


Abstract
Background Due to its ultraminimally invasive nature, endoscopic spinal surgery is an attractive tool in spinal oncologic care. To date, there has been no comprehensive review of this topic. The authors therefore present a thorough search of the medical literature on endoscopic techniques for spinal oncology.
Methods A systematic review using PubMed was conducted using the following keywords: endoscopic spine surgery, spinal oncology, and spinal tumors.
Results Collectively, 19 cases described endoscopic spine surgery for spinal oncologic care. Endoscopic spine surgery has been employed for the care of patients with spinal tumors under the following 4 circumstances: (1) to obtain a reliable tissue diagnosis; (2) to serve as an adjunct during traditional open surgery; (3) to achieve targeted debulking; or (4) to perform definitive resection. These cases employing endoscopic techniques highlight the versatility of this approach and its utility when applied to the right patient and with an experienced surgeon.
Conclusions Our systematic review suggests that, given the right patient and an experienced surgeon, endoscopic spine surgery should be considered in the armamentarium for spinal oncologic care for both staging and definitive resection.
Clinical Relevance This systematic literature review showed that endoscopic techniques have been successfully applied across the spectrum of care in spinal oncology, from diagnosis to definitive treatment.
Introduction
Tumors of the spinal column demand essential consideration within the broader oncologic disease landscape. First, tumors of the spinal column are prevalent among patients with cancer. It is estimated that 60% to 70% of patients with metastatic cancer have a metastatic disease burden to the spinal column.1–4 Second, spinal column tumors can be incredibly debilitating. Roughly 64% of patients with spinal bone metastasis have motor dysfunction, and 90% have back pain.5 Finally, although life expectancy is increasing for patients with tumors of the spinal column, these patients overall tend to have a limited prognosis.1,6 Thus, any surgical solution that can offer practical and clinically efficacious care with a short recovery period would be desirable.
Historically, open surgery for spinal tumors has been limited by the overall frailty of this patient population and the considerable recovery period required following such surgeries. Endoscopic spine surgery can potentially circumvent these challenges due to its ultra–minimally invasive nature that allows for less intensive anesthesia, reduced operative time, minimal tissue and bony disruption, less blood loss, and shorter hospital length of stay and recovery. In this context, endoscopic spine surgery represents a promising tool in spinal oncologic care.7–13 However, despite the promise of endoscopic spine surgery for spinal oncologic care, to our knowledge, there has been no comprehensive review on this topic. Therefore, the present article summarizes and discusses published literature on endoscopic spinal oncologic care. Points of discussion will include indications, outcomes, challenges, and the key elements of a learning curve to be considered when integrating endoscopic protocols into an ongoing oncologic spine care program.
Methods
A PubMed search was conducted in January 2022 for articles published in the English language between 1990 and 2021 using the following keywords: endoscopic spine surgery, percutaneous endoscopic, minimally invasive spine, transforaminal, spinal oncology, and spinal tumors. Articles that did not employ endoscopic techniques were excluded from this literature review. Articles that incorporated endoscopic procedures and presented information in a case-based or case series format were reviewed and included.
Results
The Table summarizes the key findings from this review of the literature. Overall, 242 articles were identified on initial search, and of these, 9 articles fit the inclusion criteria and thus were included in the analysis. Collectively, 19 cases described endoscopic spine surgery for spinal oncologic care. These interventions fell under 1 of 4 categories:
Reports of endoscopic spinal oncology surgery in the literature.
Biopsy (2 cases)
Adjunct during open surgery (9 cases)
Debulking (6 cases)
Definitive resection (2 cases)
Biopsy
Two reports of endoscopic biopsies were found in the literature. The first case was reported in a 35-year-old man who had a periforaminal lumbar mass with a history of stage IV Hodgkin and non-Hodgkin lymphoma.17 He had undergone a computed tomography (CT)-guided needle biopsy, but the results of this biopsy were inconclusive. The authors proceeded at that point with an endoscopic transforaminal approach without complications, and the results were conclusive for non-Hodgkin lymphoma. The second case was a 12-year-old boy who presented with a paravertebral thoracic mass. An endoscopic biopsy completed here without complication revealed a paraganglioma.18
Adjunct During Open Surgery
One case series reported endoscopic spine surgery employed as an adjunct during traditional open surgery.5 It described 9 cases of how endoscopic spine surgery could augment posterolateral thoracic vertebrectomies for metastatic tumors—adding endoscopic steps during the open debulking facilitated enhanced visualization while decreasing manipulation of neural elements. There were shorter operative times and hospital length of stays, less blood loss, and improved outcomes. There were no reported complications in this case series. While limited by being only a single case series, the report does demonstrate the promise of utilizing an endoscopic technique to augment traditional open surgery.
Debulking
A total of 6 cases were found in the literature of endoscopic spine surgery being utilized for debulking metastatic tumors to the spinal column.19–21 All but 1 of these cases occurred in adult patients.19 In the pediatric case, the authors palliatively treated a patient with thoracic radiculopathy due to a recurrent Ewing-like tumor ventral to the midthoracic spinal cord.15 The adult cases also highlighted the utility of the endoscopic approach in alleviating radicular pain due to various metastatic etiologies, including non–small cell lung cancer in the sacrum, prostate cancer in the lumbar spine, hepatocellular carcinoma to the sacrum, and colon cancer to the lumbar spine. There were no complications seen in any cases. See Figures 1–4 regarding some of these cases.
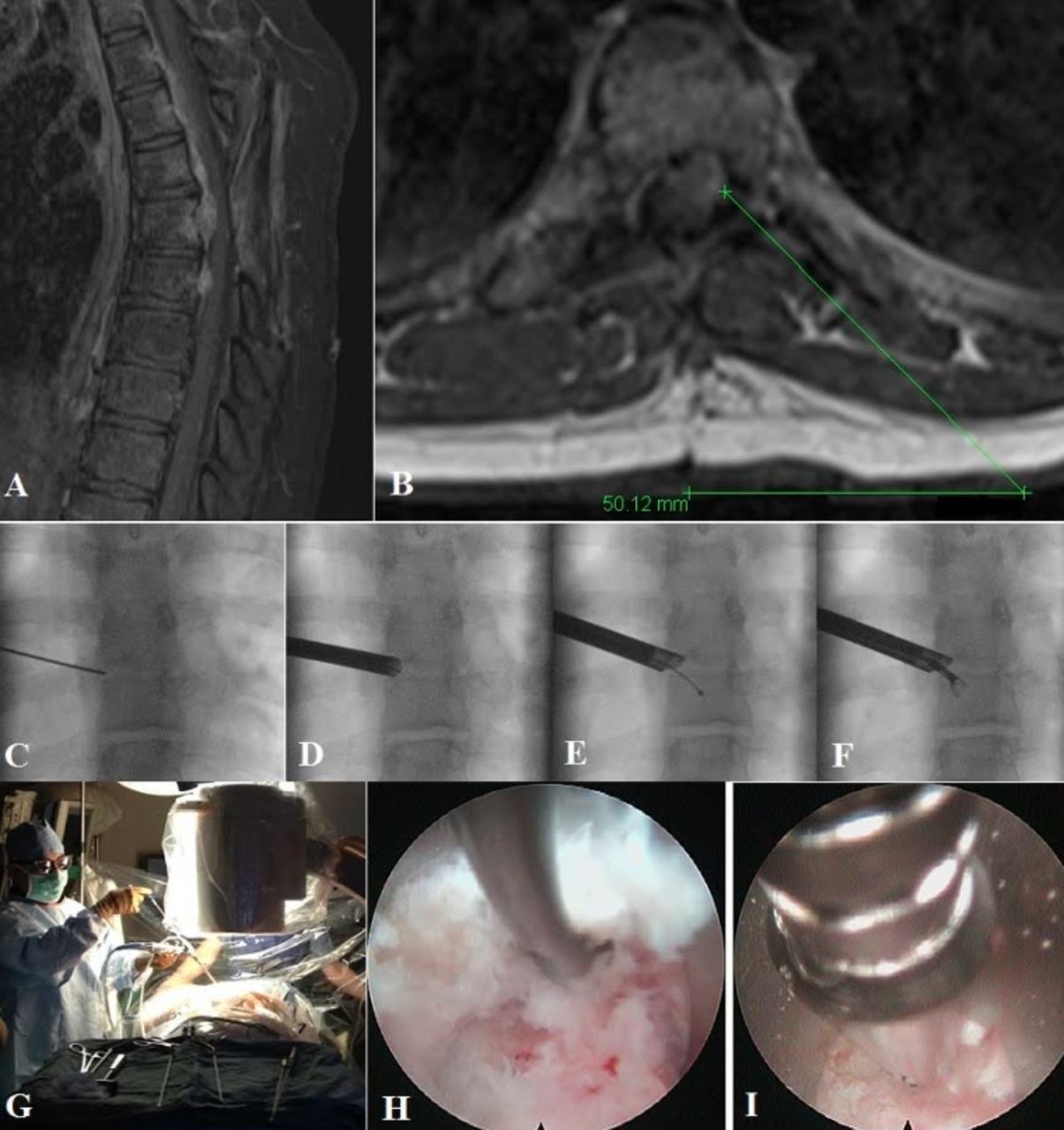
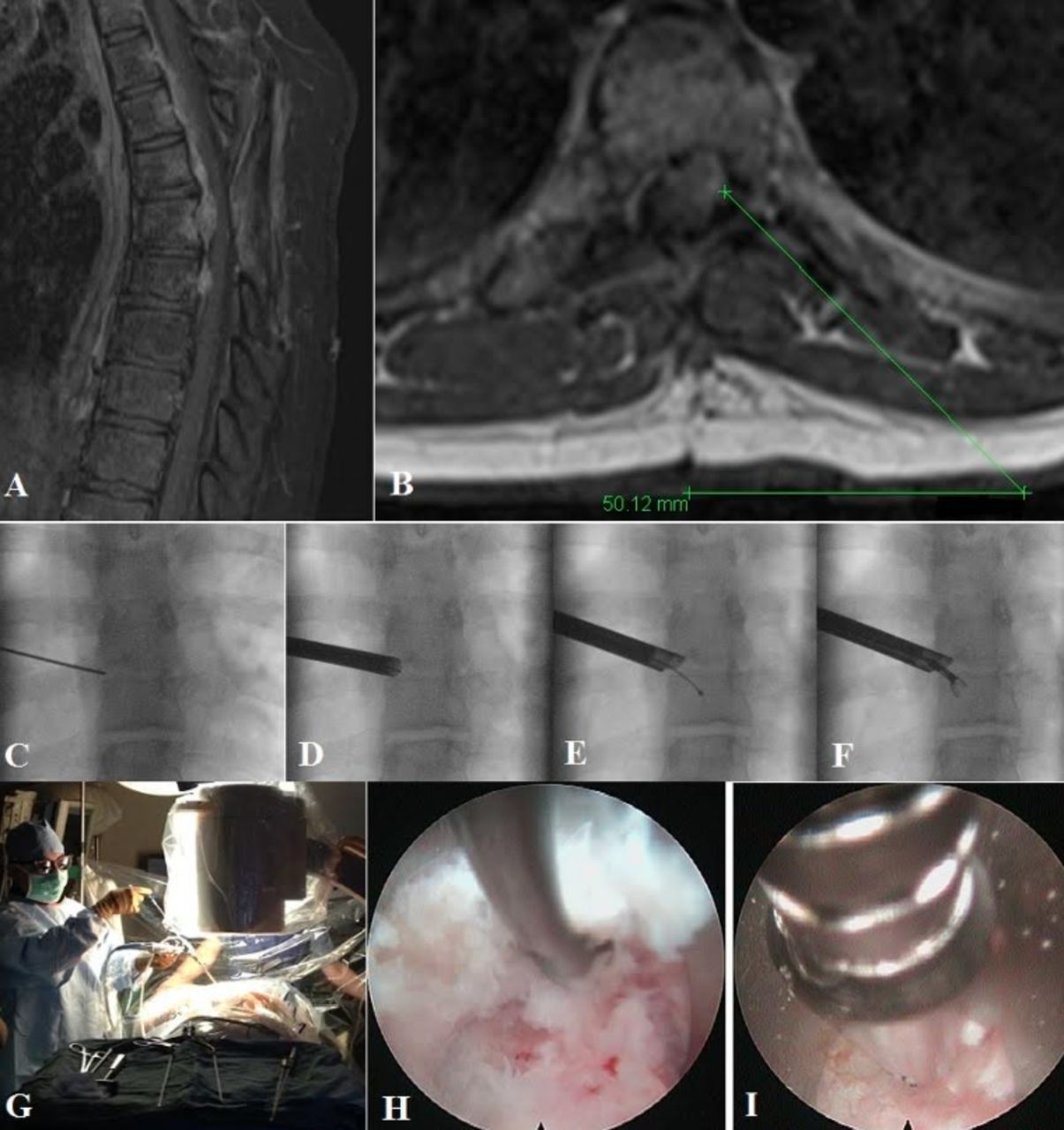
Images from a pediatric case of a ventral epidural thoracic Ewing-like tumor. Panels A and B show sagittal and axial T1 postcontrast magnetic resonance imaging of the thoracic spine with evidence of tumor recurrence in the ventral epidural region. Panels C to F show intraoperative fluoroscopic images. Panel G is an image from the operating room setup. Panels H and I are intraoperative images of the tumor debulking. Source: Figure reprinted with permission from Telfeian AE, Choi DB, Aghion DM. Transforaminal endoscopic surgery under local analgesia for ventral epidural thoracic spinal tumor: case report. Clin Neurol Neurosurg. 2015;134:1–3. doi:10.1016/j.clineuro.2015.03.022.

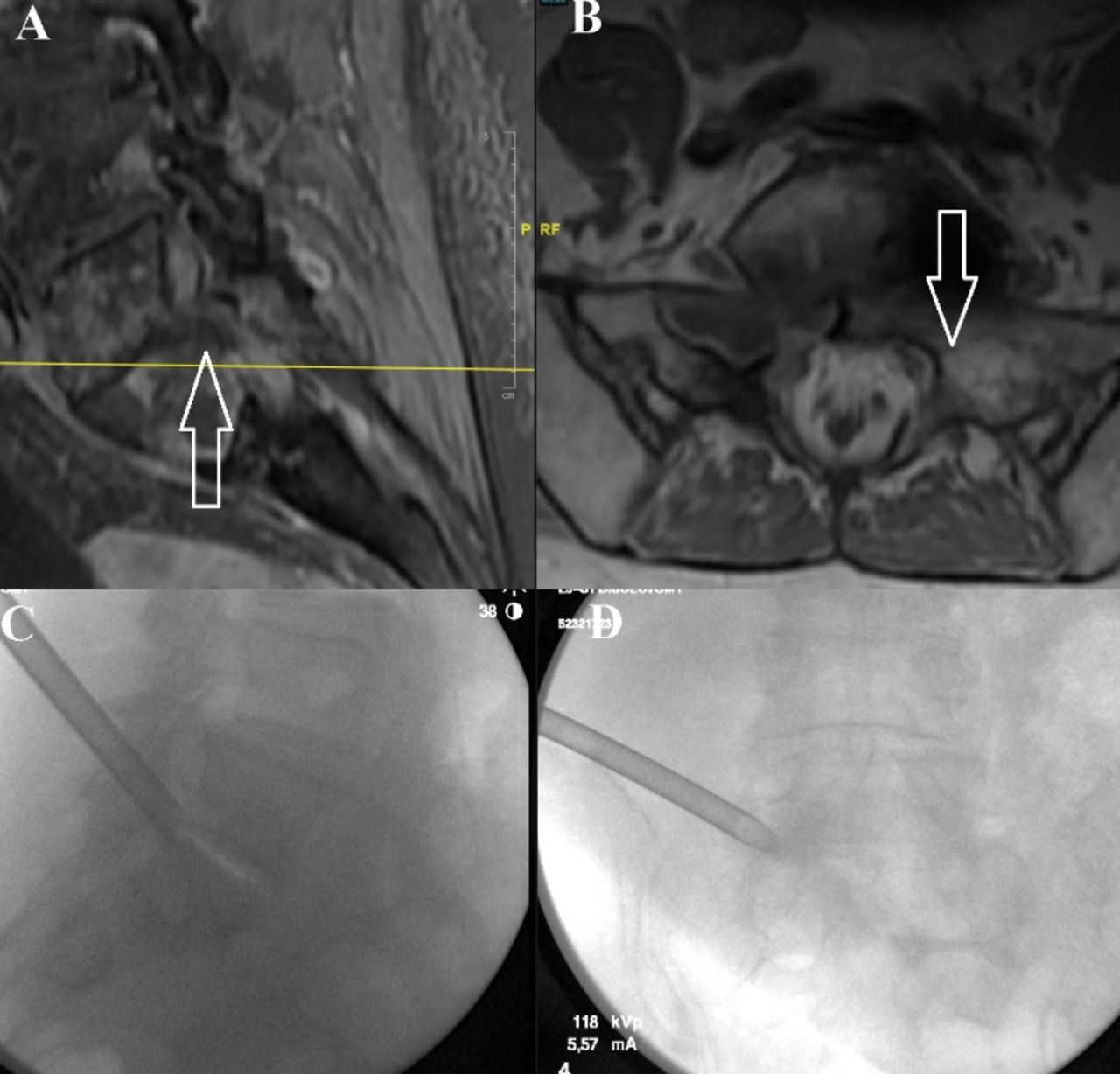
Images from the case of a 75-year-old patient with metastatic nonsmall cell lung cancer. Panels A and B show a magnetic resonance imaging demonstrating a metastatic focus at the left L5-S1 foramen compressing the exiting left L5 nerve. Panels C and D show intraoperative fluoroscopic imaging localizing this region. Source: Figure reprinted with permission fromTelfeian AE, Oyelese A, Fridley J, Doberstein C, Gokaslan ZL. Endoscopic surgical treatment for symptomatic spinal metastases in long-term cancer survivors. J Spine Surg. 2020;6(2):372-382. doi:10.21037/jss.2019.10.14.
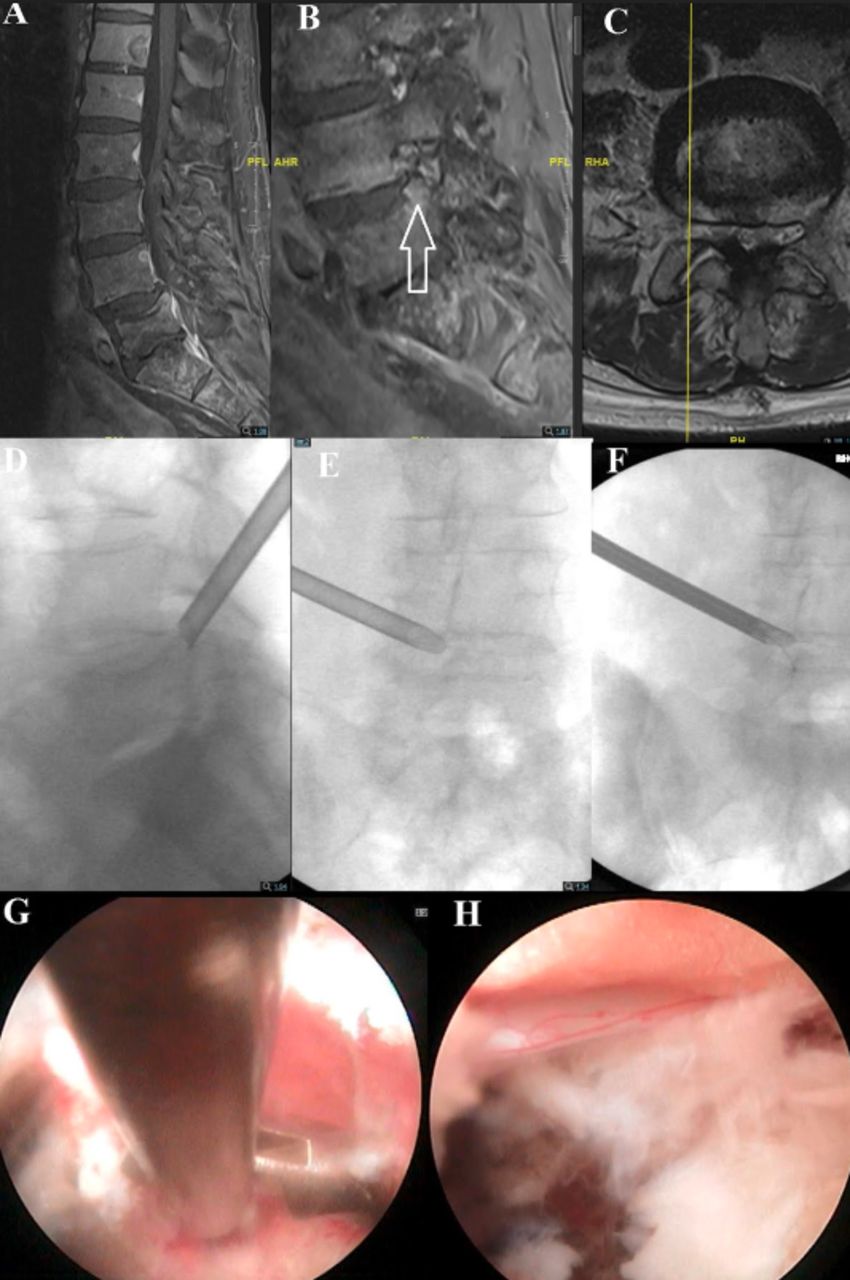
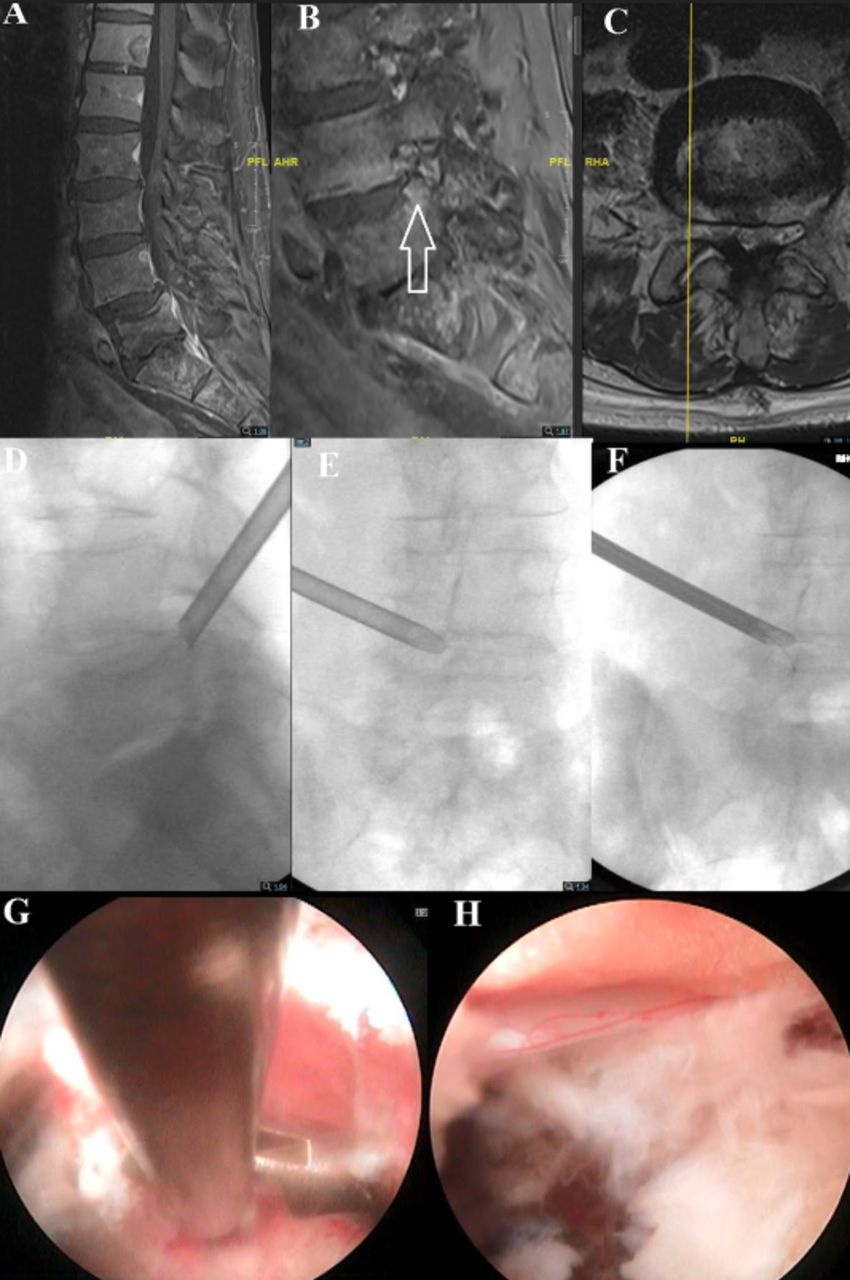
Images from the case of a 76-year-old patient with metastatic prostate cancer status after radiation. Panels A to C demonstrate a magnetic resonance imaging showing a fracture fragment from the L5 superior endplate compressing the traversing L5 nerve root. Panels D to F show intraoperative fluoroscopic localization, and panel G shows intraoperative tumor debulking. Panel H demonstrates the decompressed traversing L5 nerve root. Source: Figure reprinted with permission from Telfeian AE, Oyelese A, Fridley J, Doberstein C, Gokaslan ZL. Endoscopic surgical treatment for symptomatic spinal metastases in long-term cancer survivors. J Spine Surg. 2020;6(2):372-382. doi:10.21037/jss.2019.10.14.
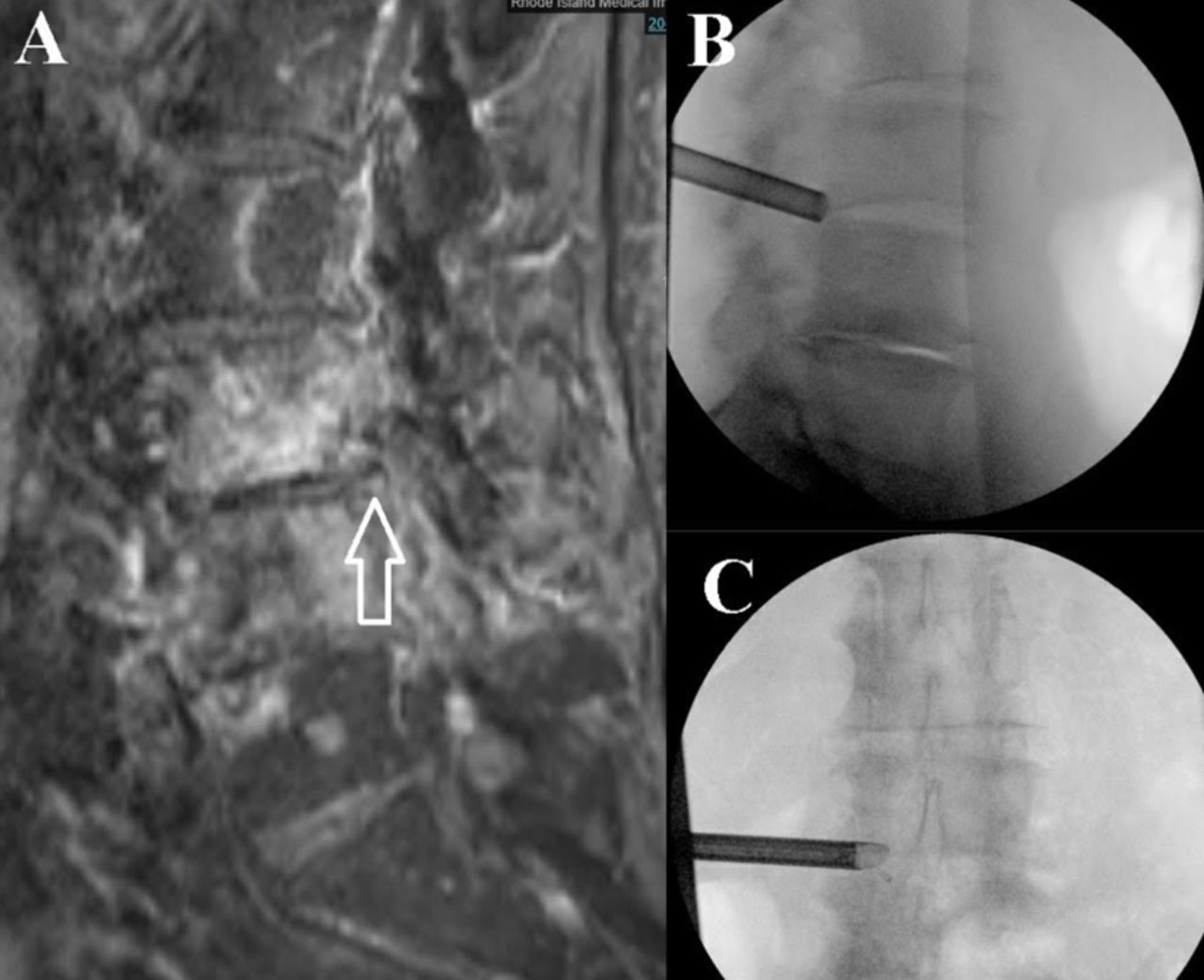
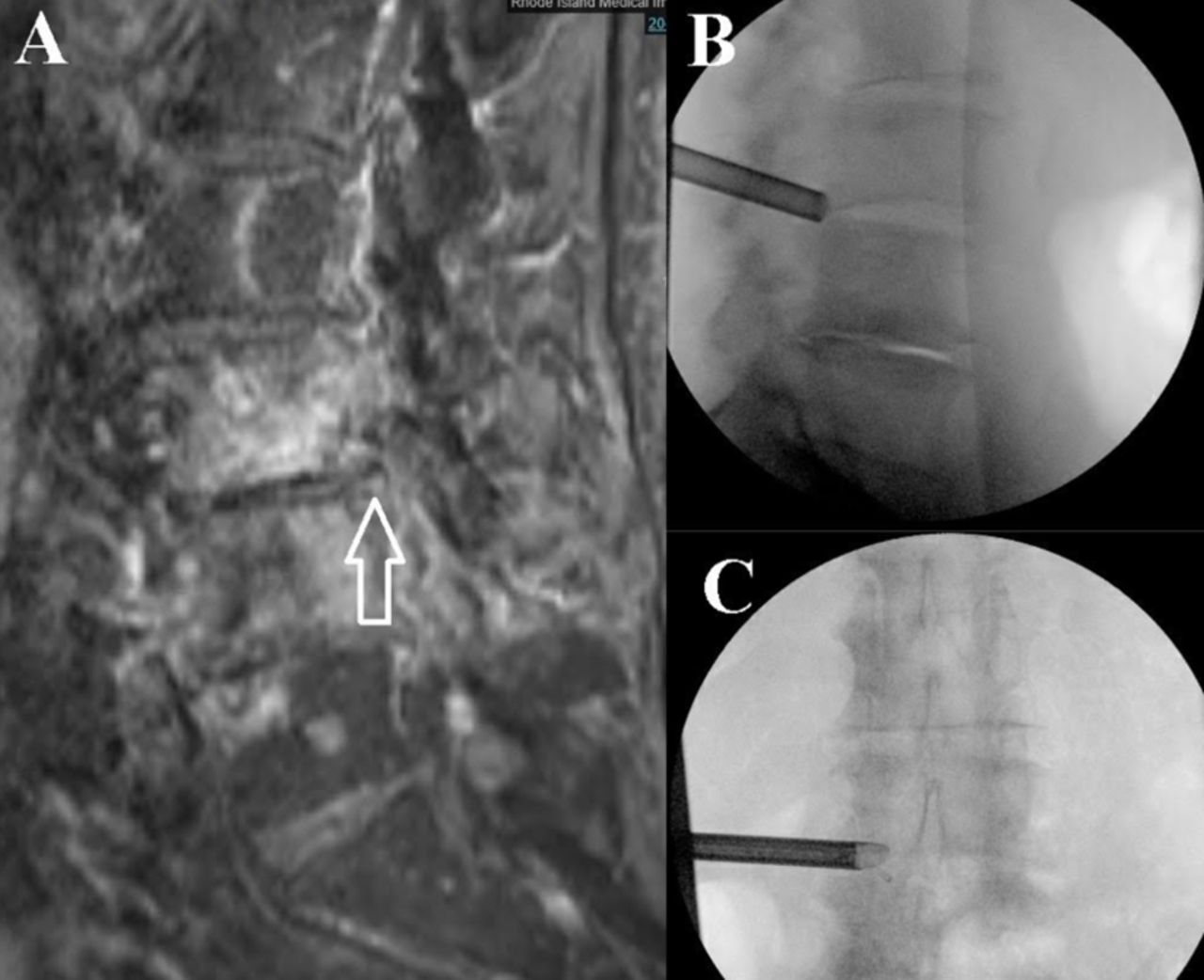
Images from the case of an 86-year-old patient with metastatic prostate cancer. Panel A shows severe left L3-L4 stenosis on magnetic resonance imaging (site marked with arrow), and panels B and C demonstrate intraoperative fluoroscopy localizing to the correct level prior to debulking. Source: Figure reprinted with permission from Telfeian AE, Oyelese A, Fridley J, Doberstein C, Gokaslan ZL. Endoscopic surgical treatment for symptomatic spinal metastases in long-term cancer survivors. J Spine Surg. 2020;6(2):372-382. doi:10.21037/jss.2019.10.14.
Definitive Resection
Two cases in the literature demonstrated complete resection of a spinal tumor via an endoscopic approach. One case was of a 67-year-old man who presented with a meningioma at the level of L1.22 Under general anesthesia, the tumor was resected via an endoscopic approach. The surgeons were able to achieve a gross total resection without complication. Another case was a 45-year-old woman with a lumbar osteoblastoma presenting with lumbar radiculopathy (the lesion was centered on the L5 superior articulating process).23 The surgeons were able to achieve a gross total resection with an endoscopic approach. At 6-month follow-up, the patient was no longer in any pain, and a magnetic resonance imaging showed no evidence of residual disease.
Discussion
The literature review shows that endoscopic techniques have been applied across the spectrum of care in spinal oncology, from diagnosis to definitive treatment. The cases demonstrate the versatility of this approach and its utility when applied to the right patient and with an experienced surgeon. Furthermore, there were no reported complications in the literature. The following areas relevant to establishing and mastering the learning curve of an endoscopic spinal oncology protocol are worthy of discussion.
Endoscopic biopsies can be very reliable forms of tissue sampling. Endoscopic biopsies can be performed under direct visualization, and significant tissue samples can be obtained. Although the 2 reported cases of endoscopic biopsies differ in terms of 1 case being pediatric and 1 adult, they share common lessons. The adult case highlights the limitations of CT-guided needle biopsies, which, owing to the small sample size inherent to biopsies with this approach, can often be nondiagnostic. Additionally, the pediatric case highlights how an endoscopic procedure can facilitate reduced radiation exposure compared with a CT-guided approach. Both cases demonstrate how the endoscopic approach minimizes tissue and bony disruption compared with more invasive techniques while still preserving the ability to maintain patient safety, such as performing hemostasis under direct visualization. Finally, patients can be discharged from the hospital quickly because of the short recovery period required after an endoscopic biopsy. Because the large tissue samples obtained from this technique facilitate more accurate diagnoses, definitive treatment can start sooner.
Despite having incredibly varied pathologies, the debulking cases collectively share some key insights. Endoscopic spine surgery can be used successfully to treat radicular pain due to metastatic tumors by alleviating the mass effect from these tumors compressing nerve roots exiting the spinal column. This can be achieved in an ambulatory surgical setting. Blood loss is minimal in these surgeries due to minimal tissue and bony disruption, ability to perform hemostasis under direct visualization, and short operative times. The minimally invasive nature of these surgeries can facilitate faster adjuvant treatment (ie, chemoradiotherapy), and the relatively quick recovery time permits patients to return more quickly to an improved quality of life.
Complete resection of spinal column tumors can be very destabilizing and necessitate fusion. However, the definitive resection cases demonstrate that in 2 inherently less stable regions of the spinal column—the thoracolumbar junction and at the L5 superior articulating process—a gross total resection without the need for instrumented fusion was possible. The cases demonstrate the feasibility of endoscopic gross complete resection of select spinal tumors with all of the benefits inherent to this ultraminimally invasive approach.
Highly experienced spine surgeons performed these advanced endoscopic cases. As impressive as the results of these published cases are that it is essential to consider challenges to endoscopic spine surgery when applied during spinal oncologic care. It has been well acknowledged that the learning curve is one of the primary barriers to the broader adoption of endoscopic spine surgery.22,24 The problem is compounded by the relative rarity of spinal oncologic cases compared with degenerative ones and the presumed lack of familiarity with these techniques by surgeons and physicians on multidisciplinary tumor boards. Patient selection is paramount with this approach, since achieving the surgical aims may require spinal column destabilization requiring fixation. Some hypervascular tumors may present a high bleeding risk, which might need to be addressed via preoperative embolization or more invasive techniques. Additional published cases, including unsuccessful ones or ones with complications, would help better define the indications and limitations for the endoscopy in an oncologic spine care program.
Conclusion
The 19 cases presented here showcase the feasibility of applying endoscopic techniques to spinal oncologic care, from biopsy to complete resection. To perform a biopsy, an endoscopic approach can obtain a large sample to yield a reliable tissue-based diagnosis. As an adjunct to traditional open surgery, endoscopic techniques may facilitate enhanced visualization for the surgeon. Endoscopic procedures can effectively debulk tumors and relieve radicular pain as a method of alleviating mass oncologic effects on the spinal neural elements. Finally, as a means to perform complete resection, endoscopic techniques may avoid the need to perform an instrumented fusion. The learning curve is one of the primary barriers to broader adoption. However, the success of the cases presented in this review calls for continued efforts to adopt endoscopic techniques in spinal oncologic care.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval Institutional review board authorization was not necessary for the present article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.