


Abstract
Background To evaluate the clinical and radiological outcomes of a novel full endoscopic procedure performed via an interlaminar approach to decompress entrapped nerve roots in patients with lumbar spondylolysis.
Methods Patients who underwent interlaminar percutaneous endoscopic pars decompression were included in this retrospective cohort study. Patients with back pain and dynamic lumbar instability were excluded from the study. Clinical parameters related to outcomes, including the Oswestry Disability Index (ODI) and visual analog scale (VAS) for leg pain, were assessed before and after surgery. The radiological outcomes, vertebral slippage percentage, and motion radiographs were evaluated preoperatively and postoperatively.
Results Of the 11 patients included in the study, 5 had spondylolysis alone, 1 of whom had spondylolysis at L3-L4 and L4-L5, and 4 of whom had it at L5-S1; and 6 patients had spondylolysis in combination with spondylolisthesis, of whom 4 had involvement at L5-S1, 1 had involvement at L4-L5, and 1 had involvement at L3-L4. At a mean follow-up period of 22.64 months, 63.3% of patients achieved more than 50% improvement in ODI score and 90.91% of patients achieved more than 50% improvement in VAS score. Spondylolysis with vertebral slippage had inferior ODI improvement outcomes as compared with spondylolysis alone, but the VAS was not significantly different. No significant difference was observed on the slippage percentage observed between the pre- and postoperative periods. However, 1 patient experienced vertebral slippage after surgery, but fusion surgery was not required.
Conclusions Interlaminar percutaneous endoscopic pars decompression is a safe and successful treatment for patients with stable lumbar spondylolysis and nerve root compression. Even in situations in which vertebral slippage occurs, spinal fusion may not be the best option for all patients with lumbar spondylolysis.
Clinical Relevance The interlaminar percutaneous endoscopic pars decompression is a safe and successful procedure for treatment of patients with stable lumbar spondylolysis and nerve root compression.
Level of Evidence 4.
- spondylolysis
- nerve root compression
- interlaminar percutaneous endoscopic uniportal pars decompression
Introduction
Spondylolysis is an anatomical deficiency of the vertebral arch or a fracture of the pars interarticularis. In the Caucasian community, spondylolysis is estimated to affect 3% to 6% of the population.1–3 Most spondylolytic abnormalities (85%–95%) occur at L5, with L4 being the second most afflicted level (5%‒15%), while more proximal lumbar levels are impacted considerably less frequently.1–3
Spondylolysis is not present at birth but usually manifests at a young age.4 In a prospective study of 500 first graders, Fredrickson et al discovered a prevalence of 4.4% by the age of 6 years, rising to 6% by the time the individuals reached adulthood.2 Spondylolysis appears to be more common in the young athletic population than in the overall population.3,5,6 Beutler et al followed up on the initial spondylolysis participants reported by Fredrickson et al over a 45-year period and discovered that the sole predictive factor for the development of vertebral slippage (spondylolisthesis) was unilateral or bilateral spondylolysis.7 After the age of 20 years, spondylolisthesis advancement is considerably less common than its progression throughout infancy and adolescence.8–10
The majority of spondylolysis cases are asymptomatic.11 However, spondylolysis with spondylolisthesis can be associated with radiculopathy or low back pain. The most relevant pathoanatomy of radiculopathy in spondylolysis is the hook-like remnant of the proximal deficient lamina of the spondylolytic lesion.12 Even though conservative treatment can help reduce pain, many patients suffer from persistent back pain or leg pain, which may require surgery. Fusion surgery must be considered in patients presenting with back pain or dynamic instability. Conversely, it is debatable whether decompression alone should be performed in patients with spondylolysis who have only radicular symptoms.
Traditional open surgical procedures that involve decompression in isolation can cause issues with the posterior supporting structures, thereby destabilizing the affected levels and increasing vertebral slippage.13 Therefore, spinal fusion is required to stabilize the involved vertebral levels, and this has become an extremely popular surgical procedure. However, fusion surgery is associated with side effects that cause a higher morbidity rate, including loss of motion segment, adjacent disc degeneration, hardware problems, and pseudarthrosis.14–16 Some cases of spondylolysis that present with only spinal nerve root compression and no back pain or spinal instability may be better suited to decompression alone rather than a combination with fusion. For this reason, minimally invasive surgery may play a significant role in preserving the posterior supporting spinal components after decompression to avoid increasing postoperative instability.17 Moreover, there is currently significant evidence to support the use of full endoscopic surgery as an alternative intervention for spinal operations.18 The endoscopic spinal surgery procedure requires a minimal incision and causes substantially less damage to the soft tissue, and provides protection of the facet joints and posterior ligaments, which may help to maintain stability of the vertebral segment as compared with conventional open surgery. Consequently, we considered that full endoscopic pars decompression would be sufficient to treat such patients if the major symptom was leg pain from nerve root compression.
The goal of this study was thus to identify the clinical outcomes of full endoscopic pars decompression in patients with spondylolysis who presented with radiculopathy.
Methods
Patients and Assessments
As part of this retrospective cohort study, 11 patients underwent full endoscopic pars decompression for lumbar spondylolysis between January 2014 and December 2020. Spondylolysis was diagnosed based on medical history, physical examination, and radiographic assessment, including computed tomography (CT) and magnetic resonance imaging (MRI). A dynamic lumbar radiography was used to examine the stability of the spine. The surgical indications for our technique were radiculopathy from nerve root compression by pars defect lesion, which was confirmed by MRI and CT ing, and all patients were required to confirm that conservative treatment had failed for at least 3 months. Patients who had experienced back discomfort or demonstrated dynamic instability (>4-mm motion on flexion/extension radiographs) were excluded from the study. Before surgery, all patients were informed of the risk of complications after surgery such as infection, nerve root injury, and postoperative further vertebral slippage. Informed consent to use medical record information was collected from all participants prior to study initiation, and the study was approved by the institutional review board of the authors’ institution.
A single surgeon (P.S.) performed interlaminar percutaneous endoscopic uniportal pars decompression at L3-L4, L4-L5, or L5-S1 in 11 patients at the Paolo Phaholyothin Hospital. Endoscopic operations were studied retrospectively for patient demographics, surgical data, and follow-up duration. Patient radiographs and MRIs were analyzed, and spondylolisthesis grade was determined using Meyerding’s classification.19 Any vertebral slippage percentage (% slippage) was measured preoperatively and postoperatively. Following lateral radiography, the % slippage was determined by dividing the anteroposterior displacement of L5 (L4) over S1 (L5) by the anteroposterior diameter of L5 (L4).
Oswestry Disability Index (ODI) scores20 were used to evaluate impairment, and the visual analog scale (VAS) score for leg pain (full score = 10) was used to measure neurological leg pain outcomes. ODI scores span 0 to 100, with 100 representing the greatest impairment. These clinical outcome indicators were assessed twice: once before surgery and again thereafter. The VAS and ODI score recovery rates were then calculated using an improvement rate of VAS = 100 (preoperative VAS − postoperative VAS)/preoperative VAS and an improvement rate of ODI = 100 (preoperative ODI − postoperative ODI)/preoperative ODI.21
Surgical Technique
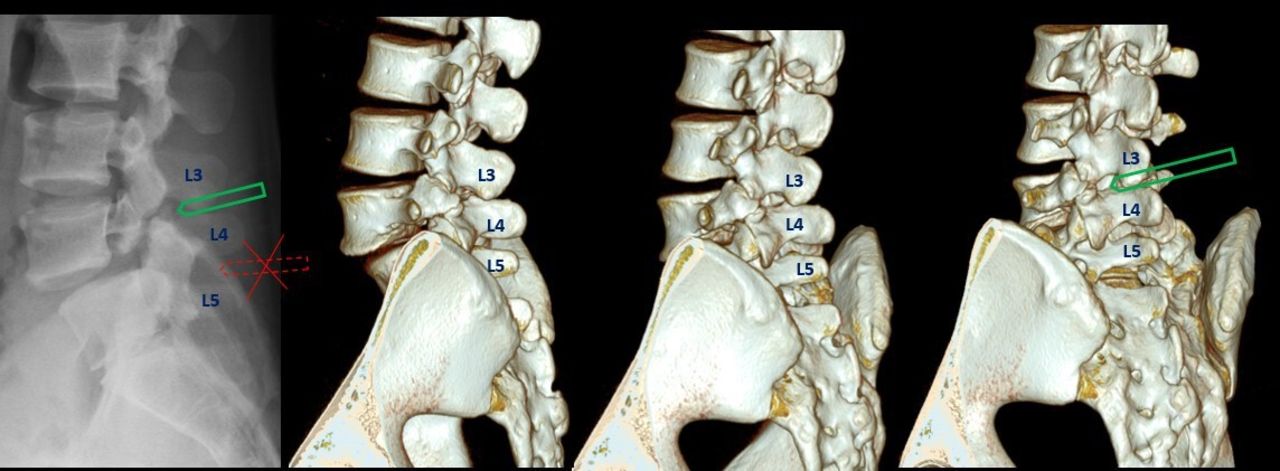
The patients were placed under general anesthesia for percutaneous endoscopic pars decompression for spondylolysis. The patient was placed in the prone position, with their hips and knees flexed. In the case of L5 spondylolysis, the lateral border of the interlaminar window at L4-L5 was the first target site (pars defect at L5 can cause L5-S1 spondylolisthesis) and L3-L4 for L4 spondylolysis (pars defect at L4 can cause L4-L5 spondylolisthesis) on the symptomatic side, under fluoroscopic guidance (Figure 1). A 10-mm skin incision was placed between the subcutaneous tissue and the thoracolumbar fascia. The paraspinal muscles were dissected from the bone of the lamina using a blunt dilator introduced through the incision toward the inferior border of the upper lamina. As the endoscope was introduced after dilatation, a cannula with a bevel was inserted into the lamina surface. A bipolar electrode and micropunches were used to locate the facet joint. To locate the pars defect, the endoscope cannula was transferred caudally next to the facet joint.
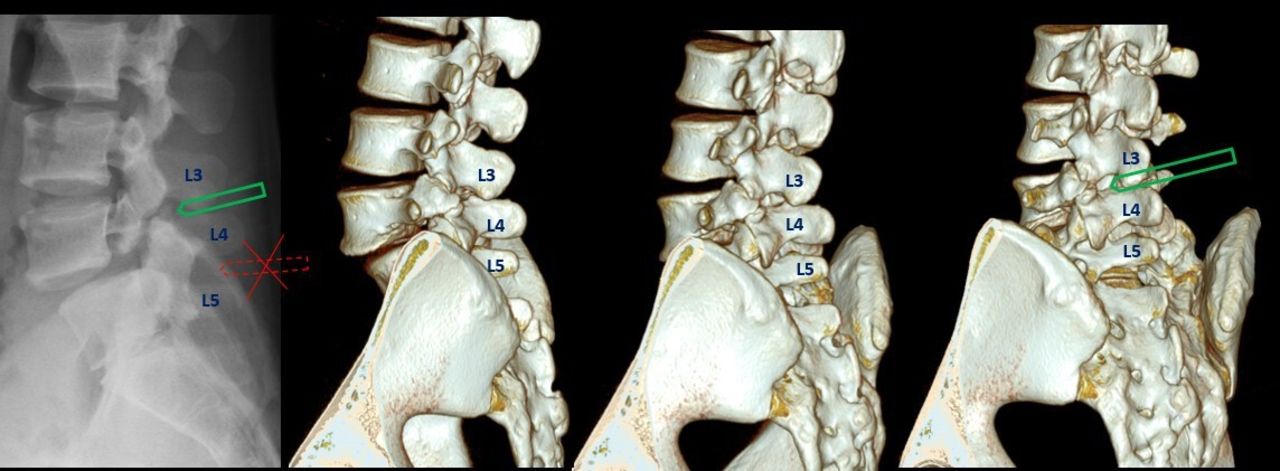
The entry point of endoscope for L4 spondylolysis (L4-L5 spondylolisthesis) is the L3-L4 interlaminar window.
Decompression
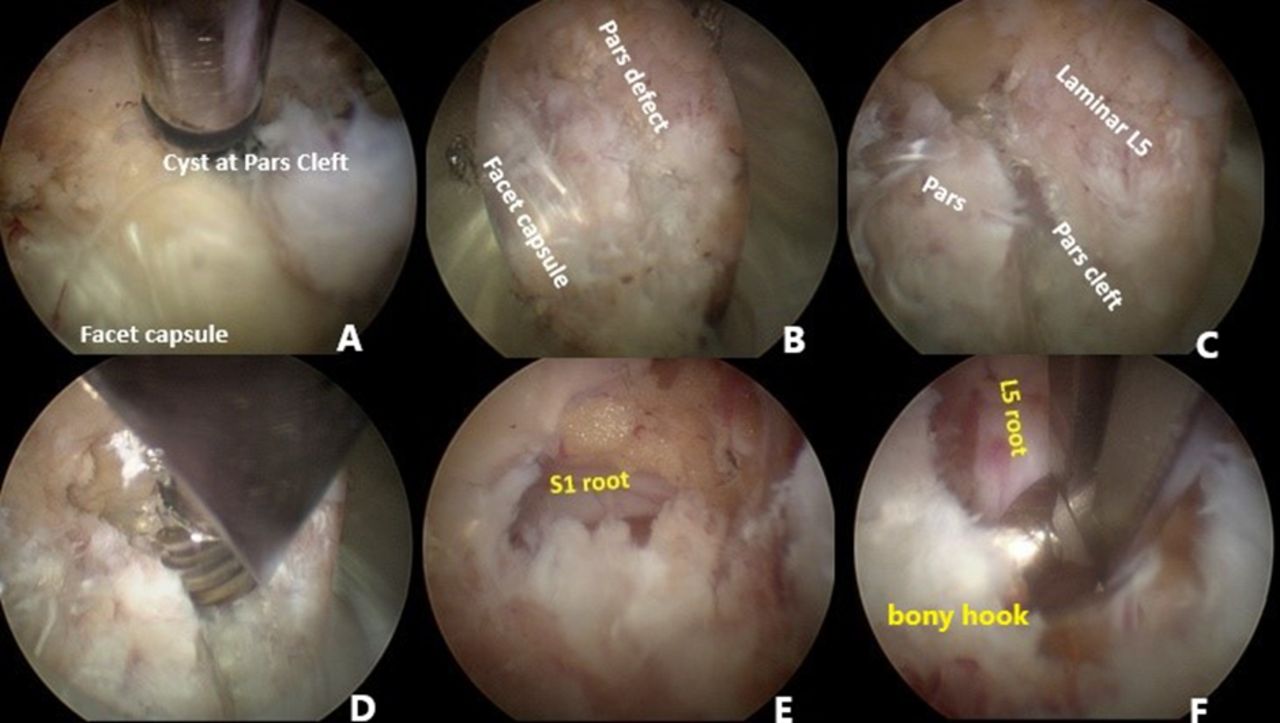
The gap between the pars defect and facet joint was located. The soft tissue and fibrocartilaginous mass in the gap were removed using a burr, rongeur, and radiofrequency probe. After the gap was clear, the traversing nerve root was identified. The next step was to define the hook-like remnant of the proximal deficient lamina of the spondylolytic lesion (bony hook) below the pars defect (Figure 2). Special attention was paid to the exiting nerve root (L5 root in L5 pars defect or L4 root in L4 pars defect), which was moved interiorly and anteriorly to the pars defect. Once the gap was clear after decompression, the bony hook was visible below the defect. In the majority of instances, the bony hook compressed the exiting nerve root firmly. A high-speed burr was used to thin the bony edge, which was then fully removed using a Kerrison rongeur until the nerve root was freed (Figure 3).

The bony hook is the hook-like remnant of the proximal deficient lamina of the L5 lamina below the pars defect in L5-S1 spondylolisthesis, which compresses the L5 exiting nerve root (red arrow).
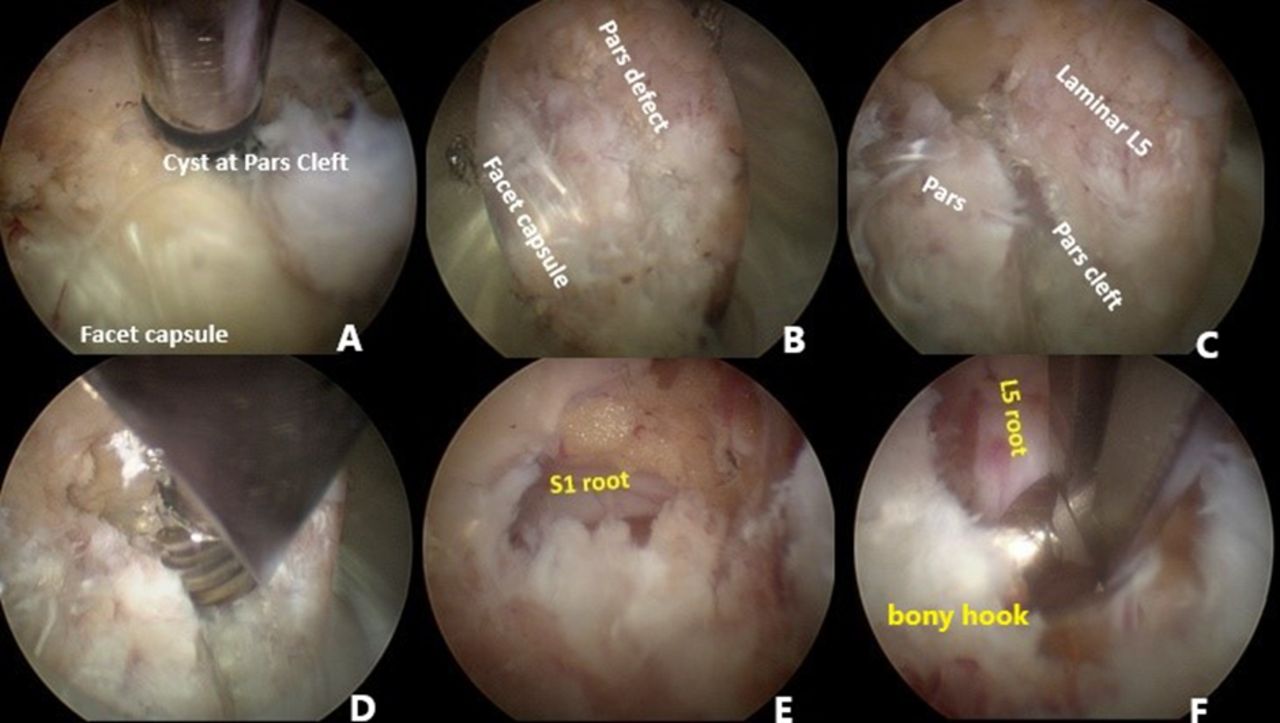
Steps of percutaneous endoscopic pars decompression in L5 spondylolysis (L5-S1 spondylolisthesis). (A) The facet joint of L4-L5 is identified. (B, C) The endoscope cannula is moved to the caudal region adjacent to the facet joint to find the pars defect of L5. (D) The soft tissue and fibrocartilaginous mass in the gap are removed with a burr. (E) After the gap is clear, the S1 traversing nerve is identified. (F) The bony hook below the gap is identified and removed using a Kerrison rongeur until the L5 exiting nerve root is free.
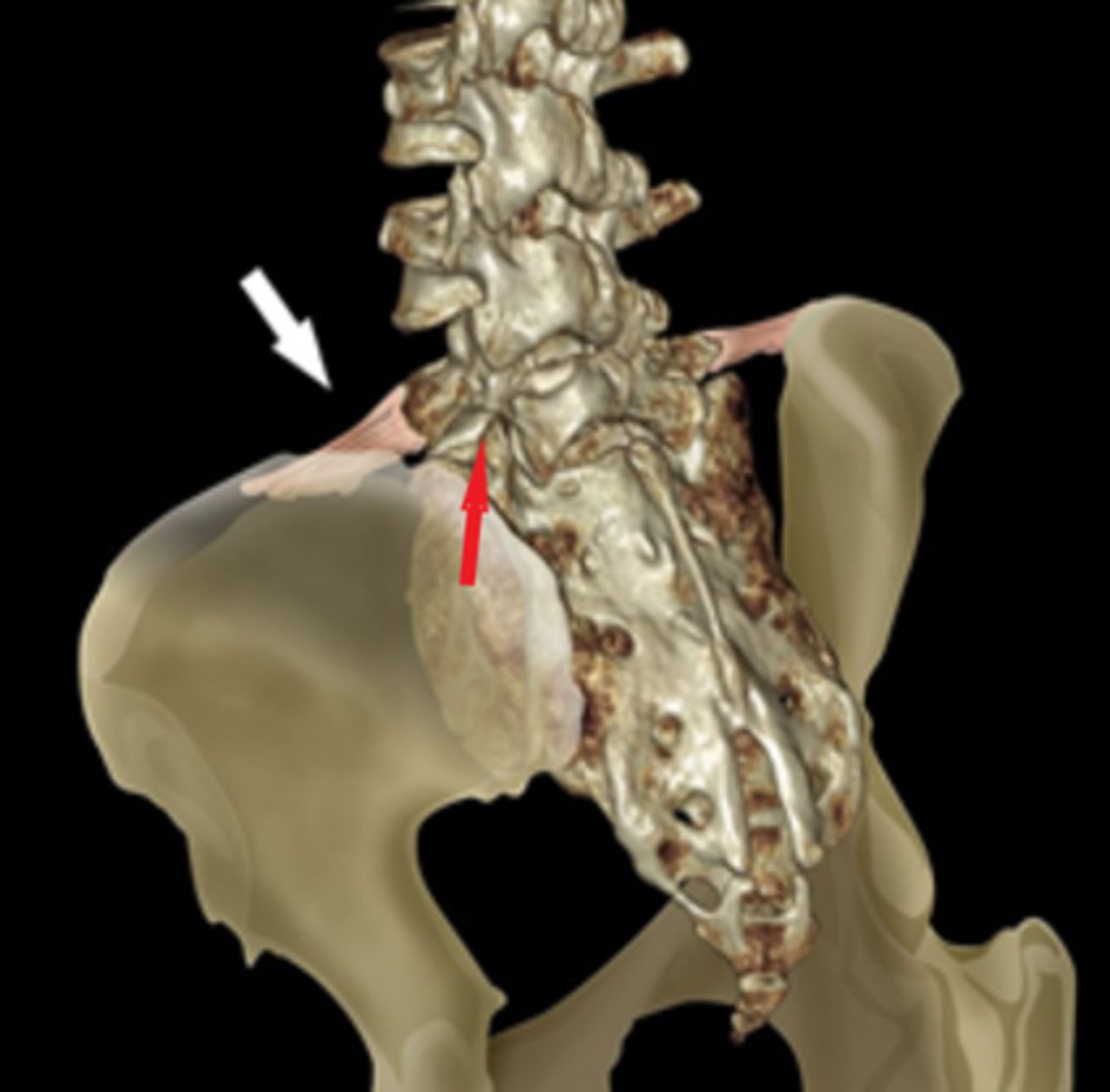
Moreover, during L5 pars decompression, the transverse process of L5 should be protected to prevent iliolumbar ligament injury. According to the role of the iliolumbar ligament, the stability of the lumbosacral junction was maintained to prevent further postoperative vertebral slippage (Figure 4).
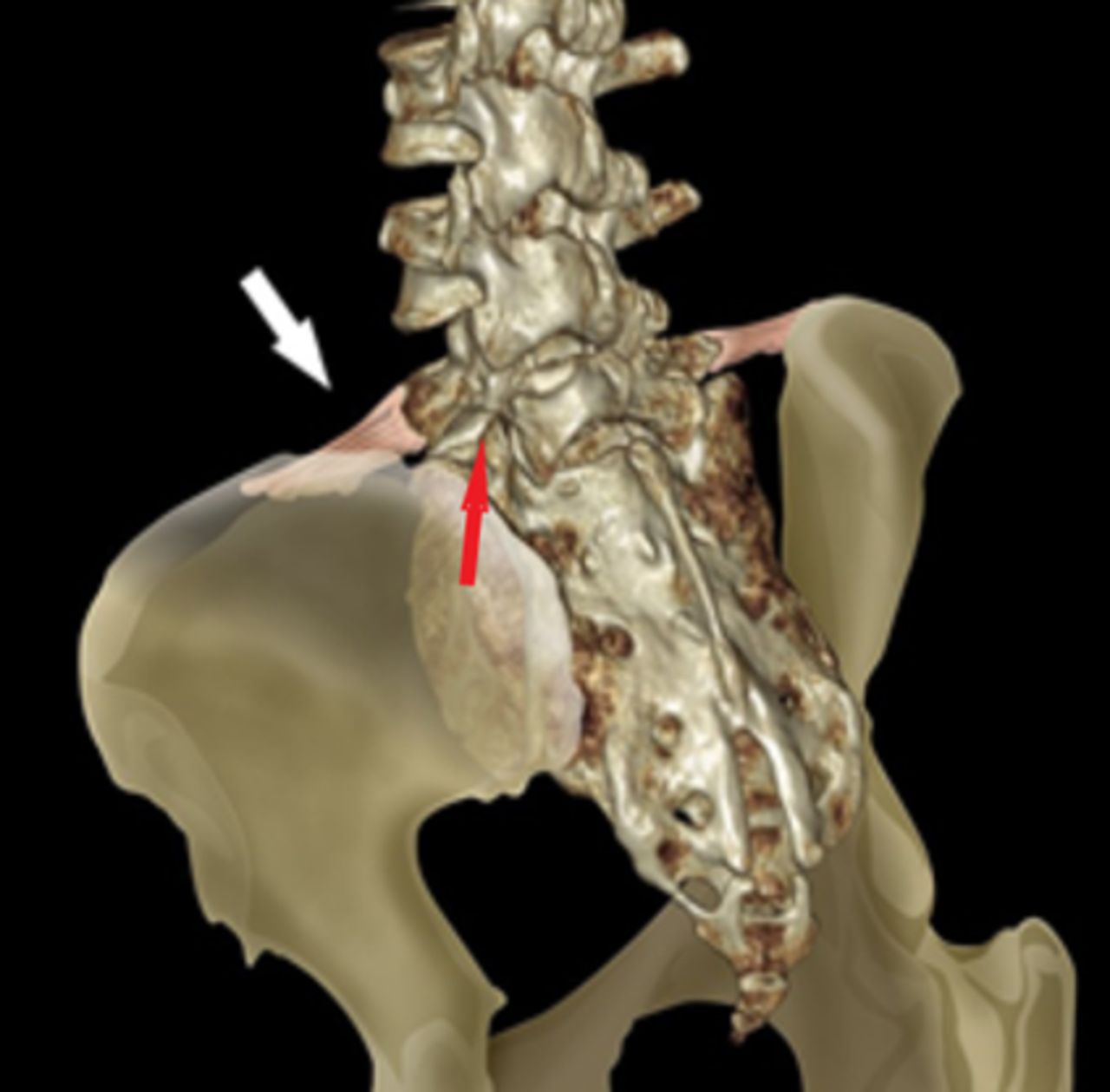
The red arrow indicates L5 pars defect. The iliolumbar ligament binds between the L5 transverse process and the ilium (white arrow).
Representative Case
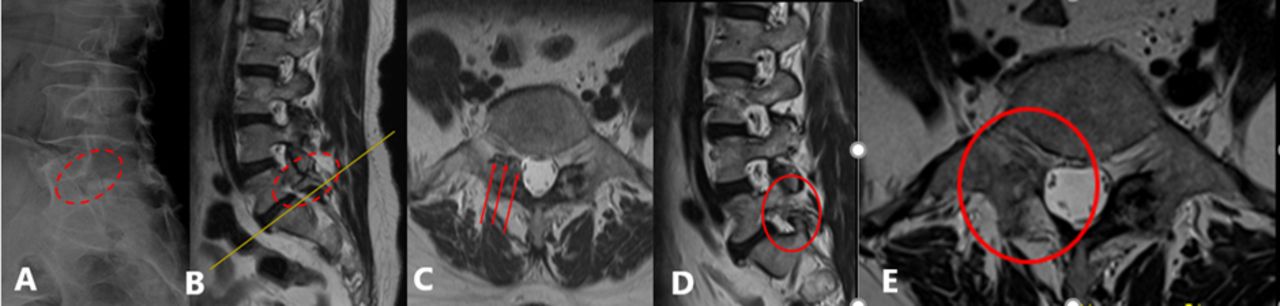
For 6 months, a 56-year-old woman had experienced discomfort and a burning sensation in her right ankle. Her condition had not improved after 3 months of treatment by a foot and ankle expert. MRI showed a pars defect at L5 and compression of the right L5 exiting nerve root in the L5-S1 intervertebral foramen. She had no instability at L5-S1. The patient decided to undergo percutaneous endoscopic pars decompression for right L5-S1. After surgery, the burning sensation of the right ankle had disappeared, and MRI revealed that the L5 exiting nerve root was free from pars compression (Figure 5).
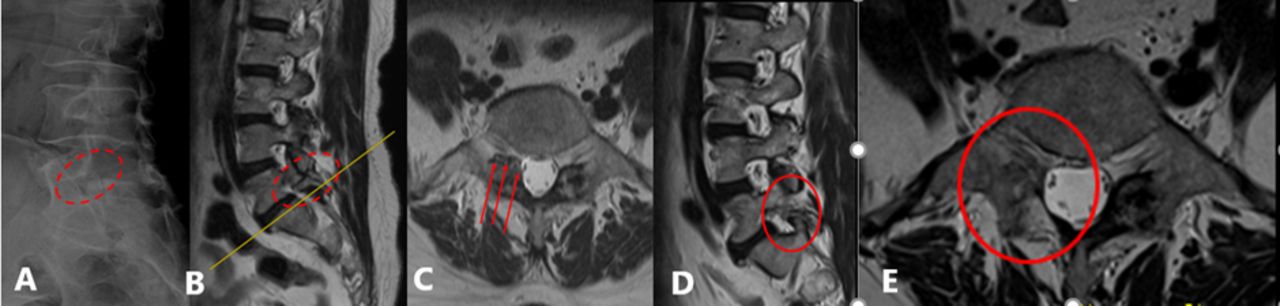
Comparison of pre- and postoperative magnetic resonance images of L5 spondylolysis in a patient who underwent percutaneous endoscopic right L5 pars decompression. (A) The pars defect at L5 observed in a lateral radiograph. (B, C) The right L5 pars defect and L5 exiting nerve root compression in the L5-S1 intervertebral foramen. (D, E) The right L5 exiting nerve root is free after surgery.
Statistical Analysis
The mean and SD of the collected data were calculated. The power was computed using the actual number of samples at a significance level of 0.05. The Wilcoxon signed-rank test was used to compare the preoperative and postoperative VAS scores for leg discomfort, ODI, and % slippage. The VAS and ODI score improvements were compared using an independent sample t test between groups with spondylolysis alone and spondylolysis with vertebral slippage. The statistical significance level was set at P < 0.05.
Results
The study included 11 patients in total, of whom 6 were men and 5 were women, with a mean age of 62.45 years. The average length of follow-up was 22.64 months. Six individuals experienced spondylolysis with vertebral slippage, in addition to concomitant spondylolisthesis. The majority of the slippage was grade 1; only 1 patient reported grade 2 slippage (Table 1). The surgical levels are shown in Table 2.
Demographics and clinical data of the patients.
Level of full endoscopic pars decompression.
Table 3 shows the patient-reported results at the end of the follow-up period. When compared with preoperative levels, the VAS and ODI scores of the patients in the series improved significantly. Moreover, there was no significant difference in % slippage between the preoperative and postoperative periods. Moreover, as can be observed in Table 4, the VAS and ODI scores improved by more than 50% in 90.91% and 63.64% of patients, respectively.
Comparison of clinical outcomes and slippage percentage of interlaminar percutaneous endoscopic pars decompression between the preoperative and postoperative periods.
Improvement rate for VAS and ODI scores after percutaneous endoscopic interlaminar pars decompression.
With regard to the presence of coexisting spondylolisthesis, patients with spondylolysis alone demonstrated significantly greater improvement in ODI score than patients with spondylolistheis after endoscopic pars decompression. No significant changes were observed in the VAS improvement rate (Table 5).
Comparison of VAS and ODI improvement between spondylolysis alone and spondylolysis with spondylolisthesis after percutaneous endoscopic pars decompression.
Discussion
In this study, we investigated the clinical and radiological outcomes of a full endoscopic procedure performed via an interlaminar approach to decompress entrapped nerve roots in patients with lumbar spondylolysis. Our results indicate that this interlaminar percutaneous endoscopic pars decompression is a safe and successful treatment for patients with stable lumbar spondylolysis and nerve root compression. Moreover, we found that, even in situations in which vertebral slippage occurs, spinal fusion may not be the best option for all patients with lumbar spondylolysis.
Lumbar spondylolysis with or without spondylolisthesis presents with 2 clinical symptoms: back pain and radiculopathy. First, low back pain could be caused by pathologic entities, such as discogenic problems, spinal instability, facet cysts, kissing spines, or pars defects.22–24 Second, radicular symptoms produced by nerve root compression from pseudarthrosis of a fractured pars defect. Edelson et al examined 34 bony specimens of isthmic spondylolisthesis and identified the osseous pathoanatomy of L5 exiting root entrapment in L5-S1 spondylolysis with spondylolisthesis. The study suggested that the L5 root is trapped in a stenotic foramen by the hook-like remnant of the proximal deficient lamina up to the base of the L5 pedicle “bony hook” and is increasingly compromised by escalating degrees of slippage.12 The surgical options for spondylolysis should be tailored to the pathoanatomy-related symptoms. To treat low back pain, spinal fusion is required for discogenic pain or spinal instability, while direct pars repair is more favored in young patients. Decompression is needed in radiculopathy due to nerve root compression. When both of these symptoms appear simultaneously, both decompression and fusion should be considered.25
Excision of the loose lamina and nerve root decompression were documented by Gill et al as potential surgical treatments for spondylolysis without fusion,26 and this method has frequently been employed. Arts et al presented long-term follow-up data (mean 10.5 years) for patients who underwent the Gill surgery without fusion and reported a 71% positive patient satisfaction rate with long-term follow-up outcomes.27 Spinal instability, in contrast, is a contraindication. Devis et al also examined data from patients who underwent the Gill surgery and concluded that, in adolescents, spinal fusion is necessary to avoid future vertebral slippage.28
Endoscopic surgery with a small incision has been found to be beneficial for the treatment of lumbar degenerative diseases.29,30 These treatments decrease tissue damage, reduce postoperative discomfort, shorten hospital stays, and allow faster recovery. Sairyo et al described microendoscopic decompression of the lumbar nerve root affected by spondylolysis via the interlaminar approach in 7 selected patients and found excellent outcomes in 3 patients and good outcomes in 4 patients.31
Recently, percutaneous endoscopic techniques have also been used for lumbar spondylolysis. Yeung et al used transforaminal endoscopic decompression in 5 patients with stable isthmic spondylolisthesis and reported markedly positive results in terms of the ODI and VAS scores.32 Liu et al described transforaminal endoscopic lumbar decompression to resect fractured bone or bone fragments and inflamed tissue compressing the L5 exiting nerve root in 2 patients with L5-S1 isthmic spondylolisthesis. Postoperatively, the patient’s back and leg pain were significantly reduced, and physical function was restored.33
However, our full endoscopic technique was different from the previous description. The pars defect is approached directly via the interlaminar window and the fibrocartilaginous mass, and hook-like projection of the proximal lamina, which is the most noteworthy component of exiting root impingement in spondylolysis, is removed.12
Radiculopathy without back pain and the lack of spinal instability on dynamic radiographs were used as surgical indications in the current study. At 22 months after surgery, the mean VAS and ODI scores in this study were considerably better than those before surgery. Furthermore, the VAS and ODI ratings of 90.91% and 63.64% of patients, respectively, improved by more than 50%.
There was no significant difference in the postoperative % slippage as compared with the preoperative period in terms of slippage progression. Our findings were similar to those of Sairyo et al, who observed no additional spondylolysis slippage at 22 months after microendoscopic decompression.31
In the present study, patients with spondylolisthesis showed less improvement in ODI than those without slippage, whereas the VAS score improvement did not differ between the 2 groups of patients. This finding is explained by the study of Wang et al, which indicated that the ODI score was significantly positively correlated with spondylolisthesis grade.34
Of the 11 patients who underwent full endoscopic pars decompression via the interlaminar approach, no patients needed further fusion at a mean follow-up of 22.64 months. Yeung et al performed transforaminal endoscopic decompression for degenerative and isthmic spondylolisthesis in 55 patients and found that 36% of patients needed fusion after 2 years, and 67% needed this procedure at 5 years, respectively.32
The benefit of an interlaminar complete endoscopic pars decompression treatment is that the posterior components, such as the interspinous and iliolumbar ligaments, are preserved. The iliolumbar ligament binds the L5 transverse process to the ileum. Several studies have demonstrated that the iliolumbar ligament plays an important role in preventing anterior displacement of L5 vertebra with a pars defect.35–37 Luk et al studied the development of the iliolumbar ligament by evaluating cadavers and found that the ligament formed during childhood and adolescence by metaplasia of muscle fibers.38 Even though the L5 exiting root was compressed at L5-S1 foraminal area and foraminal approach should be better than via interlaminar, but our experience found endoscopic decompression via the transforaminal approach in patients younger than 40 years should be avoided, to prevent iliolumbar ligament injury and avoid inducing further vertebral slippage. Moreover, we had performed left transforaminal endoscopic decompression at L5-S1 in a 27-year-old man with isthmic spondylolisthesis and found further slippage after surgery.
Our series with percutaneous endoscopic pars decompression via the interlaminar approach found that 1 case developed further slippage at L5-S1 postoperatively. However, the patient did not require fusion surgery. Postoperative CT was analyzed and showed loss of thickness of the left L5 transverse region due to extensive endoscopic decompression that was related to injury to the iliolumbar ligament insertion in the transverse process, and slippage progressed.
This study had some inherent limitations. The first limitation was the small number of patients involved, which made having a control group difficult due to the low prevalence of spondylolysis with radicular symptoms. Because the study’s follow-up time was short, additional research in larger patient populations and with longer follow-up periods should be performed.
Conclusions
Interlaminar percutaneous endoscopic pars decompression is a safe and successful treatment approach for individuals with stable lumbar spondylolysis and nerve root compression. Furthermore, nearly 2 years after the procedure, the slippage rate remained unchanged in our patients. This implies that maintaining spinal stability requires retaining vertebral components, particularly the iliolumbar ligament. Even in situations of vertebral slippage, spinal fusion may not be the best option for all patients with lumbar spondylolysis.
Footnotes
Funding This research received a grant from Paolo Medic Co., Ltd.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}