


Abstract
Background The prone transpsoas (PTP) approach for lateral lumbar interbody fusion (LLIF) is a relatively novel technique. Currently, little is known about its associated complications and early patient-reported outcomes. The aim of this study was to investigate the effect of LLIF performed via the PTP approach on sagittal radiographic parameters, patient-reported outcome measures (PROMs), and rates of complications.
Methods A retrospective review was performed of 82 consecutive patients who underwent LLIF via a PTP technique. Lumbar lordosis (LL), segmental lordosis (SL), anterior disc height (ADH), and posterior disc height (PDH) were measured on preoperative, initial postoperative, and 3-month postoperative radiographs. PROMs including the Oswestry Disability Index (ODI); the visual analog scale (VAS); and pain portions of the EQ5D, VAS back, and VAS leg ratings were collected at the preoperative and subsequent postoperative visits. Length of hospital stay and postoperative complications related to the procedure were recorded.
Results Significant improvements were seen at the initial (4.5° ± 8.6°, P < 0.001) and 3-month (4.4° ± 7.2°, P < 0.001) postoperative periods for LL, as well as SL (6.8° ± 4.8°, P < 0.001; 6.7° ± 4.4°, P < 0.001), ADH (8.0 mm ± 3.6, P < 0.001; 7.4 mm ± 3.6, P < 0.001), and PDH (3.3 mm ± 2.4, P < 0.001; 3.1 mm ± 2.5, P < 0.001). Significant improvements were seen at 3 months postoperatively for ODI (P < 0.001), EQ5D pain (P = 0.016), VAS leg (P < 0.001), and VAS back (P < 0.001). The average length of stay was 2.7 ± 4.5 days. The most common complications were ipsilateral thigh pain/numbness (45.1%), ipsilateral hip flexor weakness (39.0%), and contralateral thigh pain/numbness (14.6%).
Conclusions While early PROMs and correction of sagittal radiographic parameters show promising results for the PTP approach for LLIF, it is not without risks.
Clinical Relevance PTP interbody fusion is an emerging technique that allows for simultaneous access to the anterior and posterior columns of the lumbar spine. This early case series demonstrates significant improvement in functional outcomes and lumbar lordosis with a safety profile comparable to other well-established techniques.
Level of Evidence 3.
Introduction
Lateral lumbar interbody fusion (LLIF) is an increasingly popular minimally invasive technique developed for the surgical treatment of a variety of lumbar spinal pathology including spondylolisthesis, spinal stenosis, and deformity.1–3 This procedure has been shown to be well tolerated with good clinical and radiographic outcomes.4–6 Moreover, it results in less tissue disruption, blood loss, and postoperative pain compared with traditional open surgical approaches.7
Traditionally, LLIFs are performed with the patient in a lateral decubitus position. As LLIFs are usually supplemented with posterior pedicle screw fixation, intraoperative repositioning of the patient to a prone position is often necessary. To obviate the need for positional changes and associated increases in operative time and surgical risk, surgeons have begun to investigate alternate single-position techniques performed from the lateral decubitus8–12 and prone positions.13 Pimenta et al introduced the prone transpsoas (PTP) technique, which involves a minimally invasive approach to the anterior spinal column through the psoas muscle with the patient prone.14 This allows for simultaneous access to both the anterior column and posterior column via a single patient position to allow for circumferential release, direct and indirect decompression, anterior and posterior segmental fixation, and maintenance or correction of alignment.13,15
Few studies to date have evaluated the safety and efficacy of LLIF through a PTP approach. Walker et al compared outcomes between PTP (n = 15) and dual position (n = 15) approaches for patients with single-level spondylolisthesis and demonstrated improvement in segmental lordosis (SL) in those undergoing PTP.15 Farber et al performed a case series of 28 patients with the PTP approach and found a 11% complication rate, 23% subsidence rate with radiographic follow-up, and significant improvement in 3month postoperative functional testing.16 Pimenta et al performed a multicenter study of 32 patients undergoing the PTP approach and found the technique to be associated with a significant gain of SL and correction of spinopelvic alignment.17 These studies, however, were limited by relatively small sample sizes.
Understanding the early complication rates, patient outcomes, and radiographic results of PTP is important for surgeons considering adopting this new technique in their practice. Although it is likely that the long-term outcomes of LLIFs performed via the PTP approach will be similar to those performed with the patient positioned laterally, it is important for surgeons considering utilizing this approach to understand the early safety profile of this approach. If PTP conferred a high risk for early adverse events, it suggests that the procedure in its current state should be avoided. However, if the safety profile is in line with previous reported outcomes and is similar to that of laterally performed LLIFs, then continued research into long-term outcomes would be warranted. The goal of this study is to evaluate the early efficacy of PTP at restoring lumbar sagittal radiographic parameters and improving patient-reported outcome measures (PROMs). Additionally, this study aims to evaluate the early complications associated with this procedure. The authors hypothesized that PTP would effectively improve sagittal radiographic parameters and produce significant improvements in patient outcome measures, with a similar safety profile compared with the traditional LLIF approach.
Methods
Patient Selection
Prior to the initiation of this study, approval from the institutional review board was obtained. All patients who underwent lateral interbody fusion from a PTP approach were included for analysis regardless of surgical indication. Patients required a minimum of 1 month follow-up for inclusion. This timepoint was chosen to optimize the number of patients evaluated for immediate postoperative complications. Surgeries occurred between 5 November 2020 and 30 March 2022. Patients were excluded if they underwent greater than 5 levels of overall fusion. Age and gender were collected for each patient. Additionally, the levels at which the PTP approach was used and the total number of levels instrumented were collected.
Surgical Technique
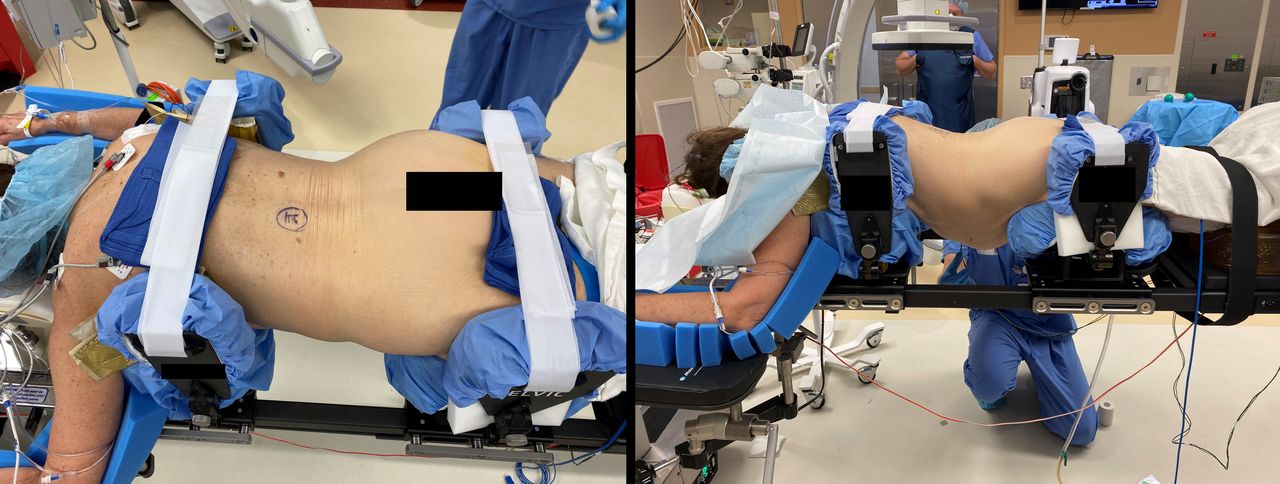
All surgeries were performed by 1 of 3 surgeons. The overall technique for the PTP approach and instrumentation is the same among the surgeons. Patients are positioned prone on a Jackson table with PTP bolsters (PTP Patient Positioner, ATEC, Carlsbad, CA, USA) to stabilize the torso and allow for control of separation between the pelvis and the ribs on the operative side (Figure 1). Neuromonitoring (SafeOps, ATEC, Carlsbad, CA, USA) of somatosensory-evoked potentials and triggered electromyography (EMG) is utilized throughout the procedure. Fluoroscopy is utilized to confirm the correct level. An incision is made through the skin and fascia, followed by blunt dissection through the external oblique, internal oblique, and transverse abdominus muscles. After piercing the deep fascia of the transverse abdominus, the retroperitoneal space is developed, and the psoas is palpated. An appropriate docking point over the midpoint of the intended disc is found using fluoroscopy and triggered EMG to ensure a safe neurologic corridor. After sequential dilation, a retractor specifically designed for this procedure (Sigma LIF-PTP Access System, ATEC, Carlsbad, CA, USA) is inserted over the dilators and opened sufficiently to access the disc space. After confirming the absence of motor nerves within the field using an EMG probe, shims are inserted to stabilize the retractor. Annular release on the ipsilateral and contralateral side is followed by disc space and endplate preparation, trialing and insertion of the final implant (IndentiTi-LIF, ATEC, Carlsbad, CA, USA) packed with demineralized bone matrix (AlphaGRAFT DBM Putty, ATEC, Carlsbad, CA, USA), and impacted into the intervertebral space. In cases where inadvertent anterior longitudinal ligament (ALL) rupture is suspected, a lateral antimigration plate attached to the implant (AMP, ATEC, Carlsbad, CA, USA) is placed. All cases in this series underwent posterior instrumentation with either percutaneous or open pedicle screws and posterolateral fusion.
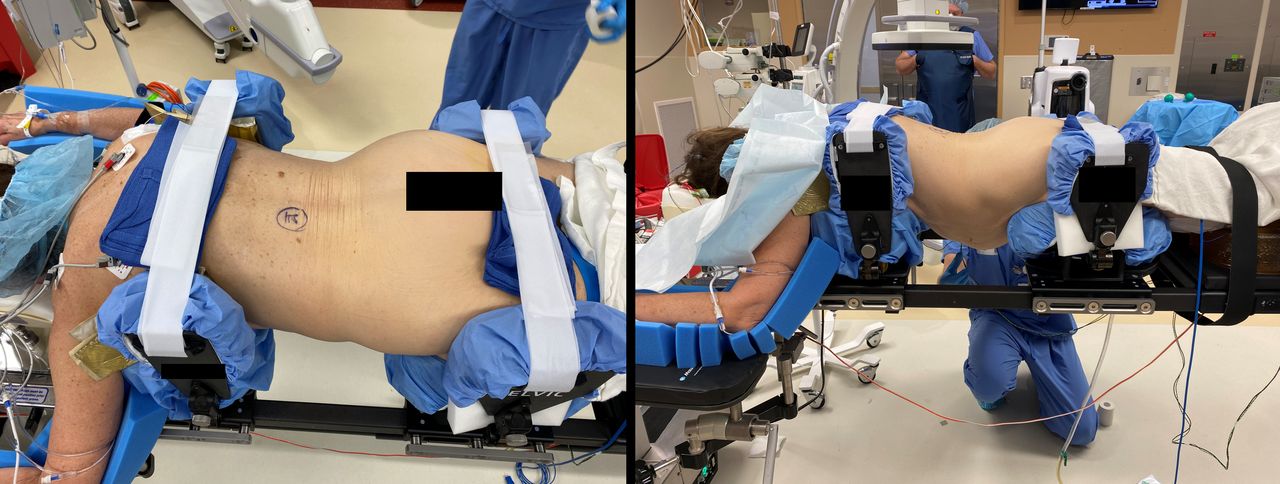
Intraoperative images depicting standard prone patient positioning. Pads placed below the axillae and around the hip induce a convex bend in the patient’s abdomen, opening up the near side of the disc space.
Radiographic Data Collection
Preoperative, as well as initial postoperative and 3-month postoperative lateral lumbar radiographs were assessed for each patient. Initial postoperative imaging was obtained on the first postoperative day in most patients and on the second postoperative day for any remaining patients. Patients with follow-up less than 3 months were excluded from a 3-month radiographic analysis. For each timepoint, lumbar lordosis (LL), SL, anterior disc height (ADH), and posterior disc height (PDH) were measured (Figure 2). LL was defined as the angle between the superior endplate of L1 and the superior endplate of S1. SL was the angle between the inferior endplate of the superiorly instrumented vertebrae and the superior endplate of the inferiorly instrumented vertebrae. ADH and PDH were the distances between the superior endplate of the inferior vertebrae and the inferior endplate of the superior vertebrae at the anterior and posterior intervertebral disc spaces, respectively.

Illustration of sagittal radiographic parameters collected.
Measurements were obtained by 2 investigators: a spine fellow and an orthopedic resident. To ensure interrater reliability between the 2 investigators, a random sample of 10 patients was measured by each investigator, and interclass correlation (ICC) analyses were performed. ICC values greater than 0.8 were deemed acceptable. Measurements were obtained at each level with instrumentation placed via the PTP approach. In multilevel procedures, LL was only measured once. In cases of severe scoliosis, in which accurate segmental measurements on lateral radiographs were not possible, patients were excluded from analysis.
Patient-Reported Outcomes
PROMs are collected from all patients pre- and postoperatively at the authors’ institution, including those patients in this study. Outcome measures were collected preoperatively, as well as at 2 weeks, 6 weeks, and 3 months postoperatively. Patients without available outcome measures, either due to lack of follow-up or lack of questionnaire completion, were excluded from this portion of the analysis. Oswestry Disability Index (ODI), the pain portion of the EQ5D (pain), the visual analog scale (VAS overall) portion of the EQ5D, as well as the VAS leg pain (VAS leg) and VAS back pain (VAS back) scores were collected for each patient. Additionally, global rating of change pain and functional scores were collected for each patient. Finally, patient acceptable symptom state scores were collected at each postoperative visit.
Complications
To determine the rate of postoperative complications, a medical record review was performed by a single investigator. Each patient’s operative report, as well as their postoperative and follow-up notes was reviewed for all complications related to the index procedure. Hip flexor pain and weakness were defined as pain or weakness with resisted hip flexion that occurred after the first postoperative day. All complications that occurred within 3 months of the index procedure were included.
Statistics
The number of single, 2-level, 3-level, and 4-level instrumentations and the disc spaces instrumented were expressed as proportions of the whole. For radiographic outcomes, paired sample t tests were used to compare the initial postoperative and the 3-month postoperative radiographic measurements with the preoperative measurements. Similarly, paired sample t tests were used to compare PROMs at 2 weeks, 6 weeks, and 3 months with the preoperative measurements. Global rating of change pain and functional scores, which are not obtained preoperatively because they are assessments of improvement after a procedure, were reported as the proportion of patients who reported at least a 10 (“a little bit better”) and those that reported at least a 13 (“quite a bit better”). A cutoff of 10 was chosen as it indicates the percentage of patients who experienced at least mild improvement from the procedure, while 13 was chosen as it indicates the proportion of patients who significantly benefied from the procedure. The percentage of patients reporting a positive patient acceptable symptom state score was reported as a proportion of the whole. All statistical analyses were performed using SPSS (v28, IBM, Armonk, NY). A P value of 0.05 or less was considered statistically significant.
Results
A total of 82 patients underwent lateral interbody fusion via a PTP technique with a total of 133 levels instrumented (Table 1). The mean age was 63 ± 12 years, and 56% of patients were women. Of the 82 total patients, 56% were single-level PTPs, 32% were 2-level, and 6% each were 3- or 4-level PTPs. The most commonly instrumented level was L4-L5 (34%), followed by L3-L4 (33%), L2-L3 (23%), and L1-L2 (8%). With PTP and non-PTP instrumented levels included, 43% of patients underwent single-level fusion, 28% had 2 levels fused, 16% had 3 levels fused, 10% had 4 levels fused, and 2% had 5 levels fused. An anterior lumbar interbody fusion was performed concomitantly in 1 patient (1.2%). Single-level transforaminal lumbar interbody fusion was performed concomitantly in 10 patients (12.2%), while 6 patients underwent concomitant 2-level transforaminal lumbar interbody fusion (7.3%).
Demographics of patients undergoing the PTP approach to lateral lumbar interbody fusion (N = 82).
The ICC values were 0.976 for LL, 0.920 for SL, 0.940 for ADH, and 0.885 for PDH. The average preoperative LL was 46° ± 13°, SL was 5° ± 5°, ADH was 8 mm ± 4, and PDH was 4 mm ± 3. LL was significantly improved by 4.5° ± 8.6° on the initial postoperative imaging (P < 0.001) and by 4.4° ± 7.2° on 3-month postoperative radiographs (P < 0.001) (Table 2). SL increased by 6.8° ± 4.8° on initial postoperative radiographs (P < 0.001) and 6.7° ± 4.4° at 3 months (P < 0.001). ADH increased by 8.0 mm ± 3.6 (P < 0.001) and 7.4 mm ± 3.6 (P < 0.001) at the initial postoperative and 3-month timepoints, respectively. Finally, PDH increased by 3.3 mm ± 2.4 (P < 0.001) and 3.1 mm ± 2.5 (P < 0.001) at the initial postoperative and 3-month timepoints, respectively.
Radiographic measurements.
The average length of stay was 2.7 ± 4.5 days. ODI values initially nonsignificantly worsened at the 2-week postoperative visit; however, these values significantly improved relative to their preoperative values at 6 weeks (−7.7 ± 20; P = 0.023) and 3 months (−18.3 ± 17.4; P < 0.001) (Table 3). Pain EQ5D scores improved at all 3 timepoints (−0.4 ± 1, –1.0 ± 1.1, –0.8 ± 0.4; P = 0.017, P < 0.001, P = 0.016), as did leg VAS scores (−2.3 ± 4.1, –3.3 ± 3.6, –3.8 ± 3.4; all P < 0.001) and back VAS scores (−1.6 ± 2.5, –3.3 ± 3.1, –3.9 ± 3.2; all P < 0.001). VAS EQ5D scores remained unchanged at 2 weeks (P = 0.541) and 3 months (P = 0.145) but were significantly improved at 6 weeks (6.6 ± 15.8; P = 0.012).
Patient-reported outcomes.
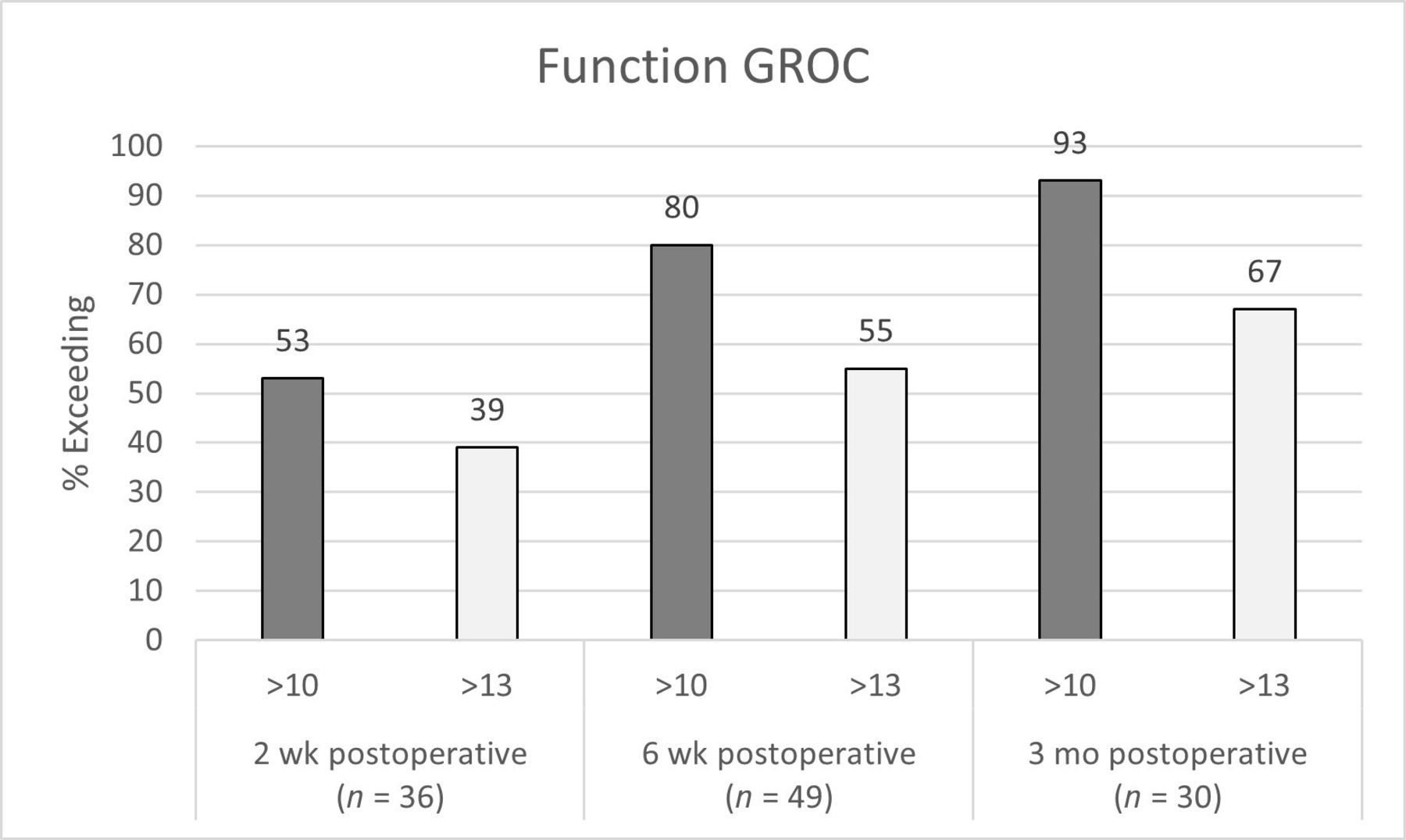
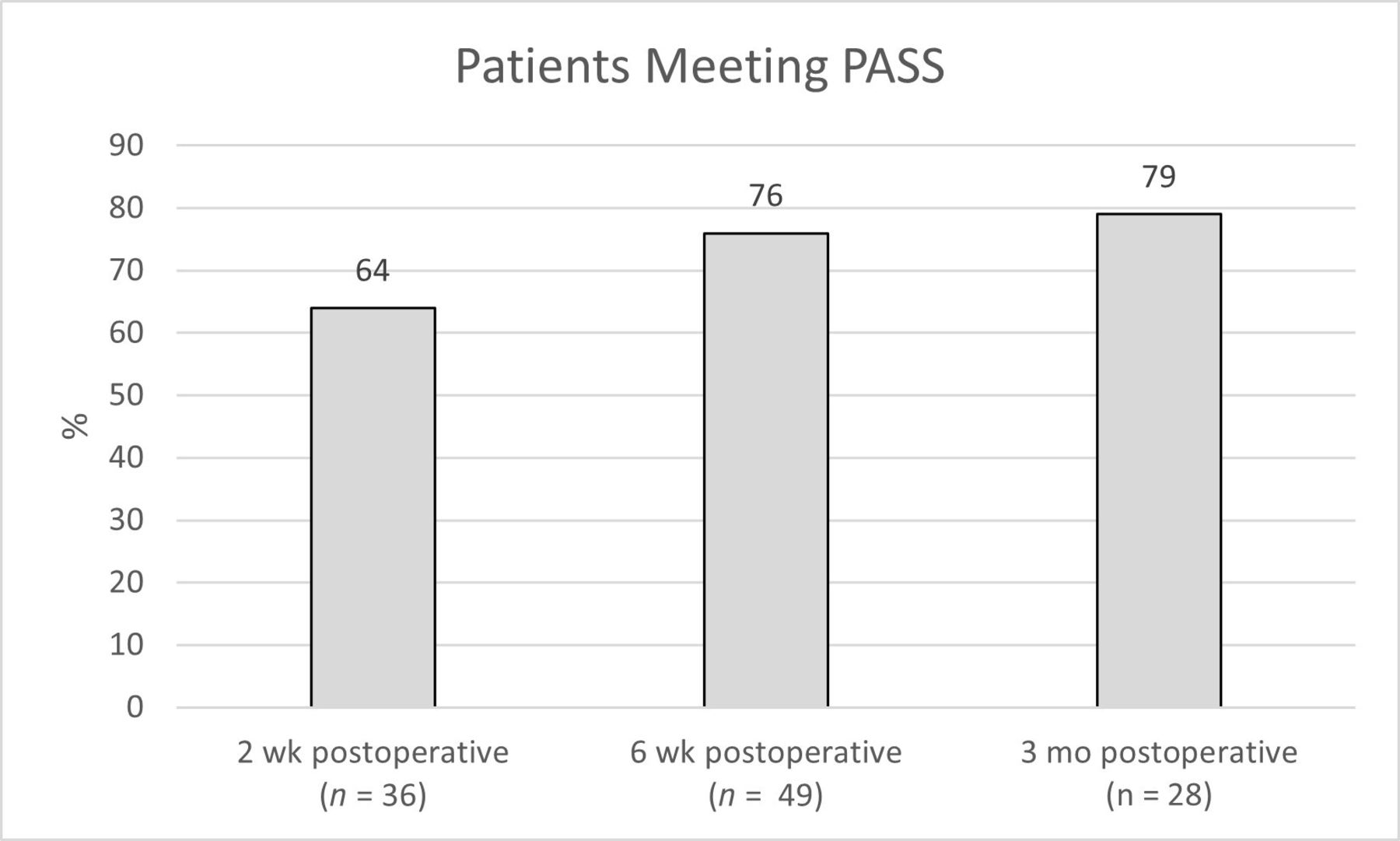
At 2 weeks from surgery, 53% of patients reported at least a “little bit better” function compared with their preoperative state (Figure 3). This improved to 80% at 6 weeks and 93% at 3 months. Similarly, 39% reported that their function was “quite a bit better” at 2 weeks, while 55% and 67% reported “quite a bit better” function at 6 weeks and 3 months, respectively. Pain followed a similar trend with 58% reporting at least “a little bit better” improvement at 2 weeks, 86% at 6 weeks, and 87% at 3 months (Figure 4). Twenty-eight percent reported their pain as at least “quite a bit better” at 2 weeks, 67% at 6 weeks, and 73% at 3 months. At 2 weeks from surgery 64% of patients reported being at an acceptable symptomatic state (Figure 5). This improved at 6 weeks to 76% of patients, and at 3 months to 79% of patients.
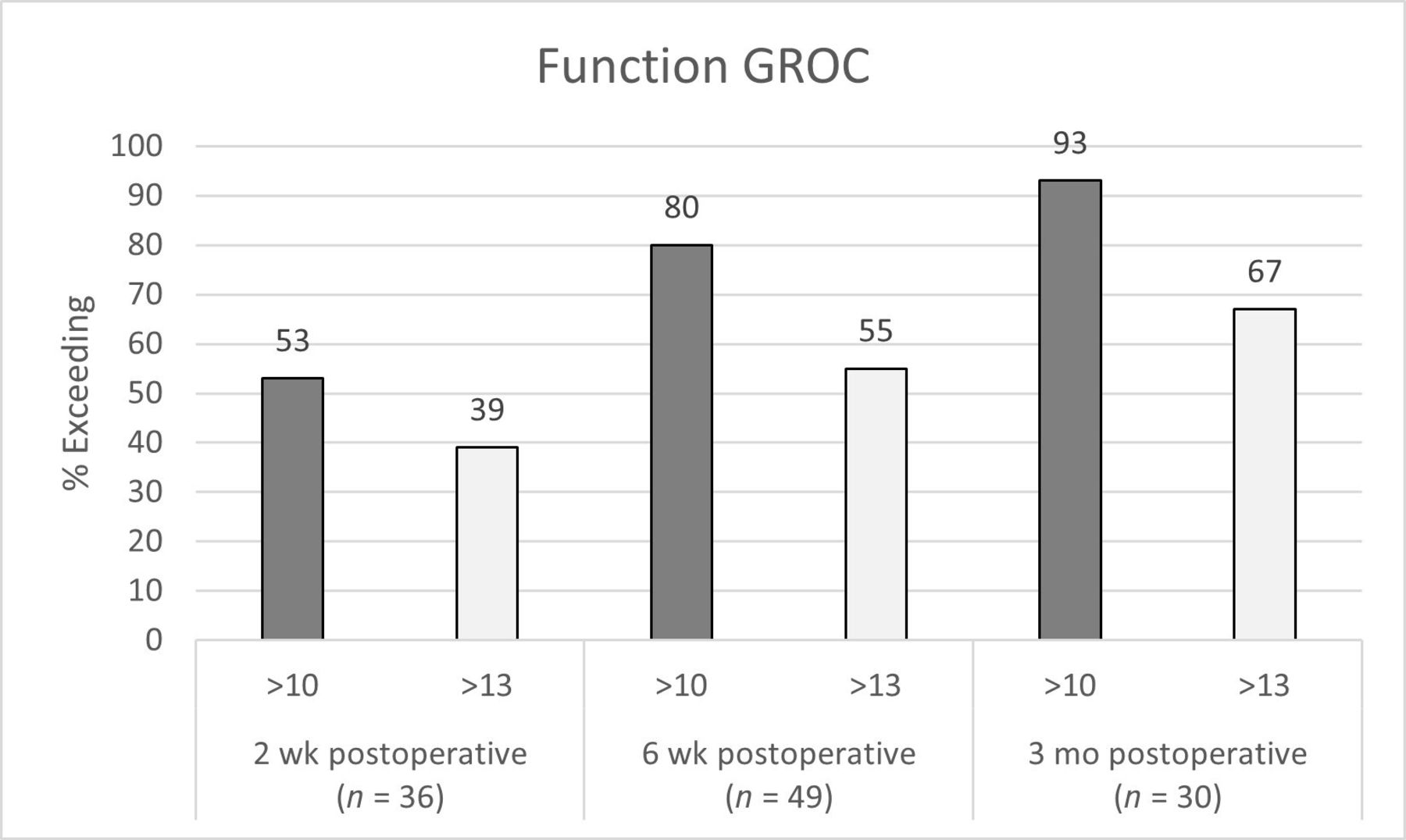
Function global rating of change (GROC) scores at 2 wk, 6 wk, and 3 mo from surgery.
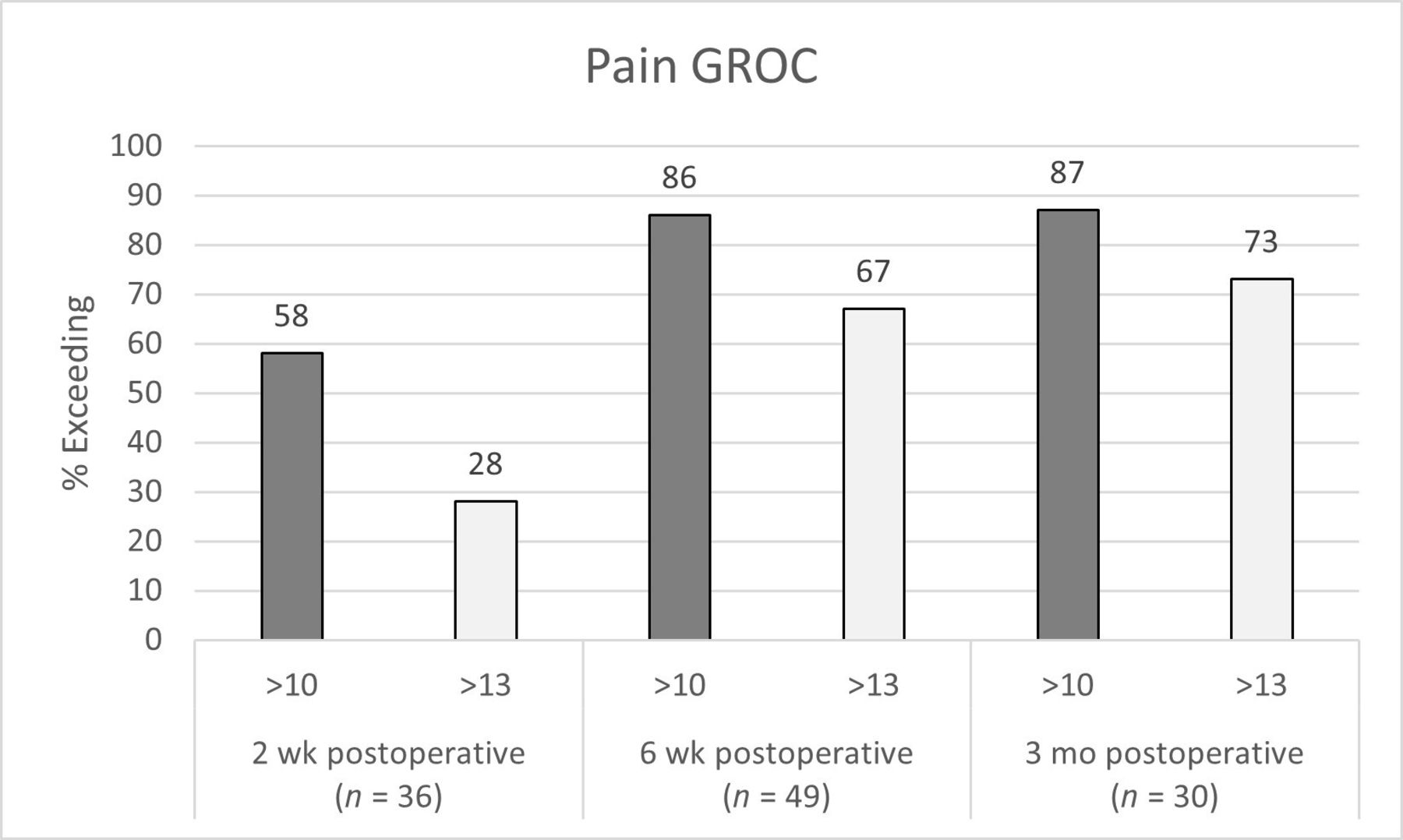
Pain global rating of change (GROC) scores at 2 wk, 6 wk, and 3 mo from surgery.

Patient acceptable symptom state (PASS) scores at 2 wk, 6 wk, and 3 mo from surgery.
Sixty-two patients (76%) experienced at least 1 postoperative complication related to their index procedure (Table 4). The most common complication was ipsilateral hip flexor pain (45%) followed by ipsilateral hip flexor weakness (39%). Intraoperative ALL rupture occurred in 3 (3.7%) of the patients. Additionally, 4 patients had a PTP level aborted after incision due to lack of a safe neurological corridor through the psoas. There was 1 case of subsidence >2 mm on 3-month postoperative radiographs. Additionally, there were 2 cases of femoral nerve palsy (2.4%) and 2 cases of death (2.4%). Both femoral nerve palsies fully recovered within 3 months of surgery. Both deaths were unrelated to the surgical approach: one of the deaths was secondary to complications from an aspiration pneumonia sustained postoperatively, and the other death was of unknown cause. This death occurred 2 weeks after surgery in a patient who was found deceased at home but had otherwise been recovering uneventfully.
Postoperative complications.
Discussion
Patients in our study undergoing PTP LLIF demonstrated significant improvement in LL and SL as well as ADH and PDH at both initial postoperative imaging and 3 months. ODI improved significantly at 6 weeks and 3 months. Pain improved significantly at all timepoints, while EQ5D VAS score demonstrated significant improvement at 6 weeks. Both leg and back pain improved significantly at all timepoints postoperatively. A majority of patients experienced at least some improvement in pain and function at 2 weeks from surgery, with 67% and 73% reporting a significant improvement in pain and function, respectively, at 3 months. The most common postoperative complications were bilateral hip flexor pain and ipsilateral hip flexor weakness. Recent studies have shown similar findings when evaluating the PTP approach, but none have included as large of a sample size as the current study.15–17
The maintenance and correction of sagittal balance are common topics within the spine surgical literature because of its direct impact on positive surgical outcomes and quality of life.18 LL, a key feature in maintaining sagittal balance, has been demonstrated to be especially important both clinically and functionally.19–23 Alimi et al evaluated radiological outcomes of laterally performed LLIF in 90 degenerative disc disease patients (145 vertebral levels) at midterm follow-up and demonstrated lumbar sagittal lordosis increases of 5.3° postoperatively (P < 0.0001) and 2.9° at latest follow-up (P = 0.014).24 Rothrock et al’s meta-analysis reported that the mean increase of SL with laterally performed LLIFs varied from 2.9° to 4.0°.25 Similarly, a systematic review by Ahlquist et al demonstrated that the mean gain of SL with LLIF was 4.4°.26 Campbell et al evaluated short-term (mean 6.2 months) outcomes of laterally performed LLIF without decompression for the treatment of symptomatic degenerative spondylolisthesis at L4-L5 and demonstrated a mean global lordosis increase of 2.1° (60.3° preoperatively and 62.4° postoperatively).1 In a radiographic review of 43 patients, Sharma et al found that although lateral LLIF significantly improved lumbar scoliosis and SL, there was no significant effect on global lordosis.27 Similarly, Johnson et al evaluated the radiographic effects of LLIF on 22 patients and found significantly increased segmental LL by 3.3° (P < 0.0001), but this did not change overall LL or significantly alter pelvic indices associated with sagittal balance.28 Our data show that PTP LLIF improves LL and SL by 4.4° (P < 0.001) and 6.7° (P < 0.001), respectively, at 3-month follow-up. We suggest that these early results are comparable or superior with those reported in previous studies evaluating the radiologic effects of LLIF on LL. These improvements in lordosis may be attributable to the prone positioning of the patient during interbody insertion as opposed to laterally performed LLIFs.
Alimi et al’s study of laterally performed LLIF outcomes at 17.6 months reported improvement in ODI 21.1 and VAS scores for back, buttock, and leg pain by 21.1 and 3.7, 3.6, and 3.7 points, respectively (P < 0.0001).24 Campbell et al demonstrated that LLIF improved mean ODI score by 29.7% at 3-month follow-up and 53% at 6-month follow-up.1 Phillips et al’s prospective multicenter study evaluated 107 patients with degenerative scoliosis treated with LLIF with or without supplemental posterior fixation and found significant mean improvements in ODI, VAS for back pain and leg pain, and short form-36 physical and mental component scores at 24-month follow-up.29 Similarly, Kotwal et al demonstrated improvements of 53%, 43%, and 41% in VAS for pain, ODI, and the physical components summary of short form-12, respectively, at minimum 2-year follow-up after LLIF.30 Our study demonstrates that PTP is associated with similar short-term improvements in PROMs. ODI improved significantly at 6 weeks and 3 months. Pain improved significantly at all timepoints, while EQ5D VAS score demonstrated significant improvement at 6 weeks. Both leg and back pain improved significantly at all timepoints. While some measures such as ODI and VAS were initially worse upon immediate follow-up, this is to be expected given that initial postoperative pain may take weeks or months to resolve. For example, while ODI values initially nonsignificantly worsened at the 2-week postoperative visit, this proved transient as these values improved relative to their preoperative counterparts at 6 weeks (P = 0.023) and 3 months (P < 0.001).
Reported complications following laterally performed LLIF include neurologic injury, hip flexion weakness, vascular injury, subsidence, vertebral body fracture, pseudohernia, visceral injury, and wound infections. The incidence of thigh paresthesia and numbness after LLIF has been reported to range widely from 0.7% to 30%, and the incidence of motor weakness has ranged from 3.4% to 23.7%.31–34 However, when neurological symptoms occur, most are temporary, with 90% resolving spontaneously within a year after surgery.33 In the largest consecutive case series of 600 patients treated with laterally performed LLIF, Rodgers et al reported a 0.7% incidence of transient neurological injury.32 Our results of thigh numbness of 7.3% and femoral nerve palsy of 2.4% are well within reported ranges for both LLIF and PTP.13,17 Moreover, our finding of 39% hip flexor weakness is both comparable with the 27.5% reported by Tohmeh et al and likely transient.35 Subsidence was reported by Le et al to be 14.3% at mean follow-up of 14.3 months; our rate of 1.2% is significantly lower, though this finding possibly stems from our shorter follow-up duration.36
Several authors have reported the incidence of ALL rupture to be 8% to 9% of patients for the treatment of adult degenerative scoliosis using laterally performed LLIF.37,38 The rate of incidental rupture of the ALL was reported to be 0.8% with oblique lumbar interbody function or LLIF in a nationwide survey in Japan.39 Maruo et al found the incidence of ALL rupture after adult spinal deformity surgery using oblique lumbar interbody function or LLIF to be 22% among patients and 8.6% among disc levels.40 Our cohort had a rate of ALL rupture of 3.7% among patients and 2.3% per level, suggesting decreased risk relative to laterally performed LLIF. However, this may be secondary to differences in surgeon technique or due to unidentified ALL ruptures in this cohort.
This study has several limitations, including its retrospective nature, which could generate bias in data gathering and analysis. Importantly, however, all PROMs were obtained prospectively. The authors attempted to utilize broad inclusion criteria to minimize selection bias. The short-term follow-up of 3 months does not allow for clear differentiation between temporary and permanent neurologic and pain-related complications, and longer-term follow-up will therefore be necessary for further evaluation of complications, radiographic parameters, and subsidence. This study was a single-center study in which all surgeries were performed by 3 surgeons, which may have increased the margin of error and decreased generalizability. However, limiting the number of surgeons enabled us to ensure consistency of surgical technique and postoperative care. Given that complications were identified with use of chart review, there is a possibility that not all complications were documented appropriately and are therefore missing from the data. Moreover, our data set was missing inputs for PROMs due to lack of patient completion; as a result, there were fewer patients in these groups, which may have affected the results of subsequent analysis and may introduce a response bias.
Conclusions
This study is the largest cohort study to date to report early outcomes of PTP LLIF. Our patients demonstrated significant improvement in LL and SL, ADH and PDH, and PROMs at 3-month follow-up. Complications including hip flexor pain and weakness were comparable with similar studies evaluating laterally performed LLIFs. While these results are limited to the immediate postoperative period, they are clinically important as they suggest that the LLIF in the prone position using this technique is, at least, a safe alternative to lateral decubitus positioning. The benefits and risks of this procedure are important to consider when determining procedure plans and counseling patients. Prospective study is warranted to directly compare prone positioning with lateral positioning for transpsoas lumbar interbody fusion.
Acknowledgments
The authors would like to acknowledge Dr. Geneva Hargis for creating the illustration used in this study.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Hardeep Singh and Isaac Moss are paid consultants for Alphatec.
Disclosures Ian Wellington, Christopher Antonacci,Chirag Chaudhary, Ergin Coskun, Mark Cote, and Scott Mallozzi have nothing to disclose. Hardeep Singh serves as a consultant for Stryker and Alphatec. Isaac Moss receives royalties from Spineart and Alphatec, owns stock in Spinal Simplicity and Orthozon, and is a consultant for Stryker, Biedermann, Alphatec, Spinewave and Nuvasive.
Ethics Approval Approval was obtained from our institution’s institutional review board prior to the initiation of this study.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}