


Abstract
Background Different strategies exist for reduction of the cervical spine. Placement of C1 lateral mass screws is a powerful technique but may be impossible in a degenerative or revision setting. We report the open, posterior-only, and instrumented reduction of a fixed C1–2 subluxation using occipital and C2/C3 fixation. The patient had rheumatoid arthritis and had undergone previous surgery of the cervical spine.
Methods We performed a retrospective chart review and focused appraisal of the literature.
Results Satisfactory reduction was achieved with this infrequently reported technique.
Conclusions/Level of Evidence Spine surgeons may consider the described procedure a viable treatment alternative in problematic subluxations of the cervical spine. Level V.
Instrumented reduction has been used to treat lumbar spondylolisthesis,1–3 thoracic fracture-dislocations,4, 5 cervicothoracic deformity,6 and most recently, craniocervical and atlantoaxial subluxation.7–10
Craniocervical subluxation and atlantoaxial subluxation produce a variety of deformities, for example, cranial settling, basilar invagination, and cervical stenosis. Different instrumented reduction techniques may be particularly suited for each. In cases of cervical stenosis and instability, placement of C1 lateral mass screws is a powerful alternative to the traditional use of wiring and transarticular screw fixation.9 C1 lateral mass screws may be difficult to place, however, in a revision or degenerative setting.
As an alternative to the placement of C1 lateral mass screws, we describe occipital plating and fixation of C2 to affect atlantoaxial reduction and correction of cervical stenosis/instability.
Case report
The subject of this case report provided written informed consent for print and electronic publication of this report. The use of bone morphogenetic protein in this case was off-label.
History
A 34-year-old woman with rheumatoid arthritis presented to our clinic 6 months after undergoing a C1–2 fusion. This procedure had been designed to correct subluxation at the atlantoaxial articulation and was accomplished with iliac crest autograft and cables. The patient had been diagnosed with rheumatoid arthritis at age 20 years, was unable to tolerate Enbrel (Entanercept; Pfizer, New York, New York), and took prednisone only. She had recently been placed in halo fixation to prevent paresthesias with neck range of motion (L'hermitte phenomenon).
Examination
The patient's pin sites were clear, and an examination of her cranial nerves yielded benign findings. Additional examination of the extremities showed her to be neurologically intact and normoreflexic. The patient was noted to have a boutonnière deformity of her left ring finger and a swan-neck deformity of her left middle finger. A cervical computed tomography scan obtained at the time of presentation to our clinic is shown in Fig. 1. The space available for the spinal cord at C1–2 was 6 mm. Revision decompression and fusion of the cervical spine were recommended.
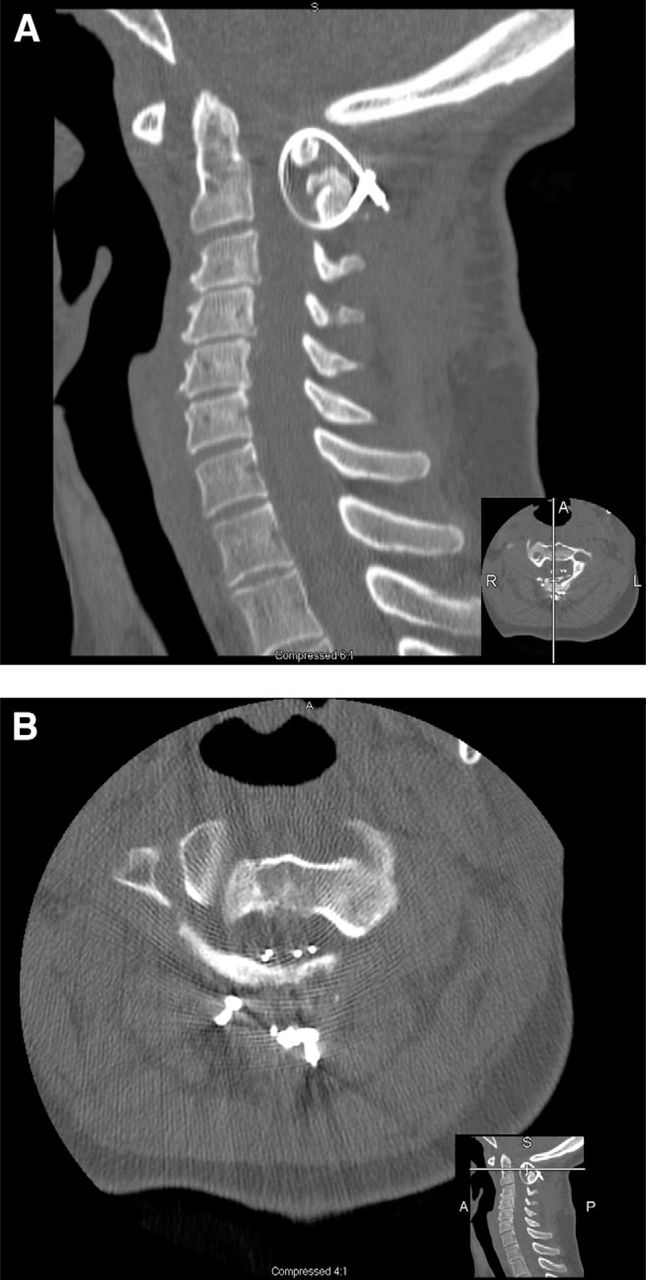
Sagittal (A) and axial (B) computed tomography images of cervical spine obtained at time of presentation to clinic.
Operation
Intravenous antibiotics were administered, fiberoptic intubation was performed with succinylcholine, and both somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) were obtained in the supine position. The halo was removed, and the patient was positioned prone with her head attached to a Jackson frame via a Mayfield clamp. Prone SSEPs and MEPs were stable. Attempted closed reduction of the C1–2 subluxation was unsuccessful (Fig. 2).

Fluoroscopic intraoperative image showing failed closed reduction.
The patient's neck was then prepared and draped, and a midline subperiosteal approach was performed with sharp dissection and bipolar electrocautery to avoid monopolar contact with the C1–2 cables. With the cervical spine exposed from the occiput to C3, laminectomy of C1 and C2 was achieved with a high-speed bur. The laminae and cables were removed en bloc, and no cerebral spinal leak occurred.
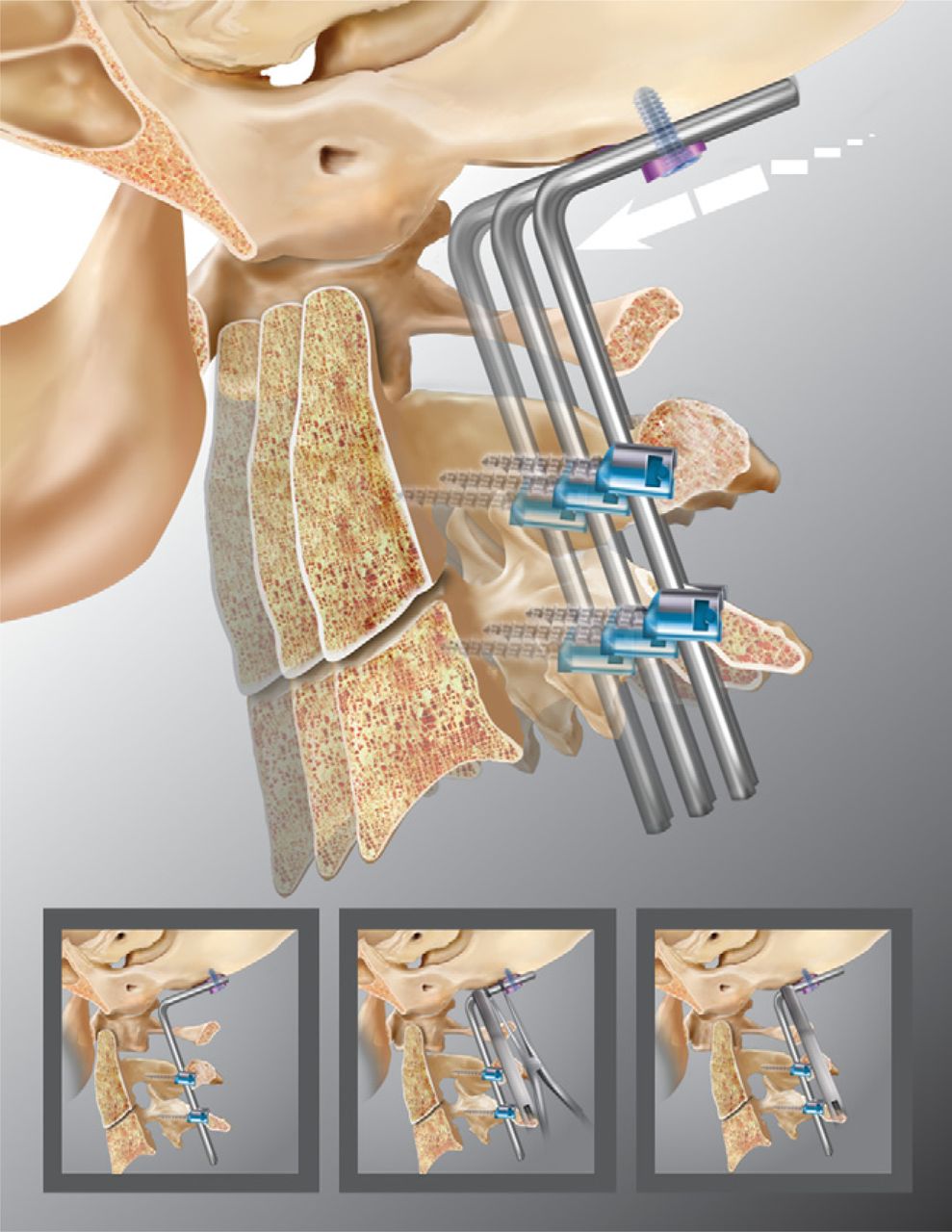
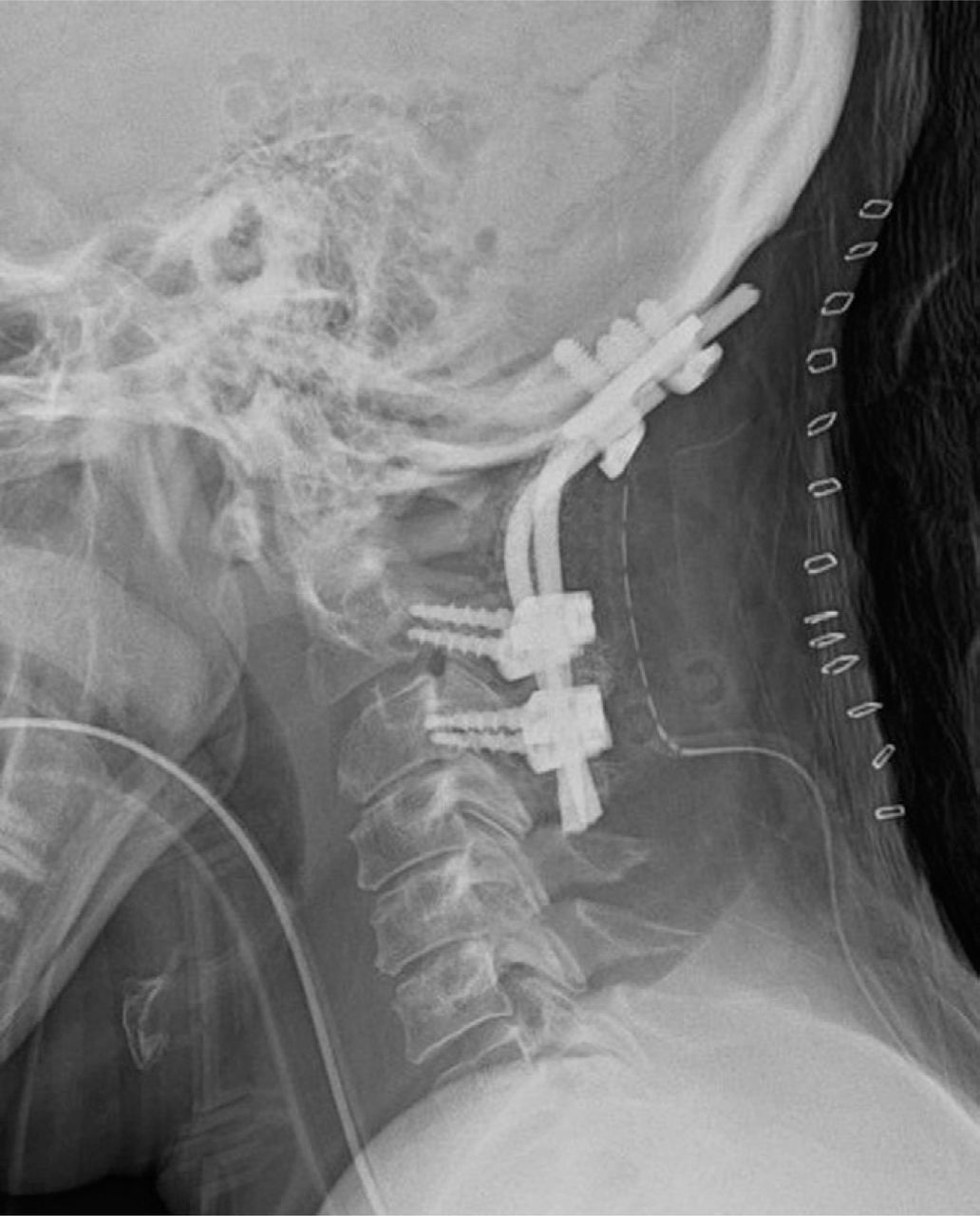
Bone graft from the patient's prior procedure was fused to the undersurface of C1 and obscured the C1 lateral mass. Scarring made exposure of this area additionally difficult. As such, the decision was made to perform an occipitalcervical fusion. A midline occipital plate, C2 pars screws, and C3 lateral mass screws were placed. Reduction was performed as follows: A rod was contoured to connect the occipital plate and distal fixation. The cervical screws were locked, and the end caps in the occipital plate were left loose. A rod holder was placed adjacent to the occipital plate (Fig. 3). Distraction between the rod holder and the occipital plate was used to translate C2 anteriorly, effecting the reduction. The end caps on the occipital plate were then locked. Bone graft derived from the laminectomy and fusion mass was placed. Ceramic and a small strip of bone morphogenetic protein was used to completely fill the gap between the occiput and the cervical spine. The soft tissues were then closed in layers, a cervical collar was placed, and the patient was taken to the recovery room. SSEPs and MEPs were noted to be stable throughout the procedure. An immediate postoperative X-ray showed satisfactory reduction (Fig. 4).
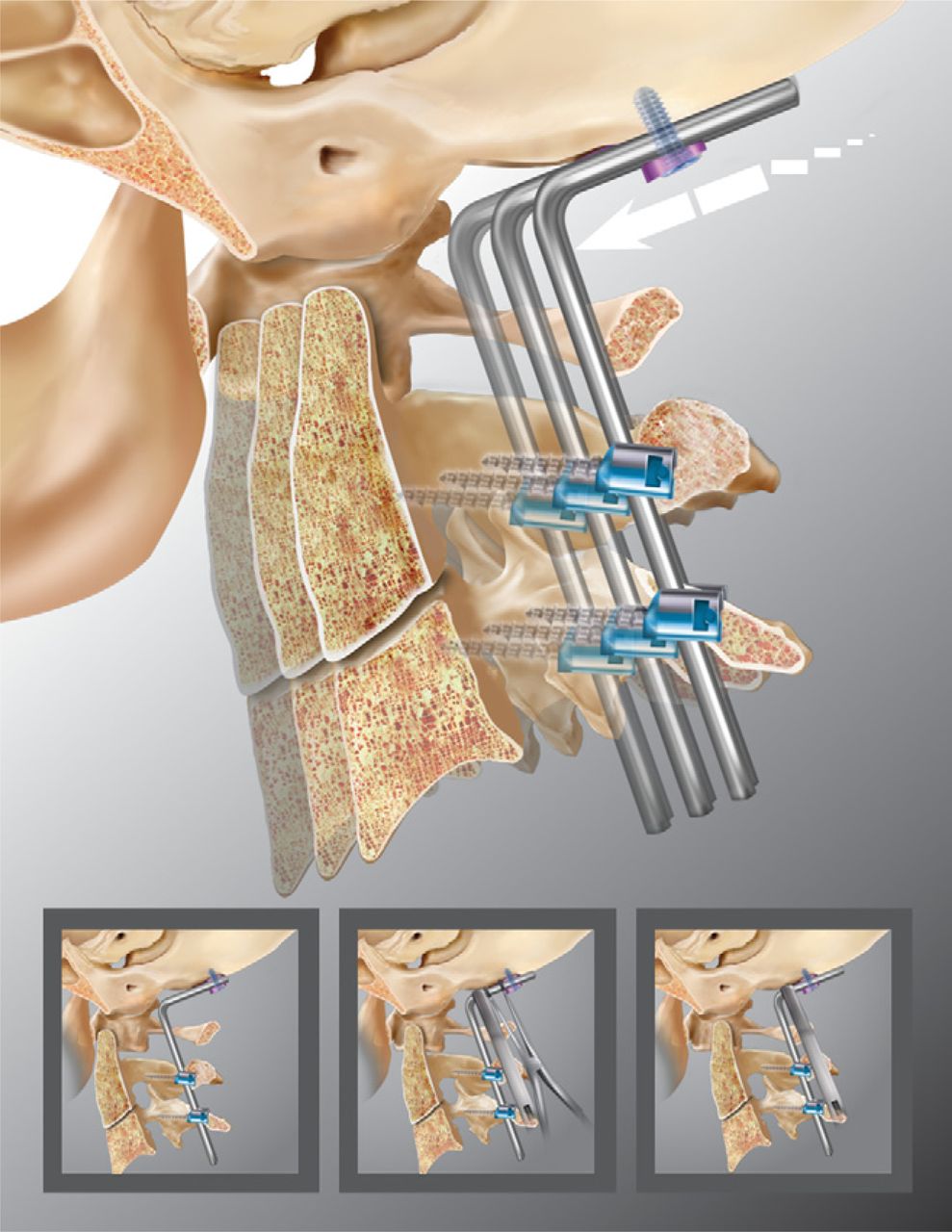
Instrumented reduction of atlantoaxial articulation using occipital plate.
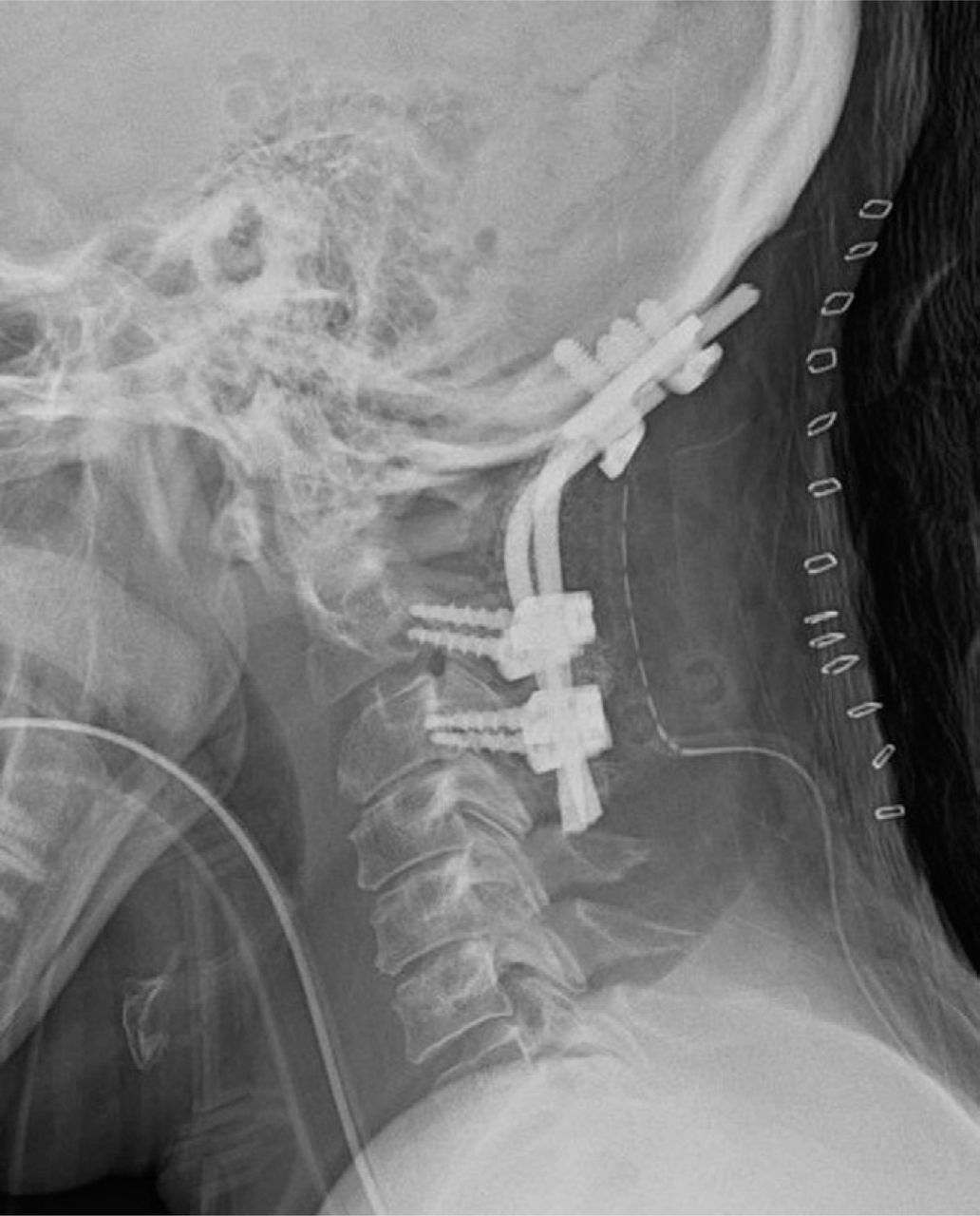
Immediate postoperative X-ray shows satisfactory reduction.
Postoperative course
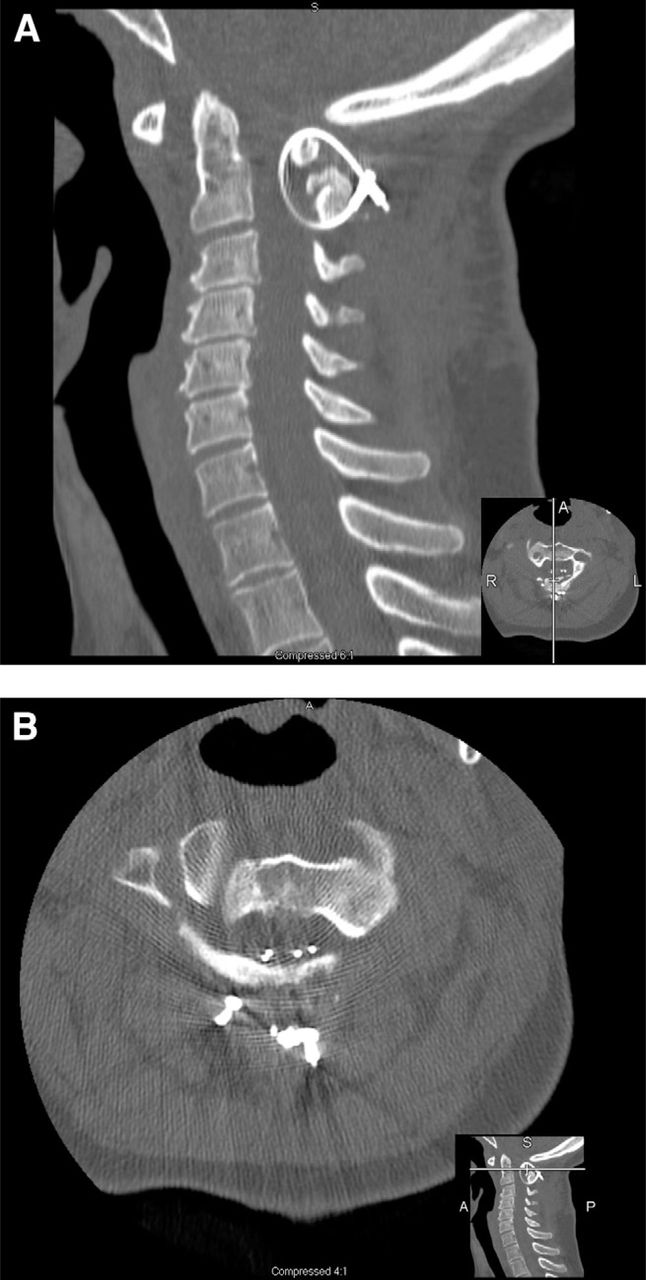
A postoperative computed tomography scan showed satisfactory decompression and reduction (Fig. 5).

Postoperative axial computed tomography image showing maintenance of reduction.
The patient's recovery was unremarkable, and she was discharged home on postoperative day 4. In the early postoperative period, a right iliac vein deep venous thrombosis developed where a femoral line had been placed. (The patient's halo had made preoperative placement of an internal jugular or subclavian line impractical.) Nine months of warfarin therapy was begun with an international normalized ratio goal of 2.5 to 3. X-rays taken 3 months after surgery showed maintenance of the patient's cervical reduction.
Discussion
As in the reported case, inflammatory arthritis may both produce cervical instability and present obstacles to its resolution. The incidence of C1–2 instability in patients with rheumatoid arthritis, in particular, is 20% to 80%.11–13 Of note, lower extremity joint arthroplasty may mark an important opportunity for prophylaxis or intervention. Fifty percent of rheumatoid arthritis patients undergoing joint replacement surgery will have some form of cervical instability. Of these patients, 8% will show cervical subluxation requiring surgical treatment.14
Inflammatory or otherwise, craniocervical and atlantoaxial subluxation may produce cranial settling, basilar invagination, cervical stenosis, or a combination of each. Anterior resection of the odontoid with posterior fixation may beused in these scenarios, especially in cases of irreducible deformity.8 This strategy necessitates anterior dissection, however, and does not facilitate reduction. Accordingly, and corresponding to the diversity of subluxation-associated deformity, a variety of posteriorly based reduction techniques have been described. Goel and Laheri7 have treated cranial settling associated with C1–2 instability by release of the C1–2 joints and atlantoaxial or occipito-atlantoaxial instrumentation with plates and screws. Several authors have described treatment of basilar invagination due to atlantoaxial instability with posterior instrumented reduction using an occipital plate.8, 10 Other instrumented reduction techniques rely on C1 lateral mass screws.9 The reported technique draws on aspects of these modern procedures7, 8, 10 and may be used to treat cervical stenosis/instability, especially in cases in which placement of a C1 lateral mass screw is impossible (Fig. 6).

Example of lateral mass erosion preventing access to C1 lateral mass.
- © 2013 ISASS - International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.