete information regarding the identification of the proposed variables, patients with rheumatoid arthritis, and patients younger than 16 years.
Data were descriptively analyzed through absolute and percentage frequencies for categorical variables and measurements: mean, SD, and median deviation of the age variable. To evaluate association between the 2 categorical variables, the Fisher’s exact test was used (since the condition for the use of the χ 2 test was not verified). The margin of error used in the decision on statistical tests was 5%.
The records were available for analysis only after the approval of the Institution’s Research Ethics Committee. Researchers were committed to the privacy and confidentiality of the data used, fully preserving the anonymity of the data found in the patients’ records. All the patients were registered and identified through electronic medical records and record number.
Results
A total of 135 patients were initially identified; however, 7 patients were excluded due to incomplete information regarding the identification of the proposed variables, 5 patients were excluded due to their age (patients younger than 16 years), and 3 patients were excluded due to the presence of rheumatoid arthritis. Among the remaining 120 patients, we recorded and profiled 145 injuries by location and classification, as well as the management performed (Table 1).
Upper cervical spine injury level and classification (N = 120).
The epidemiological profile of the sample researched is presented in Table 2. Young adults were concerned in 60% of cases ranging from 16 to 82 years with a mean (SD) age of 38.0 (17.6) years and a median of 33.5 years. Nearly half of the patients (42.5%) were 16 to 29 years old. The majority (90%) of the patients were men, and the most frequent trauma mechanisms were motorcycle accident (31.7%) followed by car accident (24.2%). Neurological deficit was present in 18 cases (15%). No significant associations (P > 0.05) were recorded between neurological deficit and the sample characterization variables (Table 3). Most patients were admitted with 24 hours delay (83%). Disorders of consciousness concerned 8 cases of serious polytrauma. There was 1 pregnant patient with hangman’s fracture who received conservative care.
Sample profile and evaluation of variables according to injury level.
Evaluation of variables according to neurological deficit.
A lower cervical spine injury was associated in 10 cases. One patient with cervical gunshot injury and miscellaneous C2 fracture died due to hemodynamic instability before surgery.
Regarding the spinal injury level, the majority of the sample (70%) had an isolated C2 injury level, 9.2% presented with an isolated C1 injury level, and 17.5% had C1-C2 injury.
The most frequent injury was isolated odontoid fracture, which was present in 35% of the sample, followed by miscellaneous C2 fracture (25%), and isolated hangman’s fracture (13.3%). The least frequent was combined odontoid fracture and hangman’s fracture (3.3%). The most frequent type of injury was type II odontoid fracture, presenting in 35 patients (29.2%).
Regarding the management, injuries considered unstable or with a high risk of instability were surgically managed. Injuries classified as AOspine type B (tension band/ligamentous injury), type C (translation injury), and type A with modifiers that suggest a risk of instability or nonunion fracture (such as type II odontoid fracture) were considered for surgical management.
Conservative treatment was performed in 44 cases (36.7%) of stable fractures using Philadelphia neck collar for 8 weeks. A total of 75 patients (62.5%) were operated on. Twenty-nine cases with posterior approach, including transoral odontoidectomy procedure and posterior fusion in 3 patients, isolated craniocervical fusion in 4 cases (Figure 1), and C1-C2 posterior arthrodesis (Figures 2–4), which is the technical approach most performed in this study, in 30 patients (25%). Both Goel-Harms and Magerl techniques of C1-C2 posterior fusion techniques were performed. In 23 cases, anterior approach was performed: 14 cases of odontoid screwing (Figures 5 and 6) and 9 cases of C2-C3 discectomy with bone graft and interbody fusion (anterior cervical discectomy and fusion) (Figures 7 and 8). A 360° cervical fusion was performed in 3 cases (Figure 9), including posterior wiring in 1 case (Figure 10). Among 11 cases of isolated C1 fracture, 10 were treated conservatively. There was no postoperative death (Tables 4 and 5). One patient in the sample was submitted to internal fixation with wiring (Figure 10), but we performed an additional anterior approach. It was not necessary to remove their hardware.

Postoperative standard x-ray images showing a patient who benefited from craniocervical fusion.
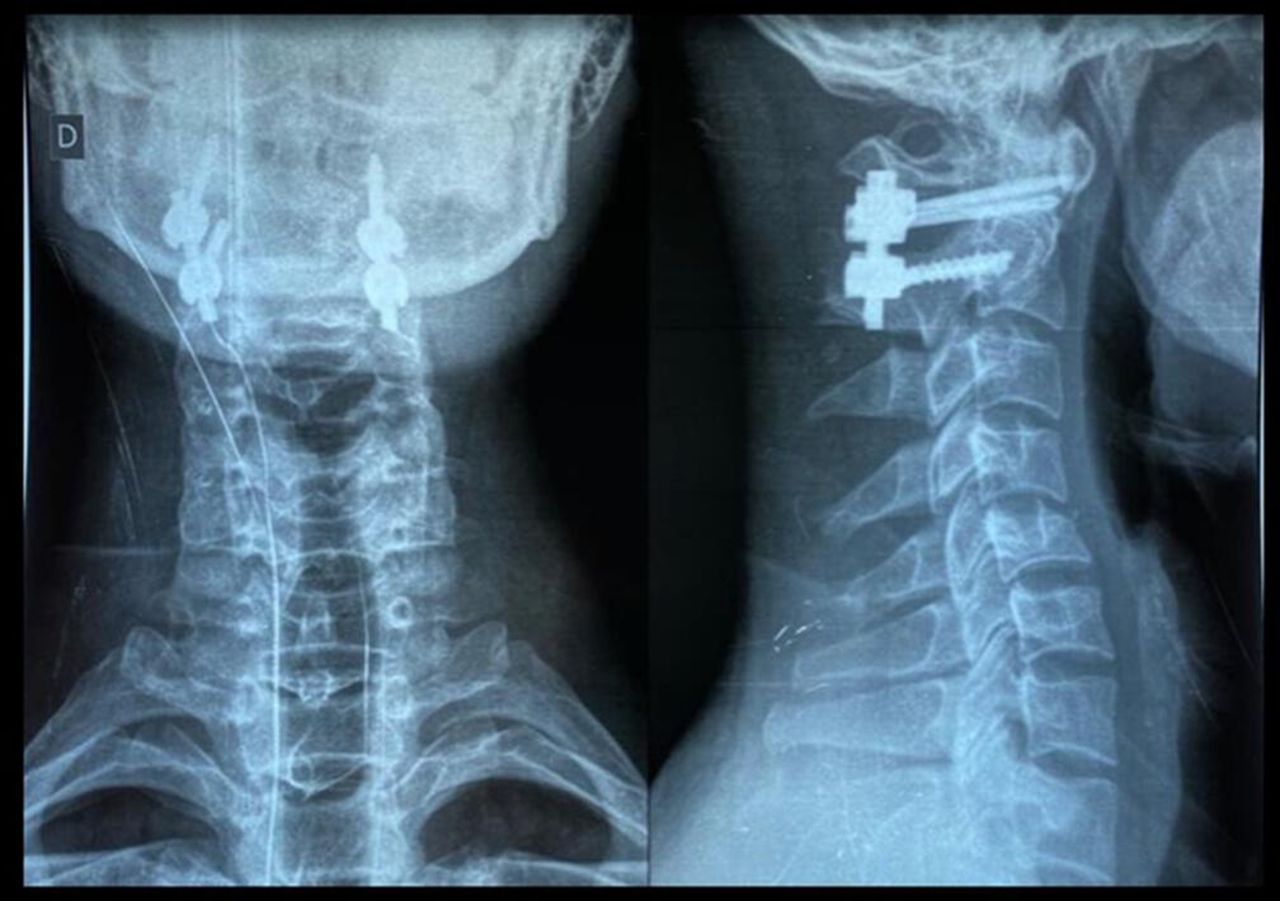
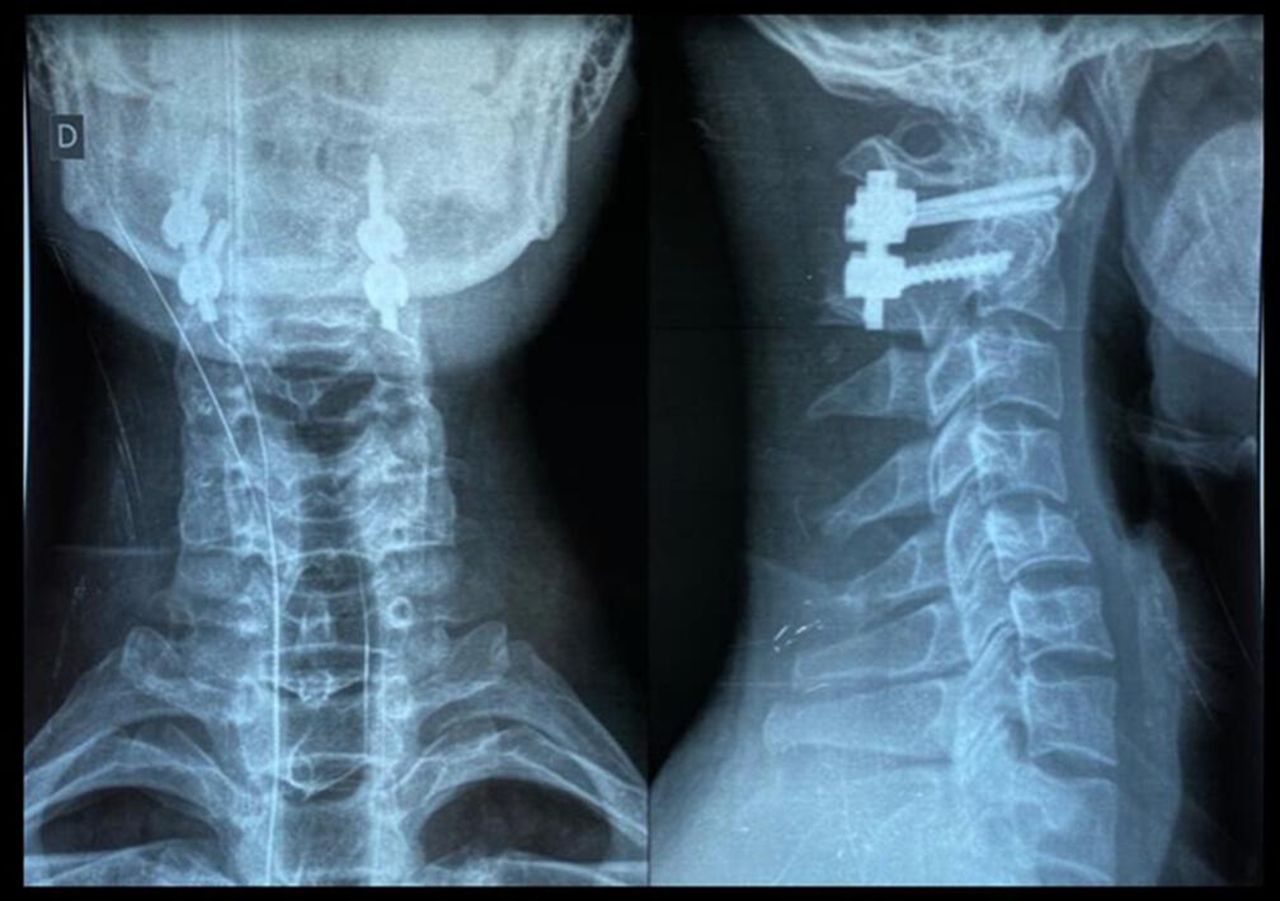
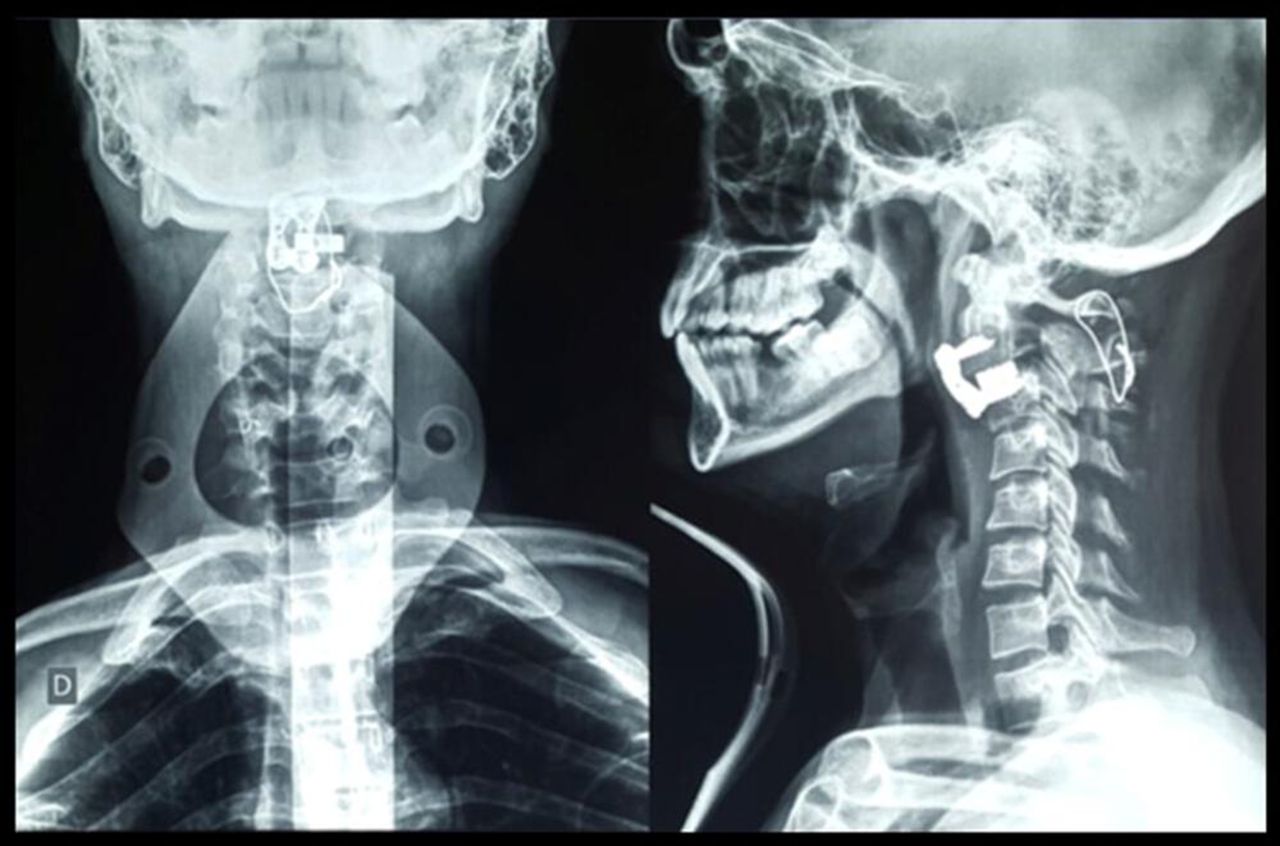
Postoperative standard x-ray images showing a patient who underwent a C1-C2 posterior arthrodesis (Goel-Harms technique).

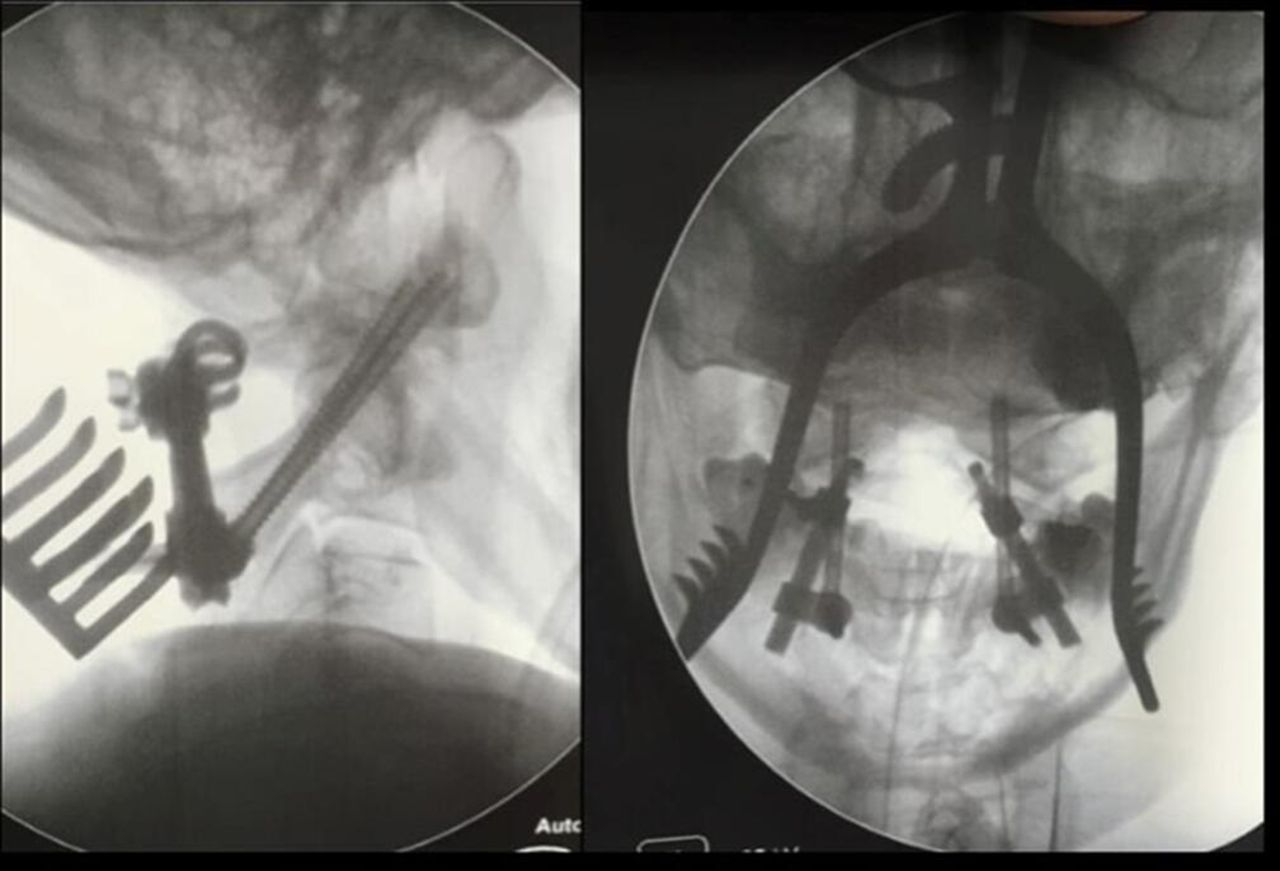
Intraoperative fluoroscopy showing a type II odontoid fracture. The patient who underwent a transarticular C1-C2 posterior arthrodesis (Magerl technique).

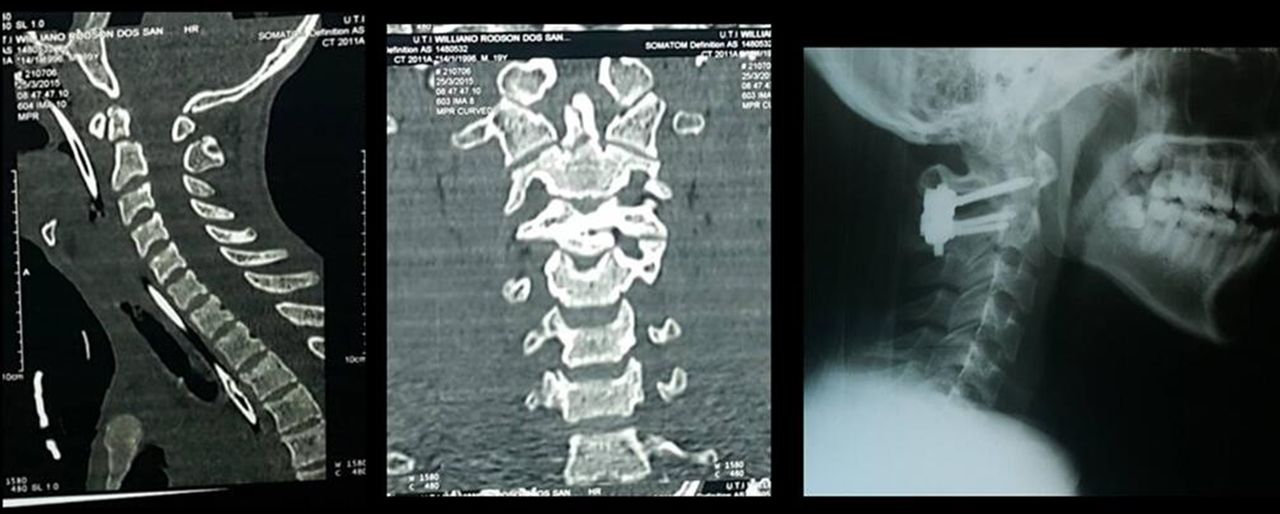
Preoperative computed tomography images showing a patient with type II odontoid fracture presenting a split in the odontoid process. The patient underwent a C1-C2 posterior arthrodesis (Goel-Harms technique), which is shown on a postoperative standard x-ray image.

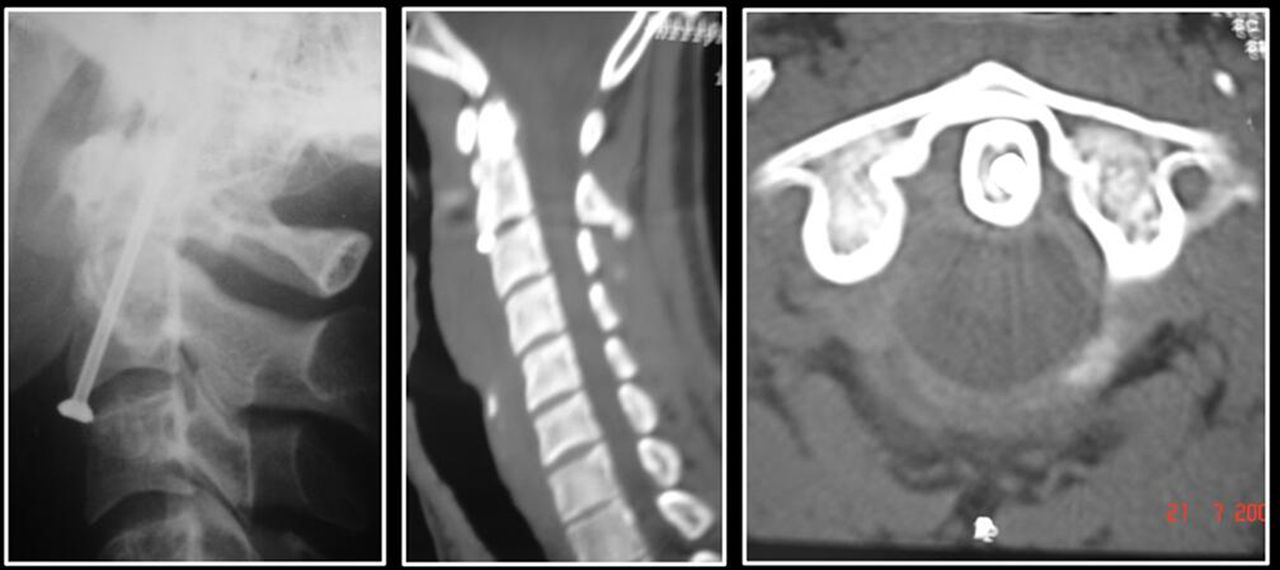
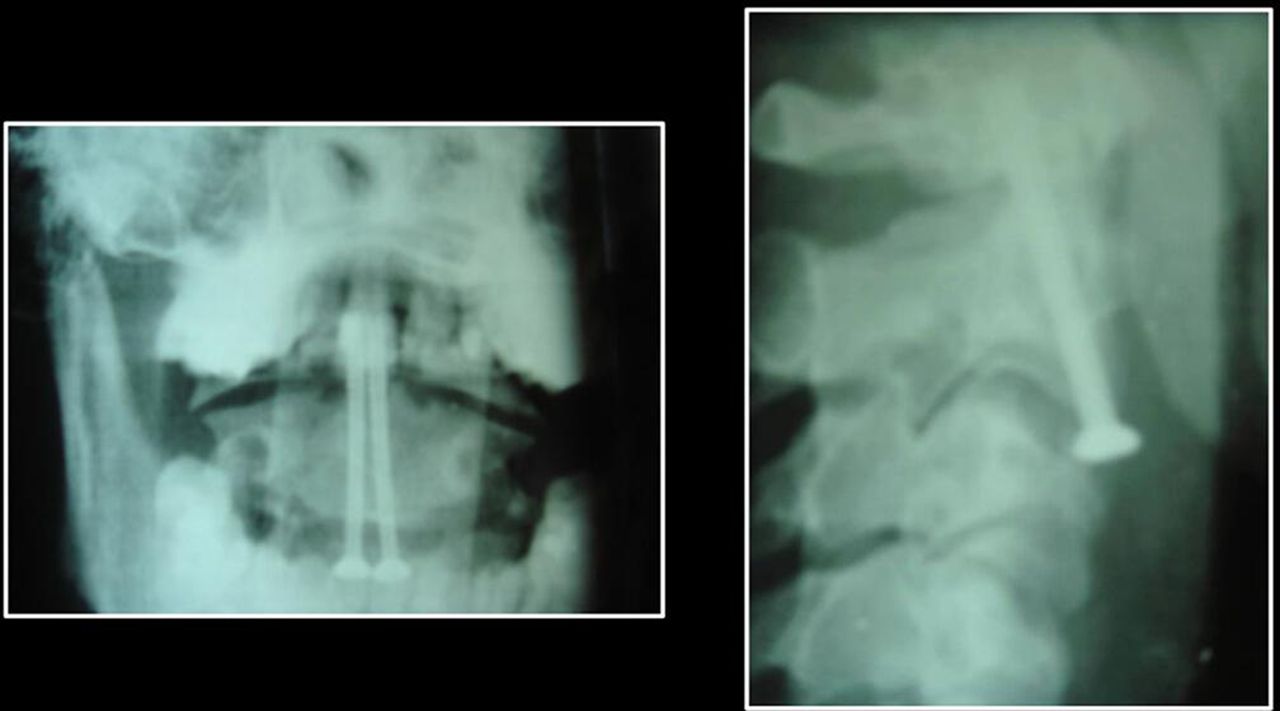
Postoperative computed tomography images showing a patient with type II odontoid fracture who benefited from anterior odontoid screwing.

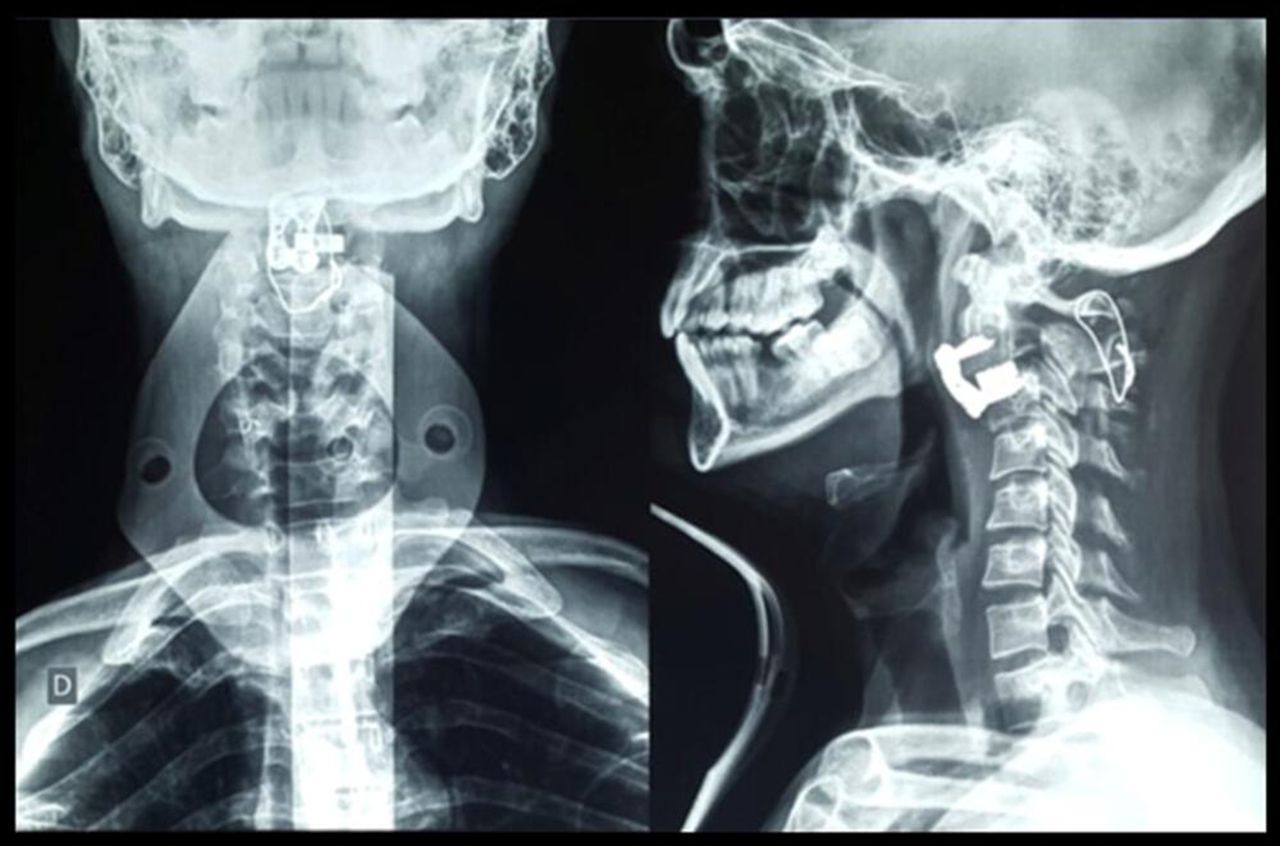
Postoperative standard x-ray images showing a patient with type II odontoid fracture who benefited from anterior fixation of the odontoid process with 2 screws.

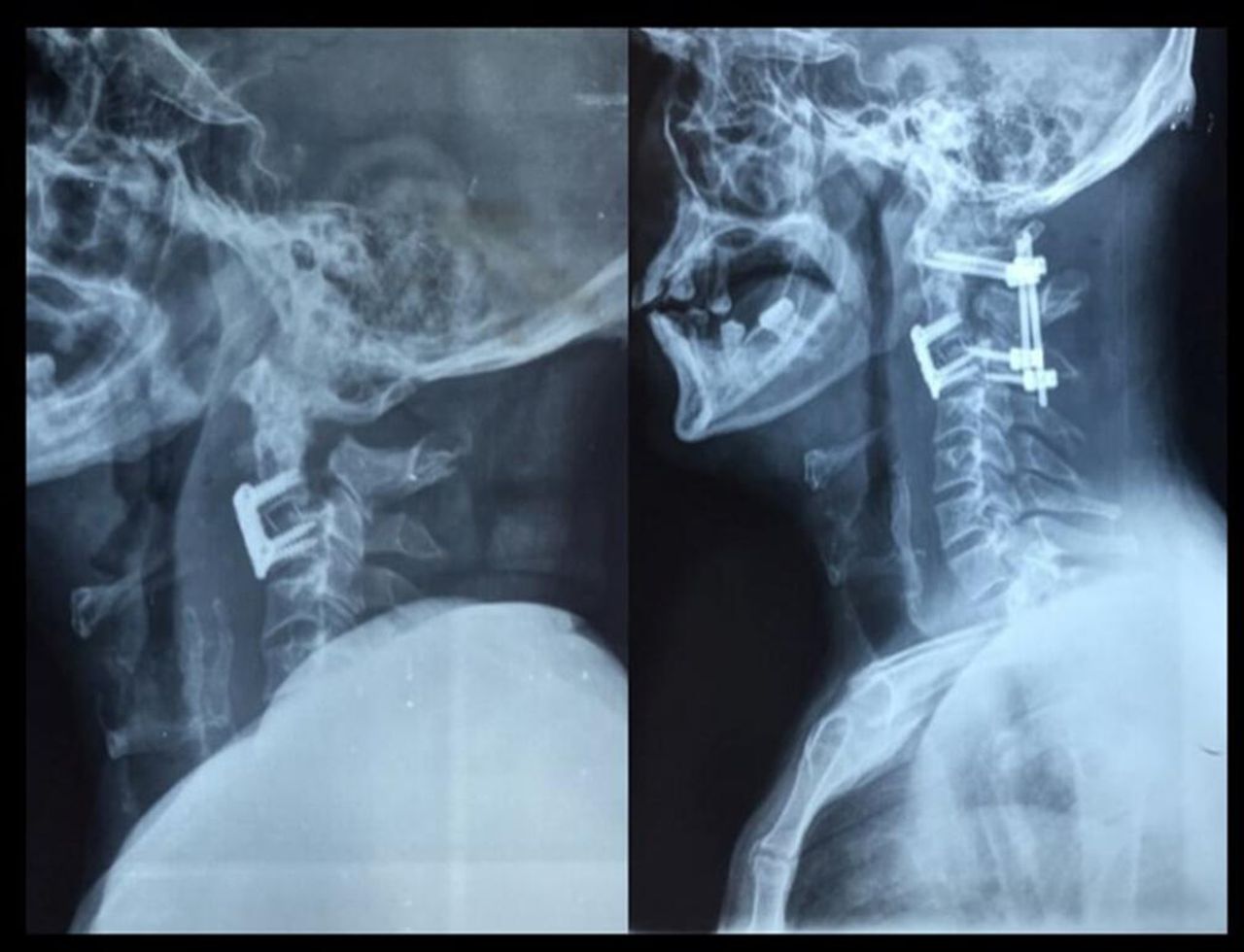
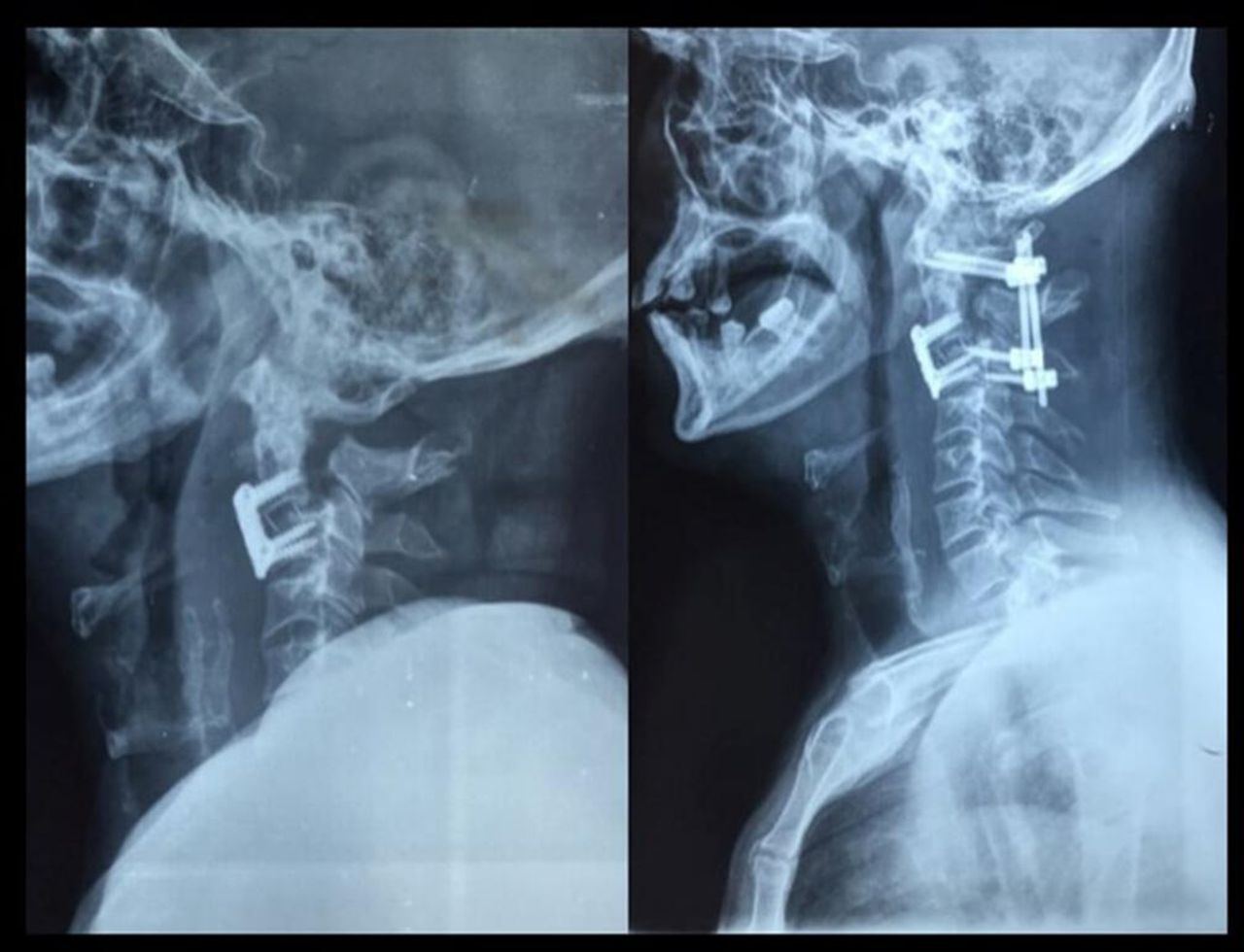
Preoperative and postoperative standard x-ray images showing a patient with hangman’s fracture who benefited from C2-C3 discectomy and interbody fusion.
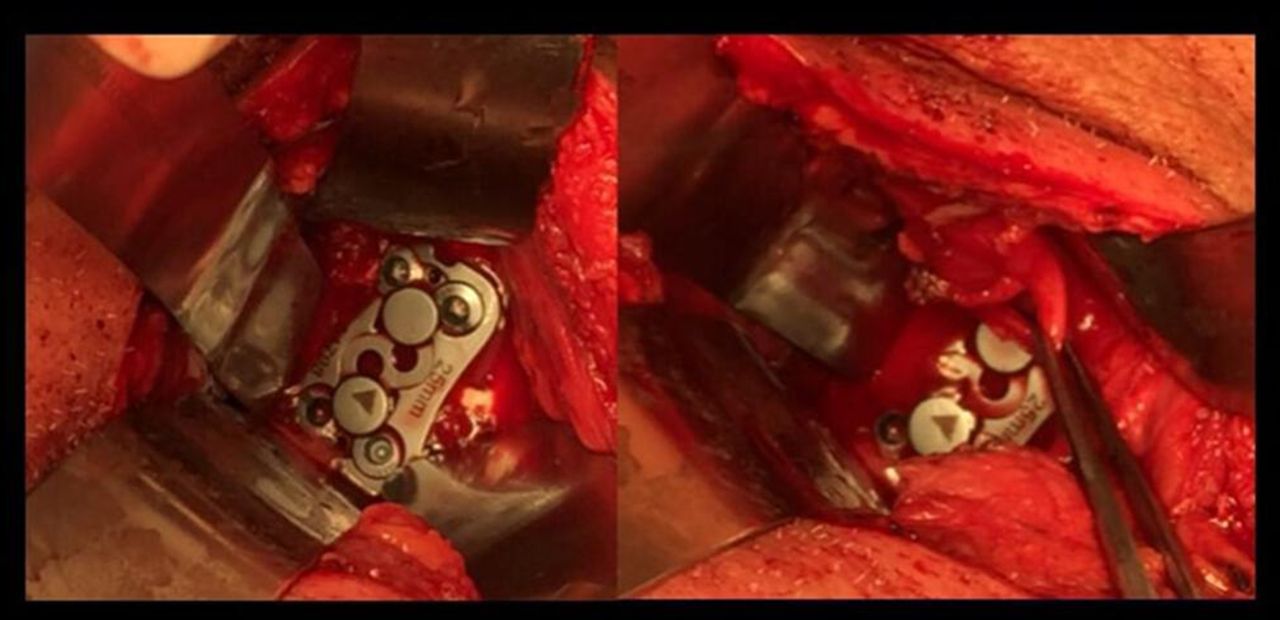
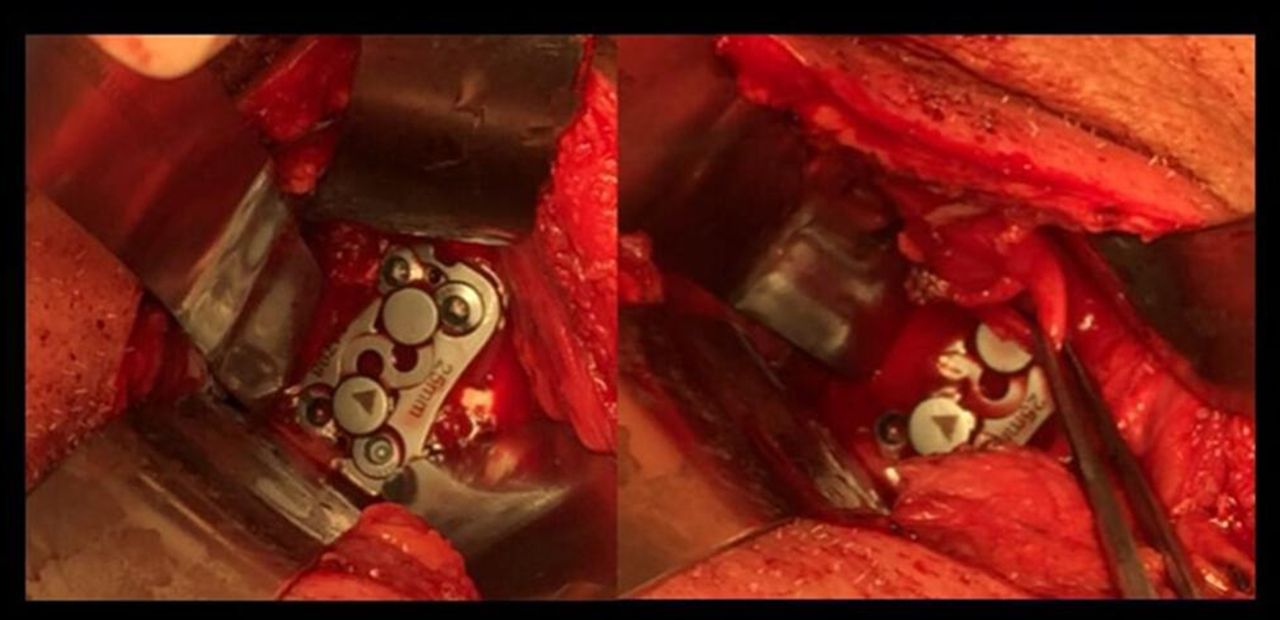
Intraoperative view showing a case of anterior C2-C3 discectomy and interbody fusion. Recurrent laryngeal nerve was identified and preserved (right).
Postoperative standard x-ray images showing a patient with hangman’s fracture who submitted to an anterior approach. The patient had an unsatisfactory large gap on fracture place (left) and who benefited from 360° fusion (right).
Postoperative standard x-ray images showing a patient who benefited from C2-C3 discectomy and interbody fusion and posterior wiring.
Injury classification and management (N = 120).
Evaluation of management performed according to the type of injury.
All the patientes were referred for outpatient follow-up, and we intend to demonstrate posterior long-term follow-up results in a future study.
Discussion
In our series, as in those of the literature, UCS injuries primarily concern a young male population.1,3,14,15 The most frequent trauma mechanisms were motorcycle accident (31.7%) followed by car accident (24.2%). Similar results were found in previous studies, such as the study by Nizare et al 14, which showed a 4 times higher prevalence in men, with traffic accidents being the main cause of UCS injury. According to Wang et al,15 young men were the majority of the sample, but the main mechanism of injury was accidental falls (48.7%).
Endorsing to literature, the majority (85%) of the patients did not present neurologic deficit, and it was demonstrated that there was no significant association of the variables analyzed with the presence of neurological deficit.1,2,8,14–16
C0-C1-C2 dislocations in UCS injuries are rare and fatal. In survivors, despite when neurological deficit is minimal or absent, there is a high instability with risk of sudden severe neurologic impairment.1,6,17,18 Thus, a complete neurological examination and radiological investigation, whenever necessary, are essential in emergencies. In this study, only 2 cases presented atlanto-occipital displacement; both were associated with odontoid fracture and treatment was performed with posterior occipitocervical fusion.
In our department, we use the Anderson and D’Alonzo classification of odontoid fracture. The present study demonstrated that most injuries were at C2 level, with type II odontoid fracture being the most frequent injury (35/120 in our series), especially concerning odontoid (35/42), compatible with what was shown in previous studies, as described by Wang et al15 (C2 with 85.5% of the cases and type II odontoid fracture with 35.3% of the cases), Nizare et al14 (62.8% at level C2 and 40% with odontoid fracture), and Vieweg et al8 (68.6% at level C2 and 44.3% with odontoid fracture). Those lesions are often unstable and need surgical fixation as described in literature. Thus, in our series, among the 42 cases with isolated odontoid fracture, the most frequent approaches were C1-C2 posterior arthrodesis (30 cases) and osteosynthesis of odontoid (14), demonstrating that the higher frequency of type II odontoid fractures leads to a higher rate of surgical than conservative approaches, consistent with data in the literature.5,18–27 Regarding the management, most (64.5%) of the patients were submitted to a surgical procedure. As shown in the results, the type of treatment presented a significant association (P < 0.05) with the level of the lesion, in which most of the injuries in C1 were treated conservatively, and most of the injuries in C2 and C1-C2 had a surgical approach.1,6,17,28,29
Moreover, concerning isolated hangman’s fracture, among 16 cases, 6 were managed conservatively; in 5 cases, C2-C3 anterior arthrodesis was performed; in 3, posterior fusion; and in 2, combined C2-C3 anterior arthrodesis and C1-C3 posterior arthrodesis. Despite the literature reviewed, our data had predominance of the surgical approach for this type of injury, with anterior cervical approach being the most performed.
Conclusion
Traumatic injuries of the UCS predominantly affect young male patients. Traffic accidents were the most frequent causes. The main presentation in the Frankel Scale of admission is grade E, and the neurological deficit is present in a small portion of patients and without statistically significant correlation with the variables studied. The main level affected is C2, and type II odontoid fracture is the most frequent subtype. Moreover, injuries at C1 level are related to conservative treatment, while injuries at the C2 level and the combined C1-C2 level are related to surgical approach with statistical significance. The management of these injuries is mainly performed with surgical treatment, with C1-C2 posterior arthrodesis and anterior odontoid osteosynthesis representing most of the approaches. Differing from the literature, our data had predominance of the surgical approach for hangman’s fracture, with anterior cervical approach being the most performed.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest or financial disclosures with respect to the research, authorship, and/or publication of this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.